
Abstract
Introduction
Psoriasis (PsO) and psoriatic arthritis (PsA) are chronic inflammatory conditions treated with primarily immune-modulating medication. However, interest is growing in gut microbiome therapies. Studies have reported altered gut microbiota in PsO/PsA and explored probiotics and fecal microbiota transplantation (FMT) as potential therapies. This review synthesizes global studies on the microbiome’s associations in PsO/PsA.
Methods
We conducted a scoping literature review to understand the association between gut microbiota in PsO and PsA patients. Pubmed was used to identify 4,126 published manuscripts between 2015-2025. Thirty studies were included, encompassing 749,275 participants, with balanced gender representation and ages ranging from 18 to 76 years. These studies included 21 case-control studies, 1 case-series, 2 genome-wide analyses, 5 clinical trials, and 1 retrospective review.
Results
Eighteen studies reported significant gut microbiome differences in PsO/PsA vs healthy controls. Variation in the Firmicutes/Bacteroides (F/B) ratio was of interest, with one study suggesting a low F/B ratio and five studies suggesting an elevated F/B ratio in PsO. A higher F/B ratio was linked to increased acetate production. Acetate and propionate, key short-chain fatty acids (SCFAs), were associated with modulation of the IL-23/Th17 axis in psoriasis and activation of keratinocytes. The role of therapeutics targeting the gut microbiome was explored. Ustekinumab and tofacitinib altered gut microbiome composition. Probiotic and FMT interventions showed mixed outcomes. Six of eight probiotic studies reported increased SCFA producing species and/or reduced inflammatory markers. FMT improved immune markers in mice but had no significant benefit in human trials.
Conclusion
Alterations in the microbiome linked to inflammation and immune response, suggest the microbiome as a potential therapeutic target for PsO/PsA.
Introduction
Psoriatic disease is a chronic, multifaceted immune-mediated inflammatory condition encompassing psoriasis, peripheral arthritis, axial disease, dactylitis, enthesitis, and nail changes. 1 Comorbidities include cardiovascular disease, inflammatory bowel disease, metabolic syndrome, and uveitis 2 with the physical burden of disease affecting mental health due to anxiety, depression, and a negative body image.3,4 These profound impacts underscore the necessity of effective treatments aimed at alleviating symptoms, improving quality of life, and preventing disease progression. 5
Psoriasis (PsO) and psoriatic arthritis (PsA) treatment has evolved significantly over time. Medical management includes topical therapies, phototherapy, non-steroidal anti-inflammatory drugs (NSAIDs), glucocorticoids, biologics, and disease-modifying antirheumatic drugs (DMARDs).5,6 Non-pharmacologic additions involve physical activity to reduce systemic inflammation7,8 and dietary changes. The recent health trend in probiotic use 9 has led to studies on the gut microbiome’s role in psoriasis. Independent studies have explored gut microbiome diversity between individuals with and without PsO/PsA. Some studies suggest probiotic usage is associated with beneficial changes in the gut microbiome of PsO/PsA 10 and the possible role of the microbiome has fueled the exploration of fecal microbiota transplants (FMT). 11 Research on understanding this role of the gut microbiome is growing, however reviews synthesizing these findings are scarce. Given the wealth of emerging data, the aim of this study is to present an updated review to identify potential common patterns and trends across studies, providing a clearer understanding of the role of the gut microbiome, probiotics, and fecal transplantation in psoriatic disease management.
