
Abstract
Purpose:
To investigate the effect of adjuvant mitomycin C (MMC) on severe traumatic retinal detachments (RDs) with advanced proliferative vitreoretinopathy secondary to open-globe injury, managed with relaxing retinotomy and retinectomy.
Methods:
Medical records of 43 consecutive patients with traumatic RD undergoing relaxing retinotomy and retinectomy between 2016 and 2022 were retrospectively analyzed. Patients were categorized into those who received 20 µg/mL MMC via the MMC sandwich method (group 1) and those who did not (group 2). Preoperative characteristics, surgical interventions, and postoperative outcomes were compared.
Results:
Group differences in baseline variables were not statistically significant, except for the time interval between trauma and vitrectomy (P = .018). The mean (±SD) follow-up time was 29.6 ± 10 months. The preoperative best-corrected visual acuity (BCVA) was a median 3.00 logMAR (interquartile range [IQR], 1.00–4.00) in group 1 and 3.50 logMAR (IQR, 1.30–4.00) in group 2. Postoperatively, the median BCVA was 1.85 logMAR (IQR, 0.00–3.00) in group 1 and 3.00 logMAR (IQR, 0.50–4.00) in group 2 (P < .001). The final sustained retinal attachment rate was 95% in group 1 and 68% in group 2 (P = .022). The postoperative intraocular pressure was a median 14 mm Hg (IQR, 8–18) in group 1 and 14 mm Hg (IQR, 4–17) in group 2 (P = .220). There was no MMC-related toxicity observed.
Conclusions:
MMC can be safely used with the MMC sandwich technique for severe traumatic RDs managed by relaxing retinotomy and retinectomy, with favorable anatomic and functional outcomes despite the small sample size.
Introduction
Proliferative vitreoretinopathy (PVR) is characterized by epiretinal membrane, intraretinal fibrosis, and subretinal bands, which are caused by an abnormal proliferation and accumulation of non-neural retinal cells after retinal detachment (RD). 1 Retinal reattachment with RD surgery is often not achieved because of the presence of PVR. 2 Trauma is the most important risk factor for development of PVR, increasing the risk to 50% to 70%.3,4 Despite the use of antiproliferative agents as a common treatment, PVR is mainly treated with vitreoretinal surgery. 5 After the development of severe PVR, such as grade C and grade D PVR, 6 conventional surgical techniques are not sufficient, necessitating more complex surgical techniques such as PVR membrane peeling and relaxing retinotomy and retinectomy. 7 In patients with traumatic RD who undergo relaxing retinotomy and retinectomy, the anatomic success rate can increase from 40% to 75%.8,9 Even if the anatomic success rate significantly increases following relaxing retinotomy and retinectomy surgery, the progression of PVR may continue, and retinal reattachment cannot be achieved in a significant proportion of patients. To reduce the development of PVR, mitomycin C (MMC) has been used successfully in patients with traumatic RD, and no MMC-related complications have been reported.10,11
In this study, we aimed to evaluate the role of the intraocular MMC application technique in severe traumatic RD with advanced PVR managed with relaxing retinotomy and retinectomy, in comparison with a control group of patients who did not undergo relaxing retinotomy and retinectomy surgery.
Methods
Patients
We retrospectively evaluated the medical records of consecutive patients with RD after open-globe injury who underwent vitreoretinal surgery with relaxing retinotomy and retinectomy between 2016 and 2022. All patients had relaxing retinotomy and retinectomy extending beyond 1 quadrant (90 degrees), had stage C1 or higher PVR, and had varying degrees of retinal shortening requiring relaxing retinotomy and retinectomy surgery. Patients who had undergone ocular surgery before trauma (except uncomplicated cataract surgery) and had a hereditary vitreoretinal disease, inadequate follow-up (<6 months), and incomplete data were excluded.
Patients were divided into 2 groups: those who received 20 µg/mL MMC via the MMC sandwich method (group 1) and those who did not (group 2). Forty-three eyes of 43 patients, including 24 receiving MMC (group 1) and 19 not receiving MMC (group 2), were included in the study. Written informed consent was obtained from all patients prior to each surgical procedure. The Ethics Committee of Gazi University approved the study protocol. The study was conducted in accordance with the principles of the Declaration of Helsinki.
