
Abstract
Introduction
Psoriasis, a chronic inflammatory disease of the skin and joints, is increasingly recognized as a systemic inflammatory process and is often associated with increased rates of comorbidity. It is estimated that 2-3% of the adult population are affected by psoriasis in the United States (US). 1 While the management of psoriasis has been extensively outlined with special emphasis on the use of biologics, 2 little is known of how disease characteristics and management vary geographically across the US. The identification of geographic patterns in certain other metabolic diseases, such as diabetes and cerebrovascular disease, has aided in focused efforts to better understand their pathophysiology as well as to provide insight into how to better address these as a public health concern.3,4 In a recent analysis of 2018 data from the CorEvitas Psoriasis Registry, a non-interventional, prospective registry with sites across the US, 5 we showed suggestion of more severe psoriasis, more frequent concurrent comorbidity (obesity, diabetes, and hyperlipidemia), as well as less frequent treatment response to biologics among registry participants in the southcentral US. 6 We aim to better understand geographic patterns in psoriasis to discover avenues for further research into the epidemiology of the disease and to identify opportunities for regionally focused advocacy, which could ultimately improve care for patients with psoriasis.
Here, we describe regional disease characteristics for all patients enrolled in CorEvitas Psoriasis Registry from 2015-2019; additionally, we report regional biologic initiations by class (TNF-, IL-17-, IL-12/23, and IL-23-inhibitors) over that same period. Lastly, we present regional outcomes data for biologic initiations with a 6-month follow-up. The data herein provides further evidence for the possible geographic pattern of more severe psoriasis, more frequent concurrent comorbidity (obesity, diabetes, and hyperlipidemia), as well as less frequent treatment response to biologics among patients in the southcentral US.
Methods
This analysis used data from CorEvitas Psoriasis Registry, a prospective, multicenter observational disease-based registry, the design of which has been previously described. 5 Briefly, starting in 2015, adult patients diagnosed with psoriasis by a dermatologist and who are starting on or switched to an eligible systemic psoriasis treatment within the previous 12 months are enrolled. Patients complete assessments for the registry during routine dermatology visits at approximately 6-month intervals.
