
Abstract
Keywords
Introduction
Macular pathology associated with high myopia is primarily attributed to posterior staphyloma, as opposed to elongated axial length (globular scleral expansion) or idiopathic macular holes (MHs) that result from tangential traction. 1 Myopic maculopathy can be classified as degenerative (involving changes in the retinal pigment epithelium–choroid complex), tractional, or of mixed pathology. Myopic traction maculopathy, which is the tractional type that affects the inner retinal structures, represents the stretched macula (maculoschisis) that is caused by forces induced by a posteriorly elongated sclera. A variable pathology may develop from the interaction between the elongated retinal layers and the firm inner vitreoretinal complex involving the adherence of the internal limiting membrane (ILM), retinal vessels, and posterior hyaloid.2,3
Previous research, as well as our case series, has demonstrated that patients with myopic traction maculopathy can be divided into 4 groups based on the presence of schisis components or significant inner retinal traction, such as epiretinal membrane (ERM) or vitreomacular traction (VMT) (Table 1). 4 Macular buckling surgery is currently recommended for patients in myopic traction maculopathy group 1 (individuals with staphyloma-related foveoschisis but no significant tractional membranes) 5 once the stage of macular detachment is reached (Table 2).2,6–8
Myopic Traction Maculopathy Classification Based on the Direction of the Tractional Force.
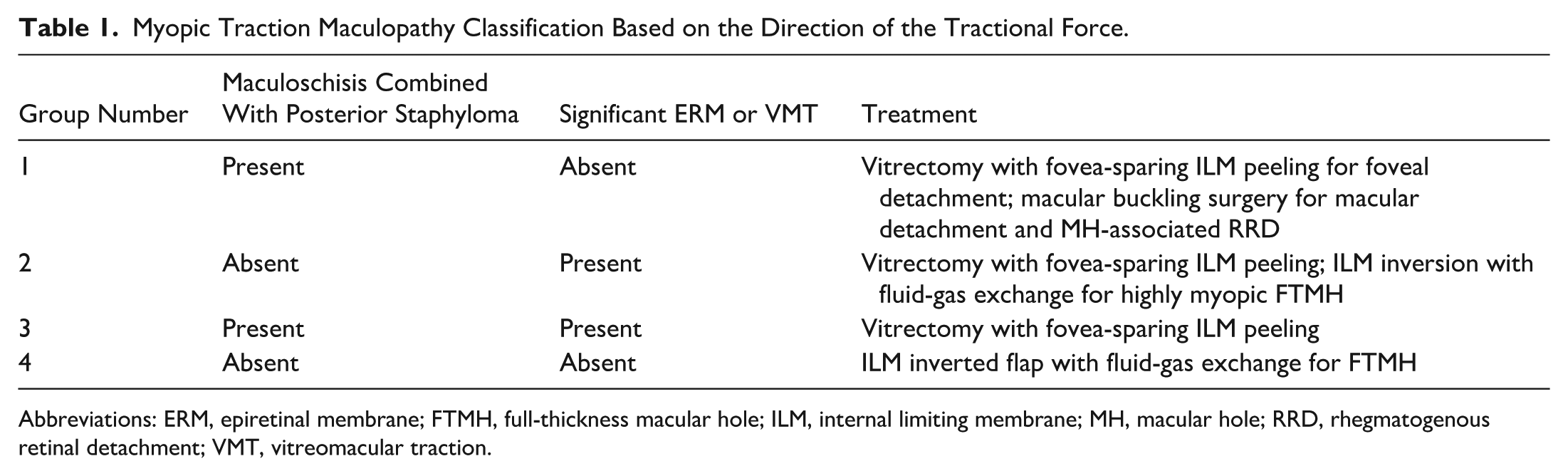
Abbreviations: ERM, epiretinal membrane; FTMH, full-thickness macular hole; ILM, internal limiting membrane; MH, macular hole; RRD, rhegmatogenous retinal detachment; VMT, vitreomacular traction.
Subdivision of Myopic Traction Maculopathy Group 1 or Patients Presenting With Staphyloma-Driven Maculoschisis Without Notable Tractional Membranes, With Treatment Categorized by Myopic Traction Maculopathy Stage.
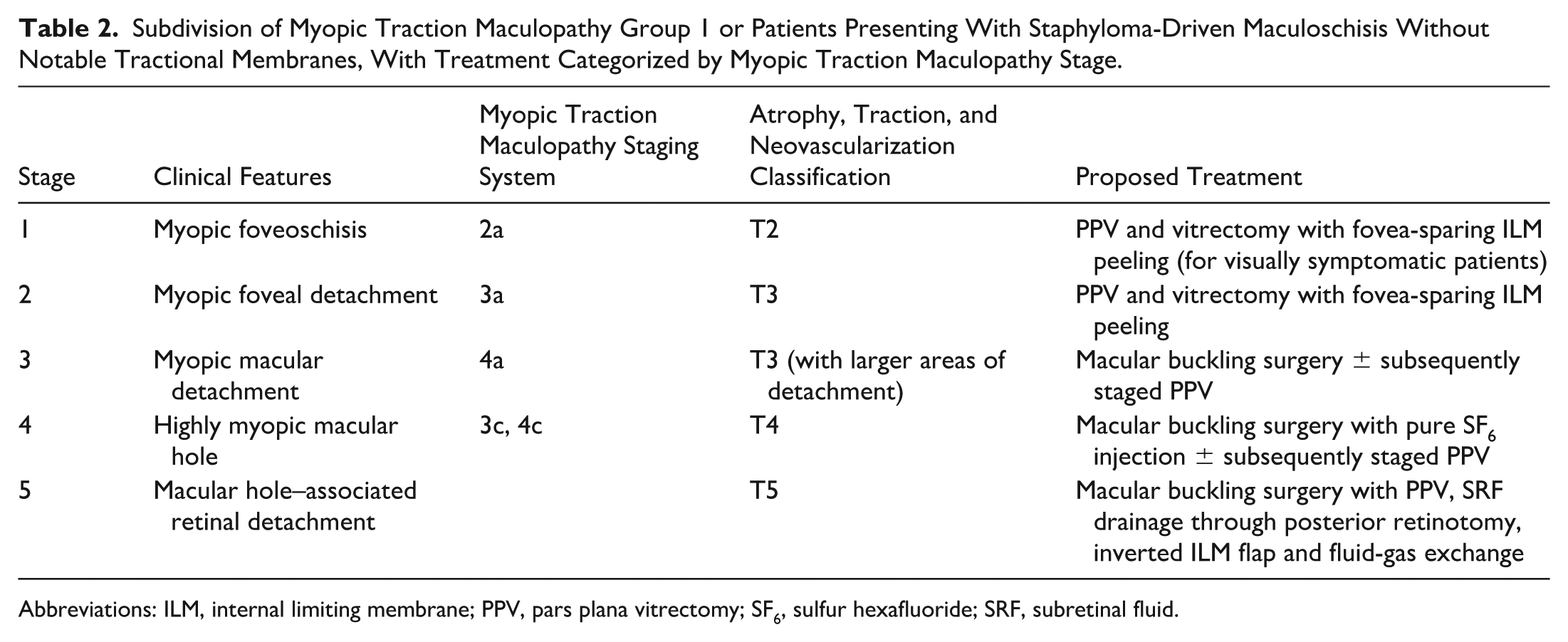
Abbreviations: ILM, internal limiting membrane; PPV, pars plana vitrectomy; SF6, sulfur hexafluoride; SRF, subretinal fluid.
