
Abstract
Background
The risk for cardiovascular events associated with systemic therapies for psoriasis, including biologics, is unclear.
Methods
We used administrative data from Medicare 2006 through 2011 to identify psoriasis patients who initiated systemic treatments. We estimated incidence rates of hospitalized myocardial infarction, stroke, and a composite cardiovascular disease outcome, adjusting for potentially confounding factors.
Results
There were 28,878 initiations of psoriasis treatments. Rates of myocardial infarction were highest for methotrexate (10.32/1000 patient-years, 95%CI 8.55–12.46) and numerically lower for biologics. Patterns were similar for stroke and the composite cardiovascular disease outcome. After multivariable adjustment, there were no significant differences between systemic therapies for any of the outcomes studied.
Conclusions
In this cohort of predominantly older psoriasis patients, there was neither an elevated nor a protective effect on cardiovascular or stroke events associated with systemic therapies for psoriasis compared to conventional treatments.
Keywords
Introduction
Psoriasis, with an estimated prevalence of 2% in the United States, is a chronic, immune-mediated disease involving primarily the skin 1 and sometimes affecting other organs such as joints (i.e. psoriatic arthritis). Psoriasis and psoriatic arthritis are characterized by a variable clinical course with episodes of exacerbation and remission which cause disability by greatly affecting the patients’ quality of life. 1 Quality of life is often poorer among patients with psoriasis and psoriatic arthritis than among those with psoriasis alone. 2 People with psoriasis are at increased risk of developing other chronic conditions, including cardiovascular disease (CVD). 3
In addition, patients with psoriasis may have a shorter life-expectancy compared to the general population. 4
This premature mortality may be explained by the fact that patients with psoriasis have a higher prevalence of cardiac risk factors than the general population, including obesity, 5 cigarette smoking, 5 dyslipidemia, 6 hypertension, 7 diabetes,7,8 and metabolic syndrome. 9 In addition, the disease itself is an independent risk factor for CVD,10,11 and some systemic medications (e.g. retinoids, cyclosporine) used to treat psoriasis and psoriatic arthritis may increase the risk of CVD,12,13 while others may decrease this risk. 13 While the pathogenesis of the development of CVD in psoriasis and psoriatic arthritis patients is not understood, systemic inflammation with the involvement of common immune pathways in both psoriasis and CVD has been proposed as a possible mechanism. 14
There is conflicting evidence in terms of whether psoriasis and psoriatic arthritis are associated with increased risk for death, and cardiovascular (CV) morbidity and mortality. In a meta analysis, patients with psoriasis were found have increased risk of CV mortality, CVD, and all other CV outcomes (including peripheral artery disease [PAD], stroke, myocardial infarction [MI], and ischemic heart disease), but not all-cause early mortality. 3 Patients with psoriatic arthritis had a higher risk of early all-cause mortality and CV mortality, PAD, and heart failure, but no significant increase in risk of overall CVD was demonstrated, perhaps because studies were underpowered to demonstrate this latter association. The increased risk for MI and coronary artery disease in patients with psoriasis and psoriatic arthritis was highest in patients with severe psoriasis or psoriasis of early-onset. 11
The effect of systemic treatments on CV risk remains to be elucidated. A cohort study using administrative and pharmacy claims data from a commercial U.S. insurer found a non-significant difference in MI risk in adult patients with psoriasis receiving systemic immunomodulatory therapies (methotrexate, cyclosporine, alefacept, efalizumab, adalimumab, etancercept, and infliximab) compared to phototherapy. 15 The use of methotrexate was associated with a reduced incidence of CV disease in patients with psoriasis in some studies,16,17 but not in others.18,19 In a nationwide study of Danish patients with severe psoriasis, the use of biological agents was associated with lower rates of the composite endpoint of death, MI, and stroke compared to patients treated with other anti-psoriatic therapies after adjusting for covariates (age, sex, medication, comorbidity, and socioeconomic status). 18 However, the patients with psoriasis treated with biological agents had fewer comorbidities (CV disease, chronic pulmonary disease, diabetes, renal disease, or peptic ulcer disease) and were less often treated with CV pharmacotherapy, NSAIDs, or antidepressants. 18
Heterogeneity in study design, outcome and exposure definitions and assessment, small size of the populations studied as well as the paucity of studies on the contribution of systemic psoriasis therapies to CV outcomes represent major limitations in previous studies evaluating the association between psoriasis and CV outcomes. Given these limitations, we evaluated patients with psoriasis enrolled in the U.S. Medicare program to describe baseline comorbidities, determine the incidence rate of key CV events, and assess the CV event incidence rates associated with the use of systemic treatments.