Patients in the current analysis included those who initiated a biologic within the 12 months prior to enrollment or at- or post-enrollment into the registry from 2015 through 2019. All initiations for all enrolled patients, those occurring both at enrollment and over follow-up, were included. Thus, patients can contribute multiple initiations to all analyses, and the unit of analysis was patient-initiation. For each patient-initiation, an index visit was defined as the enrollment visit for initiations within the 12 months prior to enrollment, and as the visit at or immediately preceding initiation for initiations occurring at- or post-enrollment. Because patients were eligible to enroll in the Registry if they initiated a biologic within the previous 12 months, for instance, some patients enrolled in 2015 the biologic initiation occurred in 2014. Two cohorts of patient-initiations were defined: (1) all patient-initiations at index, and (2) a subgroup of patient-initiations at/post-enrollment with both an index visit and a 6-month follow-up visit (5-9-month window).
Geographic Regions
Patients were categorized into 7 different geographic regions: Northeast (N East), East North Central (E North Cent), Mountain/West North Central (Mount/W North Cent), South Atlantic (S Atl), East South Central (E South Cent), West South Central (W South Cent), and Pacific (Pac). These geographic regions were derived from the 9 US census divisions, 7 with New England and Mid-Atlantic being combined into the Northeast, and Mountain and West North Central combined into Mount/W North Cent due to limited representation in these regions.
Biologic Therapy Initiations
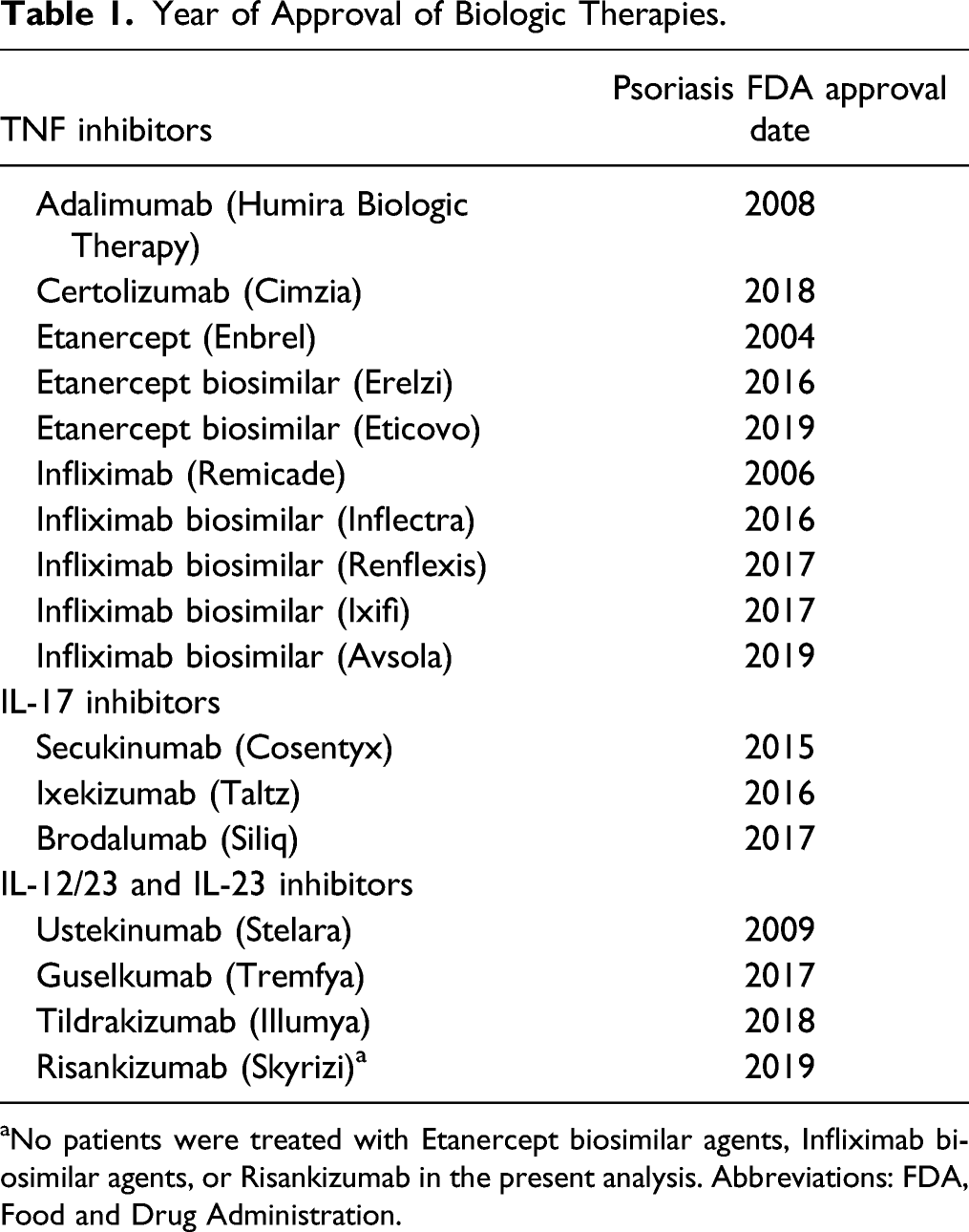
At the time of analysis, 248 US sites were actively enrolling patients (Figure 1), and biologic therapies available as of May 2019, included adalimumab, brodalumab, certolizumab pegol, etanercept, etanercept biosimilar, guselkumab, infliximab, infliximab biosimilars, ixekizumab, secukinumab, tildrakizumab, and ustekinumab (Table 1). Patient-initiations were categorized by drug class into one of three groups: (1) TNF-inhibitors (TNFi), (2) IL-17-inhibitors (IL-17i), and (3) IL-12/23 and IL-23 inhibitors (IL-12/23i and IL-23i). Distribution of CorEvitas psoriasis registry sites across the US within designated census regions. Year of Approval of Biologic Therapies. aNo patients were treated with Etanercept biosimilar agents, Infliximab biosimilar agents, or Risankizumab in the present analysis. Abbreviations: FDA, Food and Drug Administration.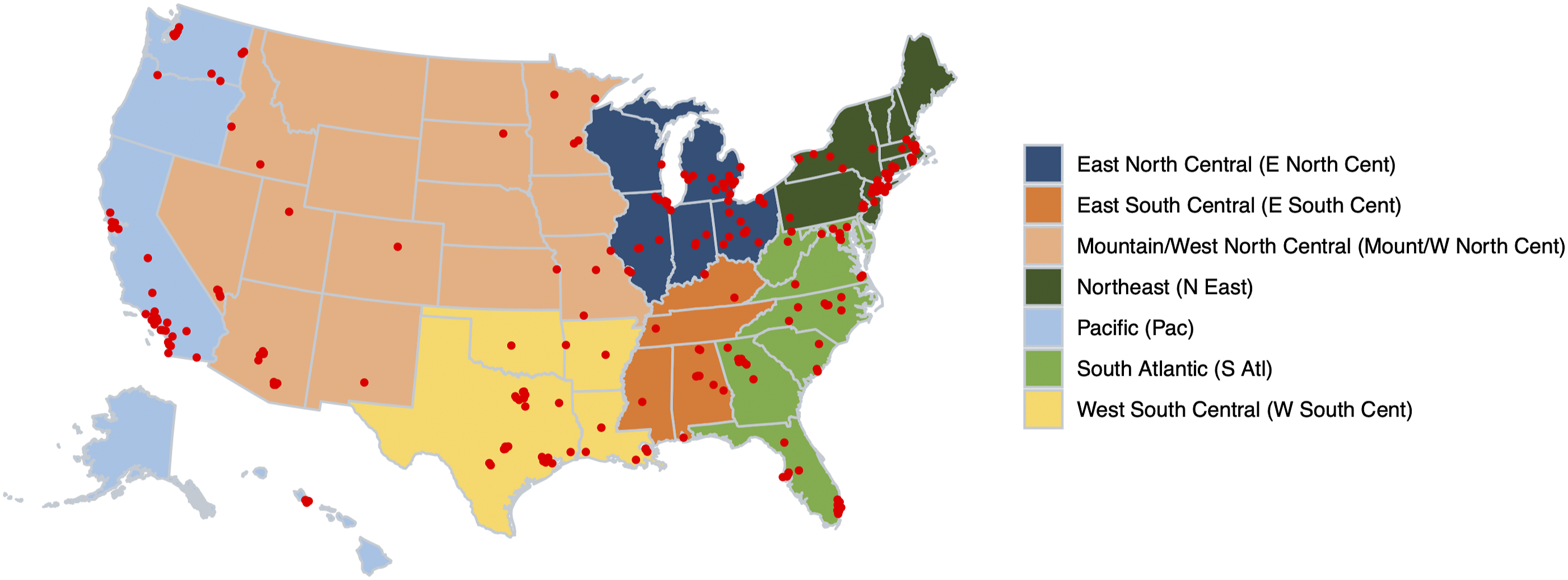
Other Variables