Methods
In January 2025, two independent investigators (JC, JK) conducted a scoping review according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines. The objective was to compile and analyze full-text articles and abstracts related to PsO and/or PsA, focusing on the gut microbiome and probiotic usage. The primary search was conducted using PubMed (Figure 1). Key search terms included “psoriasis”, “psoriatic arthritis”, “gut microbiome”, “probiotics”, “prebiotics”, and “fecal transplant”. Searches were filtered to include only full-text, peer-reviewed articles published in English between 2015 and 2025. Methodology of article selection for review. ACR, American College of Rheumatology; EULAR, European Alliance of Associations for Rheumatology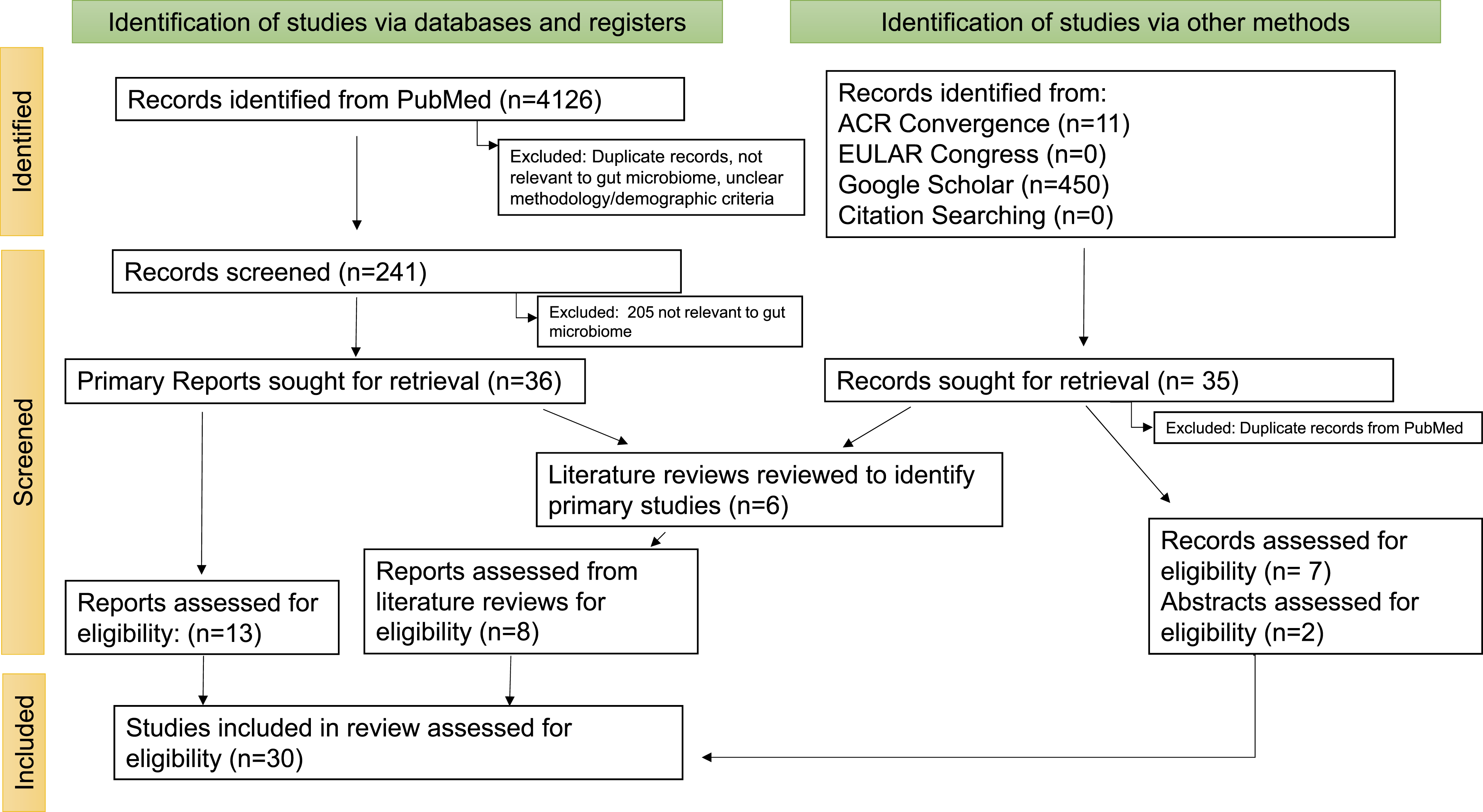
Eligibility for inclusion consisted of full-text peer-reviewed articles written in English, published between 2015-2025, and included either or both PsO and PsA. A total of 4,126 articles were identified in PubMed, of which 13 articles met the eligibility criteria and were included in this review. Furthermore, two abstracts from the American College of Rheumatology (ACR) and 7 articles from Google Scholar were found to be relevant. Although literature reviews themselves were excluded from our study, reviews were used to identify relevant primary studies. As a result, eight primary studies identified through these literature reviews met the inclusion criteria and were therefore included in our study.
Both investigators independently searched abstracts from recent international rheumatological conferences between 2020-2025: ACR Convergence and EULAR Congress. An independent full-text search was also conducted manually using Google Scholar and the citations from the included articles. The terms used for these additional searches were similar to those used in the PubMed search. Disagreements in article selection were adjudicated by a third investigator (SS).
After identifying relevant articles, data was systematically extracted to highlight key characteristics of the studies, including their definition of criteria used to diagnose PsA/PsO (clinical, histopathology, CASPAR, etc.), bacterial taxa differences between PsA, PsO, and healthy controls, and the role of probiotics. For all literature reviews, key referenced studies in these reviews that highlighted the role of PsO, PsA, and the gut microbiome were extracted for assessment and inclusion in our study.
Results
A total of 4,126 articles were identified in PubMed, of which 13 articles met the eligibility criteria and were included in this review. Furthermore, two abstracts from the American College of Rheumatology (ACR) and 7 articles from Google Scholar were found to be relevant. An additional 8 primary studies were extracted from literature reviews and included in this review.
