
Abstract
Corrona is a prospective observational registry founded in 2002 that collects data from patients and physicians about rheumatoid arthritis, psoriatic arthritis, other spondyloarthritis, and psoriasis. Here, we summarize the significant findings derived from the psoriatic arthritis Corrona database and describe future goals for Corrona's application in psoriasis.
Introduction
Corrona, first conceptualized by academic rheumatologists, is an independent registry lacking any connection to the pharmaceutical industry.1,2 Although initially designed to monitor rheumatoid arthritis (RA) in 2002, Corrona launched a spondyloarthritis registry encompassing psoriatic arthritis in 2013; an international registry in 2011 including Eastern Europe, Latin America, and India; and a psoriasis registry through a collaboration with the National Psoriasis Foundation in 2015. 2 Physicians and patients from multiple private and academic centers document information in these registries that can be analyzed to provide insight into disease natural history, comorbidities, and treatment outcomes to ultimately improve patient care and quality of life. 1
By March 2014, Corrona had collected “real world” disease activity and treatment information from more than 39,956 patients and 600 rheumatologists, comprising 111,303 total patient-years. 3 Due to their chronic disease states, psoriasis and psoriatic arthritis often require prolonged treatment with systemic agents. Although these systemic agents have numerous benefits, they are associated with adverse events (AEs) such as an increased risk of infection. 4 Corrona has the ability to produce a more robust and comprehensive characterization of these AEs without the inherent limitations of clinical trials.
With the use of a unique sign-on code, Corrona may be queried to perform a customized analysis based on gender, age, drug, insurance type, or laboratory abnormality and present it in a designated output format. 5 Researchers have utilized data from Corrona to test various hypotheses about the natural history, associated comorbidities, and treatment outcomes of psoriatic arthritis which are summarized here. We also discuss the impact Corrona will have on psoriasis in the future.
Natural History of Psoriatic Arthritis
Psoriatic arthritis is a chronic, inflammatory arthritis associated with joint swelling, stiffness, and pain. It affects approximately 0.3% of the general population and 20–30% of psoriasis patients, and is more prevalent among patients with severe skin psoriasis. 6 Psoriatic arthritis often manifests approximately a decade after the onset of skin lesions and is characterized by diverse clinical presentations, including peripheral arthritis, enthesitis, axial arthritis, and dactylitis. A hallmark of psoriatic arthritis is the simultaneous findings of bony proliferation and erosive change on radiographic examination of a single unit, which may occur at variable disease time points. 7
Bone Loss
Although generalized bone loss has been reported in psoriatic arthritis, its prevalence and risk factors are not well understood. 8 Corrona data were analyzed to determine patterns of generalized bone loss in 2,212 psoriatic arthritis patients. Associations were calculated between outcomes, including erosions on hand and feet x-rays, lumbar spine, femoral neck, and total hip t-scores, and patient variables, including gender, age, weight, C-reactive protein, functional status, Health Assessment Questionnaire scores, body mass index, medication, and medication dose. Patients with erosions demonstrated significantly lower lumbar spine bone mineral density than those without erosions when corticosteroids, disease-modifying antirheumatic drug (DMARD), and anti-TNF treatment for osteoporosis were controlled for. A proposed mechanism is the upregulation of osteoclast activity and elevated inflammatory cytokine levels in joints and circulation stressing the importance of targeted cytokine inhibitors such as anti-TNFs in controlling the progression of bone destruction in psoriatic arthritis.9,10
RA Comparison
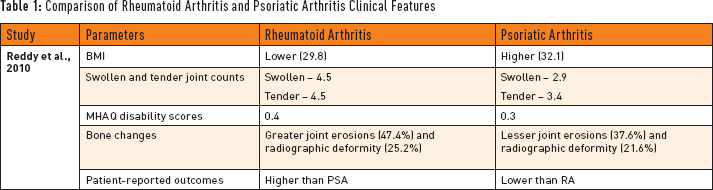
Although bone and cartilage destruction may occur in both psoriatic arthritis and RA, psoriatic arthritis has historically been viewed as a milder disease. 11 However, recent studies have demonstrated the presence of radiographic joint damage in the initial two years of diagnoses in 47% of psoriatic arthritis patients. 12 Psoriatic arthritis and RA disease severities were compared using the Corrona database; researchers assessed disease activity, radiographic features, and bone mineral density in psoriatic arthritis and RA patients matched for age, gender, and disease duration summarized in Table 1. 10 Overall, this study illustrated comparable disease severity and radiographic outcomes in psoriatic arthritis and RA warranting an early and aggressive approach to psoriatic arthritis treatment similar to that of RA treatment to ultimately decrease disease-related morbidity.
Comparison of Rheumatoid Arthritis and Psoriatic Arthritis Clinical Features
Comorbidities in Psoriatic Arthritis
Metabolic Syndrome
Metabolic syndrome, a well-established co-morbidity of psoriatic disease, is thought to result from systemic inflammation and elevated levels of pro-inflammatory cytokines such as TNF-α, interleukin-6, and interleukin-17. 13 Since inflammation is present in both the skin and joints in psoriatic arthritis, researchers used Corrona to evaluate whether the rate of metabolic syndrome and its component medical conditions was higher in psoriatic arthritis than in RA. 14 Psoriatic arthritis patients demonstrated higher rates of diabetes mellitus (15% vs 11%, p=0.02), and elevated triglyceride levels (38 % vs 28%, p= 0.003). Additionally, the rate of metabolic syndrome in patients with psoriatic arthritis was higher than that of patients with RA (27% versus 19% respectively, p=0.02). Another study of Corrona data illustrated complementary findings demonstrating higher body mass index (BMI) in psoriatic arthritis patients than RA patients. 10 Since psoriatic disease is a known independent risk factor for cardiovascular AEs, these Corrona studies underscore the importance of screening, counseling, and intervening in the metabolic syndrome and its component conditions in this population.