Data is collected at Registry visits from both patients and their dermatologists and includes demographics (age, sex, race, and health insurance type), lifestyle characteristics (Body Mass Index (BMI), smoking status, and current alcohol use), history of comorbidities (cancer, cardiovascular disease, hypertension, hyperlipidemia, diabetes mellitus, and psoriatic arthritis), treatment history (previous biologic use), and disease characteristics and patient reported outcome measures (duration of psoriasis, age at onset of psoriasis, Body Surface Area (BSA), Psoriasis Area and Severity Index (PASI), Investigator Global Assessment (IGA), and Dermatology Life Quality Index (DLQI)).
Statistical Analysis
Patient Characteristics at Biologic Initiation
Descriptive statistics were calculated for demographics, lifestyle characteristics, history of comorbidities, treatment history, and disease characteristics and patient reported outcome measures at index visit for all patient-initiations overall and within each geographic region using frequency counts and percentages for categorical variables and means and standard deviations for continuous variables. For each cofactor separately, we assessed if there was a uniform distribution of frequency or average across the geographic regions, using linear and logistic regressions for continuous and binary outcomes, respectively, using generalized estimating equations (GEE) with an unstructured covariance matrix to account for patients contributing multiple initiations. A P-value < .05 is suggestive of a distribution that is not uniform. Initiations were further stratified by the calendar year of therapy start from 2014-2019, and the proportion of total initiations within each year by drug class was reported.
Outcomes at 6 months Follow-up
In the subset of patients with a 6-month follow-up after biologic initiation, we reported treatment patterns at 6-month follow-up as the proportion of discontinuations and switches; switches to another biologic therapy were a subset of discontinuations. Targeted outcomes of PASI75, PASI90, PASI100, BSA ≤1, BSA75, IGA 0/1, and DLQI 0/1 were provided as the percentage achieving target at follow-up. For each outcome separately, we assessed if there was a uniform distribution of frequency of outcome achieved across the geographic regions, using logistic regressions with GEE with an unstructured covariance matrix to account for patients contributing multiple initiations. 8 A P-value < .05 is suggestive of a distribution that is not uniform.
Results
Patient Population
Demographics and Baseline Disease Characteristics of Patients Initiating Biologic in the CorEvitas Psoriasis Registry Overall and by US Region.