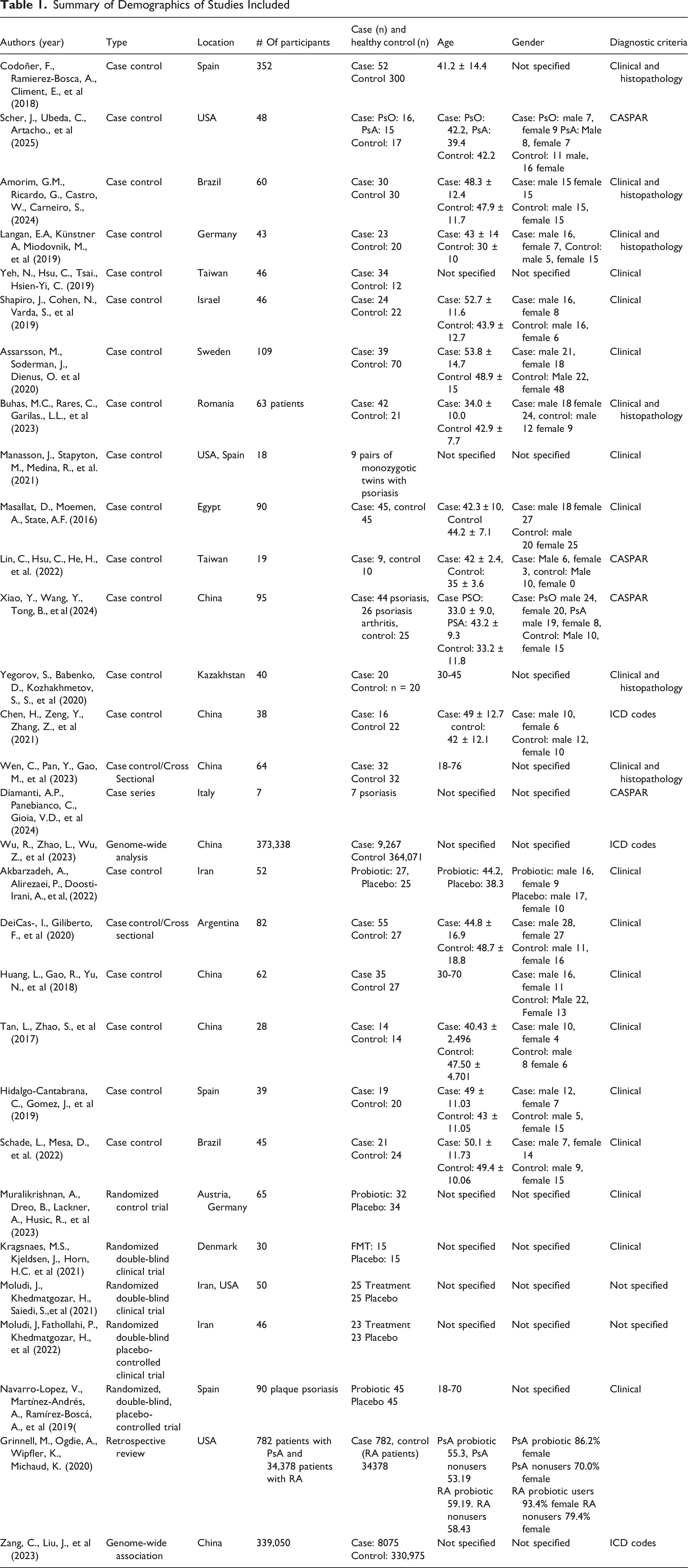
This scoping review includes 30 studies, comprising of 21 case-control studies, 1 case series, 2 genome-wide analyses, 5 clinical trials, and 1 retrospective review. Patients were diagnosed with PsO and/or PsA based on clinical diagnosis, histopathology, CASPAR criteria, and/or International Classification of Diseases (ICD) codes. Fifteen studies used clinical diagnosis, and 6 studies also incorporated histopathology as an additional diagnostic tool. Four studies applied the CASPAR criteria, while three used ICD codes.
