
Abstract
Background
In order to apply current treatment recommendations for psoriatic arthritis (PsA), a complete assessment of psoriatic disease domains must be completed by the clinician. This includes a musculoskeletal examination (including tender and swollen joints, dactylitis, enthesitis, and axial disease) as well as skin and nail examination. Documentation in the clinician’s note serves as a proxy for disease assessment.
Objective
To explore differences in documentation of psoriatic domains between PsA specialist and general rheumatologists at 2 academic centers.
Methods
We identified PsA patients seen by either general rheumatologists or by PsA combined clinic specialist providers at 2 established PPACMAN (Psoriasis and Psoriatic Arthritis Clinics Multicenter Advancement Network) sites. Records were assessed for the presence (and extent) of documentation for musculoskeletal and cutaneous PsA domains. We also examined accuracy of ICD coded diagnoses to understand the extent to which discrete data from the electronic medical record can be used to evaluate completeness of assessment.
Results
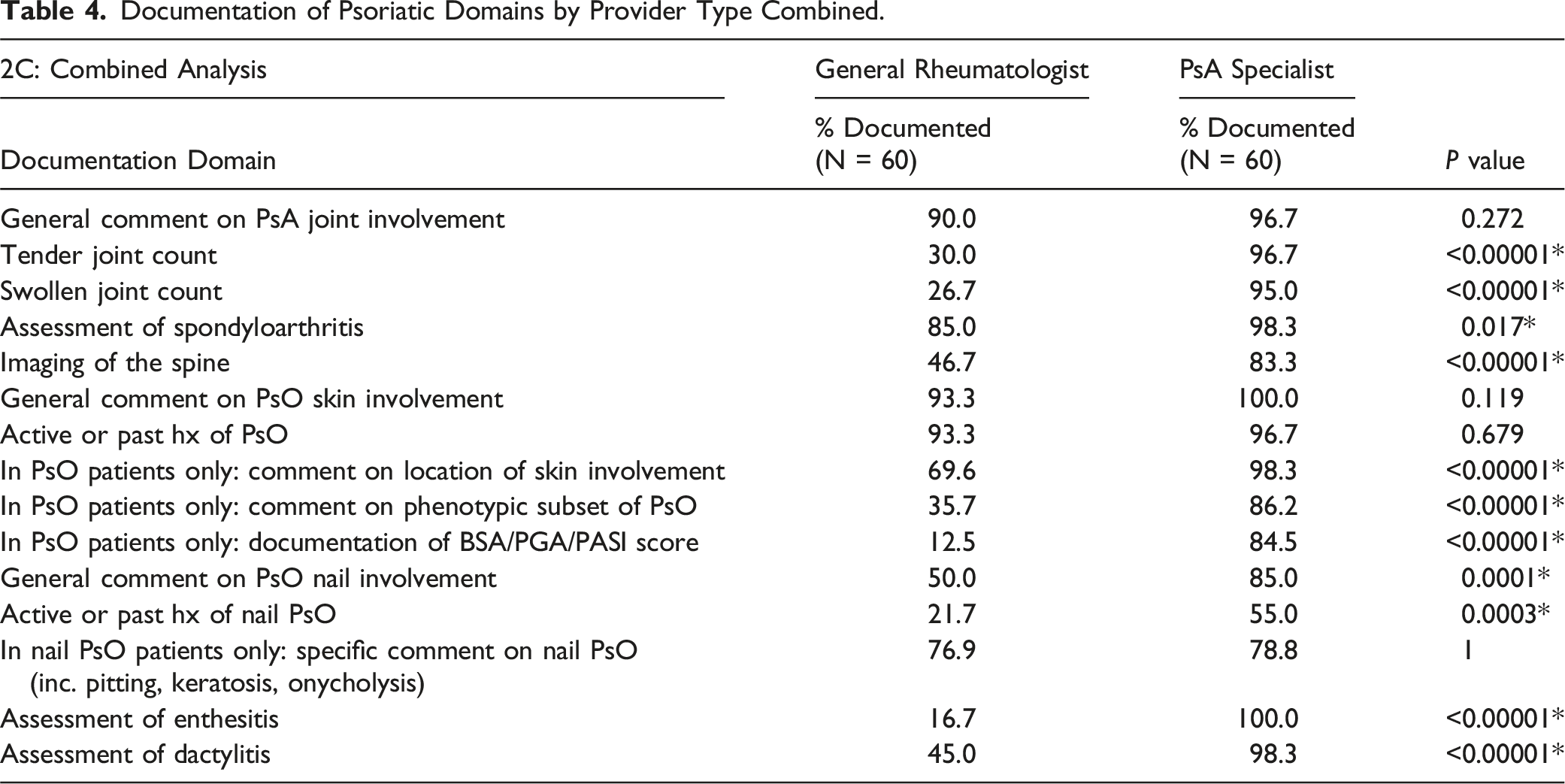
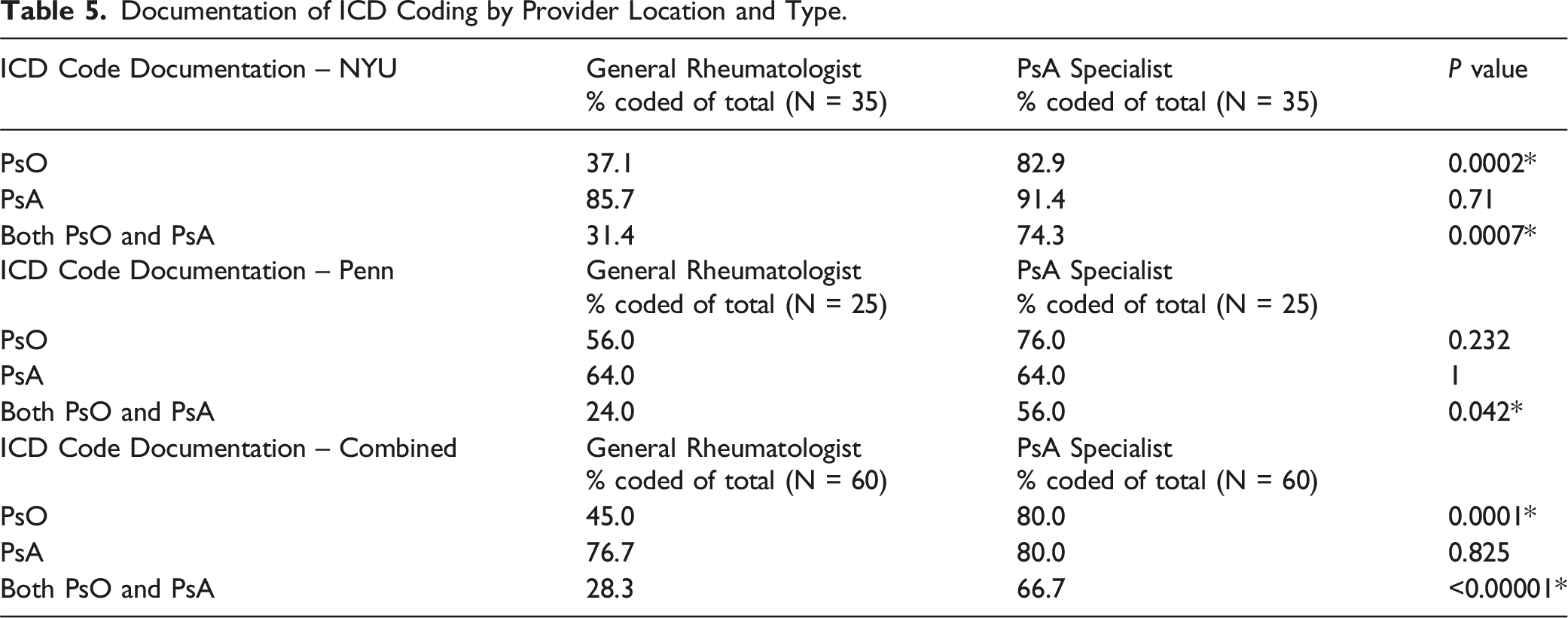
PsA combined clinic specialist providers documented disease domains significantly more consistently compared to generalists, including tender and swollen joint counts (P < 0.001), assessment of spondyloarthritis (P = 0.017), and presence/extent of skin involvement (P < 0.001). Additionally, PsA specialists more consistently coded for both psoriasis (PsO) and PsA.
Conclusions
In this multicenter, retrospective study, compared to generalists, PsA combined-clinic specialist providers more thoroughly documented both musculoskeletal and cutaneous psoriatic disease domains and ICD coding of PsO for patients, highlighting gaps in assessment and documentation. These findings underscore the need for improved training in psoriatic disease assessment and simplified modalities for documentation.
Keywords
Introduction
Psoriatic arthritis (PsA) is a complex, chronic inflammatory condition with heterogeneous clinical features and is characterized by 6 domains: peripheral arthritis, axial disease, enthesitis, dactylitis, skin and/or nail psoriasis (PsO).1,2 Complete assessment and documentation of these domains in PsA poses a challenge for busy clinicians (including rheumatologists, dermatologists, internal medicine and primary care providers). 2 Despite advancements in drug development, including combination strategies with conventional synthetic and biologic disease modifying anti-rheumatic drugs (DMARDs), the multiple pathways involved in the synovio-entheseal inflammation make PsA a difficult disease to treat. Selecting optimal pharmacologic therapy remains a challenge for providers, but is critically important for patients, as early intervention with immunomodulating or anti-inflammatory drugs is known to improve clinical and radiographic outcomes. 3 One approach to tackling this heterogenous disease is the creation of combined-rheumatology-dermatology centers (ie, PPACMAN centers, ), 4 where collaborative efforts encourage assessment of psoriatic disease in a standardized manner.
To develop an optimal treatment plan, a comprehensive patient assessment is essential. Beyond individual care, accurate documentation and coding are crucial for leveraging electronic health record (EHR) and administrative claims data to study treatment patterns, optimize therapy selection, and apply artificial intelligence in clinical decision-making. Structured documentation (ICD codes) and unstructured documentation (text notes) help identify patient characteristics associated with treatment response. However, few studies have explored how documentation and coding practices vary between disease specialists and generalists, highlighting a gap in understanding their impact on research and clinical outcomes.
We aimed to assess for differences in how PsA specialty clinicians vs general rheumatology clinicians document psoriatic arthritis assessments and whether physicians vary in their use of ICD-10 codes for PsO, PsA, or both. The objective of this study was to investigate variability in documentation of psoriatic domain assessment and ICD coding between PsA specialist rheumatologists working in combined rheumatology-dermatology centers (ie, Psoriasis and Psoriatic Arthritis Clinics Multicenter Advancement Network (PPACMAN) Centers), 4 and general rheumatologists, using 2 cohorts of providers and patients at NYU Langone Health (NYU) and University of Pennsylvania Health (Penn). Given their specific focus on psoriatic disease investigation and research endeavors, 5 we hypothesized that PsA specialists would more thoroughly and consistently capture psoriatic disease domains in the EHR compared to general rheumatologists.
Methods
Data Source and Patients
For NYU, this study was approved by the NYU Institutional Review Board (IRB# s20-00084) with waived written consent from individual participants as all data were collected in a de-identified manner. For Penn, this study was approved by the University of Pennsylvania Health Institutional Review Board with IRB exemption for the use of de-identified secondary data (IRB# 854072).
Data was obtained from the EHRs of NYU and Penn via chart review. PsA patients with a confirmed ICD 9 or 10 PsA code who were seen in-person from 01/01/2023 to 09/01/2023 were selected from each clinical site and classified as assessed by either a PsA specialist or a general rheumatologist. Patients seen in PPACMAN clinics were assessed by rheumatology providers with specific expertise in evaluating psoriatic skin involvement, gained through frequent collaboration with dermatology colleagues. All assessments were conducted solely by the rheumatologist—whether in the PPACMAN clinic or a general rheumatology setting—without involvement from a dermatologist.