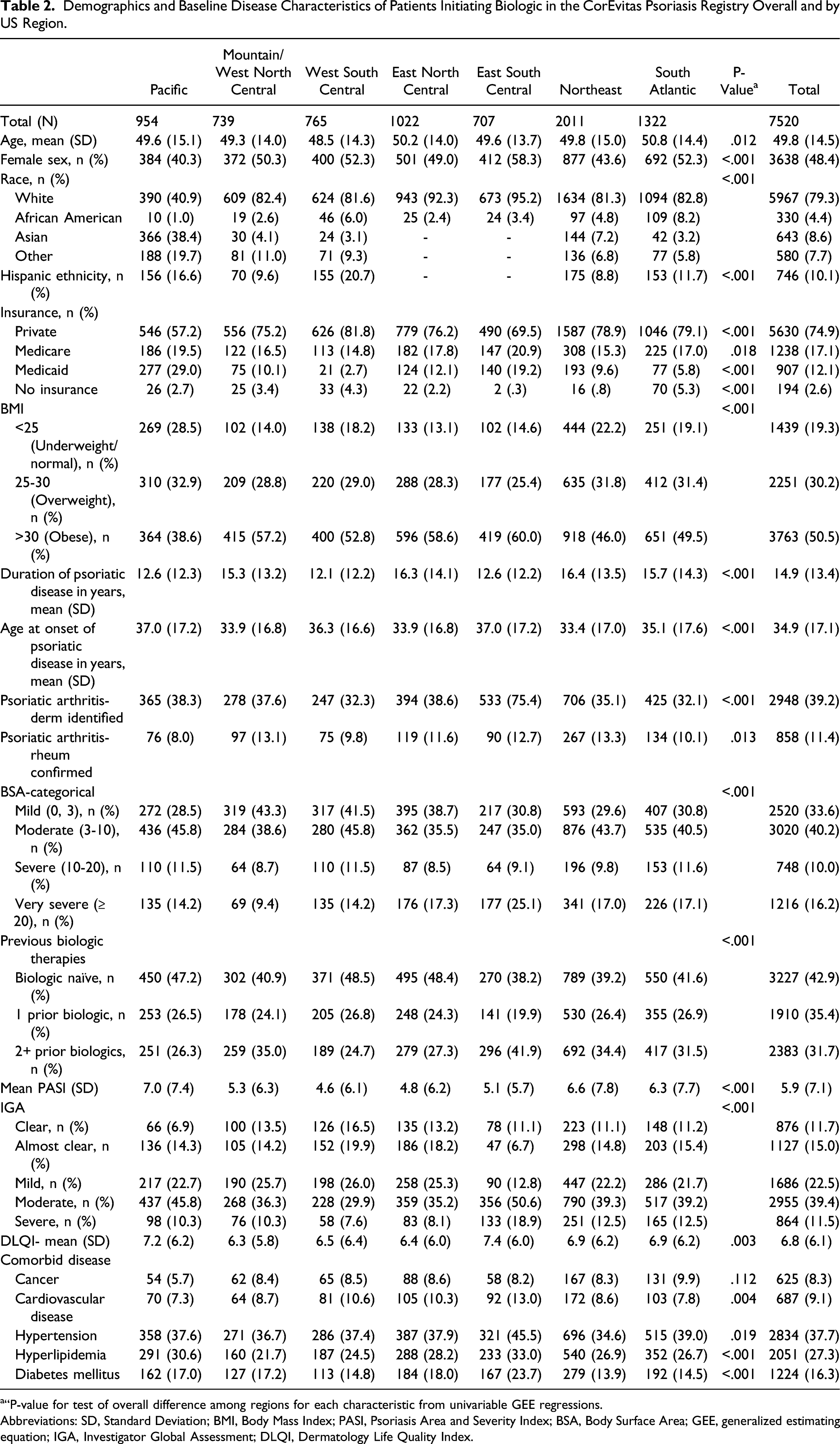
a“P-value for test of overall difference among regions for each characteristic from univariable GEE regressions.
Abbreviations: SD, Standard Deviation; BMI, Body Mass Index; PASI, Psoriasis Area and Severity Index; BSA, Body Surface Area; GEE, generalized estimating equation; IGA, Investigator Global Assessment; DLQI, Dermatology Life Quality Index.
Geographic Variation Within CorEvitas Psoriasis Registry
There were 200 active sites consisting of 13% private practices and 87% academic practices (Supplemental Table 1). The greatest proportion of patient-initiations enrolled were in the Northeast census division (26.7%) and the smallest in the Mountain/West North Central (9.8%) (Table 2). Proportions of patients identifying as White ranged from 40.9% (Pacific) to 95.2% (E South Cent). The greatest frequency of patients identifying as Asian was enrolled in the Pacific (38.4%), African American in the South Atlantic (8.2%), and Hispanic ethnicity in the West South Central (20.7%) census divisions.
Obesity was most frequently reported in the E South Cent (60%) followed by the E North Cent (58.6%). The Pacific reported the lowest frequency of obesity and the greatest proportion of underweight/normal individuals (BMI<25) (38.6% and 28.5%, respectively). Hypertension, hyperlipidemia, and diabetes mellitus were proportionally more common among patients in the E South Cent (45.5%, 33%, and 23.7%, respectively) compared to other regions.
Very severe disease (BSA >20%) was reported most frequently in the E South Cent (25.1%) with a range of 9.4-25.1% across all divisions. Psoriatic arthritis, having been confirmed by a rheumatologist, was most frequently reported in the Northeast (13.3%) and least in the Pacific (8.0%).
The greatest proportion of enrollees reporting a history of 2 + prior biologics for treatment of psoriasis at index visit was in the E South Cent (41.9%) with a range of 24.7-41.9% across all divisions. The W South Cent division reported the largest proportion of biologic naïve enrollees (48.5%), with a range of 38.2-48.5% across all divisions. Mean duration of disease ranged from 12.1 to 16.4 years with an average mean duration of disease of 14.9 years (SD: 13.4 years). Those in the Northeast (16.4) and East North Central (16.3) reported the longest duration of disease. Age at onset of disease ranged from 33.4 to 37.0 years with a mean age at onset of 34.9 years (SD: 17.1 years).