Vitrectomy is the preferred method when significant ERM or VMT is present, particularly with attached posterior hyaloid (group 2 or 3).9,10 The selection of a different approach for each group is determined by the respective mechanism underlying myopic traction maculopathy disease. For instance, macular buckling surgery is not recommended for patients in group 4 who have neither staphyloma nor significant epiretinal traction, because axial elongation may present pathologies that could emerge from evenly globular scleral expansion.
Furthermore, the status of patients in group 1 can be divided into 5 stages (Table 2). The first stage is foveoschisis, which responds well to fovea-sparing ILM peeling. However, most patients do not have visual symptoms, and ILM peeling in highly myopic eyes can be complex due to an abnormally thin retina and reduced visualization caused by chorioretinal atrophy. Hence, these patients are monitored until foveal detachment occurs. This is the optimal stage for performing pars plana vitrectomy (PPV) because although patients experience visual symptoms, they still respond effectively following PPV. 11
Once the detachment progresses to the entire macula, ILM peeling alone is insufficient to fully address the pathology. This is partly due to the breakdown of Müller cells, which contributes to the disconnection of the inner and outer retinal layers (Supplemental Figure S1). Additionally, to achieve a sufficiently relaxed macula, broad ILM peeling, which covers the detached area and the surrounding unaffected areas, is required, but this may be challenging in highly myopic eyes. Thus, patients with macular detachment who belong to myopic traction maculopathy group 1 may present with an inadequate response post–ILM peeling, as the inner retina has no supporting structures against the external limiting membrane.12,16
An important goal when treating patients with myopic traction maculopathy is to prevent the transition from tractional retinal detachment (TRD; maculoschisis with or without macular detachment) to rhegmatogenous RD (RRD; full-thickness MH or MH-associated RD), which requires a tamponade agent. Although viscoelastic-assisted grafting may be considered, restoration of photoreceptors by native foveal tissues or gliosis remains unclear, and no predictive factors have been identified. Likewise, superior anatomic outcomes for macular detachment MH-RRD were noted following macular buckling surgery, either alone or in combination with PPV when compared with PPV alone; however, the incidence of complications is lower in surgeries for macular buckling only.13–17
Some of the previous techniques, based on the principle of a temporal approach without inferior oblique muscle suspension, require exposure of the deep posterior aspect of the temporal sclera, with the rigid material or a large handle close to the lateral rectus or perioperative lateral rectus disinsertion. This may result in a long operative time, increased surgical complexity, and postoperative strabismus.12–18 More recently, a simplified method, also based on a temporal approach and utilizing a newly developed macular buckle (AJL Ophthalmic), has the potential to reduce operative time while maintaining favorable outcomes.19,20
Herein, we describe a novel technique for macular buckling surgery that aligns with the natural physiology of extraocular muscles by adjusting the buckling effects through a vertical approach. This method increases the likelihood of placing the buckle material close to the staphyloma without exposing the deep posterior sclera. Notably, this procedure uses silicone material, which is modified into a T-shaped buckle that is routinely used during RD repair. We also report the 1-year anatomic and visual outcomes following the use of this technique.
Methods
The proposed macular buckle model is an unlabeled use of a commercial product. It is not yet approved by the US Food and Drug Administration for any purpose. A retrospective case series that included patients in myopic traction maculopathy group 1 who underwent macular buckling surgery for macular detachment, MH, or MH-RRD was conducted at Vajira Hospital, Thailand, between September 2022 and June 2025. The surgical outcomes between macular buckling surgery and vitrectomy were not compared as each procedure was performed at different stages of myopic traction maculopathy (Table 2). Patients with myopic traction maculopathy and macular atrophy involving the fovea and those with subfoveal macular neovascularization scar tissues were excluded from the study.
Patients in myopic traction maculopathy group 1 who exhibited macular detachment or further progression were candidates for macular buckling surgery (Tables 1 and 2). In particular, myopic traction maculopathy group 1 refers to posterior staphyloma, diagnosed by funduscopy, optical coherence tomography (OCT) scans, or B-scan ultrasonography, combined with the manifestation of myopic traction maculopathy, specifically maculoschisis or TRD, which is primarily caused by anterior-posterior traction originating from the posteriorly elongated sclera. In this regard, patients with prominent ERM or VMT were excluded, due to the potential for internally derived tractional forces to exhibit multidirectional vectors. To construct the macular buckle element (Figure 1 and Supplemental Figure S2), the 41 band or the T-arms were matched with a 15-mm segment of a wide-grooved 287 tire (3.5-mm tunnel width), while the 240 band or the T-leg was inserted into the pocket made inside the 287 sections.
