
Abstract
Background:
Psoriatic nail dystrophy is infrequently assessed in routine care and observational cohorts due to the lack of a feasible validated outcome measure.
Objective:
To assess the measurement properties of the “Severity of NAil Psoriasis Score” (SNAPS) in PsA.
Methods:
Nail photography was performed on prospectively recruited patients at baseline and 6 months. The modified Nail Psoriasis Severity Index (mNAPSI) and Physician Nail Visual Acuity Scale (PhNVAS) were comparator instruments for construct validity. Reliability and feasibility were assessed using intra-class correlations (ICCs) and timed scoring. Responsiveness was assessed by correlating the changes in SNAPS, mNAPSI and PhNVAS. Retrospective data from the Bath PsA database was further utilized to assess responsiveness.
Results:
21 patients participated in the prospective validation at baseline. Inter- and intra-rater reliability of SNAPS were 0.94 and 0.93-0.96 (p ≤ 0.005). Mean times required to score SNAPS and mNAPSI were 59 and 136 seconds. There were strong correlations between SNAPS and mNAPSI (r = 0.95, p < 0.001) and PhNVAS (r = 0.77, p < 0.001) at baseline. There was a significant reduction in the mNAPSI and SNAPS (p < 0.005) at 6 months and a strong correlation between the change in SNAPS and mNAPSI (rho = 0.838, p < 0.001). Historical data from 57 patients commenced on Etanercept were evaluated. Mean SNAPS reduced from 3.6 to 2.0 at 3 months and 1.2 at 6 months (p < 0.05). Change in SNAPS correlated with changes in Psoriasis Area Severity Index and Dermatology Quality of Life at 3 and 6 months (r≥0.510; p ≤ 0.003).
Conclusion:
SNAPS is a feasible, reliable and responsive outcome instrument for psoriatic nail dystrophy.
Keywords
Introduction
Psoriatic nail disease (onychodystrophy) affects over 80% of patients with Psoriatic Arthritis (PsA). 1,2 Among people living with psoriasis, nail disease has a significant impact on quality of life, with over 50% of affected patients reporting associated pain. 3 -5 Psoriatic nail disease also has other important clinical implications, such as its association with distal interphalangeal joint (DIPj) inflammation and damage in patients with PsA, reflecting the anchoring of the nail bed and matrix to the DIPj and distal phalanx by components of the extensor tendon and collateral ligaments. 6 -11
Features of psoriatic nail disease include nail matrix manifestations such as pitting, leukonychia, crumbling, Beau’s lines and red spots, which are visible in the nail plate, and nail bed manifestations such as onycholysis, oil drop dyschromia, subungual hyperkeratosis and splinter hemorrhages.
Despite the existence of over 20 clinical outcome measures for the assessment of psoriatic nail dystrophy, data collection rarely occurs in observational PsA cohorts. This is likely attributable to the lack of validated feasible outcome measures for use in routine care. 12 In the Bath PsA cohort, psoriatic nail dystrophy has been assessed longitudinally using the Severity of NAil Psoriasis (SNAPS) for over a decade. This instrument was first described in 1994 by Jones et al. and is the product of collaboration between dermatology and rheumatology, but has not previously been validated. 11
The objective of this study was to evaluate the measurement properties of SNAPS in order to determine its feasibility, reliability and responsiveness as an outcome instrument for the assessment of psoriatic nail disease in routine care and longitudinal cohorts.
Methods
Consenting patients aged ≥18 years who met the ClASsification for Psoriatic ARthritis (CASPAR) Criteria and attended routine clinical appointments at the Royal National Hospital for Rheumatic Diseases in Bath were included. Two datasets were used to address the study objectives. Cohort 1 was a prospective cohort of patients assessed with serial nail assessments to determine feasibility, reliability, construct validity and responsiveness. Cohort 2 was a historical cohort of patients from the Bath biologics database for the assessment of responsiveness.
Cohort 1
A convenience sample of 21 consenting patients with a spectrum of psoriatic nail disease were approached at PsA clinics. All patients were assessed at baseline and patients who attended a routine clinic appointment at 6 months underwent follow-up assessment. Ethical approval was granted by the South West – Central Bristol Research Ethics Committee (REC: 18/SW/0226).
Clinical assessments
Patients were clinically assessed with a 66/68 Swollen and Tender Joint Count (66/68 SJC/TJC), Psoriasis Area Severity Index (PASI), Leeds Enthesitis Index (LEI), Leeds Dactylitis Index (LDI) and Physician Global Assessment for Psoriatic Arthritis (PhGA) during their clinic appointment. Patients also completed patient-reported outcome measures including the Health Assessment Questionnaire (HAQ), Patient Global Assessment for Psoriatic Arthritis (PtGA) and Dermatology Quality of Life Index (DQLI).