Temporospatial use of Biologic Classes in the Psoriasis Registry, 2014-2019
Overall, the distribution of biologic class initiations varied each year (Figure 2A). The general trend over time shows decrease in initiations of TNFi, steady increase in IL-17i initiations, and fluctuating initiations of the IL-12/23i and IL-23i class with more recent increases following approval of p19 targeted therapies. Trends of biologic initiations overall and by US region within CorEvitas psoriasis registry 2014-2019.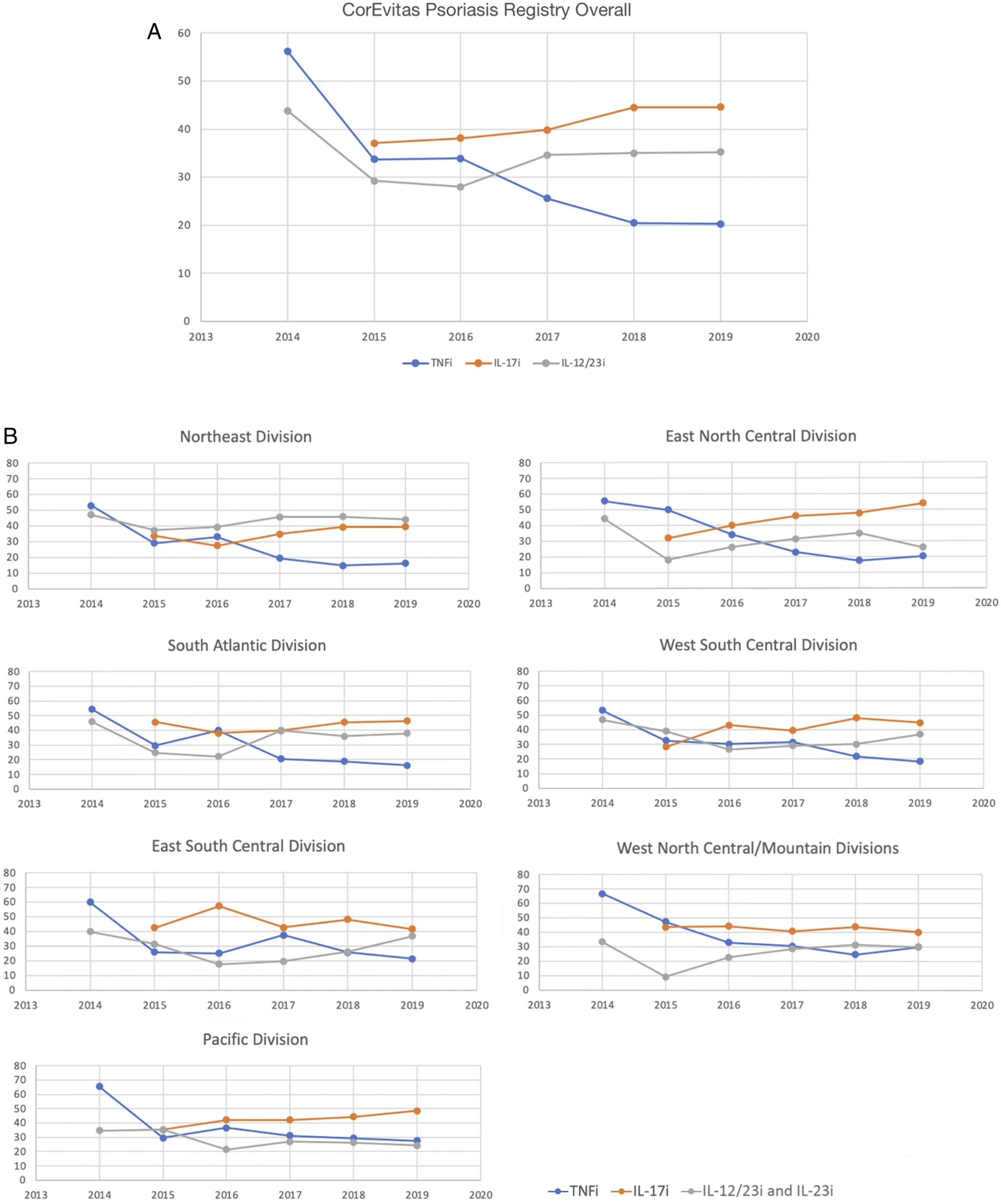
The distribution of initiated biologic class varied over time in each region (Figure 2B). Deviation from the overall trend was seen in the Northeast, where the IL-12/23i and IL-23i class was consistently initiated more frequently over the TNFi and IL-7i classes; and the Pacific where the IL-12/23i and IL-23i class was the least initiated compared to TNFi and IL-17i classes.
Geographic variation in Treatment Outcomes in the Psoriasis Registry
Outcomes 6-months Following Initiation of Biologic Among Patients in CorEvitas Psoriasis Registry Overall and by US Region.