Malignancy
The Corrona database helped to define patterns, risk factors, and relative incidences of malignancies in 19,260 RA and 2,970 psoriatic arthritis patients due to concerns about the potential additive effect of underlying skin and joint inflammation on malignancy risk in psoriatic arthritis patients. 8 Corrona analysis demonstrated no difference in the overall rate of malignancy or cancer subtypes, including non-melanoma skin cancer and lymphoma, between psoriatic arthritis and RA cohorts. Across cohorts, non-melanoma skin cancer was the most prevalent cancer sub-type. The incidence of non-melanoma skin cancer in the psoriatic arthritis population was characterized as intermediate, falling between high and low-risk control populations from north central New Mexico and Minnesota, respectively. 13 Additionally, the analysis demonstrated an association between methotrexate (MTX) treatment and increased risk of malignancy, possibly due to its antimetabolite and immunosuppressive properties. However, this finding conflicts with two prior studies of psoriatic populations demonstrating no association between MTX treatment and malignancy, warranting further investigation of the topic.15,16,17 While no association was demonstrated between anti-TNF therapy and risk of malignancy in the present study, this relationship remains controversial since anti-TNFs have effects on apoptosis, cell survival, and cancer surveillance. 17 This Corrona-driven study helps characterize the cancer risk profiles of psoriatic disease and its treatments.
Psoriatic Arthritis Treatment
Appropriate treatment of psoriatic arthritis requires an aggressive approach. 12 Highly efficacious agents such as biologics play a central role in disease control with their ability to mitigate joint and skin disease, delay or prevent the development of joint damage, and improve the quality of life. Corrona enabled the characterization of biologic and DMARD therapy utilization rates among a large sample of 2,481 psoriatic arthritis and 17,107 RA patients for the first time. 18 Biologics were used more frequently in psoriatic arthritis than in RA patients (51.3% versus 43.6%, respectively) while DMARDs (90.4% versus 86.7%) and prednisone (36.9% versus 14.6%) were used more frequently in RA than in psoriatic arthritis patients.
Safety
Psoriatic arthritis treatment with certain systemic agents such as MTX for a long period of time has inherent safety concerns and is known to cause transaminitis. 19 The Corrona database facilitated the first large-scale exploration of different DMARDs such as MTX and leflunomide (LEF) outside of a clinical trial. 20 Alanine aminotransferase and aspartate aminotransferase abnormalities were demonstrated in 14–35% of patients with RA or psoriatic arthritis receiving DMARD therapy with greater risk in patients receiving simultaneous LEF and MTX therapy, especially when the dose of MTX was greater than or equal to 10 mg/day. Finally, an approximately three-fold increased transaminitis risk was demonstrated in psoriatic arthritis patients when compared to RA patients, emphasizing the importance of monitoring for potential hepatotoxicity in psoriatic arthritis patients receiving DMARD therapy.
Psoriasis Corrona Registry
Psoriasis is a chronic, immune-mediated disease affecting nearly 3% of the U.S. population with multiple comorbidities including metabolic, cardiovascular, psychiatric, and rheumatologic comorbidities. The Corrona psoriasis registry was launched in April 2015 through a collaboration with the National Psoriasis Foundation, the major advocacy organization serving psoriasis and psoriatic arthritis patients. The primary objective is to study the comparative safety of approved systemic psoriasis therapies in a national cohort of psoriasis patients in a real-world setting.
Other proposed uses of the registry include analyzing epidemiology, comorbidities, treatment practices, and comparative effectiveness. Psoriasis patients 18 years or older who have initiated or switched systemic anti-psoriatic agents such as FDA-approved biologic (adalimumab, etanercept, infliximab, ustekinumab, secukinumab, or ixekizumab) and non-biologic (MTX, cyclosporine, and apremilast only) treatment in the past 12 months are eligible. Data are collected from participating dermatologists and patients at approximately six month intervals during scheduled outpatient visits. Corrona and the National Psoriasis Foundation plan to recruit approximately 200 sites and 10,000 patients for an expected follow-up duration of at least eight years to compile authentic information to better characterize the safety, epidemiology, comorbidities, and treatment profiles of anti-psoriatic agents.
Conclusion
Although recent progress has advanced our understanding of psoriatic disease, many gaps in our knowledge remain. “Real world” Corrona data from the clinical setting will provide valuable insight into psoriatic disease activity, side effects, and treatment choices to ultimately guide future management. Additionally, studies utilizing Corrona will deepen our understanding of many aspects of the disease, including incidence, natural history, and characteristics of psoriatic arthritis joint destruction. Corrona will allow us to address key clinical questions such as whether early systemic intervention may prevent or delay the development of psoriatic arthritis and adverse cardiovascular outcomes that will significantly influence future approaches to this complex disease.21,22
Footnotes
Amgen Inc., Astellas, Akros, Centocor (Janssen), Inc., Celgene Corp., Bristol Myers Squibb Co., Beiersdorf, Inc., Abbott Labs. (Abbvie), TEVA, Actelion, UCB, Novo Nordisk, Novartis, Dermipsor Ltd., Incyte, Pfizer, Canfite, Lilly, Coronado, Vertex, Karyopharm, CSL Behring Biotherapies for Life, Glaxo Smith Kline, Xenoport, Catabasis, Meiji Seika Pharma Co., Ltd, Takeda, Mitsubishi Tanabe Pharma Development America, Inc, Genentech, Baxalta.
Centocor (Janssen), Amgen, Abbott (Abbvie), Novartis, Celgene, Pfizer, Lilly, Coronado, Levia, Merck, Xenoport, Dermira, Baxalta
All other authors have no conflict of interest.