
Abstract
Despite advancements in psoriasis therapeutics, biologic discontinuation and switching still happen frequently, with the most common reasons being lack of efficacy or treatment intolerance. Conventional teaching has been to switch out of the class (inter-class switching) for primary non-responders and to stay in the class (intra-class switching) for secondary non-responders. Previous real-world studies have reported success with intra-class switching within the IL-17 inhibitor class, but data have been limited to secukinumab, ixekizumab, and brodalumab. Using retrospective data from cases selected for moderate-to-severe psoriasis who failed prior IL-17 therapy, we report our real-world experience using bimekizumab in 50 patients who failed a prior IL-17 inhibitor, in which 82% achieved an IGA 0/1. By demonstrating achievement of stringent benchmarks, such as IGA 0/1 and sPGAxBSA 100 in these selected patients, we challenge the conventional teaching of primary vs secondary non-responders class switching, and have found bimekizumab to be a viable option in those who have failed IL-17 inhibitor therapy in the past.
Background and Purpose
Psoriasis is a chronic, systemic, inflammatory skin disorder with an estimated global prevalence of 2-4%. 1 The burden of uncontrolled psoriasis has been well described, with an impact on quality of life comparable to cancer and chronic lung disease. 2 Studies have shown higher levels of skin clearance to be positively correlated with various quality-of-life measures. 3 While advancements in psoriasis therapeutics have led to significant levels of skin clearance, many patients still struggle to achieve or maintain complete skin clearance. Several guidelines have been published on treatment sequencing after initial biologic failure, with the general recommendation to stay within the class for secondary non-responders (loss of initial efficacy) while switching out of the class for primary non-responders (eg, < PASI 50). 4 Most phase 3 trials have excluded patients exposed to the same drug class under study (eg, prior failure to an IL-17 inhibitor would exclude a patient from an investigational study with another IL-17 inhibitor). Bimekizumab is a humanized IgG1 antibody that selectively targets IL-17 A/F and is approved for adults with moderate-to-severe plaque psoriasis and active psoriatic arthritis.14-19 In their phase 3 development program, 53% of patients had prior IL-17 inhibitor experience.14-17 However, exposure to a medication does not necessarily mean treatment failure or intolerance; therefore, one cannot extrapolate these results to real-world patients who have failed a prior IL-17 inhibitor. Moreover, clinical trials are highly regulated with strict inclusion and exclusion criteria, which oftentimes leads to a population that doesn’t accurately reflect the heterogeneity of our real-world clinical practice. To that end, we report our real-world experience using bimekizumab in patients who failed a prior IL-17 inhibitor to demonstrate efficacy, safety, and tolerability in this difficult-to-treat population.
Research Design
We conducted a multicenter, retrospective study of adult patients who failed a prior IL-17 inhibitor and were treated with bimekizumab. Patients were identified from practice data using ICD-10 codes corresponding to psoriasis and a documented history of treatment failure with an IL-17 inhibitor. Patient consent to be included in this study was obtained at a subsequent encounter. Those on multiple systemic therapies for concurrent immune-mediated disorders were excluded due to the difficulty of assessing treatment tolerability and safety. Patients treated with other biologic classes were also included in this analysis as long as they had failed a prior IL-17 inhibitor (eg, patients did not have to be treated with an IL-17 inhibitor immediately before switching to bimekizumab). Of these patients who had failed a previous IL-17 inhibitor, 2 patients were on another (Guselkumab or Adalimumab) immediately prior to initiation of bimekizumab.