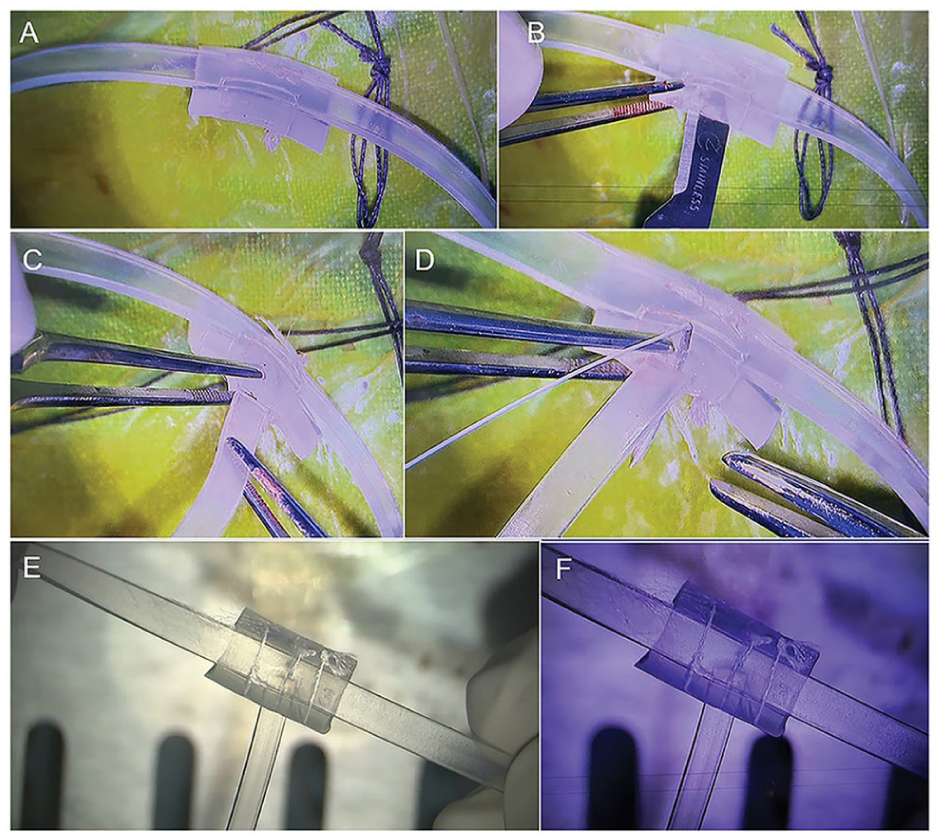
Construction of the 3-armed macular buckling segment. (A) The 41 band or the T-arms are matched with a 15-mm segment of a WG 287 tire (wide groove, 3.5-mm tunnel width), while (B and C) the 240 band or the T-leg is inserted into the pocket situated inside the buckling segment. (D and E) All silicone pieces were sutured together using 5-0 Surgidac (Medtronic) sutures. (F) A magnified image shows that the T-leg should shift in the superotemporal direction.
All silicone material (FCI S.A.S.) was stitched together using a 5-0 Surgidac (Ethicon, Johnson & Johnson) or Ethibond suture (Ethicon). The primary purpose of the T-arms was to tighten the WG-287 segment (indentation of posterior staphyloma) while the T-leg, using a thinner 240 band only, stabilized the material’s position, preventing macular buckle segment displacement toward the optic nerve head and maintaining proper angulation and alignment of the segment. We recommend slightly shifting the T-leg superotemporally to prevent its direct contact with the lateral rectus postoperatively.
The technique proceeded as follows (Figure 2; https://www.aao.org/education/clinical-video/macular-buckling-surgery-using-modified-silicone-m): The inferotemporal quadrant was exposed, and the 4 rectus muscles were suspended; the inferior oblique muscle was then identified. The superotemporal sclera was then exposed, followed by insertion of the inferior vertical T-arm beneath the lateral rectus, inferior oblique, and inferior rectus (Figure 2A and Supplemental Figure S2). The superior T-arm was then positioned below the superior rectus muscle and inserted through a 5-mm section of the 270 Waske silicone sleeve.
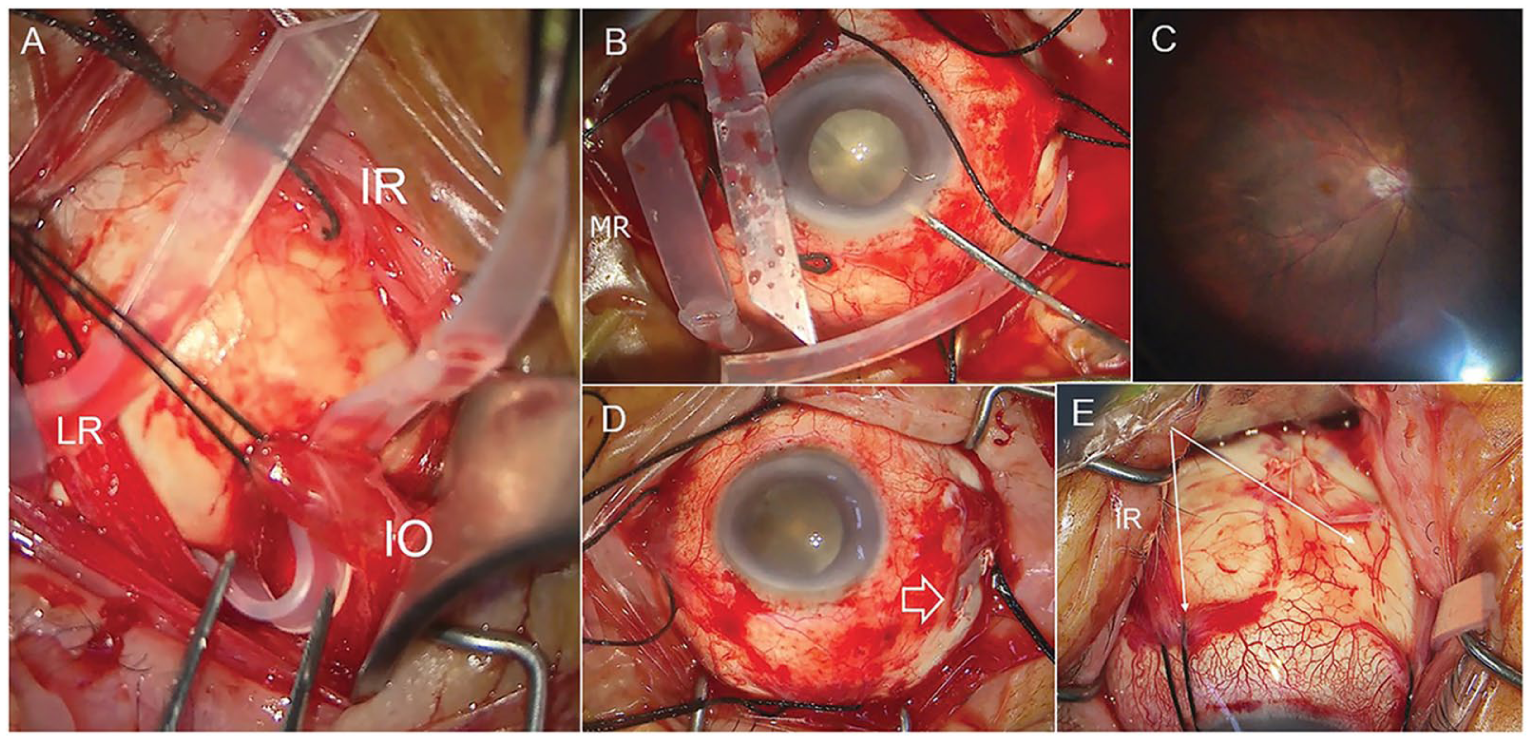
An illustration of surgical techniques. (A) After hanging the 4 rectus muscles and the inferior oblique (IO) muscle, the inferior vertical T-arm is inserted beneath the lateral rectus (LR), inferior oblique, and inferior rectus (IR). (B) Anterior chamber paracentesis was performed through a side port to assist with the posterior migration of the macular buckling segment. (C) Under chandelier-assisted visualization, the macular buckle element shifted toward the fovea, while the assistant slowly pulled the vertical 41 bands in the opposite direction. (D) The horizontal 240 band was sutured to the sclera slightly above the lateral rectus insertion (arrow), while (E) the vertical 41 bands were sutured to the sclera 45 degrees to the vertical rectus muscles. Abbreviation: MR, medial rectus.