Methods
Study Design and Data Source
U.S. Medicare claims data from July 1, 2006, through Dec. 31, 2011, including enrollment files, hospital (Part A) and outpatient medical care (Part B) claims, and claims for prescription drugs (Part D) were queried for the study.
Patient Population
To be eligible in this analysis, patients had to have i) at least 6 months of continuous enrollment in Medicare part A, part B, and part D prescription drug coverage, and not have been enrolled in a Medicare Advantage (Part C) plan prior to the first date of use of at least one treatment examined in this study, defined as “baseline;” and ii) met the case definition for psoriasis. Psoriasis was defined as > 1 dermatologist-assigned diagnosis code for psoriasis (ICD 9696.1), followed by a psoriasis-specific prescription or treatment (defined below). To ensure inclusion of only incident CV events in the analysis, we excluded prevalent CV events occurring during the six-month baseline period. Patients with a history of organ transplantation, infection with human immunodeficiency virus, advanced kidney (hemodialysis-dependent) disease, liver injury, or cancer diagnoses within the six-month baseline period prior to each new exposure episode were excluded. Given the requirement for a six-month baseline period, the earliest possible start of follow-up was therefore July 1, 2006.
The date of start of follow-up was the date of the first claim for a prescription or for the administration of one of the treatments of interest in the pharmacy or procedure database after an initial observation period of six months (termed baseline period). Patients contributed one or more treatment exposure episodes that began at time of first use of the treatment of interest and ended at the date of death, first occurrence of the outcome of interest, end of study period (12/31/2011), loss of Medicare Part A, Part B, and Part D coverage, or treatment switch or discontinuation, whichever event came first. Treatment discontinuation included a 90-day extension to current exposure, defined as the end of the days’ supply of filled prescription or the usual treatment interval for parenterally given drugs (e.g. 56 days for infliximab, 84 days for ustekinumab). Medicare beneficiaries who newly initiated another treatment of interest were at risk for a CV outcome as long as they met all eligibility criteria described above.
Treatment Episodes for Psoriasis and Psoriatic Arthritis
We evaluated the following treatments according to a “new user” design: etanercept (ETA), adalimumab (ADA), infliximab (INF), ustekinumab (UST), methotrexate (MTX), cyclosporine (CIC), and ultraviolet light therapy (UV, phototherapy). The date for the start of each treatment exposure episode was the first date of prescription or the first date of administration of the treatment in the pharmacy or procedure database. We identified treatments using both National Drug Codes in pharmacy data, and Healthcare Common Procedure Coding System level II injection/infusion codes (i.e. J-codes). “New use” was defined as evidence of a specific treatment for which there was no previous use in all the data available.
A hierarchy of treatment exposures was applied, ranking biologic exposure (ADA, ETA, INF, and UST) highest, followed by non-biologic disease modifying therapies (DMARDs) (MTX and CIC), followed by ultraviolet light therapy (UV). Consistent with this hierarchy, we excluded new exposure episodes of UV therapy if patients were on biologics or DMARDS at baseline, because these represented patients who added UV therapy to their biologic or non-biologic DMARD exposure. Likewise, patients initiating biologics who subsequently started a non-biologic therapy remained in the biologic exposure category. For example, a new user of ETA who 5 months later added MTX continued to accrue exposure time in the ETA exposure cohort, rather than being included in the MTX exposure cohort.
Outcomes
The outcomes of interest were: hospitalized MI, hospitalized ischemic stroke, and a composite CVD endpoint that included the first hospitalized MI or ischemic stroke. 20 Case definitions for each of these outcomes are described in footnotes to Table 2. The validity of administrative data to identify these outcomes is high, ranging from approximately 80% (stroke) to 95% (MI).21–26
Covariates
Demographic and socioeconomic variables of interest included age, gender, median household income, residence (nursing home vs community), geographic region of residence, and rural/urban residence. Race/ethnicity was categorized as white, black, black non-Hispanic, white non-Hispanic, Hispanic, Asian, unknown, or other. Health services related variables included baseline hospitalization, number of outpatient and emergency room visits, and number of medication classes. Specific comorbidities of interest included diabetes, hypertension, and chronic lung disease. The Charlson comorbidity index 27 was calculated as an overall measure of comorbidity burden. Concomitant medications of interest (e.g. systemic glucocorticoids, narcotics, NSAIDs) also were examined. All factors were measured at the start of follow-up in the baseline period.