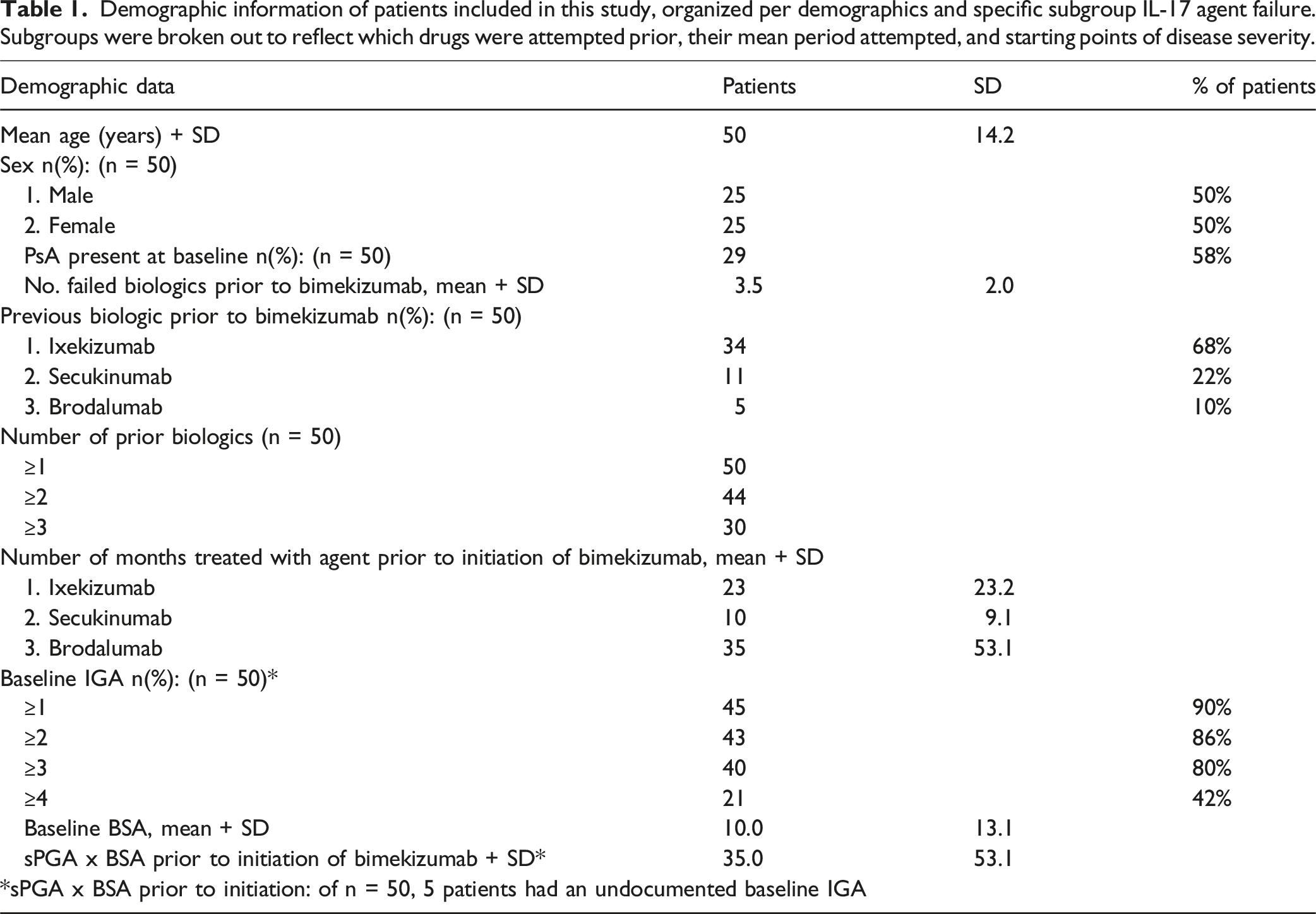
Demographic information of patients included in this study, organized per demographics and specific subgroup IL-17 agent failure. Subgroups were broken out to reflect which drugs were attempted prior, their mean period attempted, and starting points of disease severity.