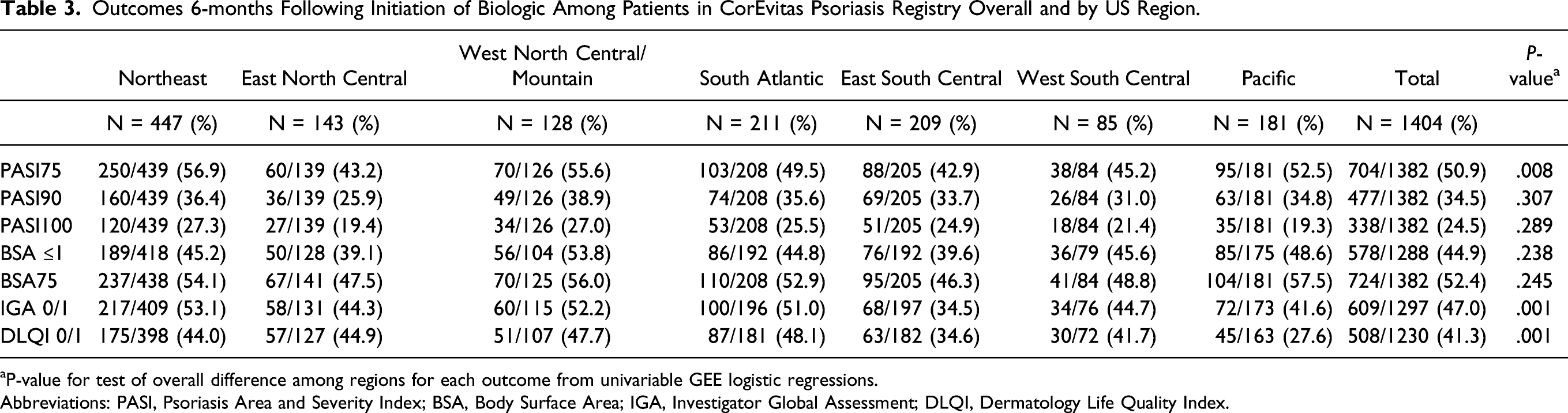
aP-value for test of overall difference among regions for each outcome from univariable GEE logistic regressions.
Abbreviations: PASI, Psoriasis Area and Severity Index; BSA, Body Surface Area; IGA, Investigator Global Assessment; DLQI, Dermatology Life Quality Index.
Overall, 41.3% reported a target DLQI 0/1 response at 6-month follow-up. The range of DLQI 0/1 response varied across regions (27.6%-48.1) (P = .001) (Table 3). Patients in the Pacific had the lowest proportion achieving DLQI0/1 (27.6%) followed by the E South Cent (34.6%).
Geographic Variation in Treatment Patterns at 6-months Following Initiation of Biologic
Across the entire registry, 15.8% had discontinued biologic therapy at 6-months, of which 11.5% had switched biologic class (Figure 3). The most commonly reported reason for altering therapy was efficacy (54.5%, data not shown). The E South Cent reported the greatest frequency of alteration in treatment (28.2%) (Range across regions: 9.4-28.2%). Proportions of patients in CorEvitas Psoriasis Registry that discontinued or switched biologic therapy within 6-months of initiation by US region.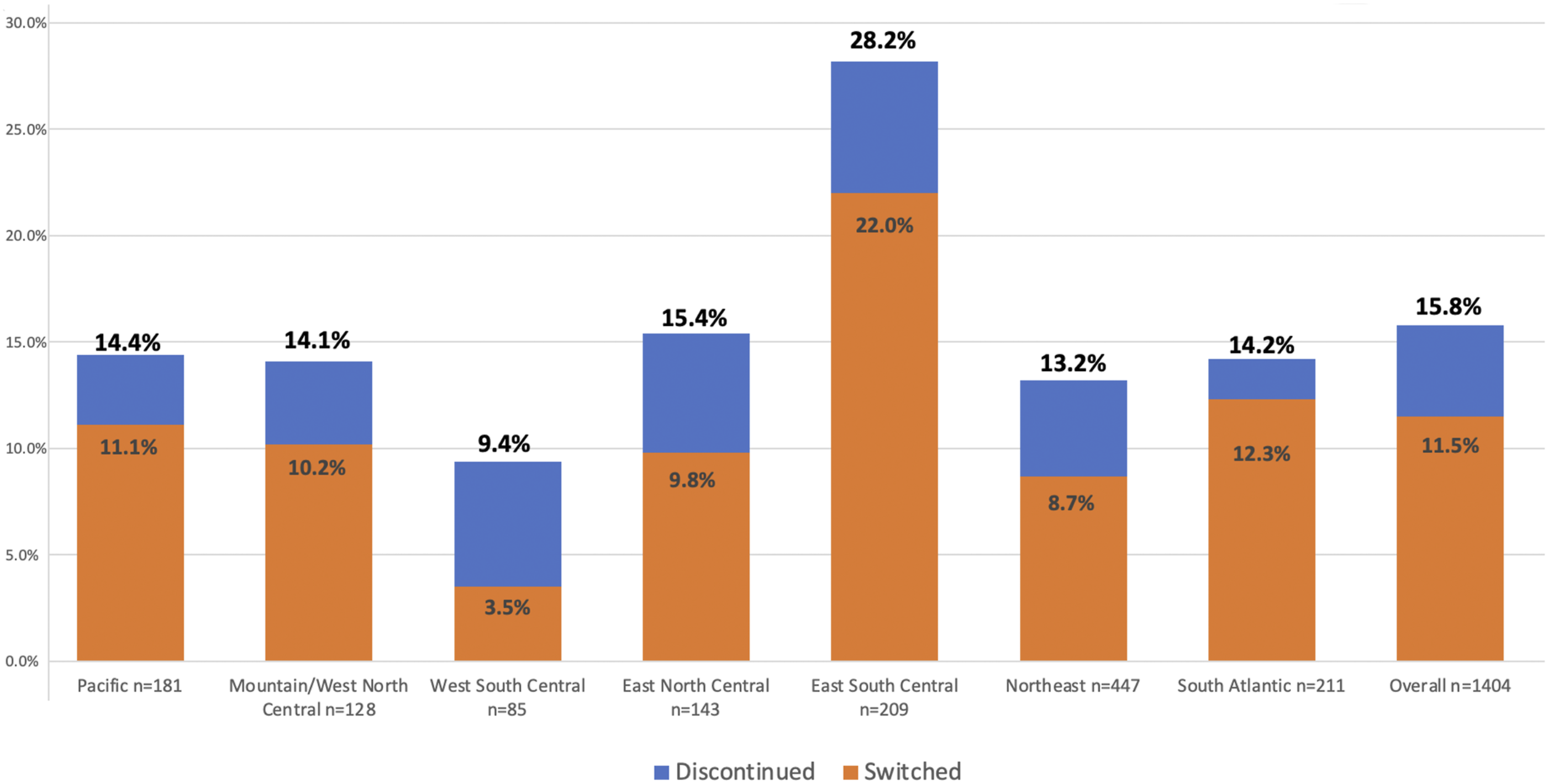
Discussion
The CorEvitas Psoriasis registry was created to provide the dermatology community with pertinent information to advance the care of psoriasis patients. 5 The registry has active sites across the US allowing for unique comparisons of patient populations located in different geographic regions.
A strong association between psoriasis and cardiometabolic disease exists and there is an established dose-response relationship between psoriasis severity and the burden of major co-morbid diseases.9-17 In concordance with these, obesity, Diabetes Mellitus (DM), Hypertension (HTN), and Hyperlipidemia (HLD) were the most frequently reported comorbid conditions in the registry overall. Further, patients in the E South Cent, who reported the greatest proportion of very severe psoriasis, reported proportionally higher frequencies of these metabolic comorbid diseases than the remaining Census divisions. In support of this geographic phenomenon, the prevalence of these cardiometabolic diseases has been shown to vary geographically among US adults in the general population, specifically with the prevalence of obesity and diabetes being significantly elevated in the E South Cent. 18