The sleeve was sutured to the superotemporal sclera 45 degrees to the vertical rectus muscles. This will serve as an anchoring point for the 41 band during the buckle height adjustment. Note that it is essential to separate the orbital fat surrounding the inferior oblique muscle to facilitate the adequate advancement of the buckle. Although using an indirect ophthalmoscope is less invasive, a 25-gauge chandelier was used for intraoperative visualization to maintain consistency. To assist in the posterior migration of the 287-segment, anterior chamber paracentesis was performed through a 1-mm corneal side port (Figure 2B). Following the insertion of the macular buckle segment beneath the lateral rectus muscle, the macular buckle element shifted from the temporal areas toward the fovea as the assistant gently pulled or tucked the vertical 41 bands temporally (Figure 2C). After achieving adequate indentation and buckling’s position, 1 vertical 41 band (preferably the lower band) was fixed and sutured to the sleeve segment fixated to the sclera. The horizontal 240 band was then sutured to the superotemporal sclera slightly above the lateral rectus (Figure 2D). The buckle’s position was re-checked before fixing another vertical band to the sclera.
Postoperative complications and standard ocular parameters, including visual acuity (VA), refraction, axial length based on the IOLMaster 700 (Carl Zeiss Meditec), and the choroidal vascularity index based on swept-source OCT angiography (PLEX Elite 9000, Carl Zeiss Meditec) were collected at baseline (preoperative) and at 1, 3, 6, and 12 months postoperatively. Outcomes of patients who underwent macular buckling were not compared with those who underwent vitrectomy due to differences in preoperative disease stages. The paired t-test was used to compare the preoperative and postoperative outcomes, which included logMAR best-corrected VA (BCVA), axial length, intraocular pressure (IOP), and choroidal vascularity index. Statistical tools were not employed to address missing time points. A 2-sided P value <.05 indicated statistical significance. Mean values are ± SD. All calculations were performed using Stata version 15.0 (StataCorp).
Results
Overall, 22 patients (22 eyes) were included in the study. The average age was 67.2 ± 10.1 years, and 15 patients (68.1%) were women. When all eyes were included, the logMAR BCVA improved from a preoperative value of 1.34 ± 0.3 (20/400) to 0.9 ± 0.35 (20/160) after the 12-month follow-up (P = .05). In 15 patients who underwent macular buckling surgery alone for macular detachment, the mean postoperative logMAR BCVA improved from 1.22 ± 0.50 (20/320–1) to 0.82 ± 0.40 (20/125−1) and 0.67 ± 0.42 (20/100+1) at 6 and 12 months (P = .07, P = .03), respectively. The median duration for the first observation of foveal reattachment was 14 weeks. Additionally, the mean axial length decreased from 29.9 ± 2.4 mm preoperatively to 28.2 ± 3.09 mm at 6 months and 28.4 ± 2.78 mm at 12 months (P = 0.13) postoperatively.
At 6 months postoperatively, the median spherical equivalent changes were 3.25 diopters in 14 eyes (63.6%), with directly indented foveas and 1.75 diopters in 8 eyes (36.3%) with parafoveal indentation, where the buckle segment did not directly compress the fovea. Due to a limited number of samples, a valid linear regression analysis for comparison between these 2 cohorts could not be performed.