Data Analysis and Results
Baseline demographics, prior treatment history, and treatment response with bimekizumab are summarized in Figure 1. Fifty patients met the inclusion criteria, with 50% female and a mean age of 50 years (range: 18-77 years). 29/50 of patients had clinician-diagnosed concomitant psoriatic arthritis, of which 4 patients were evaluated by rheumatology as well. Patients were treated with an average of 3.5 biologics before initiating bimekizumab. The average treatment duration on a previous IL-17 inhibitor was 16.8 months, with the most common reason for switching being a partial responder or secondary non-responder. The average duration of time on bimekizumab was 11.5 months. 43/50 patients had improved skin clearance after switching to bimekizumab, with 82 % achieving IGA 0/1. 9/50 of patients had persistent scalp involvement at the time of the switch to bimekizumab, with 5 of these patients eventually achieving either partial or complete scalp clearance. 7 patients switched to bimekizumab due to uncontrolled psoriatic arthritis, in which 4 patients experienced improvement in joint symptoms. One patient reported worsening back, hip, wrist, and hand pain after starting bimekizumab, which improved after switching to a combination of adalimumab and deucravacitinib. Comparison of groups with prior IL-17 failure (Ixekizumab, Secukizumab, Brodalinumab) and their achieved sPGAxBSA improvement at 16 weeks of total Bimekizumab treatment.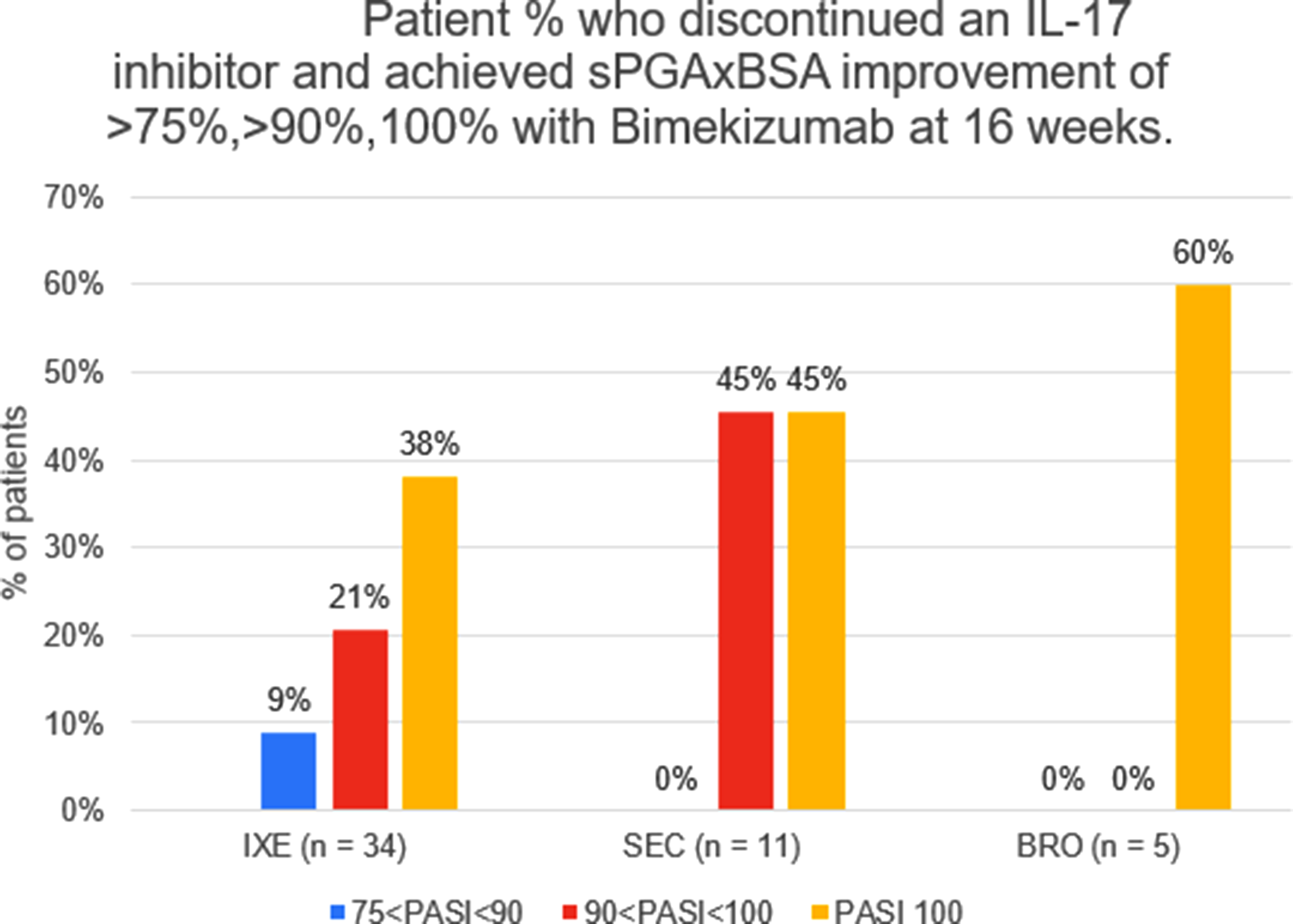
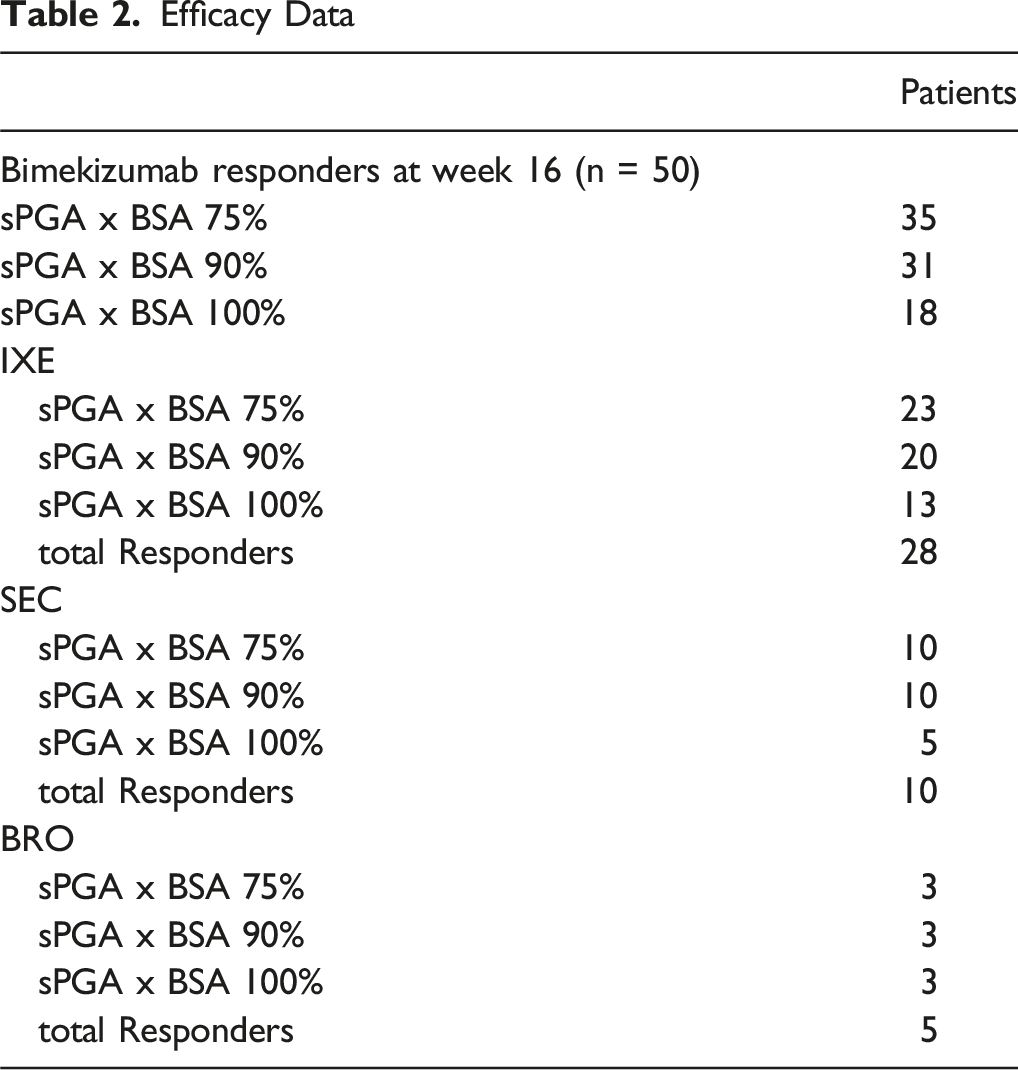