Following their clinic appointment, patients underwent digital photography of their fingernails. Dorsal images of individual fingernails were acquired using a tripod-mounted digital SLR camera with standardized exposure settings. In order to achieve consistency in image acquisition, a paper template with markings to guide digit placement and a scale to guide magnification was utilized. The templates were affixed with the patient’s study ID number and labeled, to indicate the digit which was being photographed and to achieve anonymization. A second image was taken of each nail, focusing on the reflection of each nail in an adjacent angled mirror, in order to adequately visualize the hyponychium and capture subungual hyperkeratosis.
Physician assessment of nail outcome measures
All available photographs were scored at baseline and at 6 months using the modified Nail Psoriasis Severity Index (mNAPSI), SNAPS and Physician Nail Visual Acuity Scale (PhNVAS).
SNAPS was developed by a dermatologist (CL) and rheumatologist (NMcH) to collect longitudinal data on psoriatic nail disease in the Bath PsA cohort. SNAPS assesses the presence of 4 features: pitting, onycholysis, subungal hyperkeratosis, and severe nail disease. It captures the common features of both nail bed and matrix disease. 1,13,14 Severe nail disease is defined as onycholysis, pitting or subungual hyperkeratosis affecting both sides of the nail across its longitudinal midline. This functions as a measure of severity while avoiding the potential reliability issues associated with estimating the percentage of nail involvement. The presence of each feature in a nail confers a score of 1 resulting in a score range of 0-40 in the fingernails.
The mNAPSI (range 0-130) assesses for the presence of leukonychia, red spots, subungual hyperkeratosis and splinter hemorrhages, with a score of 1 if present per nail. Onycholysis/oil spots and crumbling are each scored based on the percentage of nail surface area affected (range 0-3 per nail) and pitting is scored based on number of pits (range 0-3 per nail).
Physician Nail VAS (PhNVAS) in this study was scored on a scale of 0-100. Variants of the PhNVAS have been utilized in other studies and it has been shown to correlate with the mNAPSI and patient Nail VAS. 15,16 No anchor terms were used to define severity in this study.
Photographs were scored by 2 assessors who have been trained to use the mNAPSI, and use SNAPS routinely (WT and AA). Assessors were blinded to patient identity, clinical data and previous nail scores. The photographs of subset of patients were scored by both assessors on 2 separate occasions 2 weeks apart to assess inter- and intra-rater reliability. Scores at baseline and follow-up were evaluated to assess for responsiveness. The scoring process for was timed in a subset of consecutive patients to assess comparative feasibility.
Cohort 2: Retrospective Biologics Cohort
Retrospective data for patients from the Bath PsA biologics database who were commenced on etanercept and had routine clinical data including SNAPS that was prospectively collected at baseline, 3 months and 6 months was extracted. Clinical variables extracted included the 66/68 SJC/TJC, PASI, PtGA, PhGA, HAQ and DLQI.
Statistical Analysis
Descriptive methods were used to assess patient demographics, characteristics of nail disease and feasibility. A formal sample size calculation was not undertaken. The normality of data was assessed using the Shapiro-Wilk test given the small sample sizes.
In cohort 1, comparative floor and ceiling effects for the mNAPSI, SNAPS and PhNVAS were illustrated using histograms. Inter- and intra-rater reliability was assessed in 5 consecutive patients using intra-class correlations (ICCs) for single measures, with a 2-way random analysis for absolute agreement. Construct validity was assessed cross-sectionally between the SNAPS and the mNAPSI, PhNVAS, PASI, TJC, SJC, LEI and LDI using pairwise correlations. Responsiveness was assessed using pairwise correlations between changes in these variables in patients for whom follow-up data was available and by determining the standardised response mean (SRM) over 6 months.
In cohort 2, paired t-tests or Wilcoxon rank tests were used where appropriate to analyze the change in scores over time. Responsiveness was assessed using pairwise correlations between the change in SNAPS and in the 66/68 SJC/TJC, PASI, PtGA, PhGA, HAQ and DLQI, and by calculating the SRM at 3 and 6 months. All statistical analyses were performed using SPSS v23.0 (IBM Corp., Armonk, NY, USA).