Among 7 patients who had myopic traction maculopathy progression to MH and beyond, 1 patient underwent macular buckling surgery alone for highly myopic-MH with an adherent operculum (Figure 3), resulting in MH closure with retinal reattachment at 14 weeks postoperatively. At 3 and 7 weeks postoperatively, an initial gliosis bonding the hole edges, followed by separation of the posterior hyaloid (operculum), was noted (Figure 3D). Two patients with MH and early-stage RRD underwent macular buckling surgery followed by administration of 0.7 mL of pure sulfur hexafluoride (SF6) and anterior chamber paracentesis as staged procedures within 48 to 72 hours post–macular buckling surgery (Figure 4). Four patients underwent macular buckling surgery combined with PPV, fluid-gas exchange, and ILM inversion (for MH with total RRD). Three patients (13.6%) had inadequate buckling effects, in which the indentation did not reach the staphyloma border; 2 of them required subsequent PPV due to postoperative MH formation.
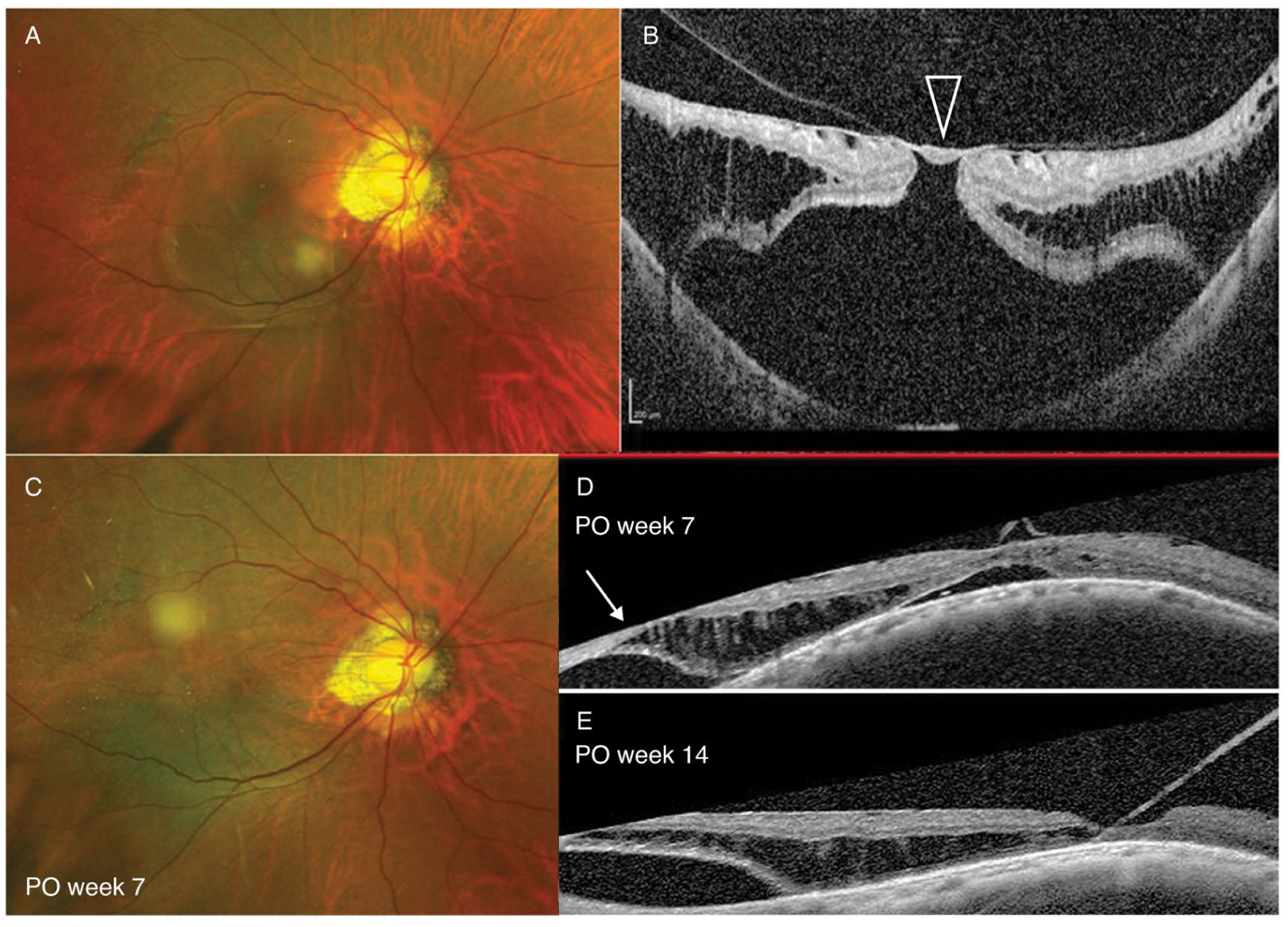
(A and B) Macular buckling surgery in a 52-year-old man with myopic macular detachment combined with a full-thickness macular hole and adherent foveal operculum (visual acuity, counting fingers). (B) Despite the presence of an epiretinal membrane, the potential consequences of removing the posterior hyaloid and foveal operculum (arrowhead) during vitrectomy include unbridging the hole edges. (C and D) Consequently, the patient underwent macular buckling surgery alone and achieved hole closure with parafoveal attachment (best-corrected visual acuity, 20/125) and a decrease in the schisis components (arrows) within the first 2 months after surgery. (E) Foveal reattachment was observed at week 14 postoperatively. Abbreviation: PO, postoperative.