Treatment response to bimekizumab based on IL-17 inhibitor failure type is summarized in Figure 2. Given the non-uniformity in how treatment failure was defined amongst the investigators, one cannot draw any conclusions on treatment response based on treatment failure type. Still, our data demonstrate that in those who were primary failures, secondary failures, and partial responders to an IL-17 inhibitor, 100%, 81%, and 71% achieved sPGAxBSA of 75%, respectively (Table 2). Comparisons of sPGAxBSA achivements on the basis of prior therapy failure type (primary vs secondary vs partial). Efficacy Data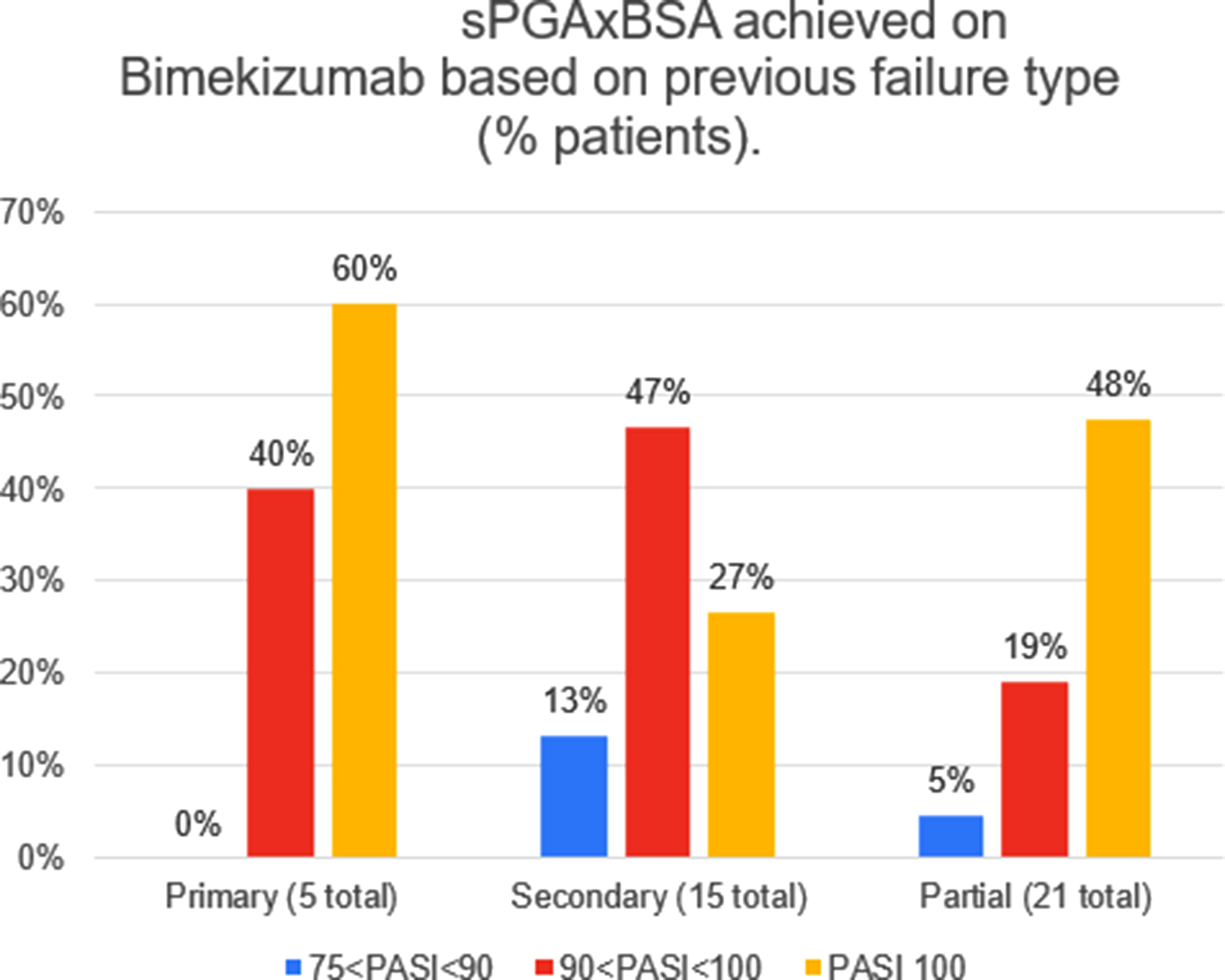
Adverse Events on Bimekizumab

Conclusion
Guidance on treatment sequencing after initial biologic failure remains highly relevant given the unexpectedly high drug discontinuation and switching rates reported with even our most effective psoriasis therapies. 5 Switching to another class (inter-class switching) has been the preferred approach for non-responders, but there may be compelling reasons to stay within the class, particularly to treat comorbid diseases such as psoriatic arthritis. Furthermore, studies have shown that there can be notable differences in binding affinity, epitope surface area, half-life, and immunogenicity amongst biologics within the same class, which may have implications on treatment efficacy and safety. 6 In the phase 3b/4 BE RADIANT study, bimekizumab demonstrated superiority over secukinumab in PASI 100 achievement at 16 weeks. 7 In addition, 79% of patients who were PASI 90 non-responders on secukinumab at 48 weeks achieved this stringent endpoint after switching to open-label bimekizumab after 48 weeks of treatment. 8