Results
Cohort 1: Prospective Validation
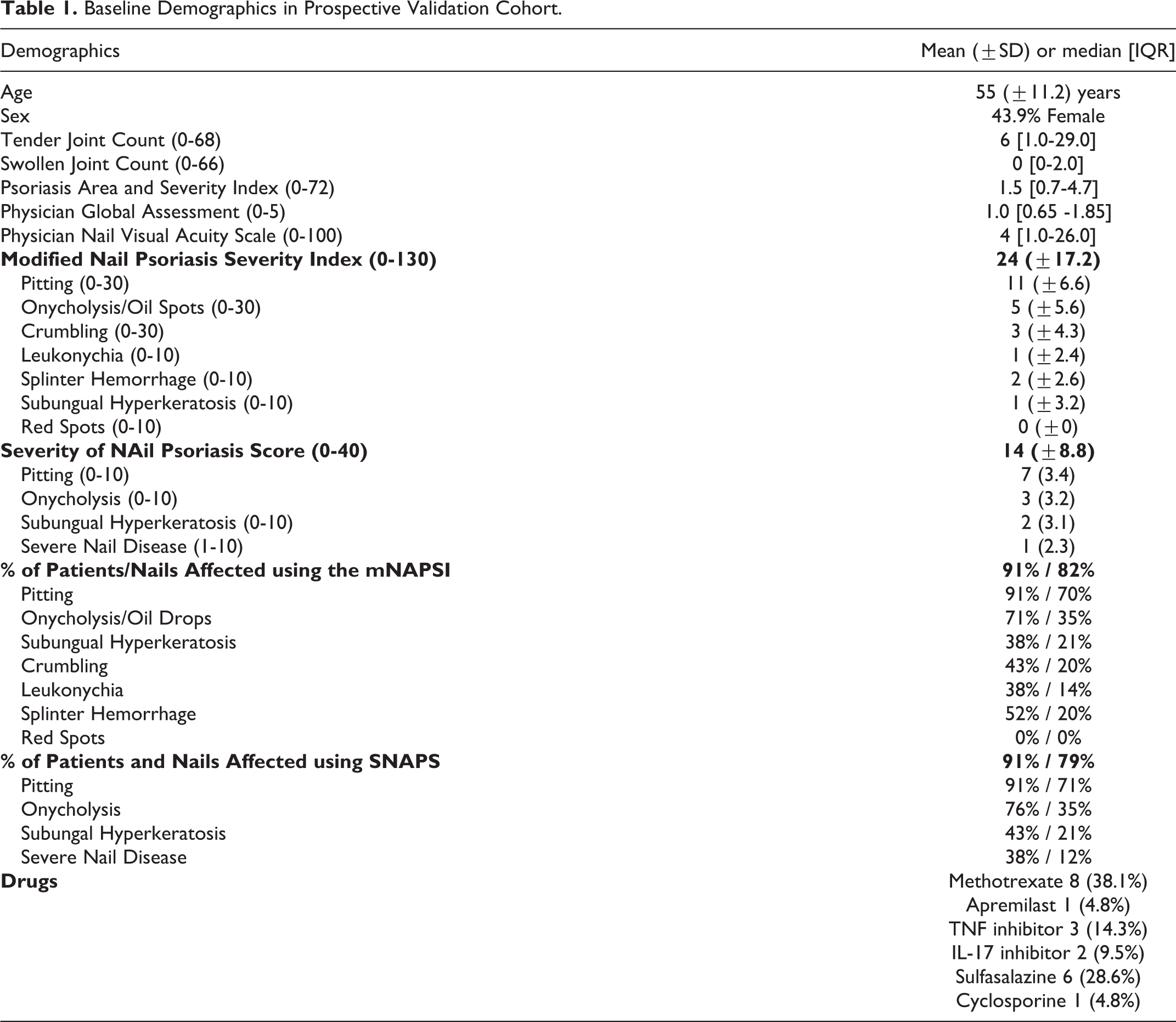
The 21 participants had a mean (SD) age of 55 (±11.2) years. Forty-five percent were female and 24% were on biologic disease-modifying drugs (bDMARDs) at baseline (Table 1). Nineteen of the 21 patients (90.5%) had evidence of nail disease using a nail outcome measure. Nail disease was identified in 82.4% of patients using the mNAPSI and 79% using SNAPS. The most frequently identified features of nail dystrophy using either instruments were pitting, onycholysis and/or oil drop dyschromia, and subungual hyperkeratosis, which affected approximately 70%, 35% and 21% of nails respectively. (Table 1). Histograms suggested a ceiling effect with SNAPS, with one participant having the maximal score of 40 (Figure 1).
Baseline Demographics in Prospective Validation Cohort.