The patients’ medical records were reviewed for age, sex, and medical history. All included patients underwent detailed ophthalmic examination to identify the cause of ocular injury, the best-corrected visual acuity (BCVA), time from trauma to first vitreoretinal surgery, preoperative intraocular pressure (IOP), lens status, the extent of RD, the extent of retinotomy/retinectomy, and the surgical interventions applied. Classification of injury zones was made according to the International Classification System for Ocular Trauma. 12 PVR was graded intraoperatively according to the Retina Society Classification of RD with PVR. 6
All patients underwent a comprehensive ophthalmologic examination at all visits. The patients were evaluated on day 1, weeks 1 and 2, month 1, and every 1 to 3 months during follow-up. Data from color fundus photographs, anterior segment photographs, macular optical coherence tomography (OCT) imaging, and retinal nerve fiber layer (RNFL) thickness scans (Spectralis) were documented at all visits except postoperative day 1.
Outcome Measures
Postoperative BCVA, IOP, retinal reattachment, final anatomic and visual outcomes, and postoperative complications were evaluated. Final anatomic success was defined as retinal attachment sustained for at least 6 months. Previously described potential intraocular MMC toxicity, such as intraocular inflammation, ciliary body atrophy and hypotony, optic atrophy, macular atrophy, and retinal vascular occlusion, were investigated postoperatively. 13 OCT and RNFL thickness scans were used to screen for possible retinal toxicity. IOP was used to screen for potential ciliary epithelial toxicity. Presence of hypotony was accepted if the IOP was lower than 6 mm Hg.
Surgical Technique
The MMC sandwich technique is used to prevent PVR and has been described previously. 11 A preclinical study has reported the use of the MMC sandwich technique at concentrations up to 20 µg/mL MMC without toxic effects on vital intraocular structures. 14 MMC was prepared in a vial using a serial dilution technique, in which 20 mg of MMC was diluted in 10 mL balanced salt solution, followed by 2 sequential 1:10 dilutions to obtain a final concentration of 20 µg/mL. This solution was used intraoperatively. All surgeries were performed by a consistent team of 2 senior vitreoretinal surgeons (I.G.G. and H.B.O.), with each surgeon performing approximately 50% of surgeries in both groups, using identical vitrectomy systems. The decision to use adjuvant MMC intraoperatively was based on preoperative clinical assessment. It was reserved for eyes with more extensive trauma and the highest risk for PVR, as supported by current evidence.10,11,15
After completion of the advanced vitreoretinal surgical procedures, such as pars plana vitrectomy, membrane peeling, and relaxing retinotomy and retinectomy, the retina was attached with fluid-air exchange. Perfluorocarbon liquid was injected until covering the posterior vital structures, including the optic disc and macula, to the border of relaxing retinotomy and retinectomy sites, chorioretinal wounds, and retinal breaks. Ciliary epithelium and other anterior segment structures were protected from MMC contact, with air filling the rest of the eye. A 20 μg/mL concentration of MMC solution (dyed with 0.05 cc of Brilliant Blue to make it visible) was then carefully injected above the perfluorocarbon liquid bubble until it covered the major vascular arcade, proliferating sites, and potential areas of PVR development, such as relaxing retinotomy and retinectomy sites and retinal tears (Figure 1). MMC was removed after 60 seconds. Finally, the remaining perfluorocarbon liquid was removed, and all eyes were filled with silicone oil after endolaser. The patients were followed up for at least 6 months.