Several published studies have reported intra-class switching with IL-17 inhibitors, including secukinumab to ixekizumab, 9 and secukinumab and/or ixekizumab to brodalumab. 10 More recently, Sood et al 11 published a 52-week real-world study of bimekizumab in a Canadian cohort, which included 59 patients with prior IL-17 inhibitor exposure. While 76.6% (23/30) of these patients achieved an IGA 0/1 after switching to bimekizumab, this study did not differentiate prior experience vs prior failure to an IL-17 inhibitor.
Our study has several notable strengths. Patients were collected from various practice settings, ranging from independent private practices to larger group practices and academic centers across different geographic regions. All authors in the study specialize in psoriasis, so clinical outcomes were meticulously documented. While not specifically assessed for, our study also captured efficacy data in special site areas, including scalp and genital psoriasis, as well as psoriatic arthritis. Finally, we included patients who were non-responders to brodalumab, which has been widely considered to be the most effective treatment for multiple biologic failures. 12
Our study also has limitations. The definition of primary non-responder, secondary non-responder, and partial responder was not standardized amongst investigators and was left open to their interpretation. Therefore, response rates based on prior treatment failure type should be interpreted with caution. Laboratory tests were not consistently collected, and there may be differences in how patients were screened for suicidal ideation and behavior and inflammatory bowel disease. Additional patient selection metrics such as age, gender and ethnicity were not collected as this was not central to the studies central focus but does overall pose a limitation on the study. Treatment duration on bimekizumab is also limited, so one cannot conclude how durable, safe, and well-tolerated bimekizumab would be with longer drug exposure. Finally, a BSAxPGA composite was used to measure disease severity and treatment response rather than a psoriasis area severity index (PASI) score, which is the standard in clinical trials. However, several studies have validated the utility of a BSAxPGA composite as a proxy for PASI in the real world. 13
Collectively, our data demonstrate that even in a treatment-refractory population that was enriched for prior IL-17 inhibitor failure, bimekizumab is a viable treatment option. This adds to the growing body of literature on biologic switching and provides clinicians with another set of data points to optimize the management of patients who have inadequately responded to an IL-17 inhibitor.
Footnotes
Ethical Considerations
Our institutions collectively do not require ethics approval for reporting of multicenter retrospective reviews based on secondary analyses. Consent was obtained verbally during patient encounters - no additional consents were required.
Author Contributions
All authors have contributed to the data generation, analysis, writing, and critical review of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declarations of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: