
Abstract
Cervical cancer remains a primary cause of gynecologic oncology-related mortality globally, with a disproportionate burden in sub-Saharan Africa. The pathogenesis of the disease is fundamentally driven by persistent infection with high-risk human papillomavirus (HPV) genotypes, most notably HPV-16 and HPV-18. The evolution of prophylactic HPV vaccination has transformed preventive oncology, progressing from first-generation bivalent and quadrivalent formulations to the nonavalent vaccine, which extended protection to five additional oncogenic types. These vaccines, composed of L1 virus-like particles (VLPs), induce robust and durable humoral and cellular immune responses, leading to population-level reductions of up to 98% in vaccine-type infections and 80% in high-grade cervical lesions. To address persistent global health disparities, regionally produced, cost-effective alternatives such as Cecolin and Cervavac have been introduced to enhance accessibility within low- and middle-income countries. This shift toward broader coverage is further supported by the 2022 WHO recommendation for a single-dose schedule, aimed at optimizing resource-limited immunization programs. Current research is now pivoting toward next-generation candidates targeting the conserved L2 protein for pan-genotype protection, as well as therapeutic vaccines targeting E6 and E7 oncoproteins to clear established infections. However, achieving the WHO’s 2030 cervical cancer elimination targets remains contingent upon overcoming infrastructural, cultural, and informational barriers that hinder vaccine uptake. This review synthesizes the molecular composition and immunological mechanisms of current and emerging HPV vaccines, evaluating their clinical efficacy and the systemic strategies required to ensure equitable global access.
Plain language summary
Cervical cancer, primarily caused by persistent infection with high-risk human papillomavirus (HR-HPV) genotypes, remains a major cause of morbidity and mortality among women, particularly in low- and middle-income countries. This review provides an overview of the mechanisms, clinical efficacy, and established safety profiles of currently available recombinant HPV vaccines. It highlights important developments in the field, including the shift toward simplified single-dose schedules, the emergence of more affordable vaccines produced in emerging markets, and the validation of heterologous mix-and-match strategies to address supply-chain limitations. The review also examines the future direction of HPV immunization, including next-generation vaccine candidates with broader cross-protective potential and therapeutic vaccines designed to target existing HPV-related disease. Taken together, these developments may contribute substantially to improving global vaccine access and coverage, thereby supporting ongoing efforts to eliminate cervical cancer as a public health threat in line with the World Health Organization strategy.
Keywords
Introduction
Cervical cancer remains a significant global health challenge, primarily driven by persistent infection with oncogenic human papillomavirus (HPV) genotypes. Among these, HPV-16 and HPV-18 are the most prevalent, accounting for approximately 70% of cases worldwide.1,2 The viral life cycle begins with the infection of basal epithelial cells, a process mediated by the major capsid protein L1, which binds to host heparan sulfate proteoglycans, and the minor capsid protein L2, which facilitates viral entry and endosomal escape for genome delivery. 3 The transition from infection to cervical carcinogenesis is predicated on the failure of the host to clear high-risk HPV (HR-HPV). While most infections are transient and resolve spontaneously within 6–24 months, sustained persistence leads to the continuous expression of the E6 and E7 oncoproteins.3,4 These viral proteins orchestrate malignant transformation by inactivating the tumor suppressors p53 and retinoblastoma protein (pRb), respectively, thereby inducing genomic instability and relentless cellular proliferation. 5 Evidence from longitudinal studies underscores that women with type-specific HR-HPV persistence face a substantially higher risk of developing high-grade cervical intraepithelial neoplasia (CIN 2/3) compared to those who achieve viral clearance.6,7 This clinical progression is fundamentally driven by the host immune system, which serves as the primary determinant of infection outcome.