To reach a desired number of patients in each group, patient records were selected in a consecutive, retrospective manner, with follow up visits beginning on 09/01/2023 and moving backward towards 01/01/2023. Qualifying patients had at least 2 in-person outpatient visits within the EHR (one baseline visit, and one follow up visit with the same rheumatology provider). The baseline visit was defined as the first clinical interaction with the NYU or Penn health systems regardless of timepoint in PsA disease duration or treatment.
Data Collection
Data extraction from the EHR was performed on the patient’s baseline visit with their respective rheumatology provider. Data from both institutions were collected in a de-identified manner to ensure patient confidentiality. Demographics were collected from each patient, including age, sex, race, ethnicity, date seen by provider, provider location, and provider type (general rheumatologist or psoriatic disease specialist). Assessment for documentation was based upon whether or not the practitioner commented on features of psoriatic disease during the standard of care encounter anywhere within the confines of their note. These features included: tender joint count (TJC), swollen joint count (SJC), spondyloarthritis, dactylitis, and enthesitis. Cutaneous domains included assessment of skin involvement, location, phenotype, percentage of body surface area (%BSA) affected and nail psoriasis. Case definitions for documentation variables were created in conjunction with PsA specialists from both institutions to ensure consistency of data retrieval (Supplemental Methods Table 1).