Summary of Demographics of Studies Included
Differences in Gut Microbiome
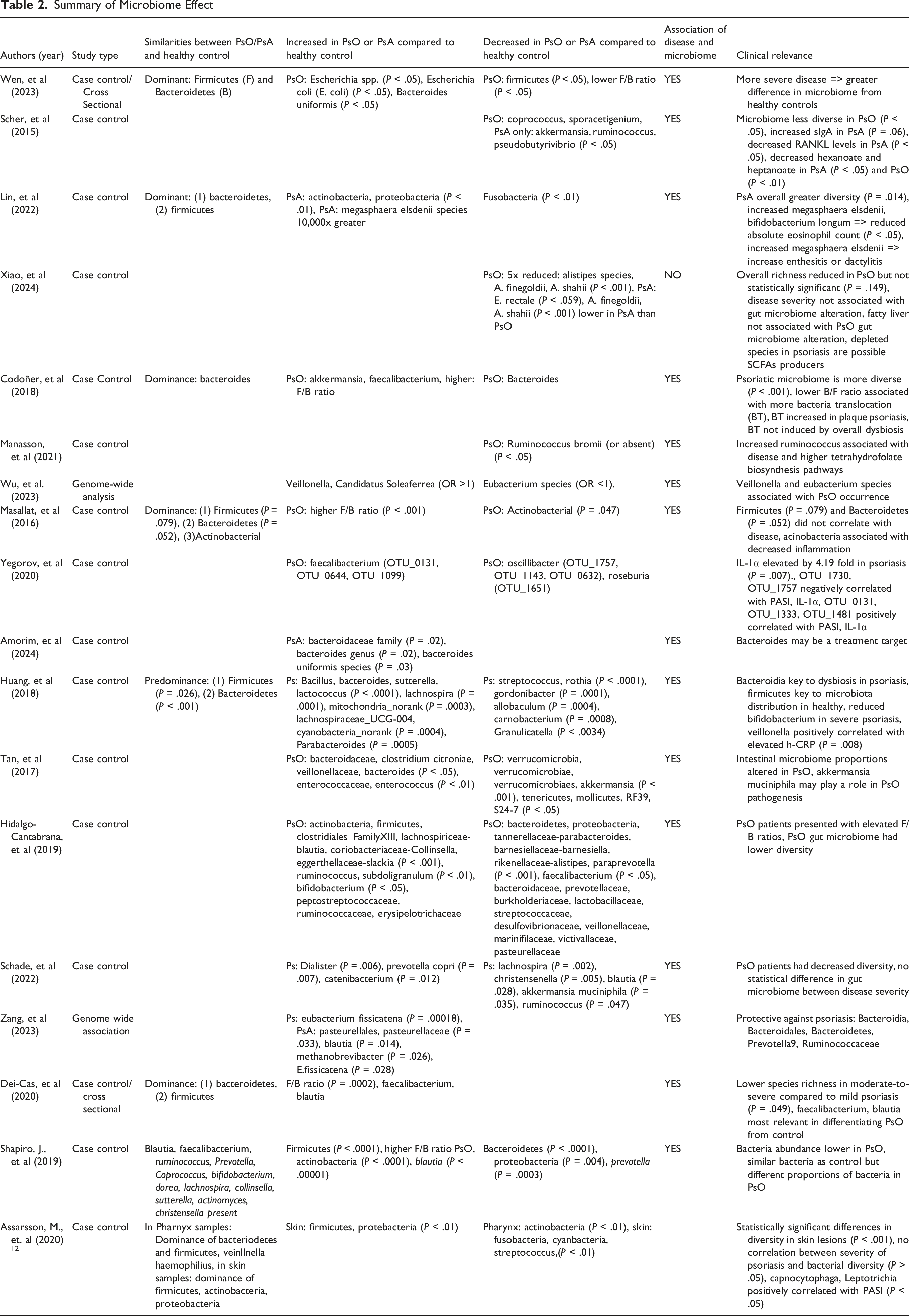
Summary of Microbiome Effect
Differences in Bacterial Community Composition in PsO/PsA
In PsO, increases in Bacteroides Uniformis, Escherichia species, notably E. Coli, 13 Sporacetigenium, 14 and Veillonella 15 were found in comparison to healthy controls. PsO patients were found to have an abundance of Firmicutes 16 and Faecalibacterium.16,17 Four studies noted elevated Blautia in PsO.17–20 Faecalibacterium and Blautia were considered relevant in discriminating PsO from non-PsO patients. 17
PsO individuals had reduced Alistipes,20,21 A. Finegoldii, 21 A. Shahii,2 21 Parabacteroides, 20 Coprococcus, 14 Oscillibacter, 16 Roseburia 16 and Actinobacteria. 22 A study by Huang, et al 23 linked a reduced Bifidobacterium with severe psoriasis. However, Schade, et al 23 found no differences between gut microbiome and disease severities.
Veillonella was associated with elevated c-reactive protein. 23 Gut microbiota changes in PsO were associated with a 4.19x elevation of Interleukin-1 alpha (IL-1α), independent of sociodemographic factors. 16 Additionally, several unclassified OTUs were positively correlated with Psoriasis Area and Severity Index (PASI) and IL-1α. 16 But OTU_1730 and OTU_1757 abundance were negatively correlated with PASI and IL-1α. 16
In PsA, an elevation of Actinobacteria was found by three studies.18,20,24 Others demonstrated enrichments including Megasphaera elsdenii 24 , Bacteroidaceae family, 25 Erysipelotrichia Class, Erysipelotrichales Order, Acidaminococcaceae, Erysipelotrichaceae, and Peptostreptococcaceae families, Clostridium innocuum, Intestinimonas, Morganella Catenibacterium, Turicibacter and Tyzzerella Genus, and Family XIII_AD3011. 24 Four studies noted a reduction of Akkermansia muciniphila.14,20,26,27 Bacteroides,18,20,28 Ruminococcus, 14 Coprococcus 14 and Pseudobutyrivibrio 14 were also found to be significantly reduced. Akkermansia was considered relevant in discriminating PsA from non-PsA14,27 patients.