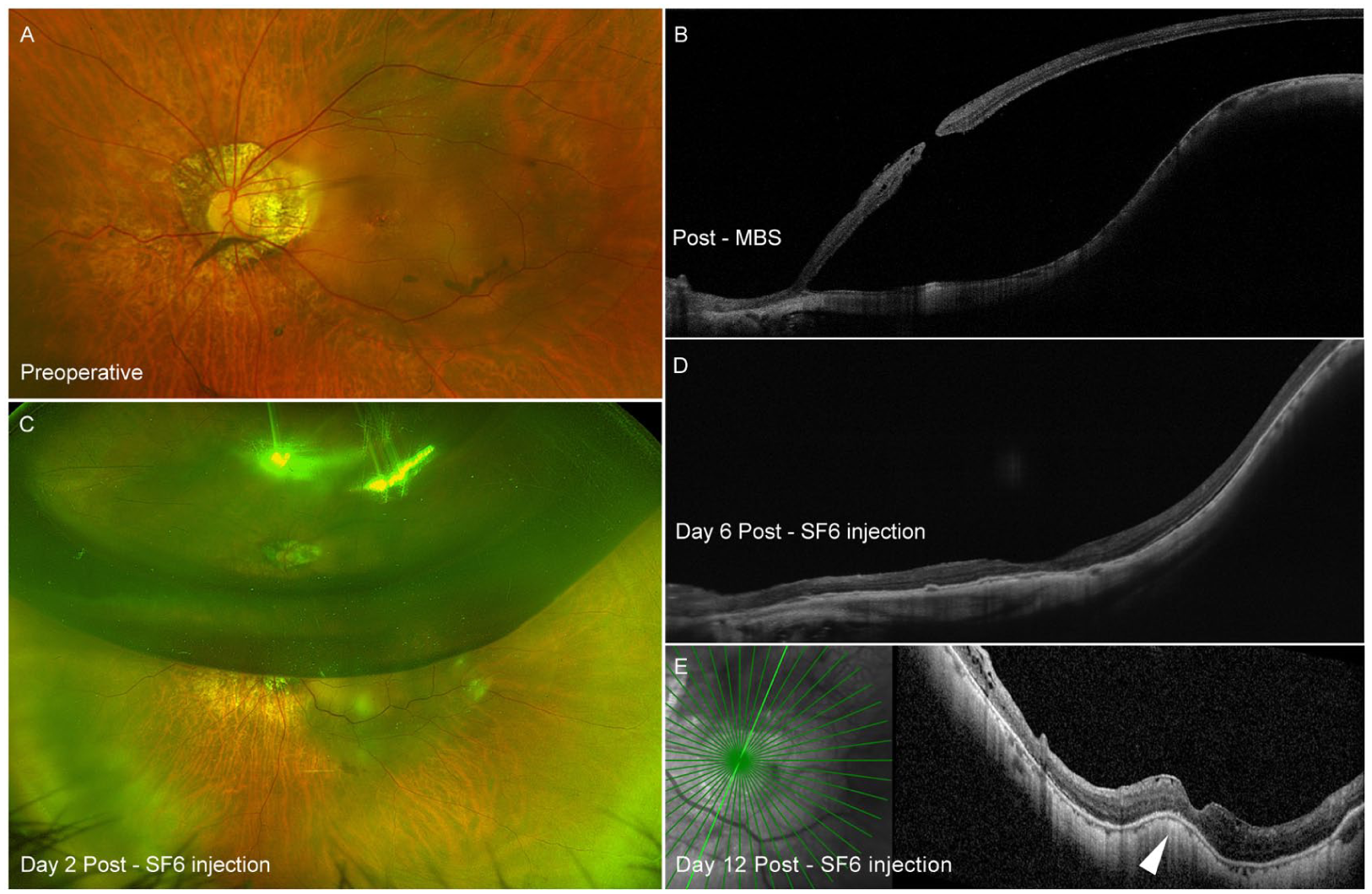
A 2-stage procedure consisting of macular buckling surgery (MBS) followed by intravitreal injection of a pure gas bubble. (A) Preoperative images show a macular hole associated with retinal detachment. (B) Wide field optical coherence tomography image at postoperative day 3 after macular buckling surgery reveals the buckling effect at the temporal aspect of the posterior staphyloma, with persistent retinal detachment. (C) Pure sulfur hexafluoride (SF6) was administered on postoperative day 2, (D) resulting in a reattached macula with subsequent initial gliosis and hole closure starting the sixth day following gas injection. (E) A small redundancy of the sclera under the fovea was observed at 2 weeks post–buckling surgery.
Despite a lack of evidence for the association between IOP and choroidal perfusion, IOP was maintained at less than 14 mm Hg using topical brinzolamide/timolol. Notably, none of the patients developed macular atrophy, and the choroidal vascularity index remained unchanged from the third to the 12th month in all patients (P = .70). The mean operative time in 16 patients who underwent macular buckling surgery for macular detachment was 104.5 ± 31.2 minutes (range, 52-138). The mean operating room time in the first 10 and last 6 patients was 115.4 ± 35.5 minutes and 86 ± 28.2 minutes, respectively.
Although all patients had final retinal reattachment, MH closure failed in 3 individuals (13.6%), all of whom presented with postoperative diameters greater than 1000 µm following the combination of macular buckling surgery and PPV for MH-associated RRD. Accordingly, 17 cases (86.3%) achieved complete anatomic success, characterized by both retina reattachment and MH closure.
The most common complication was self-limited subretinal hemorrhage (3 cases) in the temporal areas, all of which occurred in those who underwent surgery combined with vitrectomy. One patient had a partial extrusion of the buckle material (T-leg) that was subsequently trimmed. Worth 4 dot tests did not reveal diplopia in 4 patients, with a VA ranging from 20/50 to 20/63.
Conclusions
According to our results, the foveal reattachment and MH closure seen after macular buckling surgery without vitrectomy for releasing tangential tractions may support a significant role of posteriorly elongated sclera in the pathophysiology of myopic traction maculopathy. Correspondingly, we observed that reducing the posterior staphyloma volume without direct compression beneath the fovea could restore retinal architecture in patients with macular detachment, beginning with the schisis components, followed by absorption of submacular fluid. Nevertheless, the relationship is not definitively established due to the lack of a control group, particularly 1 in which vitrectomy is combined with ILM peeling.
Similar outcomes were observed in 2 patients who reached the rhegmatogenous stage (involving MH and ERM with early RD) and later achieved retinal reattachment and closed MH after treatment with macular buckling surgery, followed by 0.6 mL of pure SF6 (Figure 4. The initial success in avoiding vitrectomy and foveal indentation suggests that these staged approaches should be further evaluated in studies with a larger cohort of patients with myopic traction maculopathy and early-stage MH RRD.