A robust cell-mediated response, driven by cytotoxic CD8+ T cells and Th1 cytokines such as interferon-gamma (IFN-γ) and interleukin-2 (IL-2), is essential for viral eradication.4,8 Nevertheless, HR-HPV has evolved sophisticated evasion strategies; for instance, the E5 and E7 oncoproteins downregulate major histocompatibility complex (MHC) class I expression, thereby impairing antigen presentation. 9 Furthermore, the cervical microenvironment in persistent cases is often characterized by an influx of regulatory T cells (Tregs) and elevated levels of immunosuppressive cytokines (IL-10 and TGF-β), which facilitate a chronic infection state.10,11 Recent studies also highlight the importance of tissue-resident memory T (TRM) cells in local surveillance, noting that deficient TRM responses are strongly associated with viral persistence.12,13 Beyond immunological factors, epigenetic and microenvironmental variables influence disease progression. Hypermethylation of viral and host genes such as PAX1 and ZNF582 has emerged as a potential biomarker for identifying transforming infections, especially when integrated with p16/Ki-67 immunoscores. 14 Additionally, the cervicovaginal microbiota plays a modulatory role, where a depletion of Lactobacillus crispatus and increased microbial diversity are linked to higher lesion grades. 15 Despite the promise of these biomarkers in risk stratification and post-treatment surveillance, their clinical utility is currently limited by geographical heterogeneity and a lack of standardized testing methods. Given the complexities of managing persistent infection and the associated risk factors, such as immunosuppression, age, and smoking, primary prevention through vaccination remains the most effective public health strategy.
The landscape of HPV prevention has evolved from first-generation bivalent and quadrivalent vaccines to the current nonavalent formulations, which have significantly reduced the global burden of disease. More recently, the introduction of regionally developed, cost-effective vaccines such as Cecolin, WalrinVax, and Cervavac has addressed barriers to accessibility in low- and middle-income countries (LMICs). 16 Understanding the clinical success of these interventions requires a detailed examination of their molecular architecture and the immunological pathways they activate.
Composition and mechanism of action
The structural foundation of prophylactic HPV vaccines is the L1-derived virus-like particle (VLP). These recombinant particles are synthesized to be non-infectious, as they lack the viral genome, yet they maintain the highly organized, icosahedral symmetry of the native virion. 17 This structural fidelity is critical for efficient immune recognition and high immunogenicity. Specific composition and manufacturing of these vaccines vary significantly based on their valency, the host expression system utilized for protein synthesis, and the proprietary adjuvant systems employed to enhance long-term immunological memory. The selection of a biological expression system represents a primary technical differentiator among these vaccines, directly influencing both the complexity of protein folding and the scalability of production. While the established Gardasil series utilizes Saccharomyces cerevisiae, more recently developed vaccines such as Cervavac and WalrinVax leverage alternative yeast strains to optimize antigen yield and thermal stability.18,19 In contrast, Cervarix is distinct in its utilization of a baculovirus expression system within insect cells; a platform that facilitates complex post-translational modifications, such as glycosylation patterns that more closely resemble human proteins. 20 To address the imperatives of global affordability and supply, Cecolin employs an E. coli bacterial system. Although this necessitates in vitro protein refolding, it offers a highly cost-effective manufacturing pathway for LMICs. 16
The adjuvant component is also critical for modulating the magnitude and duration of the vaccine-induced IgG response. While most formulations rely on traditional aluminum-based salts, Cervarix incorporates the AS04 adjuvant system. This specialized system combines aluminum hydroxide with 3-O-desacyl-4’-monophosphoryl lipid A (MPL), a Toll-like receptor 4 (TLR4) agonist which promotes higher and more sustained antibody titers compared to conventional aluminum salts alone (Table 1). 21
Comparative composition of global HPV vaccines.