Statistical Analysis
To calculate the crude incidence rate (IR) for each outcome of interest, the number of incident events was divided by the total person-years of observation within each cohort. Person-time was calculated by summing the number of days of enrollment between the start of follow-up and disenrollment or end of the observation period. Estimated rates per 1,000 person-years of follow-up and 95% confidence intervals (CIs) were calculated using the Poisson approximation. Pairwise propensity scores were estimated for each exposure contrast of interest using logistic regression, modeling the probability that patients received one treatment versus another. Covariates included in the propensity score were selected based on clinical interest and included demographics, markers of socioeconomic status (e.g. rural/urban, median household income of census block group of residence), concomitant psoriatic arthritis, comorbidities (e.g. diabetes, hypertension), and additional factors as described in Table 1. Glucocorticoid dose was not included in the propensity score since it was included separately in the statistical model for each outcome considered. Those patients in non-overlapping trails of the propensity score distribution were removed (i.e. “trimmed”). The propensity scores were graphed for each pairwise contrast.
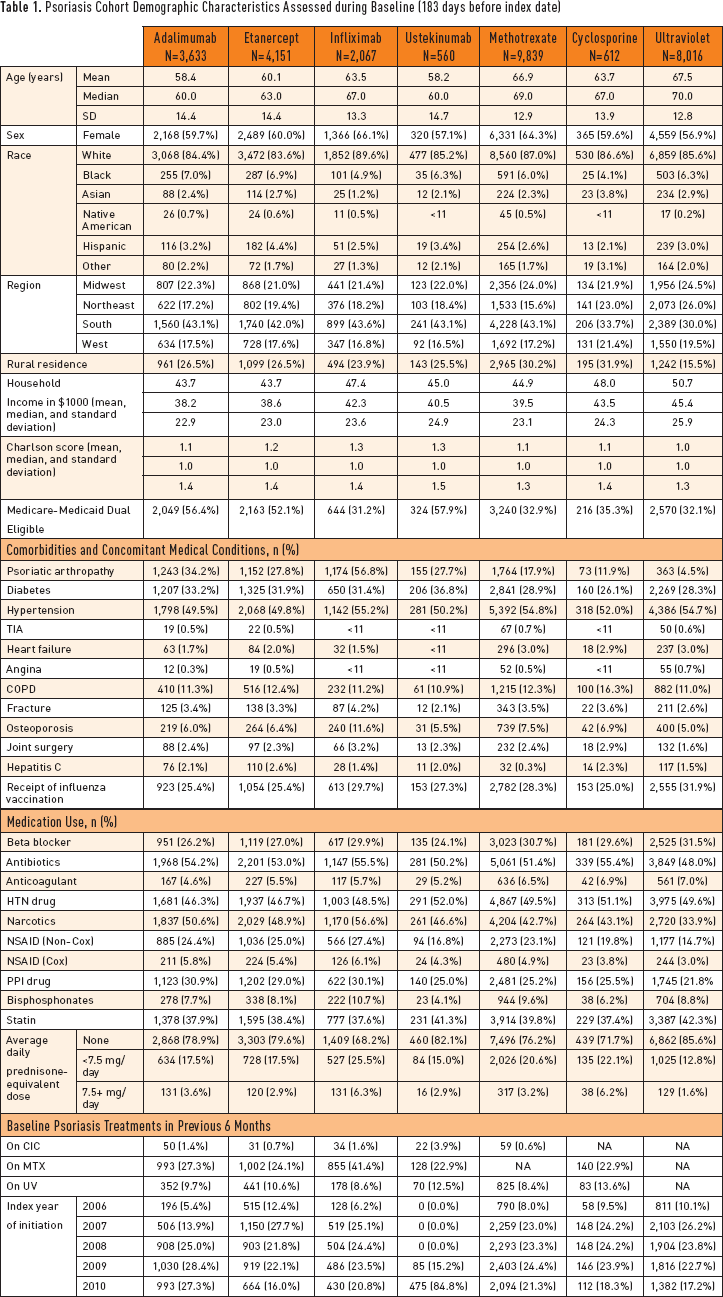
Psoriasis Cohort Demographic Characteristics Assessed during Baseline (183 days before index date)
Cox-proportional hazard regression models were used to calculate hazard ratios (HR) between propensity score-trimmed exposure groups of interest after controlling for potentially confounding covariates by adjusting for the propensity score quintile.28,29 For comparison of events between drug exposure groups, Cox-proportional hazard regression models were adjusted for age, gender, baseline prednisone use, and propensity score quintile. 30 Standard errors were adjusted for clustering of multiple exposure episodes within each patient using a sandwich estimator. 31 Data use agreement with Centers of Medicare Services prohibited showing information for cell sizes < 11. Therefore in the tables when the number of cases that was less than 11, “< 11” was indicated. Analyses were performed using SAS (version 9.3, SAS Institute, Cary, NC, USA). The study was governed by the institutional review boards of both participating universities.