Compared to PsO, PsA had a greater relative abundance of B. Vulgatus, B. Stercoris, B. Uniformis, and B. Plebeius. 25 Between PsO and PsA, Xiao, et al 21 found no community-level difference in the gut microbiome, but a reduction in E. Rectale levels. Scher, et al 13 differed in conclusion demonstrating PsA and PsO had reduced gut microbiome diversity compared to healthy controls.
F/B Ratio and Dominating Species
Wen et al 13 reported decreased Firmicutes in PsO, resulting in a lower F/B ratio compared to health controls. Zang, et al 18 found Bacteroidia, Bacteroidales, Bacteroidetes, Prevotella, Ruminococcaceae were protective against PsO, while Huang, et al 22 concluded Bacteroidia was key to PsO dysbiosis, and Firmicutes was key to the microbiota distribution seen in healthy patients.
However, five studies17,18,20,22,28 noted a higher F/B ratio in PsO, emphasizing a predominance of Firmicutes and a decrease in Bacteroides compared to healthy controls. Lin, et al 24 concluded both patients with PsA and patients without PsA had microbiota profiles dominated first by Bacteroides, followed subsequently by Firmicutes.
Overall Diversity Differences
A study by Wen, et al 12 demonstrated PsO had no substantial differences in microbial diversity, but there were differences in the distribution of microbial taxa. In PsO, Escherichia species, Bacteroides Uniformis, and Escherichia coli (E. coli) were enriched with 4 metabolic pathways upregulated and 3 metabolic pathways downregulated. In severe PsO, Enterobacter and Paraprevotella were enriched; Gemella was decreased; and Parabacteroides goldsteinii, Streptococcus mitis oralis pneumoniae, and Roseburia intestinalis were depleted. Compared to healthy controls, Xiao, et al 20 demonstrated changes in gut microbiome that resulted in decreased richness but not evenness. Dei-Cas et al 16 found a reduction in species richness with greater psoriasis severity, but no difference in beta diversity.
In contrast, Codoñer, et al 27 found the PsO microbiome more diverse than healthy controls and found bacterial DNA translocation (BT) may occur in 25% of PsO patients. Compared to healthy controls, BT + psoriasis patients had an increase in the genus Streptococcus, Bifidobacterium, and Akkermansia. An increase in Bifidobacterium was also found by Hidalgo-Cantabra, et al. 19 The presence of blood circulating bacterial DNA, originating from the intestinal lumen, may be linked to immune activation and plaque psoriasis outbreaks. 29
Medication Effects
Summary of Medication Effect
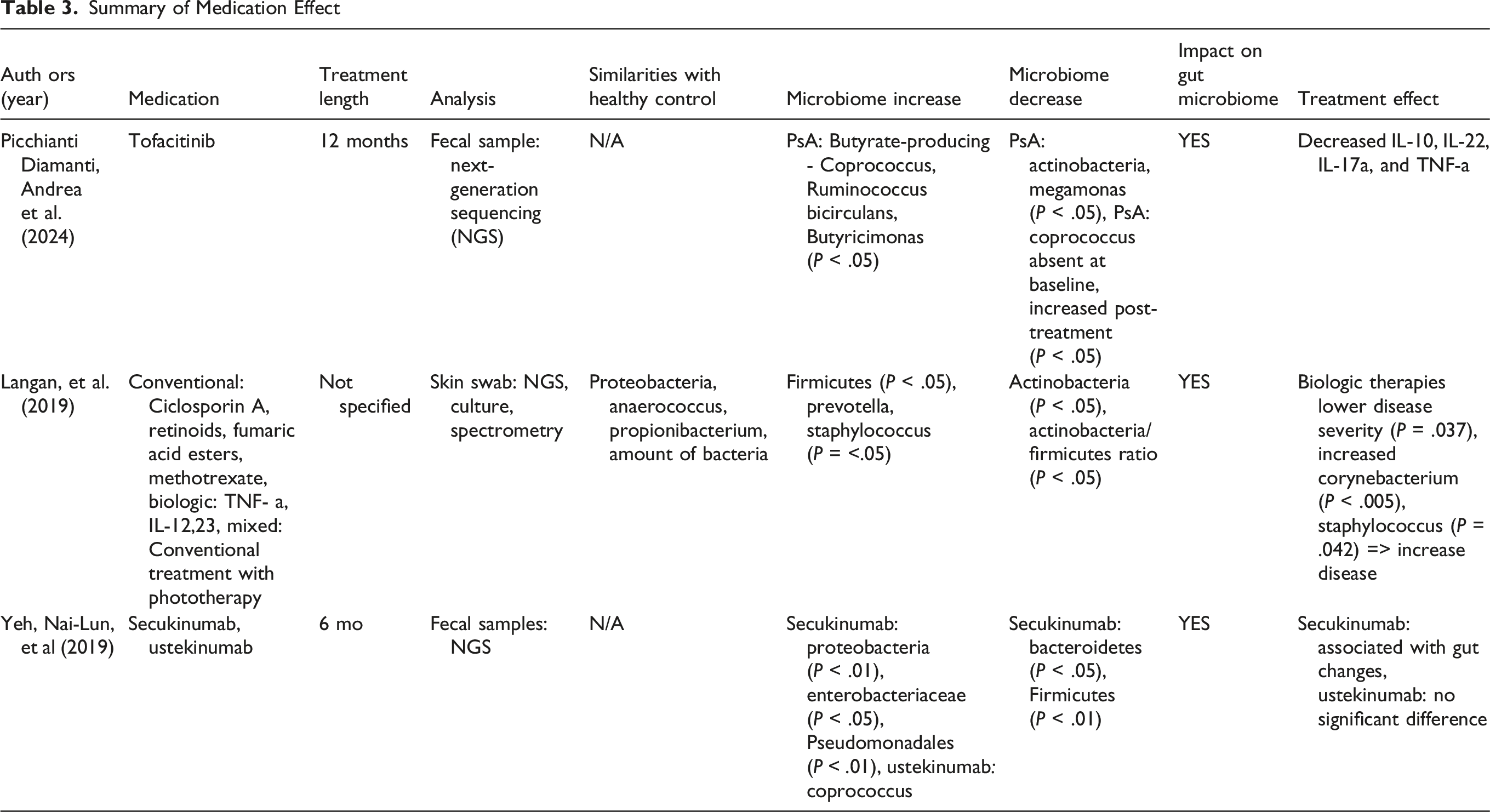
Yeh, N., et al 30 found secukinumab treatment had a greater impact on the gut microbiome compared to ustekinumab treatment. On the phylum level, Proteobacteria was increased and Bacteroidetes and Firmicutes were decreased. On the family level, Pseudomonadaceae and Enterobacteriaceae and the order Pseudomonadales were increased. Baseline gut microbiome differences were also noted between Secukinumab responders and nonresponders. Following 6 months of ustekinumab treatment, there was a significant increase in Coprococcus.