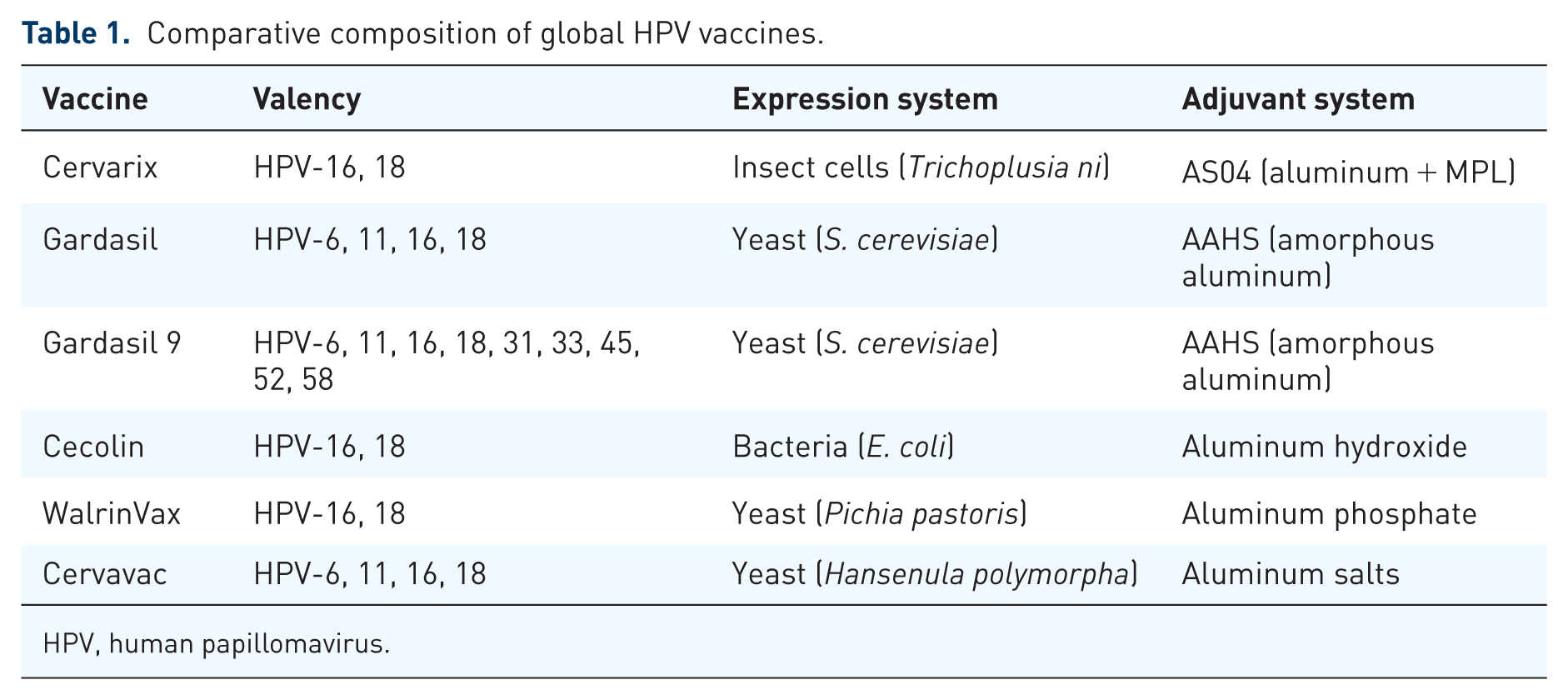
HPV, human papillomavirus.
Mechanism of action of HPV vaccines
Upon intramuscular administration, these VLPs function as potent antigens that are rapidly sequestered by professional antigen-presenting cells (APCs). 22 The APCs process the VLPs and migrate to regional lymphoid tissues to present L1 epitopes to naive CD4+ T helper cells. This interaction facilitates the formation of germinal centers, driving B-cell activation, class switching, and affinity maturation. The resulting immunological output is characterized by high-titer, high-affinity neutralizing antibodies specifically targeting the conformational epitopes of the L1 capsid.23,24 These vaccine-induced anti-L1 antibodies circulate systemically and transudate through the capillary walls into the cervicovaginal mucosa. Here, they provide a first line of defense by binding to incoming virions, effectively neutralizing the virus before it can attach to or enter the basal epithelial cells. 24 By arresting the viral life cycle at this nascent stage, the vaccines prevent the establishment of the persistent infection that is necessary for cervical oncogenesis. Consequently, serum neutralizing antibody titers serve as the primary immunological correlate of protection against de novo HPV infection. 25
While the humoral response is paramount, HPV vaccines also elicit supportive cellular immunity that ensures durable protection. CD4+ T cells are instrumental in orchestrating long-term immunological memory through the generation of memory B cells, which provide a rapid and robust recall response upon viral re-exposure. 26 It is important to note, however, that while standard L1-VLP vaccines induce modest CD8+ T-cell responses, these are insufficient for the clearance of established, intracellular infections. 27 This mechanistic limitation necessitates a different approach for patients with existing disease. Emerging therapeutic HPV vaccine strategies are specifically engineered to bypass the L1-mediated antibody pathway. They aim to stimulate potent cytotoxic T-lymphocyte (CTL) responses directed against the viral oncoproteins E6 and E7. By targeting these early-phase proteins expressed in infected and malignant cells, therapeutic candidates seek to achieve the clearance of established lesions and advanced HPV-associated malignancies.28,29 Figure 1 shows the development of anti-L1 antibodies and long-lasting immunological memory against HPV.