A sensitivity analysis was performed using 1:1 propensity score matching to ensure similarity of treatment groups with respect to baseline demographic and medical characteristics. Details of comparison regimens and propensity score methodology have been previously published. 30
Results
There were 305,838 people who met inclusion criteria for the psoriasis cohort before exclusion criteria were considered. New users of each of six treatment exposures were subsequently identified. There were 3,633 users of ADA, 4,151 users of ETA, 2,069 users of IFN, 560 users of UST, 9839 users of MTX, 612 users of CIC, and 8,016 users of UV in the final psoriasis cohort. Demographic characteristics (region, rural residence, sex, and age), medical conditions of interest, and medication use stratified by each of the six treatment exposures in the psoriasis cohort are presented in Table 1. The cohort was predominantly female (57–66%) and white (84–90%) with a mean age range of 58–68 years. Half of patients treated with ETA or ADA were dual-eligible for both Medicare and Medicaid, and similar patterns were observed for use of ETA and ADA versus other therapies. Approximately 30% of patients had diabetes, and one-half had hypertension. The prevalence of various comorbidities was generally comparable between exposure groups. Roughly one-third of patients were treated with anti-hyperlipidemia therapy.
Propensity scores, representing the probability of initiating one treatment over the other for each treatment exposure pairwise comparison, were graphed (Appendix Figures; Appendix Figures and Table available in Online Supplement at www.psoriasis.org/jppa). For most comparisons, there was appreciable overlap between curves, indicating that the majority of patients were comparable to patients in the other treatment groups based upon observed characteristics. For example, the propensity score distributions were very similar between initiators of ETA and ADA. There was more asymmetry in the contrasts between biologics and conventional treatments such as MTX and CIC. As described, the treatment episodes from people whose scores were in the tails of each propensity score distribution were removed from analysis. The proportion of treatment episodes removed by trimming ranged from as low as 5% for ETA versus ADA to as high as 19.8% for UST versus MTX.
Crude incidence rates (Table 2) and adjusted hazard ratios (Table 3) were calculated for all outcomes of interest. The overall crude incidence rate for the composite endpoint was 14.99 (95% CI 13.66, 16.44) per 1000 patient years. Overall, the incidence rate per 1000 patient-years for MI was 9.46 (8.42, 10.63) and was greater than the corresponding incidence rate for stroke, 5.97 (5.16, 6.91). Rates were highest for MTX and numerically lower for all biologics, although confidence intervals overlapped. After multivariable adjustment for propensity score quintile and glucocorticoid dose, there was no significant difference between any of the psoriasis treatments for each of the three outcomes. In the sensitivity analysis that matched patients 1:1 by propensity score, there were no significant differences between any of the psoriasis treatments evaluated in pairwise comparisons (Appendix Table; Appendix Figures and Table available in Online Supplement at www.psoriasis.org/jppa).