Picchianti Diamanti, A, et al 30 explored tofacitinib’s role on the gut microbiome. Post-tofactinib treatment showed reduced phylum Actinobacteria and genus Megamonas, and butryate-producing species of Coprococcus comes, Ruminococcus bicirculans, and Butyricimonas sp. AT11 were increased. Pre-treatment, Coprococcus comes was absent in PsA. This study also correlated bacteria post treatment to groups of cytokines. IL-22, IL-17a, and TNF-α were negatively associated with Euryarcheota and Lentisphaerae, and positively associated with Verrucomicrobia. These cytokines were negatively associated with Methanobacteriaceae, Odoribacteriaceae and Victivallaceae, and positively associated with Desulfovibrionaceae, Enterobacteriaceae, and Lactobacillaceae. The results suggest a potential bidirectional effect of the gut microbiome on treatment response and treatment on the gut microbiome.
Probiotic/Prebiotic Use
The role of probiotics in altering the gut microbiome varies. After 12 weeks, Buhas, M., et al 10 found supplementation with probiotics (Bacillus indicus (HU36), Bacillus subtilis (HU58), Bacillus coagulans (SC208), Bacillus licheniformis (SL307), and Bacillus clausii (SC109)) and precision prebiotics (fructooligosaccharides, xylooligosaccharides, and galactooligosaccharides, lipopolysaccharide positive bacteria) led to significantly reduced TNF-α and IL-6, and significantly increased IL-10. This study noted significantly decreased uric acid with probiotics treatment, suggesting a possible benefit for those with hyperuricemia, reduced response to anti-psoriatic medication, and greater joint destruction. A significantly increased population of Akkermansia muciniphila and Ruminococcus spp, and F/B ratio were found. Higher F/B ratios, Akkermansia muciniphila, and Ruminococcus spp were associated with increased acetate and propionate production, and subsequent modulation of the IL-23/Th17 axis.31,32
Moludi, et al 34 using probiotic drinks with Lactobacilus strains and Akbarzadeh, A., et al 33 using Lactocare probiotic, both concluded probiotics may be a beneficial treatment in improving quality of life, decreasing inflammatory markers, PASI, and Psoriasis Symptom Scale (PSS) scores. The study by Akbarzadeh, A., et al 33 showed a positive association between Lactocare (probiotic) and a reduction in disease activity scores after 12 weeks. When Lactocare and pharmacological therapy of hydrocortisone were administered together, there were increased effects on the reduction of disease activity. However, the two studies did not perform microbiome sequencing to directly assess changes in gut microbial composition with probiotic use and the corresponding effects on psoriatic disease measures.