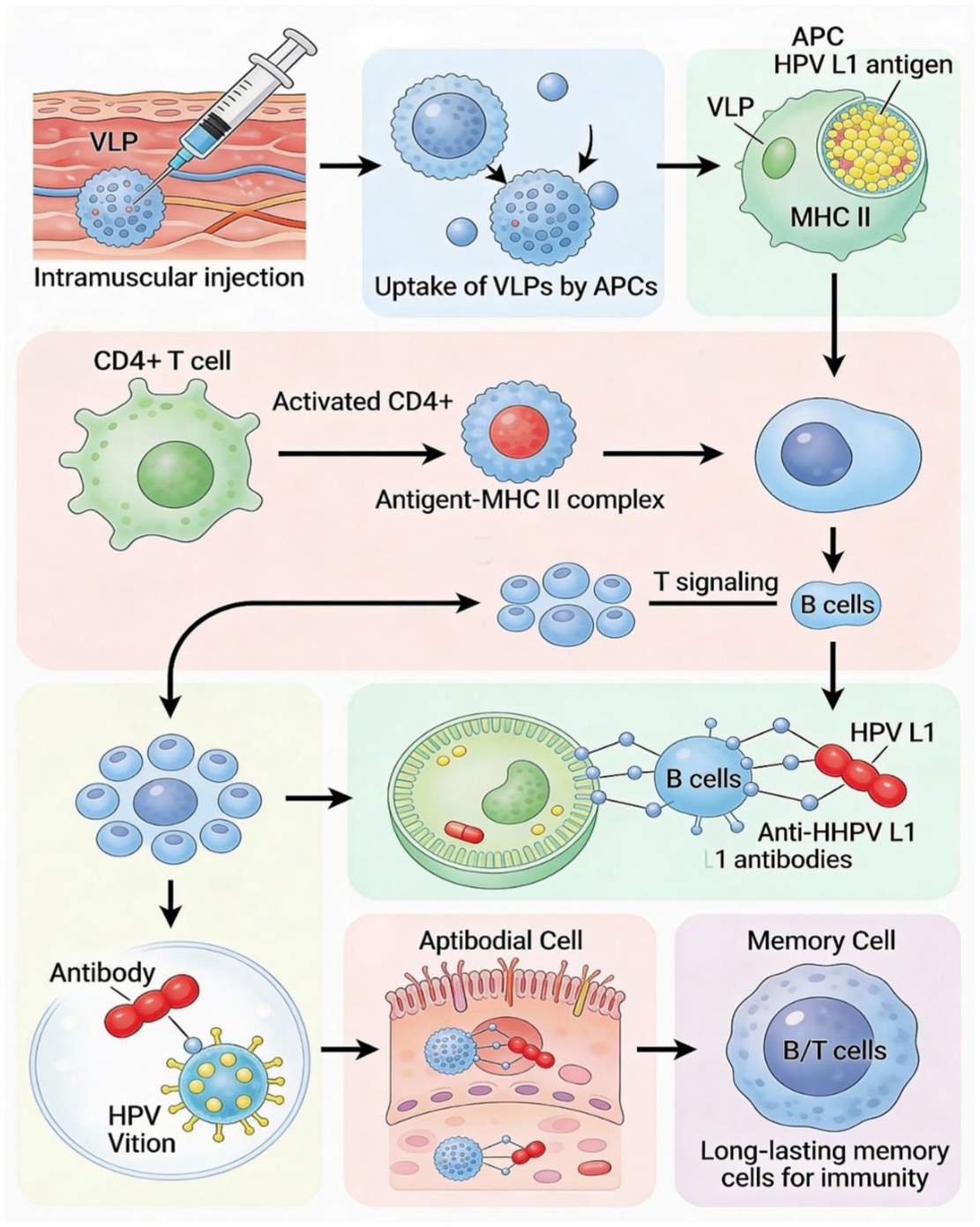
Immune response to HPV: anti-L1 antibody production and memory cell formation over time.