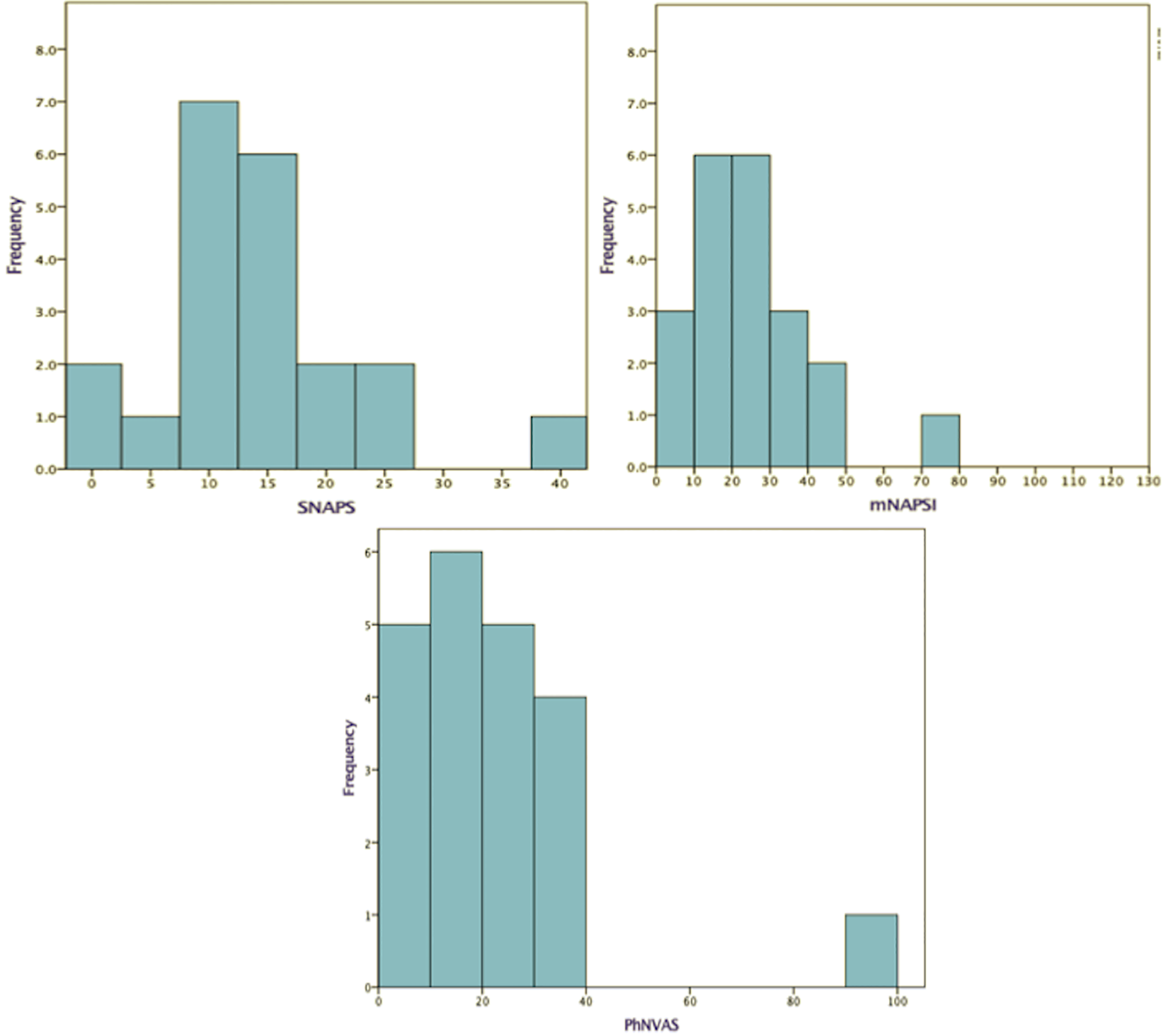
Histograms of scores for floor and ceiling effects of nail instruments at baseline.
The mean (SD) time required to score the SNAPS and mNAPSI in 7 consecutive patients were 59 (±13.0) and 136 (±27.8) seconds respectively. Intra-rater reliability (ICC [95% confidence interval; p-value]) was 0.96 [0.693-0.995; p = 0.001] and 0.93 [0.495-0.992; p = 0.005] for SNAPS, 0.95 [0.657-0.994; p = 0.002] and 0.97 [0.785-0.997; p = 0.001] for the mNAPSI and 0.84 [0.021-0.982; p = 0.026] and 0.82 [-0.075-0.979; p = 0.033] for PhNVAS. Inter-rater reliability was 0.94 [0.479-0.994; p = 0.001] for SNAPS, 0.78 [0.085-0.974; p = 0.027] for the mNAPSI and 0.91 [0.338-0.990; p = 0.009] for PhNVAS.
There was a strong positive correlation between SNAPS and the mNAPSI (Pearson’s r = 0.95, p < 0.001), and between SNAPS and PhNVAS (r = 0.77 p < 0.001) (Figures 2a and b). The mNAPSI also correlated strongly with the PhNVAS (r = 0.84, p < 0.001) (Figure 2b). There were no other significant correlations.