Data was additionally collected on ICD billing codes selected as the primary diagnoses for the encounter, including for PsO, PsA, or both. REDCap was used to record documentation of disease domains and ICD coding, one for NYU patients and one for Penn patients. Two investigators performed data extraction from the EHR into REDCap, one for each site. Once data collection was complete, it was securely exported from REDCap and combined from both institutions to create a unified dataset in Excel.
Data Analysis
Demographic data was descriptively reported. Fisher exact tests were performed to evaluate the relationships between documentation of psoriatic disease variables and ICD coding across provider type within the dataset, with analyses for NYU, Penn, and both institutions combined. Type 1 error was set at 0.05. We did not correct for multiple testing as this included only descriptive data.
Results
Demographics for NYU, Penn, and Overall Patient Populations.
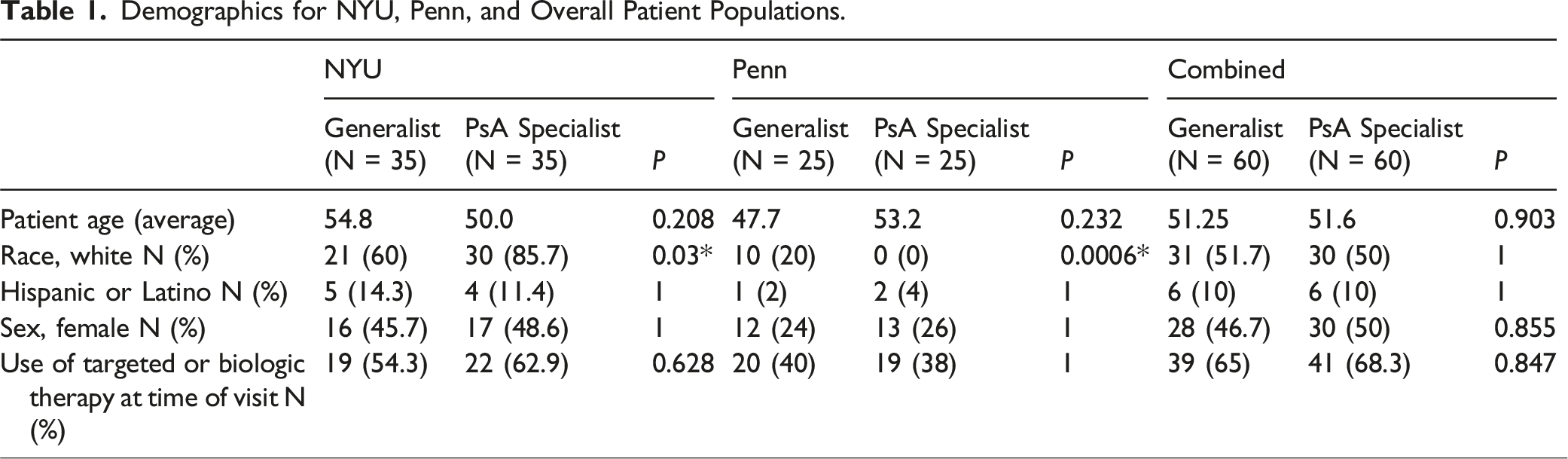
There were no significant differences in demographic variables including patient age (P = 0.208, 0.232, 0.903), Hispanic or Latino (P = 1, 1, 1), female sex (P = 1, 1, 0.855), or use of biologic or targeted therapy at time of visit (P = 0.628, 1, 0.847) for patients seen by general rheumatology vs PsA specialist providers, respectively for NYU, Penn, and as a whole (Table 1). The PsA specialist group had significantly more patients with white race at NYU (85.7% vs 60%, P = 0.03) and Penn (20% vs 0%, P = 0.0006), though not significantly different overall (51.7% vs 50%, P = 1).
Documentation of Psoriatic Disease Domains by Provider Type
Documentation of psoriatic disease domains was compared between general and PsA specialist rheumatologist providers.
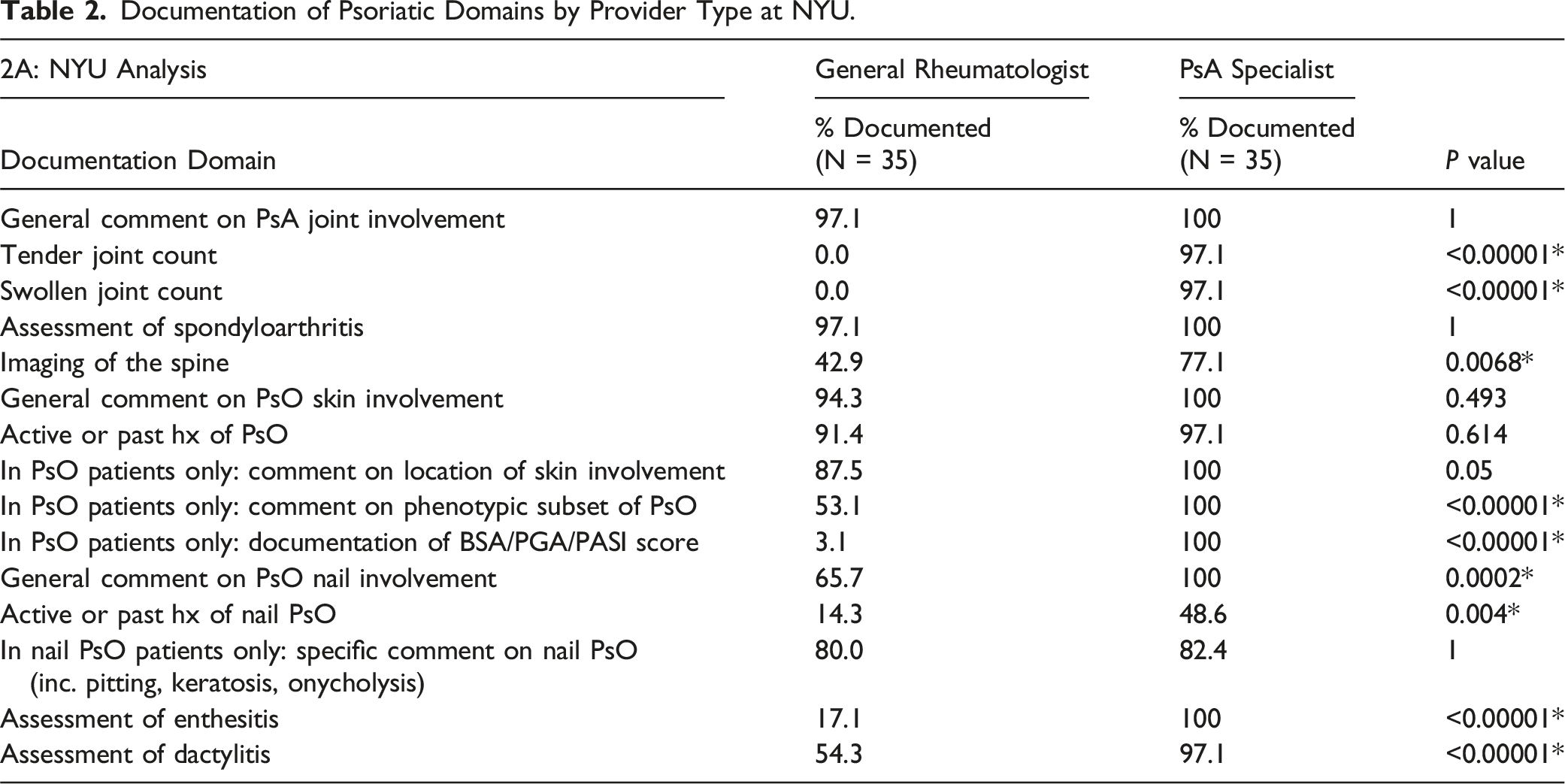
Documentation of Psoriatic Domains by Provider Type at NYU.