Following intramuscular injection, HPV L1 VLPs are taken up by antigen-presenting cells. The VLPs are then processed and presented through MHC class II, which activates CD4+ T helper cells. This T-cell activation stimulates B cells to differentiate into plasma cells that produce neutralizing antibodies. These antibodies prevent HPV from infecting epithelial cells while memory B and T cells form, providing long-term immunity. Image was generated using the Seedream tool, version 4.5 (ByteDance Ltd., China).
Efficacy and longevity
The clinical utility of HPV vaccines is evidenced by consistent data from global randomized controlled trials and longitudinal population-based studies. These findings demonstrate that licensed formulations provide high, albeit variable, protection against persistent infection and the subsequent development of high-grade precancerous lesions. The nonavalent vaccine—Gardasil 9, currently offers the broadest spectrum of protection, achieving approximately 97% efficacy against CIN2+ associated with five additional high-risk genotypes (HPV-31, 33, 45, 52, and 58) while maintaining the robust protection against the original four types (HPV-6, 11, 16, 18) established by earlier formulations.30–32 The predecessor quadrivalent vaccine—Gardasil, has shown up to 98% efficacy against cervical lesions linked to HPV-16 and -18, as well as nearly 100% protection against genital warts caused by types 6 and 11.33,34 Similarly, the bivalent vaccine—Cervarix, demonstrates over 90% efficacy against persistent HPV-16 and 18 infections and associated CIN2+; notably, it also provides significant partial cross-protection against non-vaccine types HPV-31 and HPV-45.35,36
A defining hallmark of these L1-VLP vaccines is the remarkable durability of the immune response. Neutralizing antibody titers remain well above protective thresholds for at least 10–14 years post-vaccination, and ongoing immunogenicity studies suggest that the induction of long-lasting immune memory may negate the need for booster doses in immunocompetent populations.34,37 Accumulating evidence further corroborates these clinical findings. For instance, CDC analyses have reported an 80% reduction in precancerous lesions among women aged 20–24 years, the cohort with the highest early vaccine uptake.38,39 Parallel to these established platforms, evaluations of newer, regionally developed vaccines indicate comparable clinical performance. Cecolin has demonstrated nearly 100% efficacy against persistent HPV-16 and 18 infections during a 5-year follow-up, characterized by robust seroconversion and sustained antibody levels.40,41 Furthermore, WalrinVax and Cervavac have exhibited immunogenicity non-inferior to WHO-prequalified vaccines, with Cervavac producing antibody responses similar to those of the quadrivalent Gardasil.19,42
While long-term data for these emerging vaccines beyond 5 years is still accumulating, current evidence suggests that their ability to induce durable protection and immunological memory is consistent with established VLP technology. As these vaccines expand global coverage, the focus shifts from clinical efficacy to ensuring their safety profiles are rigorously monitored to maintain public confidence (Table 2).
Clinical trials status of the global HPV vaccines.