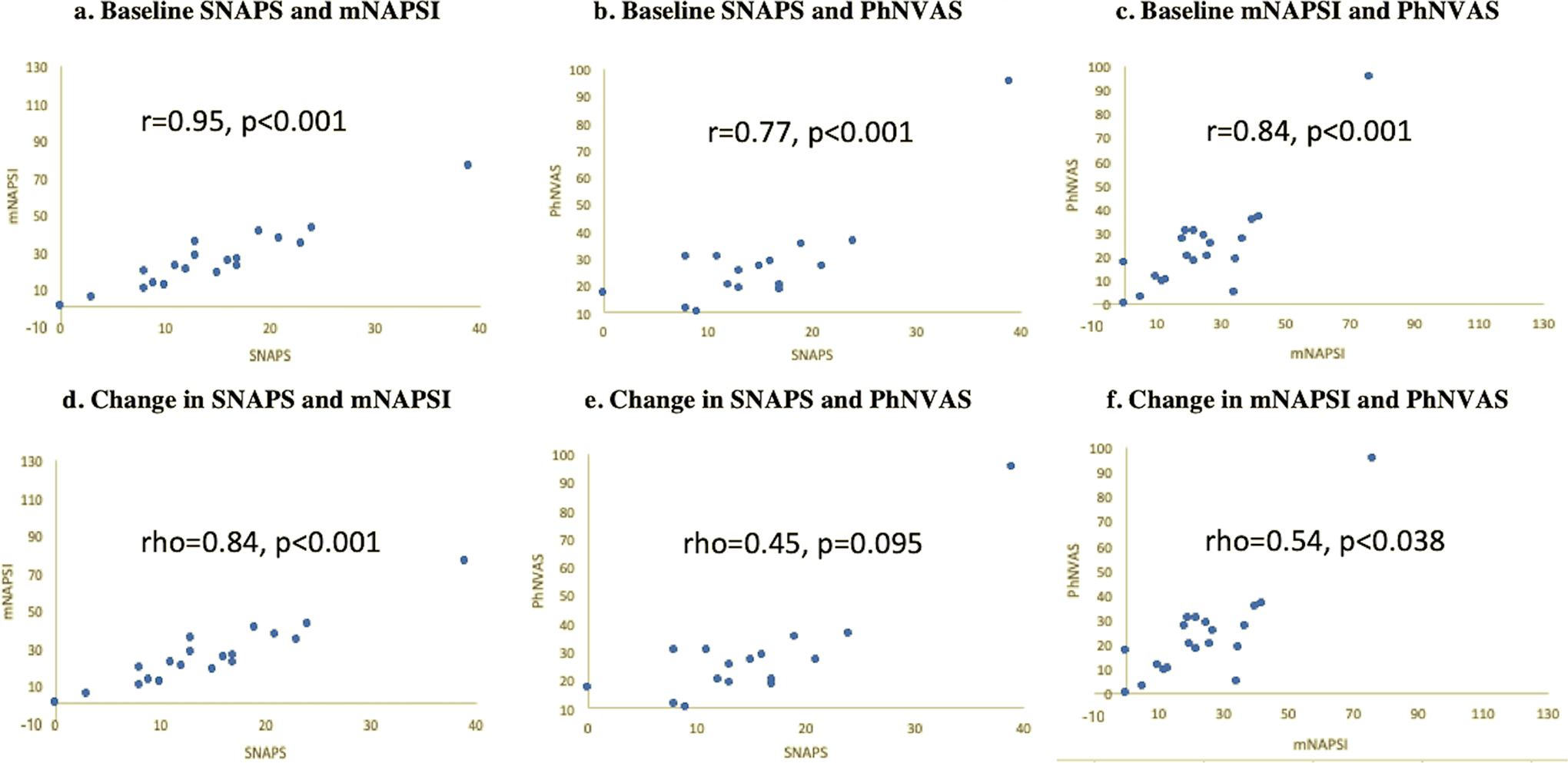
Correlations between SNAPS, mNAPSI and PhNVAS in prospective validation cohort.
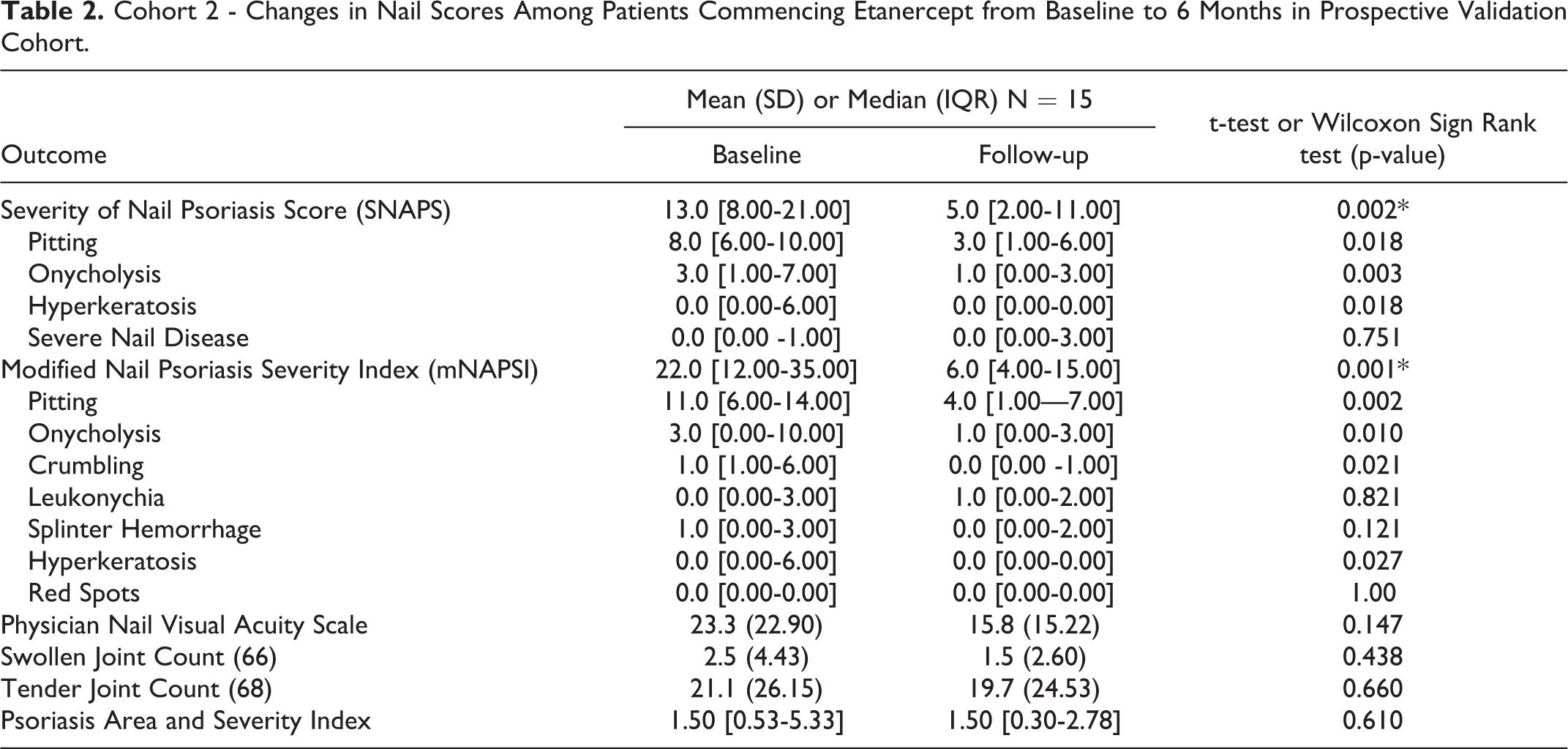
Follow-up nail assessments were available for 15 patients. There were no statistically significant differences between the demographics of this subgroup and those of the 21 patients at baseline, but the distribution of nail scores at follow-up was not parametric. There was a statistically significant reduction in both the mNAPSI and SNAPS (p < 0.005), with improvements in pitting, onycholysis/oil drop dyschromia, and subungual hyperkeratosis being the most frequently observed changes at 6 months (Table 2). Other than nail crumbling, no feature specific to the mNAPSI improved significantly over time. The improvement in PhNVAS was not statistically significant.
Cohort 2 - Changes in Nail Scores Among Patients Commencing Etanercept from Baseline to 6 Months in Prospective Validation Cohort.
There was a strong correlation between the change in SNAPS and the mNAPSI (Spearman’s rho = 0.838, p < 0.001) and moderate correlation between the change in SNAPS and in PhNVAS (rho = 0.45, p = 0.095), but the latter was not statistically significant (Figures 2d and e). The correlation between change in mNAPSI and change in PhNVAS was moderate and statistically significant (rho = 0.540; p = 0.038) (Figure 2f). Both instruments had similar effect sizes as measured by the SRM (1.15) and were superior to PhNVAS (0.40) in this cohort.
Cohort 2: Responsiveness in a Retrospective Cohort
Data for 57 patients commencing Etanercept was available, with a mean (SD±) age of 61.3 (±11.5) years and disease duration of 13.3 (±10.82) years. The mean (SD±) SNAPS was 3.6 (±6.13) at baseline, 2.0 (±3.74, p = 0.018 for change from baseline) at 3 months and 1.2 (±2.40; p = 0.001 from baseline and 0.039 from 3 months) at 6 months, mirroring improvement in other clinical outcomes with biologic therapy (Table 3). The SRM was 0.32 at 3 months and 0.44 at 6 months.
Baseline and Follow-Up Clinical Variables in the Biologics Validation Cohort.
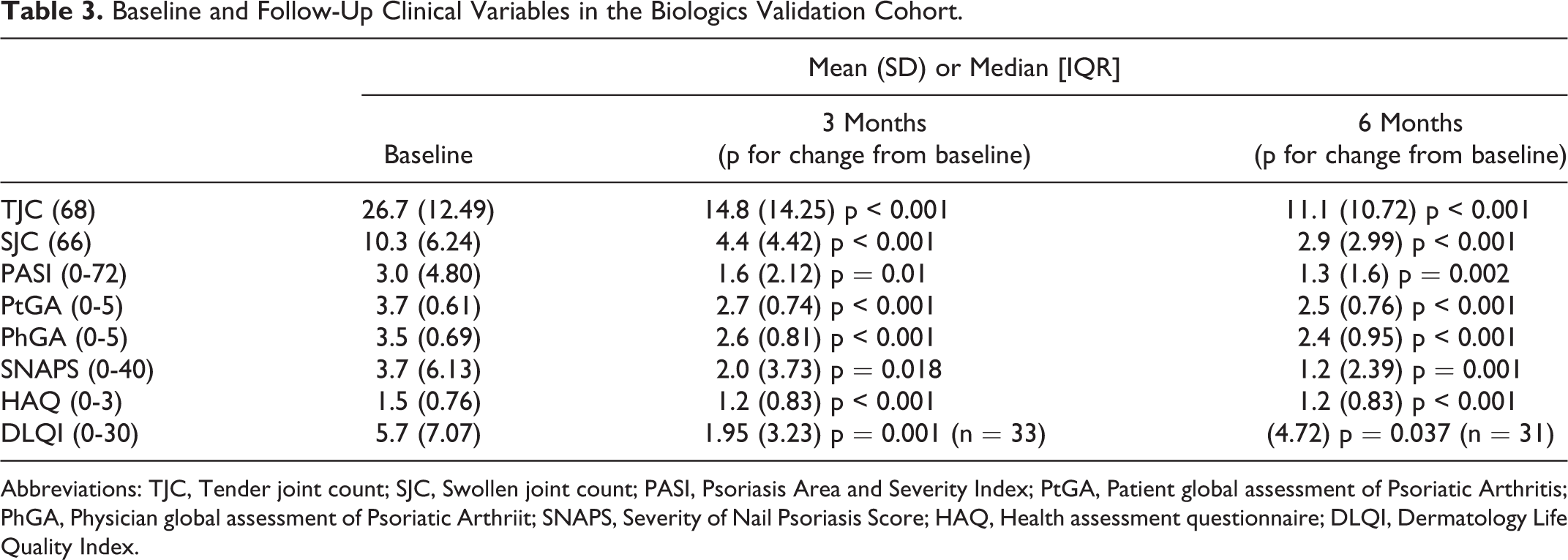
Abbreviations: TJC, Tender joint count; SJC, Swollen joint count; PASI, Psoriasis Area and Severity Index; PtGA, Patient global assessment of Psoriatic Arthritis; PhGA, Physician global assessment of Psoriatic Arthriit; SNAPS, Severity of Nail Psoriasis Score; HAQ, Health assessment questionnaire; DLQI, Dermatology Life Quality Index.