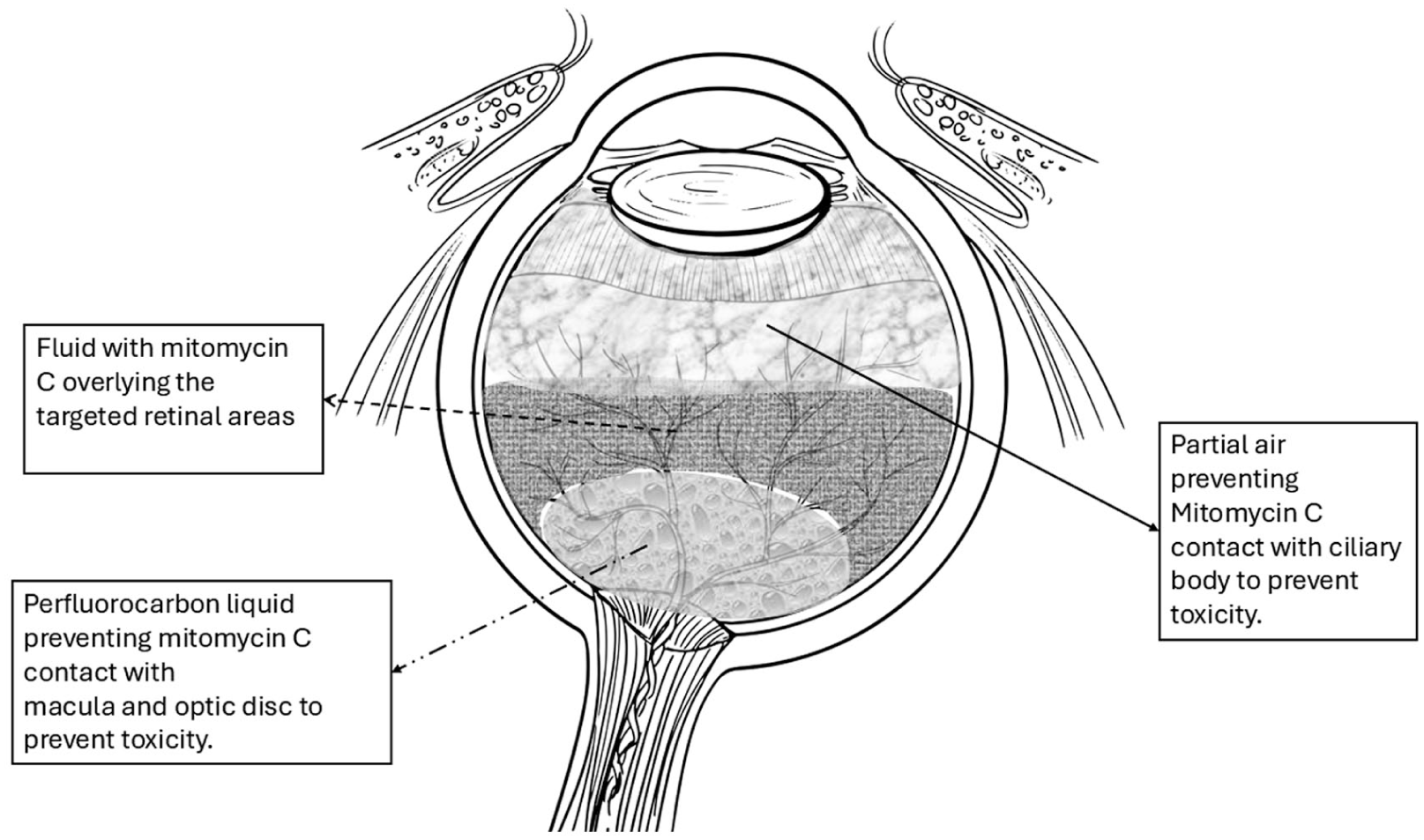
Schematic illustration demonstrating the intraoperative mitomycin C sandwich technique for adjuvant use during relaxing retinotomy and retinectomy in patients with retinal detachments secondary to trauma.
Statistical Analysis
The data were analyzed using SPSS version 22.0 (IBM SPSS Statistics). A significance level of P < .05 was set for all analyses. The significance of preoperative and postoperative changes within each group was tested using the Wilcoxon signed-rank test. Mann-Whitney U tests were used to assess the significance of group differences in baseline variables. For categorical variables, the significance of group differences was assessed using the χ2 test and Fisher exact test.