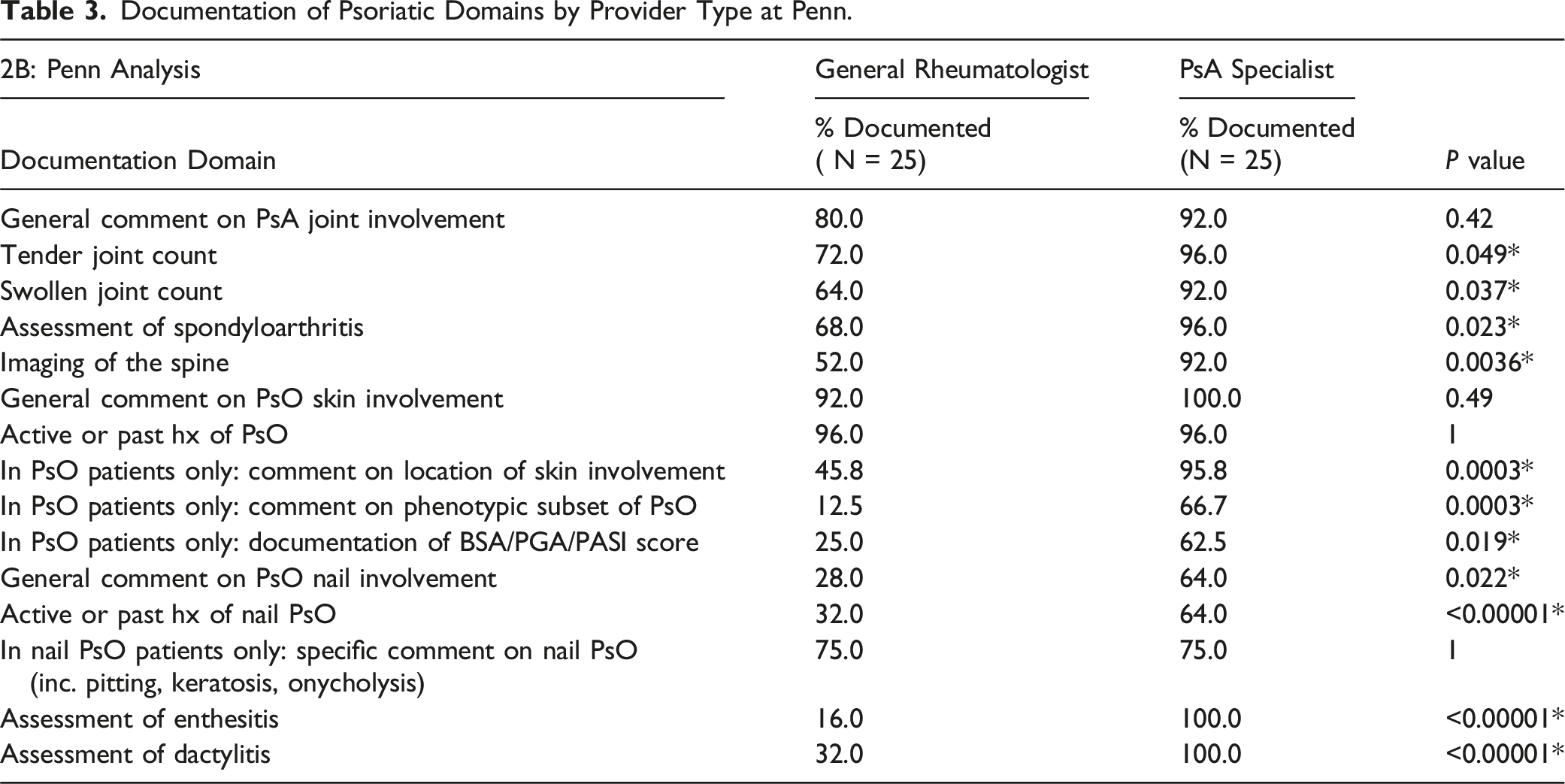
Documentation of Psoriatic Domains by Provider Type at Penn.
Documentation of Psoriatic Disease Domains Overall
Documentation of Psoriatic Domains by Provider Type Combined.
ICD Coding of Psoriatic Disease between Providers
Documentation of ICD Coding by Provider Location and Type.
Discussion
In this retrospective study, PsA combined-clinic specialist providers documented psoriatic disease domains more frequently than general rheumatologists. In the combined analysis of 2 academic institutions, specialists more consistently recorded 11 out of 15 disease variables, encompassing both musculoskeletal and cutaneous domains. General and specialist providers similarly documented general comments on joint and skin involvement, history of skin PsO, and specific comments on nail PsO. Differences were observed in the documentation of musculoskeletal domains, including numerical tender- and swollen-joint counts, spondyloarthritis assessment, spinal imaging, and evaluation of enthesitis and dactylitis. These differences may reflect variations in patient populations, clinical focus, and familiarity with comprehensive PsA assessments between provider types.
Diagnosis and management of PsA is challenging given the heterogeneity of disease presentation and lack of diagnostic biomarkers. 6 The provider’s initial diagnostic impression and treatment plan requires thorough evaluation of both musculoskeletal and skin domains to characterize the extent of psoriatic disease and choose appropriate therapies. Assessment of psoriasis varied between provider groups in this study, with less documentation of nail PsO and psoriasis severity scores such as BSA, PGA, and PASI. Given that psoriatic skin and nail disease significantly impacts patient morbidity, its evaluation and documentation remain important considerations in guiding treatment decisions. 7 This reflects room for improvement in rheumatologic assessment of skin disease. We also observed rather large disparities in musculoskeletal domain documentation, especially for enthesitis and dactylitis, which are hallmark features of PsA. 2 The lack of documentation for enthesitis and dactylitis in PsA by general rheumatology providers may also suggest the need for more thorough trainee education during fellowship and beyond. 8
Noticeably, while this study utilized documentation as a proxy for disease assessment, EHRs may not always accurately reflect the physician’s full clinical evaluation, which could have been more thorough in practice. This limitation may partly explain differences in the documentation of domains such as tender and swollen joint counts, enthesitis, and dactylitis between specialist and generalist providers. Generalist providers, even when conducting thorough assessments, may document these findings less explicitly than specialists with a focused interest or research background in psoriatic disease.
When evaluating ICD code documentation, we found that specialists were more complete and thorough in ICD documentation in the EHR. This finding is particularly relevant for studies relying on EHR or administrative claims data, as it highlights the presence of informative missing data – and that this missing data is not evenly distributed across all providers. Use of such data remains valuable for research; therefore it is essential to account for this informative missingness and its potential impact on study findings.