There was a moderate correlation between the change in SNAPS and changes in PASI and DLQI at 3 (r = 0.511 and 0.558 respectively, p = 0.001) and 6 months (r = 0.672, p < 0.001 and r = 0.510, p < 0.003). There was a weak correlation between change in SNAPS and change in PhGA (r = 0.289, p = 0.032).
Discussion
The validation of an outcome measure ideally encompasses the demonstration of its content and face validity, feasibility, reliability, construct validity and responsiveness. The results of this study suggest that SNAPS is feasible and demonstrates inter- and intra-rater reliability, construct validity and responsiveness.
SNAPS includes the most frequently described features of psoriatic nail disease and captures both nail matrix and nail bed features. 1,13,14 Furthermore, it does not include features such as red spots and leukonychia, that are infrequent or, in the case of leukonychia, equally common in the healthy population. 17 -19 SNAPS does not, however, capture crumbling, which potentially reflects severe and/or prolonged keratinization of the nail matrix, and oil drop dyschromia, which results from parakeratotic and acanthotic pathology in the underlying nail bed. 20 SNAPS also does not capture splinter hemorrhage, a non-specific feature that is common in some series. 13,14 Despite this, SNAPS was comparable to the mNAPSI in terms of quantifying the prevalence of nail dystrophy at a patient and individual nail level in our cohort, missing the presence of nail disease in <3% of affected nails (Table 1).
SNAPS did appear to have a ceiling effect, with one patient scoring a maximal score of 40 in the prospective validation. This patient had a mNAPSI of 76/130 and a PhNVAS of 95/100, which reflects the lack of a ceiling affect in the mNAPSI conferred by its redundant upper range. The presence of the ceiling effect may in part relate to patients with more severe nail disease being more inclined to participate. This ceiling effect was not evident in the biologics validation cohort, where the SNAPS score range was 0-25.
In regard to feasibility, SNAPS is a simple tool which can be learnt and taught quickly, and its use is not associated with any costs. Scoring nail dystrophy using SNAPS was twice as quick as the mNAPSI, which is an important consideration in routine care.