Results
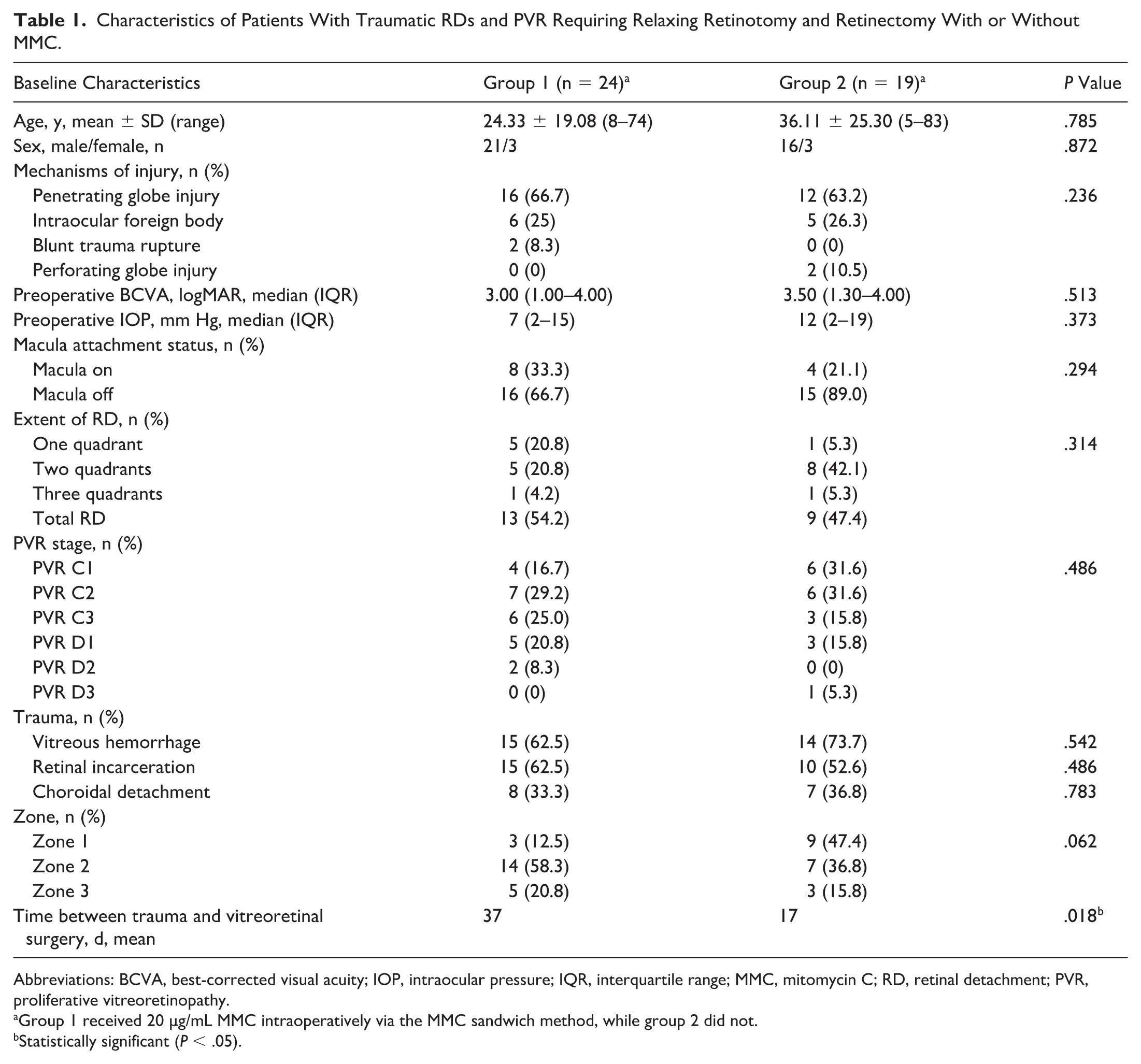
Forty-three eyes of 43 patients (37 male, 6 female) with traumatic RD and PVR requiring relaxing retinotomy and retinectomy extending 90 degrees or more were included in the study. The mean (±SD) follow-up time was 29.6 ± 10 months (range, 12–85 months). There were no statistically significant differences in preoperative characteristics, including sex, age, preoperative IOP, visual acuity, macula attachment status, RD extension, PVR severity, or trauma type (vitreous hemorrhage, retinal incarceration, or choroidal detachment). Baseline demographics, clinical characteristics, and mechanisms of injury are summarized in Table 1.
Characteristics of Patients With Traumatic RDs and PVR Requiring Relaxing Retinotomy and Retinectomy With or Without MMC.
Abbreviations: BCVA, best-corrected visual acuity; IOP, intraocular pressure; IQR, interquartile range; MMC, mitomycin C; RD, retinal detachment; PVR, proliferative vitreoretinopathy.
Group 1 received 20 µg/mL MMC intraoperatively via the MMC sandwich method, while group 2 did not.
Statistically significant (P < .05).
The mean interval between primary open-globe injury repair and vitreoretinal surgery was longer in group 1 than in group 2 (mean, 37 days vs 17 days), and this difference was statistically significant (P = .018). In group 1, the injuries were mostly in zones 2 (58.3%) and 3 (20.8%), whereas in group 2, they were mostly in zones 1 (47.4%) and 2 (36.8%), but this difference was not statistically significant (P = .062).