Regarding the anatomic fundamentals of extraocular muscles, the main concern with techniques that introduce buckles via a temporal approach is the direct interference with the force of the inferior oblique muscle and the surrounding orbital fat, especially when the material is placed at the most posterior aspect of the sclera. Ideally, macular indentation should be performed and adjusted through a vertical approach, wherein the inferior oblique and surrounding soft tissues are separated from the buckle element to facilitate its posterior placement. The T-shaped model allows for the implementation of these concepts, with vertical T-arms for indenting and the horizontal T-leg for angulating the buckle’s plane and stabilizing the material’s position.
Nonetheless, although the 3-armed macular buckle model is frequently referenced in the literature, the designs vary across studies and are no longer commercially available. 21 Thus, macular buckle surgery mostly relies on materials sourced from fields outside of ophthalmology. These options include a silicone capsule, a scleral graft, a titanium plate connected to sponge materials, and a titanium macular buckle with a concave shape designed to lessen the effects on choroidal circulation.14,22–25
Considering surgical techniques, despite several studies reporting favorable results following combined vitrectomy with macular buckling surgery, we propose that the 2 procedures be performed separately to lower the risk of intraoperative hypotony, choroidal detachment, and development of postoperative MH. 26 Of the procedures described, the most crucial step is the final adjustment of the buckle’s height and position, wherein the IOP is normalized to achieve an optimal buckling effect. We recommend adjusting the suture before performing the final fixation of the vertical T-arm.
Implementing intraoperative OCT into the procedures might improve their precision. Complete separation of orbital fat from the inferior oblique during initial muscle suspension would facilitate buckle advancement. Before the end of surgery, the buckle element should be advanced as posteriorly as needed without resulting in IOP elevation. This is imperative to prevent postoperative ocular hypertension and potential disruption of macular choroid circulation, though the fovea is not directly supported. After completion of the first 10 macular buckling surgeries for macular detachment, the average procedure duration dropped by approximately 25%, from 115 to 86 minutes. This may indicate learning-curve improvements in specific steps, such as buckle creation, inferior oblique suspension, eye pressure adjustment, and buckle height adjustment before final band fixation to the sclera.
Regarding changes in scleral contour, potential distortion in infrared-guided imaging can lead to measurement variations for patients with deep preoperative staphyloma or dome-shaped macula postsurgery. Our findings are similar to those of others in which a gradual reduction in the indented effect took place over the first postoperative year, then typically remained stable afterwards. 12 The mean axial length of our cohort decreased from 29.9 mm preoperatively to 28.4 mm at 12 months. The shortened axial length corresponded to the spherical equivalent changes of 3.25 diopters in 14 eyes (63.6%) with directly indented foveas.
Although statistical significance was not achieved (P = .13), the average axial length decrease of nearly 1.5 mm was relatively modest and was similar to results seen when using soft tissue substitutes such as cross-linked sclera (1.65-mm reduction) 27 or the single-armed macular buckle device (1.5-mm axial length reduction). 20 However, these effects are shorter than those of the other studies using the 3-armed macular buckle model, resulting in axial length shortening ranging from 2.3 mm (28.5-26.2 mm) in the Devin-Morren model 28 and 3.1 mm (29.15-26.08 mm) 12 to a maximum of 4.9 mm (33.98-29.09 mm). 13 The reduced surgical indentation likely contributed to our methodology; instead of using a rigid temporal handle to exert pressure toward the macula as is typically seen, we pull the 240 band (T-leg) in the opposite (temporal) direction for buckle angulation.
Macular buckling surgery may be considered an alternative approach for patients with schisis-related myopic traction maculopathy with macular detachment and beyond, as this externally approached surgery directly addresses the primary pathophysiology, decreasing the risk of postoperative MH formation or recurrence of RD associated with a progressive staphyloma. Although a straightforward reversal of pathophysiology in any stage of myopic traction maculopathy requires posterior scleral reinforcement, vitrectomy is still preferred as an alternative for early-stage myopic traction maculopathy due to comparable outcomes, inconsistent macular buckling procedures across publications, and the unavailability of macular buckle devices.4,6,7,11
The benefits of macular buckling surgery are theoretically more obvious in patients with an attached posterior hyaloid, as the outermost vitreous complex could act as a scaffold for foveal bridging after macular buckling surgery. 23 Separating the inner retinal complex from the posterior hyaloid from vitrectomy may result in the development of postoperative MH. Regarding the clinical application of macular buckling surgery, if the buckling effects become too convex, the silicone bands can be loosened or removed under local anesthesia. In cases of inadequate buckling effects, macular buckling surgery does not compromise the outcomes of a subsequent vitrectomy; instead, it may facilitate easier ILM peeling due to the shortened axial length and improved visibility of the partially compressed retinal pigment epithelium (Supplemental Figure S3).
The ILM inversion procedures in a patient who received macular buckling surgery 3 months previously were less challenging due to the reduced axial length and the absence of tigroid appearance over the former staphyloma, which improved the surgeon’s visibility. In contrast, persistent MH or retinal redetachment requiring long-term silicone oil tamponade likely occurs following failed vitrectomy in patients with advanced-stage myopic traction maculopathy. Additionally, a study reported that PPV could accelerate the progression of myopic traction maculopathy, with the mean interval for progression to a different stage being shortened from 87 months to 31 months. 29
In clinical practice, given the comparable anatomic and functional results across different macular buckle models, it is recommended to adopt the simplest technique while balancing with device accessibility, potential complications, reproducibility in their operative settings, and management trends among the local retina community. For instance, compared with a technique using a single-armed model, our technique may require longer operative time due to more muscle suspension, including superior rectus, inferior rectus, and inferior oblique, and scleral suturing to anchor the vertical T-arms; however, positioning adjustment through vertical segment at the end of the operation may be simpler, as the T-arms are larger and more rigid than the T-leg, leading to neither slippage nor decentration in our cohort.