The inter-rater reliability of SNAPS was excellent, comparable to the PhNVAS and superior to the mNAPSI in our study. It is important to note however that the mNAPSI, which was developed to overcome the perceived limitations of the Nail Psoriasis Severity Index (NAPSI) relating to the latter’s use of a quadrant system for scoring and its impact on reliability and responsiveness, has previously demonstrated excellent inter-rater reliability (ICC = 0.92) in its original validation which was based on nail photography of 20 patients and in a further validation based on real-time assessments in 20 patients (ICC >0.80). 19,21,22,23
SNAPS, the mNAPSI and PhNVAS demonstrated excellent intra-rater reliability in this study (ICCs ≥0.84), which is a novel finding for each of these instruments. This is a particularly important finding for an instrument that is to be used in routine clinical care, where there may be significant variability in the experience of the assessor. Intra-rater reliability for NAPSI as measured by the ICC have not been reported. 22
Two previous studies have addressed the construct validity of SNAPS (referred to as PNSS in some studies). A modification of the instrument by Williamson et al. who included the assessment of fingernails and toenails, has demonstrated cross-sectional correlations with PsA outcome measures including body surface area (Pearson’s r = 0.34, p = 0.004), PhGA (r = 0.45; p < 0.001), HAQ (r = 0.34; p = 0.004), depression (r = 0.39, p < 0.001) and anxiety (r = 0.34; p = 0.004). 1 Additionally, Klassen et al. examined the construct validity of various nail outcome measures with the PhGA as a comparator instrument, and found an excellent correlation between SNAPS and PGA; unfortunately, the definition of severe nail disease used in the study was inaccurate as it had not previously been formally described. 24
The comparator instruments chosen for our study were the mNAPSI and PhNVAS. The former has demonstrated cross-sectional construct validity, with moderate correlations with patient nail global and other measures of PsA disease activity such as swollen and tender joint count (rho = 0.41-0.55). 15 The latter has demonstrated excellent inter- and intra-rater correlations with the mNAPSI, and moderate correlations (rho = 0.47) with patient nail global score and other measures of disease activity. 15 We found strong correlations between SNAPS and the mNAPSI (r = 0.95, p < 0.001), SNAPS and PhNVAS (r = 0.77, p < 0.001), and the mNAPSI and PhNVAS (r = 0.84, p < 0.001) (Figure 1). There were no significant correlations with SJC, TJC, PhGA or PASI.