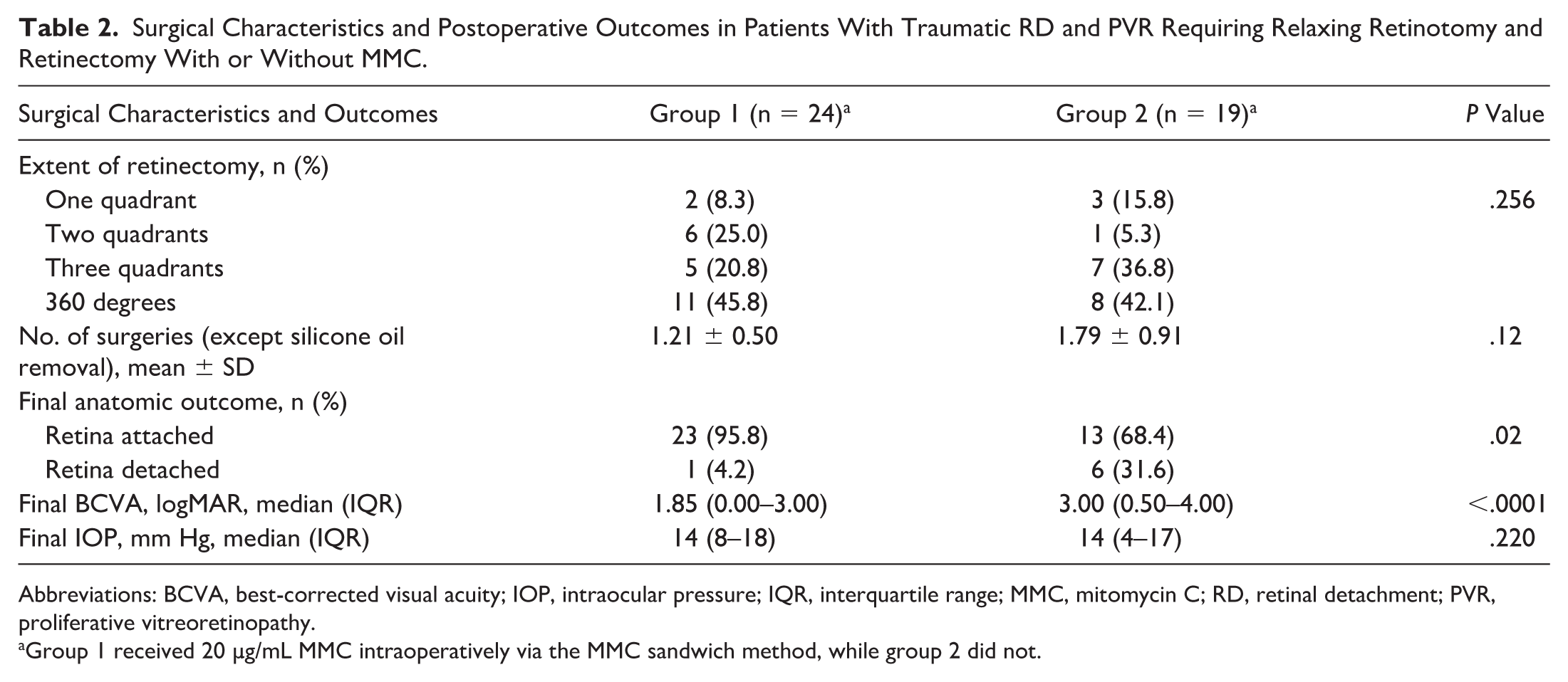
Surgical procedures, outcomes, and complications are listed in Table 2. In both groups, 90-degree to 360-degree relaxing retinotomy and retinectomy was performed with advanced vitreoretinal surgery techniques. There was no significant difference in the number of patients undergoing relaxing retinotomy and retinectomy according to degree (P = .256). Although the mean (±SD) number of operations (except for silicone removal) in group 1 (1.21 ± 0.50) was lower than in group 2 (1.79 ± 0.91), the difference was not statistically significant (P = .12).
Surgical Characteristics and Postoperative Outcomes in Patients With Traumatic RD and PVR Requiring Relaxing Retinotomy and Retinectomy With or Without MMC.
Abbreviations: BCVA, best-corrected visual acuity; IOP, intraocular pressure; IQR, interquartile range; MMC, mitomycin C; RD, retinal detachment; PVR, proliferative vitreoretinopathy.
Group 1 received 20 µg/mL MMC intraoperatively via the MMC sandwich method, while group 2 did not.