Limitations
This study was limited by a relatively small sample size (n = 120). Additionally, our study included only patient-providers from academic medical centers, which given the nature of this environment, may see a more specialized population of patients compared to non-academic centers in the community. The retrospective nature of this analysis is, similarly to all observational studies, susceptible to inherent biases.9,10 Data collection for each cohort was performed by 2 separate but trained individuals, which at least partially mitigates the biases that would arise from a single data collector. Patient reported outcome (PRO) measures, such as HAQ-DI, PsAID, patient global assessments, and QoL indices, were not systematically collected across this cohort and therefore were not included in this study. Future studies may seek to evaluate differences in standardized collection of PROs for both general rheumatologists and combined-clinic PsA specialists.
Conclusions
Our study highlights the unmet need for a streamlined approach to assessment and documentation that fully captures the disease state in patients with psoriatic disease. Comprehensive assessment of current disease state was under-captured in patients seen in general rheumatology practice. Despite significant efforts from multiple organizations, patient advocacy foundations and academics to increase awareness, improvement in both assessment and documentation are still needed. Enhanced educational efforts and easier methods of psoriatic disease assessment and documentation could improve clinician confidence in assessing PsA domains as well as research in the field that relies on claims data.
Supplemental Material
Supplemental Material - Gaps in Documentation of Psoriatic Domains in General Rheumatologic Practices Compared to Rheumatology-Dermatology Combined Clinics
Supplemental Material for Gaps in Documentation of Psoriatic Domains in General Rheumatologic Practices Compared to Rheumatology-Dermatology Combined Clinics by Rice AL, Gillespie S, Sai N, Reddy SM, Merola JF, Haberman RH, Ogdie A, Scher JU in Journal of Psoriasis and Psoriatic Arthritis
Footnotes
Acknowledgements
We are grateful to the Departments of Medicine at NYU Langone Health and University of Pennsylvania Health for their support and resources.
Author Contributions
ALR, SG, RH, AO, and JUS contributed to conception of this original manuscript, interpretation of data, and writing the manuscript. All authors reviewed and approved the final version of the manuscript.
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ALR, SG, and NS declared no potential conflicts of interest with respect to the research, authorship or publication of this article. SMR has served as a consultant for BMS, Johnson & Johnson, Novartis and UCB. JFM is a consultant and/or investigator for Amgen, Astra-Zeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Abbvie, Dermavant, Eli Lilly, Moonlake, Novartis, Janssen, Oruka, UCB, Sanofi, Regeneron, Sun Pharma, Biogen and Pfizer. RHH has served as a consultant for Johnson & Johnson and Novartis. AO has served as a consultant for Abbvie, Amgen, BMS, Celgene, CorEvitas, Gilead, GSK, Janssen, Lilly, Novartis, Pfizer, Spyre, Takeda, TREG, and UCB and has received grants from Abbvie to Penn, Amgen to Forward/NDB, BMS to NDB/Forward, Janssen to Penn, Novartis to Penn, Pfizer to Penn, UCB to Penn. JUS has served as a consultant for BMS, Johnson & Johnson, Novartis, Pfizer, and UCB; he received research funding from Johnson & Johnson.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by NIH/NIAMS (1UC2AR081029 to Scher, R01AR084274 to Scher, 1K23AR082955 to Haberman, 3UC2AR081039-02S1 to Haberman, T32-AR-069515 to Scher), NYU Colton Center for Autoimmunity, The National Psoriasis Foundation, The Beatrice Snyder Foundation, The Riley Family Foundation, and PPACMAN Fellowship Grant.
Ethical Statement
Informed Consent
This study with waived written consent from individual participants as all data were collected in a de-identified manner.
Data Availability Statement
Data may be made available upon request to the authors. Supplementary methods with case definitions for each documentation domain utilized in this study are available online to accompany this publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.