Crude Incidence Rates of Composite Cardiovascular Disease Endpoint, Hospitalized Myocardial Infarction, and Ischemic Stroke among Psoriasis Patients
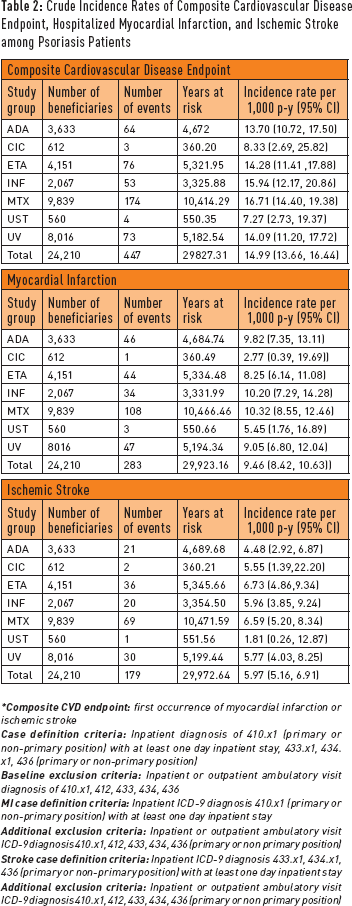
*
Multivariable Adjusted * Risk of Composite Cardiovascular Disease Endpoint, Hospitalized Myocardial Infarction, and Ischemic Stroke among Psoriasis Patients
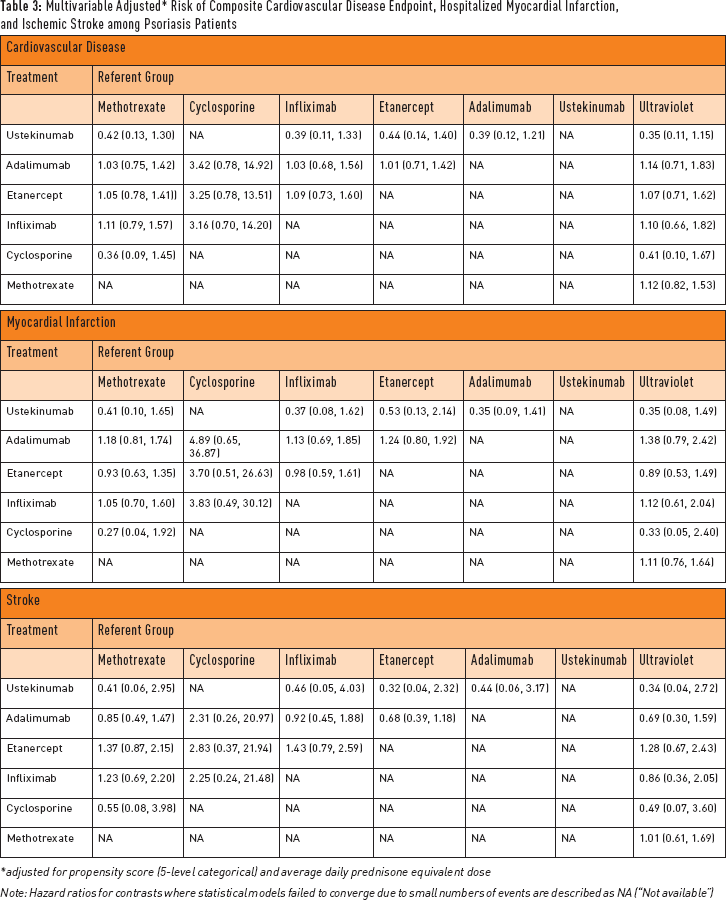
adjusted for propensity score (5-level categorical) and average daily prednisone equivalent dose
Note: Hazard ratios for contrasts where statistical models failed to converge due to small numbers of events are described as NA (“Not available”)
Discussion
We utilized data from a large psoriasis cohort to estimate comorbidities associated with CVD events and to quantify the incidence of CV outcomes including hospitalized MI and ischemic stroke associated with exposure to ETA, ADA, INF, UST, MTX, CIC, and UV. There was a numerically lower crude rate of CVD events in the biologic treatment groups compared to systemic therapy with MTX. However, after multivariable adjustment, we did not find significant differences between systemic psoriasis treatments that were associated with either incremental CV harm or a protective benefit.