The postoperative BCVA in group 1 (median, 1.85 logMAR, interquartile range [IQR], 0.00–3.00) was higher than in group 2 (median, 3.00 logMAR, IQR, 0.50–4.00); this difference was statistically significant (P < .001). Corneal scarring affecting postoperative visual level occurred in 8 patients (33%) in group 1 and 6 patients (31%) in group 2. The final sustained retinal attachment rate was 95% in group 1 and 68% in group 2, which was a statistically significant difference (P = .022).
A total of 10 patients (41.7%) in group 1 and 8 patients (42.1%) in group 2 were followed up with silicone oil, with no statistically significant difference between the groups (P = .769). Following up with silicone oil for the risk of hypotony was done in 10 patients in group 1 and 8 patients in group 2. At the final examination, the mean IOP was 14 mm Hg (IQR 8–18) in group 1 and 14 mm Hg (IQR, 4–17) in group 2. One patient in group 1 and 2 patients in group 2 developed an IOP elevation, which was treated with topical treatment.
No postoperative toxicity related to intraoperative use of MMC was observed in this case series. There was no acute or accelerated macular or RNFL atrophy in either group, as determined by OCT/RNFL thickness measurements. No late retinal redetachments were observed after the 6-month follow-up threshold.
Conclusions
With modern devices and techniques, the anatomic success rate in patients with RDs has increased to 90% to 95%. 16 However, PVR development remains a significant cause of recurrent RD. 2 Trauma triggers inflammation and cell migration in retinal tissue, both of which are important risk factors for PVR development. 16 All pathophysiologic stimulants presumed to cause PVR development occur during the wound-healing process after trauma. Numerous experimental studies have demonstrated that posterior segment injuries disrupt the blood–retina barrier, trigger an inflammatory response, and lead to PVR development and RD.17,18 The development of PVR after trauma makes it difficult to manage and worsens anatomic and functional outcomes. 19 Various outcomes have been reported in the literature evaluating anatomic success rates in patients with RDs secondary to trauma. 9 The final anatomic success rate ranges between 27% and 90%. 20 Challenges in comparing the various results in the literature include difficulties in precisely categorizing patients with trauma-related RDs according to preoperative risk factors associated with trauma, such as vitreous hemorrhage, choroidal detachment, retinal incarceration, the extent of RD, and trauma zone, variability in surgical techniques applied during the operation, and the extent of retinectomy performed. In this study, preoperative PVR grade, relaxing retinotomy and retinectomy extension, and surgery timing were similar between groups to ensure similar conditions.
Over the years, several studies have been conducted to assess whether PVR development can be prevented using adjuvant therapies, including use of oral prednisolone, intravitreal triamcinolone, dexamethasone, low-molecular-weight heparin, 5-fluorouracil, daunorubicin, oral isotretinoin, and methotrexate. However, their effectiveness to be used routinely in clinical practice has yet to be sufficiently demonstrated. 21 MMC has been used for many years in procedures such as trabeculectomy, pterygium surgery, and photorefractive keratectomy. 22 It is known to reduce the primary fibrovascular proliferation response, which is the main process in the development of PVR. This effect of MMC has been demonstrated on retinal pigment epithelium cells in studies in vitro and in experimental PVR models. 23 Although the effect of MMC on cell proliferation has been known for a long time, its potential toxic effects on posterior segment structures has hindered its use in retinal surgeries until recent years. However, new technologies facilitating imaging and surgical techniques have prompted studies on their clinical use.10,11 Assi et al applied a soaked sponge from the sclerotomy area to the air-filled vitreous and the chorioretinal wound site. 10 In our application, we prevented MMC contact and toxicity on the posterior segment structures using perfluorocarbon liquid, while air was used to fill the rest of the eye to protect the anterior segment structures. This procedure is defined as the MMC sandwich technique. Use of this technique has been observed to successfully prevent PVR development in all eyes that received it. 11
In the present study, our findings suggest that MMC application may reduce the development of PVR and increase both anatomic and functional outcomes. There was no significant complication or MMC-related toxicity with the MMC sandwich technique. 16 In both groups, mean IOP measurements were improved compared with preoperative levels. There was no acute or accelerated macular or RNFL atrophy in either group, as assessed by OCT/RNFL thickness measurements. There was no worsening of corneal transparency in either group. Regarding ocular toxicity, given our long follow-up period (29.6 ± 10 months), we suggest that adjuvant MMC can be safely delivered using the MMC sandwich technique.