There is no current, standard algorithm for treating psoriatic disease with biologics, though experts have made recommendations for the use of various biologics based on the presence of different comorbidities.2,19,20 For example, there is weight-based dosing for both ustekinumab and infliximab when treating obese patients. 21 Despite these, it is interesting to see that by 2019, the relative proportions of biologic classes initiated were similar across the majority of US regions (IL-17i most frequently prescribed followed by IL-12/23 and IL-23 then TNFi), despite regional differences in comorbid conditions. The reasons behind this pattern in biologic use are not known, though a recent systematic review of phase III trial data shows that IL-17i medications have consistently resulted in improved outcomes (PASI 75, PASI 90, and PASI 100) when compared with IL-23 and TNF inhibitors. 22 Therefore, one possible interpretation for this pattern of biologic choice could be driven by clinical trial data. Also, initiations commonly shifted over time following Food and Drug Administration (FDA) approval of a new agent or class (Table 1).
Variation from the overall pattern of biologic class initiations seen here (decreases in TNFi use and increases in IL-17i with fluctuation in IL-12/23i and IL-23i) in the Northeast and Pacific could be driven by other influences related to payer preference, step therapy formularies, provider-familiarity with drug from participation in clinical trials, and/or a variation in insurance formularies. A recent study utilizing the Medical Expenditure Panel Survey identified regional differences in healthcare expenditures and access to biologic medications in the United States. Researchers reported the Northeast had significantly increased total health care costs per patient per year and higher ambulatory care costs, while patients in the southern US had the greatest access to biologic medications (measured by proportion of patients using biologics). 23 Similarly, another study examining claims in commercially insured patients from 2009-2013 for etanercept, adalimumab, and ustekinumab found the South census region to have the most biologic prescriptions, whereas the Northeast had the least prescriptions. 24 Finally, within the asthma literature, commercial insurance has been associated with a higher likelihood of biologic use. 25 While all patients in our analysis had access to biologics, these studies demonstrate that, overall, factors influencing prescribing patterns may vary by region across the US. Further research is needed to better understand the reasons behind variation in biologic usage and treatment outcomes.