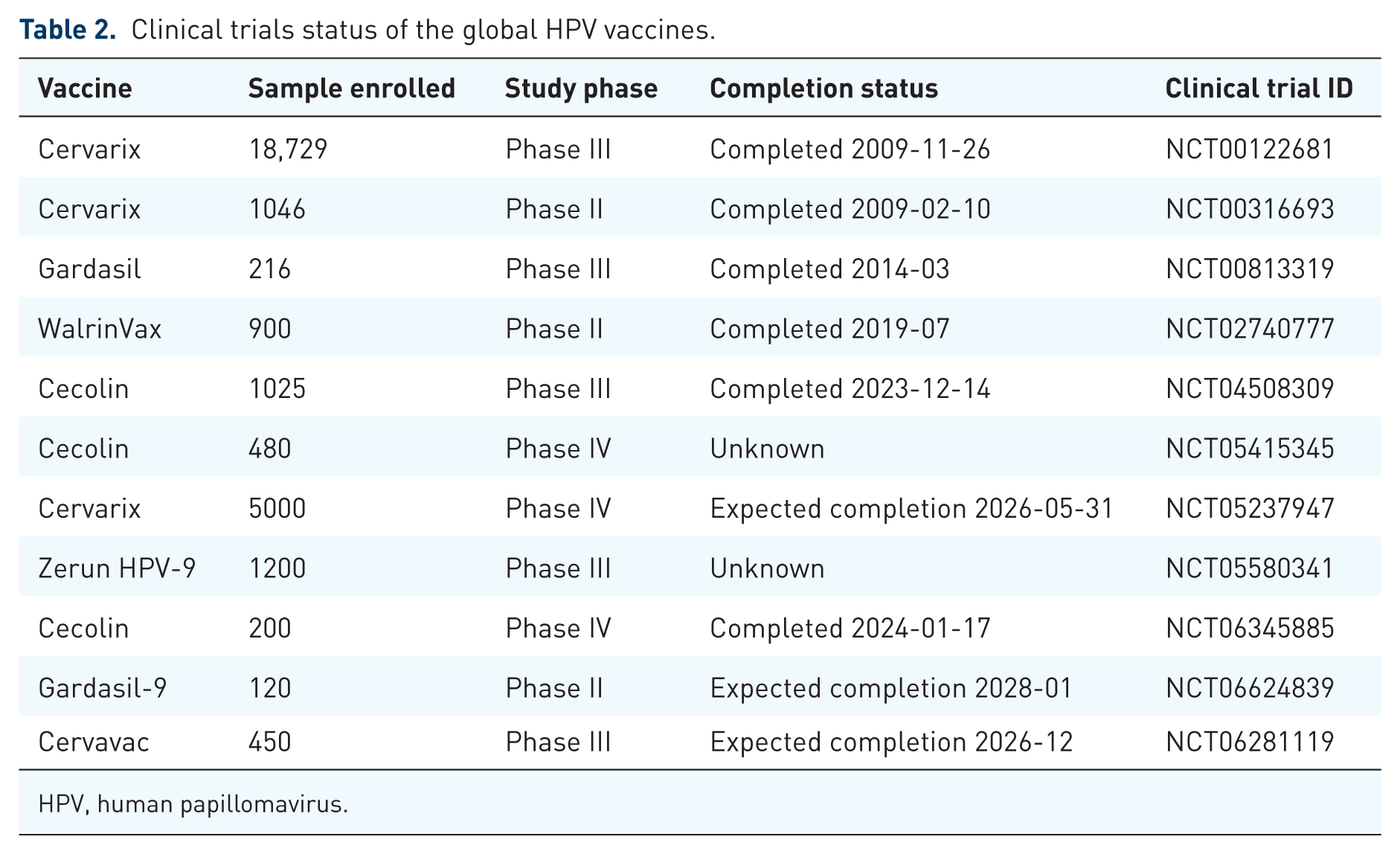
HPV, human papillomavirus.