Additionally, our technique uses buckle elements routinely intended for encircling surgery, making the surgery readily available and universal for retina surgeons. Regarding 2 patients (9.1%) who showed no indenting effects within the staphyloma area and required subsequent vitrectomy, their myopic traction maculopathy progression to MH may occur naturally because macular buckling surgery provided no therapeutic effect. We speculate that ocular hypotony during the final buckle positioning might result in buckle displacement once the pressure normalizes and scleral expansion occurs.
Restrictive diplopia and metamorphopsia are 2 leading complications following macular buckling surgery; both tend to gradually resolve after 3 months to 2 years of follow-up.12,14 Although this study did not provide ocular movement range data for the initial 6 months, 4 individuals with BCVA between 20/50 and 20/63 showed no diplopia on Worth 4 dot tests at their 1-year follow-up. Regarding perioperative complications, self-limited subretinal hemorrhage at the temporal areas, noted in 3 patients during an initial phase of the study, might occur during scleral suturing due to insufficient scleral rigidity in their surgery combined with vitrectomy; slight leakage through retained cannulas could be aggravated during the suturing process with muscle traction. We recommend using backhand insertion to fix the temporal 240 band to ease needle handling and minimize the risk of full-thickness scleral sutures.
One patient (4.5%) experienced a partial extrusion of the temporal 240 band. Although this did not influence postoperative macular morphology, the material was subsequently trimmed to avoid any prospective infection risks. Earlier studies and our findings indicate that buckle extrusion, with incidences ranging from 2.5% to 7.5%, generally involves only 1 arm and is unrelated to infections or displaced macular indentation.14,20
To discuss postoperative choroidal perfusion, we applied the choroidal vascularity index, the ratio of the luminal area of the choroidal vessels, to the total choroid to represent a quantitative measurement of choriocapillaris dysfunction. Previous studies indicated that choroidal circulation in highly myopic eyes are more vulnerable to IOP elevation (choroidal vascularity index decreases by 2 at every increment of 1 mm Hg) than moderately myopic or emmetropic eyes.30,31 Although no large studies have explored a relationship between choroidal vascularity index parameter and IOP in patients with myopic traction maculopathy, an inverse correlation between IOP and choroidal blood flow has been established by several studies investigating different indicators. The majority of choroidal flow metrics significantly increase as IOP reduces from an interval of 22 to 30 mm Hg into the lower teens, irrespective of the therapeutic intervention applied (pharmacotherapy, trabeculectomy, or ocular massage) or the cohort studied (healthy controls or glaucomatous patients).31,32 Considering that IOP typically rose to an average of approximately 22 mm Hg following macular buckling surgery, 12 maintaining a low IOP, preferably 14 mm Hg or lower, may be justified by its potential to preserve choroidal circulation.
Unlike the established connection between choroidal vascularity index and the expansion rates of geographic atrophy in age-related macular degeneration, 33 there is no definitive evidence confirming that a low choroidal vascularity index serves as a predictor for pachyatrophy progression in myopic traction maculopathy. Previous findings indirectly suggest that choriocapillaris perfusion defects may contribute to the pathogenesis of myopic macular atrophy. Specifically, lower choroidal vascularity index values were associated with patients with maculoschisis-related myopic traction maculopathy when compared with highly myopic eyes without myopic traction maculopathy. 34 Moreover, a 2.3 times greater deficit in choriocapillaris perfusion was identified in highly myopic patients with eccentric macular atrophy and good visual acuity, relative to the healthy controls. 35
We did not observe changes in the 6 × 6 mm choroidal vascularity index values or a development of macular atrophy during follow-up. These findings correspond to those of a larger case series, wherein no macular buckle–related pigmentary changes or atrophy were observed at a mean follow-up duration of 55 months. 36 Nevertheless, a longer observation period is warranted to detect hypoperfusion of both the optic nerve head and macular choroid.
This study has several limitations. The investigational use of the device is not yet approved by the Food and Drug Administration for any purpose. The sample size was small, and outcomes between macular buckling surgery and vitrectomy were not compared. Type II errors exist, as there were no statistical approaches to address missing data. Therefore, the proposed surgical algorithm is currently conceptual and requires prospective research with a control group. Notably, the positive visual results may be affected by the exclusion of eyes with foveal macular atrophy or subfoveal macular neovascularization scars and may be associated with the initial disease duration, although this variable was not recorded in this study.
Furthermore, a disparity in BCVA gains was noted between the macular detachment category and the full eye group (P = .03 vs P = .05). This drop in significance might stem from delayed foveal recovery following progression to rhegmatogenous stages or MH formation, which necessitates more complex surgeries with tamponade. Additionally, the clinical significance of choroidal vascularity index stability must be further warranted by longer follow-up durations, and a larger sample size could validate these findings. Although patients with myopic lamellar MH were not included herein, those presenting with type B foveal morphology are advised to undergo surgery if they are visually symptomatic. 4
Because of the progressively posterior traction driven by posterior staphyloma, macular buckling surgery could represent an alternative treatment for individuals with a detached macula that does not significantly affect the complexity or success rates of subsequent vitrectomy when required. Our technique used common devices in RD surgery and showed favorable morphologic success in this patient group.
Supplemental Material
sj-docx-1-vrd-10.1177_24741264261465000 – Supplemental material for Modification of Silicone Materials in T-Shaped Macular Buckling Surgery
Supplemental material, sj-docx-1-vrd-10.1177_24741264261465000 for Modification of Silicone Materials in T-Shaped Macular Buckling Surgery by Yodpong Chantarasorn, Chairat Saovaprut, Thanaporn Kritfuangfoo, Itsara Pokawattana, Kornwipa Hemarat and Plern Sutra in Journal of VitreoRetinal Diseases
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board of the Faculty of Medicine Vajira Hospital (COA No. 199/2567), and the principles for this research were in full compliance with the Declaration of Helsinki and ICH-GCP.
Consent to Participate
All participants who met the inclusion criteria provided informed consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during the current study are not publicly available to protect the patients’ personal information. They are available from the corresponding author upon request.
Supplemental Material
Supplemental material is available online with this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.