While there was an overall pattern of biologic class initiations across the majority of US regions, our findings also suggest that the real-world response to biologics may not be universal across the US, with the current data highlighting the E South Cent. In support of this, we previously have shown that the E South Cent was less likely to achieve treatment response to biologics compared to the Northeast based on 2018 CorEvitas data. 6 The association of proportionally more severe disease, greater comorbid disease burden, and low frequencies of achieving treatment response at 6-months is a concept of great importance, especially considering that the E South Cent also reported the greatest frequency of discontinuing/switching therapy. This is complimented by our recent findings that the presence of metabolic comorbid diseases, such as diabetes, reduces odds of achieving PASI75 by 31%, independent of obesity. 26 Therefore, providers should be aware of regional trends in comorbid disease 18 and thorough assessment of concurrent comorbid disease is recommended when initiating a biologic.
The trends observed in the E South Cent are a pertinent geographic pattern to note. In 2011, Barker et al described a geographic pattern of diabetes burden in the southeastern US, deemed the diabetes belt. 3 Subsequently, it was discovered that obesity and sedentary lifestyle were among key differences separating the diabetes belt apart from other regions in the US. We suspect specific genetic and lifestyle characteristics may be enriched in the E South Cent and may influence psoriatic disease course and treatment response similar to that of the diabetes belt. Providers in all regions, but especially in the E South Cent, should consider multidisciplinary care to manage modifiable comorbid conditions to advance the care of patients with psoriasis.
While a major strength of this study is the use of real-world data, there are limitations. CorEvitas Psoriasis Registry is not a random, population-based, representative sample; the registry cohort is composed of patients invited to participate in the registry by their dermatologists. Regions are derived from the practice location, not residential addresses of patients. Some regions are underrepresented compared to others, and patients seen at participating sites may not represent all patients in the overall region. In addition, recruitment into registry is based on initiation of drugs, and the patterns of uptake should be interpreted with caution, as they may not represent fully the pattern of uptake across the country. Insurance variation and out of pocket expenses were not accounted for and may represent possible limitations. Varying exposure to ultraviolet (UV) light may have impacted results, though patients in the southeastern US, with likely more exposure to UV light, are less likely to achieve treatment response compared to the Northeast patients. It is possible that specific endemic diseases (eg, mycobacterium and endemic mycoses) may differ across regions, though there is limited evidence that these impact response to biologic therapy. Differences in response and treatment patterns are unlikely to reflect regional differences in access to care as all patients in the CorEvitas Registry have access to biologic therapies. We could not account for the potential impact of variable compliance as CorEvitas does not collect this information. Disease characteristics at index visit among patients initiating therapy prior to enrollment were measured after starting therapy and are confounded by this exposure. Initiations in the years 2014 and 2019 had only partial coverage of those years at the time of analysis. Statistical tests were not adjusted for covariates such as line of therapy, and there were no ad-hoc adjustments for multiple comparisons. Results should be interpreted cautiously.
Conclusion
Here, we describe the regional demographics and baseline characteristics of all new biologic initiations in CorEvitas Psoriasis registry and depict the use of biologics from 2014 to 2019. Over time, biologic use in most US regions within the Registry resulted in a pattern of IL-17i>IL-12/23i + IL-23i >TNFi, despite variations in geographic demographics and disease characteristics. We provide further evidence that the E South Cent region of the US, along with other regions, may be disproportionately burdened with more severe disease, comorbidity, and poorer outcomes. Providers in these regions should be aware of the greater burden of disease among the patients they care for and should employ all options for disease control.
Supplemental Material
sj-pdf-1-jps-10.1177_24755303221081799 – Supplemental Material for Geographic Patterns in Psoriasis: An Observational Study of CorEvitas Psoriasis Registry
Supplemental Material, sj-pdf-1-jps-10.1177_24755303221081799 for Geographic Patterns in Psoriasis: An Observational Study of CorEvitas Psoriasis Registry by Clinton W. Enos, Katie A. O’Connell, Ryan W. Harrison, Robert R. McLean, Blessing Dube and Abby S. Van Voorhees in Journal of Psoriasis and Psoriatic Arthritis
Footnotes
Acknowledgments
The authors thank the participating providers and patients for contributing data to CorEvitas Psoriasis Registry. This study was supported through a partnership between CorEvitas Psoriasis Registry and the National Psoriasis Foundation Medical Board.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by CorEvitas (formerly Corrona), LLC, and the analysis was funded by CorEvitas LLC. Access to study data was limited to CorEvitas, and CorEvitas statisticians completed all of the analysis; all authors contributed to the interpretation of the results. CorEvitas has been supported through contracted subscriptions in the last 2 years by AbbVie, Amgen, Arena, Boehringer Ingelheim, Bristol Myers Squibb, Celgene, Chugai, Eli Lilly and Company, Genentech, Gilead, GSK, Janssen, LEO, Novartis, Ortho Dermatologics, Pfizer Inc., Regeneron, Sanofi, Sun, and UCB.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.