Safety and side effects
The clinical implementation of HPV vaccination is supported by an exemplary safety record, established through rigorous clinical trials and reinforced by decades of global post-marketing surveillance. Data consistently demonstrate that all licensed formulations possess high safety margins, with the majority of adverse events (AEs) classified as mild and self-limiting. The most frequently reported AEs across all platforms are localized injection-site reactions, including pain, erythema, and edema. Systemic effects, such as headache, fatigue, nausea, and low-grade pyrexia, occur less frequently and typically resolve spontaneously without medical intervention.43,44 Notably, the reactogenicity profile varies slightly by formulation; for instance, the AS04 adjuvant system used in Cervarix is associated with a marginal increase in local reactogenicity compared to traditional aluminum-only salts, though this carries no significant clinical concern. 45 Similarly, Gardasil 9 may elicit slightly higher rates of local reactions than its quadrivalent predecessor due to higher antigen and adjuvant concentrations, yet its overall safety profile remains comparable.46,47 Serious adverse events (SAEs), such as anaphylaxis, are exceedingly rare, and extensive epidemiological studies have failed to establish a causal link between HPV vaccination and autoimmune, neurological, or reproductive disorders. This safety consensus is shared by global health authorities, including the WHO and the CDC, whose continuous monitoring affirms that the benefits of preventing HPV-related malignancies far outweigh the risks of transient side effects.48,49
The safety profiles of newer, regionally developed vaccines, including Cecolin, WalrinVax, and Cervavac, mirror those of established WHO-prequalified formulations. Cecolin has demonstrated a tolerability profile comparable to both Gardasil and Cervarix, with injection-site reactions remaining the most common event, while systemic myalgia and fatigue remain infrequent.16,40,50 WalrinVax and Cervavac have also exhibited minimal reactogenicity in Phase III evaluations, with no reported vaccine-related SAEs to date.51,52 This foundation of clinical safety is essential for sustaining the public trust required for broad population coverage. However, translating these safe and effective clinical tools into a successful public health outcome requires overcoming significant logistical, economic, and sociocultural barriers, particularly in high-burden regions.
Acceptability and coverage