The absence of observed toxicity in our series deserves careful consideration. The relatively low concentration of MMC (20 µg/mL) used in our study may have contributed to the absence of observed toxicity. This low-dose approach was intentionally preferred to minimize potential cytotoxic effects while maintaining antifibrotic activity. Although no toxicity was observed in our series, this finding should be interpreted with caution. MMC is a potent cytotoxic agent, and its intraocular use carries a known risk of toxicity. Several factors may explain the absence of adverse events in our study, including controlled delivery using the sandwich technique, avoidance of direct contact with the posterior pole and ciliary body, and the relatively low dose used. Additionally, all procedures were performed in a controlled surgical setting by experienced vitreoretinal surgeons. Nevertheless, the possibility of subclinical or delayed toxicity cannot be excluded, and further studies are required to better define the safety profile of intraocular MMC.
Various outcomes have been reported in the literature on anatomic success rates with relaxing retinotomy and retinectomy in patients with RDs secondary to trauma. 9 The final anatomic success rates have ranged between 27% and 90%. 20 In a meta-analysis, the final sustained retinal attachment success rate was reported as 85% in patients undergoing retinectomy due to trauma. 9 The included studies in the meta-analysis reported a range of proportion of patients with RDs, ranging between 37% and 93%. In our study, all of our patients had RDs. Only 1 study reported a similar frequency of patients with RDs (93%), and the anatomic success rate was 62%. 24
The timing of vitrectomy in traumatic RDs is still controversial. Recent studies have shown that prolonged time between trauma and vitrectomy increases the risk of PVR development and recurrent detachment.20,25,26 Feng et al demonstrated that the risk of PVR development increased 18-fold after 14 days and reached 140-fold after 30 days. 26 In our study, the mean time interval between trauma and vitrectomy was 17 days in group 2 patients and 37 days in group 1 patients. As a tertiary referral center, our institution received the majority of cases as transfers from secondary hospitals, resulting in longer intervals between primary repair and definitive vitreoretinal surgery. Upon arrival, all patients underwent surgery at the earliest feasible time.
Relaxing retinotomy and retinectomy techniques for treating complex RD associated with PVR have been described. 27 However, they are preferred to treat only complex PVR-associated RD cases due to the potential for inducing PVR and the risk of hypotony. 28 The extent of the RD is one of the essential preoperative indicators for severe PVR and recurrent detachment. 26 The extent of RD was similar between the 2 groups in our study, with more than half of the patients having total RD. The presence of PVR before vitrectomy is a significant risk factor for poor anatomic and functional outcomes after trauma. 19 Vitreous hemorrhage, choroidal detachment, and retinal incarceration have been shown to correlate with the development of PVR and recurrent RD after surgery. 26 Considering all these factors, the patients included in this study can be considered to have been at high risk for PVR development and recurrent RD. In our study cohort, a high anatomic and functional success rate was achieved with adjuvant MMC use.
It is known that the risk of postoperative hypotony increases with the extent of relaxing retinotomy and retinectomy. 28 This measure was determined intraoperatively to avoid both insufficient and excessive retinal excision, in line with established recommendations.27,28 In our study, there was no newly developed hypotony after the surgery in either group. Among patients in both groups with silicone oil in the eye, all had preexisting hypotony.
The limitations of our study include its retrospective design and relatively small sample size. Due to the retrospective nature of the study, the exact number of patients excluded because of insufficient follow-up could not be reliably determined, which may introduce a potential selection bias. Although some intergroup differences reached statistical significance, these findings should be interpreted with caution given the limited sample size and retrospective design. A strength of our study is that all data were obtained from a single academic institution, allowing for control of intersurgeon variability, along with a relatively long follow-up period (29.6 ± 10 months).
In conclusion, the MMC sandwich technique can be safely used in complex traumatic RDs, with encouraging anatomic and functional outcomes. These findings warrant confirmation in larger prospective studies.
Footnotes
Author Note
Presented at the Turkish Ophthalmological Association 56th National Congress, Antalya, Turkey, in November 2022.
Ethical Considerations
This study was approved by the Ethics Commission of Gazi University (approval no. 2022-1151) and adhered to the principles of the Declaration of Helsinki.
Consent to Participate
Written informed consent to participate in the study was obtained from all patients.
Author Contributions
All authors attested that they meet the current ICMJE Criteria for Authorship.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.