Additionally, Moludi, et al 34 builds off of another study 35 which found improvements in both quality of life and PASI scores, and reductions in lipopolysaccharides (LPS), high-sensitivity C-reactive protein (hs-CRP), and Interleukin-1 beta (IL1β) levels in PsO patients that took probiotic capsules containing multi-strains of at least 1.6 × 109 CFU/g bacteria. A 12-week study by Navarro-Lopez, et al 36 found greater reduction in PASI and Physician’s Global Assessment (PGA) scores when probiotic supplementation was used in conjunction with topical steroids, compared to with topical steroids alone. Incidence of relapse was reduced by half at 6 months post-probiotic supplementation. A complete depletion of the genera Micromonospora and Rhodococcus, and an increase in Collinsella and Lactobacillus were also observed with supplementation.
However, in a study by Muralikrishnan, A., et al 38 using probiotic containing Bifidobacterium and Lactobacillus strains, the disease activity, measured by Psoriatic Arthritis Disease Activity Score (PASDAS) score, was significantly reduced with treatment regardless of probiotic intervention. There was also no difference in the proportion achieving remission between the probiotic and placebo groups. An increase in Th2 cells in the probiotic group was found, but there was no significant difference in other lymphocytes including Th1, Th17, and Tregs. Grinnell M., et al 39 concluded no statistically significant difference in health outcomes or patient function scores pre- and post-probiotic intervention.
Fecal Transplant
There are limited studies conducted on FMT. Chen, H., et al 40 demonstrated that FMT using stool from healthy donors, when transplanted into psoriasis mice, resulted in protective effects against the Treg/Th17 imbalance commonly seen in psoriasis. Mice receiving stool from healthy donors showed an increase in Lactobacillus reuteri, which in turn was associated with promoted expression of anti-inflammatory cytokines, IL-10, leading to a reduction in Th17 cells and offering protective anti-inflammatory effects.
A study by Kragsnaes, M., et al 41 involving human subjects in a double-blind, placebo-controlled design, found no adverse effects of FMT on active PsA. However, treatment failure rate was higher in the FMT treated group than in the sham group (HR 4.87 P = 0.018). This study assessed outcomes using the Health Assessment Questionnaire Disability Index (HAQ-DI) and American College of Rheumatology (ACR20) response criteria, over 26 weeks post-FMT. The HAQ-DI improved more in the sham group.
Discussion
This review provides a comprehensive synthesis of literature on the role of gut microbiome in psoriatic disease. Our review reflects the substantial growth in understanding gut microbial associations in PsO and PsA. Previous reviews focused on PsO and only one study involved PsA. 37 Additional studies, including those examining probiotics and FMT, have provided new insights into microbial influences on disease pathogenesis. Our review incorporates 30 studies, including 5 clinical trials from a globally diverse set of PsO/PsA patients, allowing for a comparative analysis across study types and a more detailed and nuanced understanding of the microbiome’s role in PsO/PsA.
We found a report of a decrease in Firmicutes and increase in Bacteroides (low F/B) in PsO patients of interest, as a higher F/B ratio was associated with increased acetate synthesis. The SCFAs acetate and propionate are associated with anti-inflammatory properties and modulation of the IL-23/Th17 axis 10 which is implicated in pathogenesis of psoriatic disease. 38 However, several studies also concluded a high F/B ratio in PsO patients and mixed results regarding alpha and beta diversity in PsO/PsA, suggesting a unified psoriatic gut microbiome signature has not been fully identified. While phylum ratios can be markers in disease, gut microbiome phylum can be highly sensitive to external factors including diet, treatment exposure, and environment suggesting confounding variables. 31 Prior studies have demonstrated an association between obesity and elevated F/B ratios. 39 BMI may also serve as a confounding factor contributing to discrepancies between studies.
Data regarding the role of therapeutics is scarce. Ustekinumab and tofacitinib treatment were seen to alter the gut microbiome composition. Results with probiotic supplementation showed mixed results, with some demonstrating low to moderate improvements in PASI scores, quality of life measurements, and inflammatory markers with increased population of species correlating with acetate and propionate. Downregulation of inflammatory markers and uric acid were also demonstrated. However, other studies concluded no statistically significant differences in health outcomes with supplementation. These inconsistencies observed with probiotic supplementation may be related to the unique structural differences or effects of different probiotics 40 and variation in study durations. Probiotic studies in PsA have not shown a beneficial correlation between usage and disease activity.