In our study, there was a strong correlation between the change in SNAPS and mNAPSI over 6 months (rho = 0.872, p < 0.001). The correlation between change in SNAPS and PhNVAS was moderate but not statistically significant. We also demonstrated a significant correlation between change in mNAPSI and PhNVAS (Figure 2f). These findings are important, as the longitudinal construct validity of the mNAPSI has not previously been assessed against a comparator instrument. The NAPSI is the only outcome instrument for nail dystrophy that has previously has demonstrated weak longitudinal convergent construct validity with PASI (r = 0.2777; p < 0.001) in patients with psoriasis treated with infliximab. 25
In terms of the responsiveness of the individual features of nail dystrophy captured in SNAPS, there were significant improvements in pitting, onycholysis and hyperkeratosis at 6 months. The variable of ‘severe nail disease’ did not change significantly, which was unsurprising given the median score [IQR] for this at baseline was 0 [0 -1]. This may also reflect the fact that more severe disease may take a longer time to improve and may be more treatment-refractory. Of the features captured by the mNAPSI, only pitting, onycholysis/oil drop dyschromia, hyperkeratosis and crumbling scores improved significantly at 6 months; the remaining features were uncommon and the median baseline scores for these were low. The standardised response means (SRM) of SNAPS and the mNAPSI were comparable and superior to the PhNVAS in this small cohort.
Randomized controlled trials and retrospective cohort studies have shown that tools such as the mNAPSI and NAPSI can demonstrate significant improvement in nail disease as early as 10-12 weeks. 26 -28 In our biologic validation cohort, treatment with etanercept resulted in a statistically significant improvement in SNAPS at 3 and 6 months, despite a low mean SNAPS score of 3.2 at baseline. This change correlated moderately with changes in the DLQI and PASI, with PASI being a potential confounder for the correlation with DLQI. The effect size (SRM) was small at 3 months and moderate at 6 months.
Our validation exercise had a number of limitations. A significant limitation was the small sample size in our prospective validation cohort, which is a feature of most studies undertaking the validation of outcome instruments for psoriatic nail disease. This was particularly pertinent for the estimation of reliability. The use of nail photography is a potential limitation of our prospective validation, but is common approach in studies validating nail outcome instruments. We also had a long interval between assessments in our observational cohort, and were therefore unable to make any conclusions regarding the responsiveness of the instrument at intervals of < 6 months in cohorts not treated with bDMARDs.
The biologics validation cohort data are limited by the lack of a control arm and the open-label nature of treatment; however, these results support the validity of SNAPS given the assessors conducted the assessment of nail disease directly on patients (as opposed to photographs) as part of routine care and were not influenced by a study hypothesis. Finally, we did not utilize an anchor instrument to allow for the estimate of the minimally-clinically important difference (MCID) of SNAPS or mNAPSI, neither of which has been defined.
Despite these limitations, the cumulative evidence from our prospective and biologic validation cohorts does support our hypothesis that SNAPS is a valid instrument for measuring psoriatic nail disease. The instrument demonstrates excellent feasibility and reliability, and good cross-sectional validity and responsiveness. The findings of the relative responsiveness of the mNAPSI and SNAPS does require further study prior to drawing firm conclusions, as we expect that the mNAPSI may have a superior responsiveness conferred by the gradation of severity in pitting, crumbling and onycholysis, as well as the incorporation of oil spots into the onycholysis domain. While the PhNVAS is an attractive alternative instrument on the basis of its feasibility and its reliability, its responsiveness to change was inferior and further validation studies are necessary particularly given the lack of anchoring terms used in this study.
Conclusion
SNAPS demonstrated validity for the assessment of psoriatic nail dystrophy in the routine clinical care of patients with PsA and may be a useful instrument in longitudinal observational cohorts. It had adequate responsiveness and was able to detect change in patients with significant nail dystrophy at baseline and in those commenced on Etanercept.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.