Individuals with psoriasis and psoriatic arthritis are at increased risk of developing CVD 3 and exposure to an increased burden of inflammation (i.e. more severe disease as measured by disease activity for psoriatic arthritis [DAPSA]) has been associated with more severe atherosclerosis in patients with psoriatic arthritis, an association that appeared to be mediated by traditional CV risk factors. 32 Thus, screening and management of traditional CV risk factors in patients with psoriasis and psoriatic arthritis is recommended by professional societies;3,12,33 however, physicians and patients are often not cognizant of the increased CV risk associated with psoriasis and routine screening for CV risk factors is not often performed.34,35 For example, a study using National Ambulatory Medical Care Survey data reported that among 11.4 million psoriasis patient visits from 2005 to 2009, screening for CVD risk factors occurred infrequently, with blood pressure recorded for 32.2%, serum glucose for 5.9%, serum cholesterol for 9%, and body mass index for 26% of visits. 34 However, only 8% of the patients with psoriasis and dyslipidemia underwent treatment, while 78% of patients with psoriasis and abnormal glycemic tests underwent treatment. 36 No association was found between the severity of psoriasis and dyslipidemia, glycemic disorders, or hypertension. 36
Biologics may improve metabolic syndrome and insulin sensitivity in patients with psoriasis or psoriatic arthritis. The impact of therapy with ETA, ADA, and MTX on metabolic syndrome components (waist circumference, triglycerides, high-density lipoprotein cholesterol, and glucose) was evaluated in a cohort of 210 psoriatic arthritis patients followed over 24 months and achieving psoriatic arthritis response criteria. 37 The results showed that when the specific components of the metabolic syndrome were considered, the patients on ETA and ADA showed a significant improvement in the components of the metabolic syndrome as compared to those on MTX. In addition, significant improvement in insulin sensitivity was observed after six months of ADA therapy with moderate to severe psoriasis. 38
Our study adds to the body of literature evaluating the CV risk in patients with psoriasis taking systemic immunomodulatory therapy.15–19 A major strength of this study is the large size of the administrative database utilized, which allowed us to evaluate individual biologic, non-biologic DMARDs, and UV therapy for their association with CV events rather than considering them as a single group (e.g. all anti-TNF treatments). Because of the ability to link the pharmacy data (Medicare Part D) with the medical claims data (Medicare Parts A and B), Medicare has become an important data source for comparative effectiveness research.
Our study is subject to limitations inherent in the use of administrative datasets. The data may contain inaccuracies and inconsistencies in data coding by providers. Moreover, within Medicare administrative claims data, there is limited clinical information available (e.g., physiological measurements, test results, timing of events). 39 Because data for important covariates, such as smoking and obesity, which are risk factors for CVD, are not reliably captured in administrative claims data, we could not adjust our models for these confounders. In addition, some conditions, such as hypertension, depression, and diabetes, may be under-diagnosed, resulting in an under-estimate of their prevalence in administrative claims data. However, the outcomes of interest and comorbid conditions we studied were identified from the Medicare database using previously published algorithms that relied on diagnosis and procedure codes shown to have high validity. While it is possible that the differential misclassification of comorbidity status based on these algorithms could have introduced bias, there is no strong reason to believe that any misclassification of this type would be differential by psoriasis treatment.
Despite the large size of the study database, the external validity (generalizability) of our findings is subject to several considerations. The Medicare data system includes nearly all people aged 65 years and older in the U.S., younger people with disabling medical conditions, and people with end-stage renal disease. While these results are therefore generalizable to the fee-for-service Medicare population, generalizability to younger, commercially insured patients with psoriasis is unclear. Moreover, not all therapies are equally available to all patients. Insurance coverage options and the patient's ability to pay necessarily influence which treatments are prescribed. For example, patients receiving subcutaneously injected biologic medications typically would incur high out-of-pocket expenses under the Medicare Part D program unless they also qualified for Medicaid. Patients dually eligible for Medicare and Medicaid comprised approximately one-third to one-half of each exposure cohort. Thus, due to cost, self-administered biologic medications may be inaccessible to all but the more affluent or low income patients. In contrast, non-biologic therapies such as MTX or CIC are accessible to Medicare beneficiaries of all income levels. Thus, to the extent that idiosyncrasies of Medicare coverage dictate choice of treatment, care should be taken in generalizing these results to other populations.
Conclusions
Using data from a large psoriasis cohort of predominantly older patients, we found that the risk of CV events such MI and ischemic stroke were broadly comparable between systemic treatments used to treat moderate to severe psoriasis. Future investigation is needed on the impact of these treatments on the risk of CV events for newer therapies for psoriasis and psoriatic arthritis (e.g. apremilast or secukinumab) and in other populations with psoriasis and psoriatic arthritis, such as younger individuals.
Footnotes
Acknowledgements
This study was sponsored by Pfizer. The sponsor had no role in the design, analysis, or the decision to publish the manuscript. Dr. Curtis receives salary support from the National Institutes of Health (P60 AR064172) and the Patient Centered Outcomes Research Institute (PCORI).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.