Likewise, FMT had mixed results. FMT in mice resulted in increased IL-10, leading to a reduction in Th17 cells, 41 while a human study of FMT resulted in higher treatment failure rates in the treatment group compared to controls. 42 These studies suggest a need for further investigation into dysbiosis profiles in PsO/PsA, FMT methods, categorization of ”beneficial” and ”non-beneficial” donations, and controlling for confounding variables including individual baseline gut microbiome composition, genetics, and diet.
Our review highlights the complexity of pathophysiology of psoriatic disease, which is an interplay between possible modifiable risk factors, genetic predisposition, and immune dysfunction. 43 Increasing evidence highlights the role of modifiable risk factors in influencing disease onset and severity, and possibly through the gut microbiome. 43
Stress increases inflammatory cytokines, which exacerbate immune activation and promotes psoriatic flares. Similarly, skin injury or infection can trigger immune cell, including dendritic cells, T cells, and neutrophils, recruitment to the epidermis. 41 These stimuli result in upregulation of TNF-α, which orchestrates systemic inflammation, apoptosis, and immune responses 44 by increasing production of acute phase reactants and pro-inflammatory cytokines. 44 This process is also increased in obesity. Living in food deserts or consuming processed foods increases obesity risk, a known PsO risk factor. 45 Obesity and poor diet alter the gut microbiome, 40 leading to inflammation via increased secretion of TNF-α and other cytokines from adipose tissue, contributing to immune dysregulation related to psoriasis pathogenesis. 46
Psoriatic disease is marked by increased TNF-α, IL-17, IL-22, and IL-23, known as the IL-23/Th17 axis. 47 IL-17 and IL-22, produced by Th17 cells, drive keratinocyte proliferation and amplify local inflammation. IL-22 contributes to epidermal hyperplasia and thickening, whereas IL-17 promotes chemokine expression, leading to recruitment of monocytes, macrophages, and neutrophils to inflammatory sites. 48 This cascade perpetuates immune activity and contributes to vascular remodeling, resulting in erythematous and scaly plaques. 48
Understanding these pathways has influenced clinically effective targeted biologic therapies that inhibit or reduce IL-17, IL-23, or TNF-α. Furthermore, our review suggests that understanding of gut microbiome profiles and their links to inflammation and immune response may lead to focus on the microbiome as a potential therapeutic target for PsO/PsA. 45
A strength of this review is the comprehensive inclusion of diverse study types, large patient samples, and global representation of patients. Our review is subject to limitations as only studies published in English within the last 10 years were included. Additionally, the methodological quality and strength of the included studies were not systematically assessed, limiting the ability to evaluate the robustness of the evidence. The variability in study designs, patient populations, and analytical methods presents limitations hindering the ability to draw definitive, universally applicable conclusions. Our review highlights the variability in reported gut microbiome signatures associated with psoriatic disease across studies. Differences in microbial composition such as alterations in the F/B ratio or changes in specific bacterial taxa were not always consistent between cohorts. This heterogeneity may be attributed to several confounding variables that are not consistently controlled across studies. One possible reason for these differences is the use of different sequencing methodologies. Studies that utilize 16S ribosomal RNA gene sequencing primarily characterize bacterial taxonomic composition, while metagenomic sequencing provides higher taxonomic resolution and allows for the assessment of microbial functional capacity. 47 Additionally, systemic medications, obesity and metabolic status, environment, genetics, and dietary patterns are modulators of gut microbial composition and may substantially shape microbiome profiles in patients with psoriatic disease. 44
These observations suggest gut microbiome alterations may be associated with psoriatic disease, but the specific microbial signatures reported may be influenced by underlying host and environmental factors. Future studies with more standardized approaches and careful control of these variables will be important to clarify consistent microbiome patterns and their potential role in disease pathogenesis and therapeutic targeting.
Conclusion
The gut microbiome and psoriasis relationship is complex, with studies showing alterations such as variability in F/B ratios. Differences in the gut microbiota may be correlated to alterations in the regulation of metabolic pathways or immune response. With limited research with mixed results, further research on therapeutics involving prebiotics, probiotics, biologics, and FMT, as well the metabolic and immune implications of gut microbiome shifts can increase understanding of psoriasis pathogenesis.
Footnotes
Ethical Considerations
Research ethics approval was not required as no human or animal subjects were involved.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
1. Jessica Kent: nothing to disclose
2. Jessica Chao, nothing to disclose
3. Wilson Liao, received research grant funding from Amgen, Janssen, Leo, and Regeneron
4. Shikha Singla, received consulting fees from AbbVie, Johnson & Johnson, and UCB, speaker fees from Johnson & Johnson, research grants from AbbVie, Eli Lilly and Prometheus Biosciences
Patient and Public Involvement
There was no patient or public involvement with this manuscript.
Data Availability Statement
Data will be made available upon reasonable request.