While international guidelines prioritize HPV vaccination for females aged 9–14 years, with catch-up protocols extending to age 26 and gender-neutral strategies enhancing herd immunity, global uptake remains deeply stratified.31,53–55 In high-income regions, including North America, Europe, and Australia, integrated health systems have achieved coverage rates of 80%–90%.56–58 Conversely, uptake in LMICs, particularly within sub-Saharan Africa, remains constrained. Although nations like Rwanda and Tanzania have exceeded 70% first-dose coverage, the regional average stagnates near 50%, with several countries reporting rates below 20%.59–61 Figure 2 shows HPV vaccine coverage across various WHO regions.
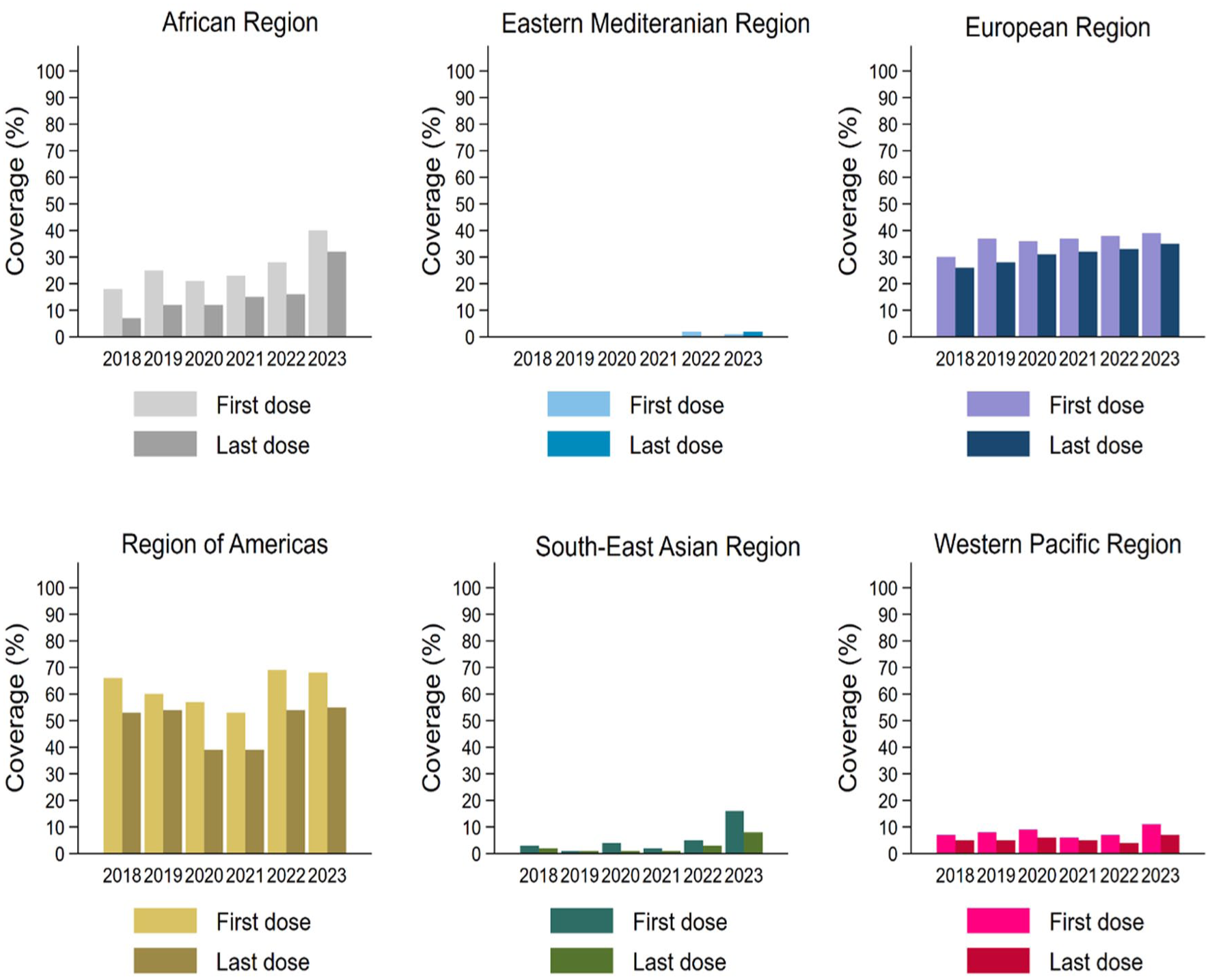
HPV vaccine coverage (first and last dose) among females across WHO regions, 2018–2023.
Logistical and manufacturing constraints
The mass production of L1-VLP vaccines is a sophisticated bioprocess requiring Good Manufacturing Practices (GMP)-certified facilities, precise fermentation technologies, and rigorous downstream purification to maintain particle stability.62,63 The scarcity of such specialized infrastructure in LMICs, compounded by the logistical demands of maintaining a continuous cold chain in remote settings, contributes significantly to global supply disparities. The emergence of regionally produced, cost-effective alternatives such as Cecolin and Cervavac is pivotal in addressing these vulnerabilities. Cervavac’s integration into India’s national immunization program serves as a critical model for improving sustainable access in high-burden, resource-limited environments.64,65
Economic and sociocultural barriers
Human papillomavirus vaccination is highly cost-effective. Evidence consistently demonstrates that even with variable delivery costs, immunization programs yield substantial public health returns by averting cervical cancer mortality, achieving a highly favorable cost-per-disability-adjusted life-year (DALY) averted.66,67 Despite this economic value, implementation in sub-Saharan Africa is hindered by weak health infrastructure, limited political commitment, and cultural stigma. Studies in Tanzania, Kenya, Uganda, and Ghana highlight that inadequate HPV literacy among stakeholders and historical distrust in immunization programs, exacerbated by COVID-19 pandemic disruptions, remain significant impediments to demand creation.68–70
Strategic policy evolutions
The 2022 WHO endorsement of a single-dose schedule for individuals aged 9–20 years represents a landmark shift in global health policy, specifically designed to circumvent persistent systemic hurdles. This transition is anchored by robust clinical evidence from the KEN SHE, DoRIS, and ESCUDDO trials, which collectively demonstrate that a solitary dose elicits a durable immune response and protection against persistent high-risk HPV (HR-HPV) infection comparable to traditional multi-dose regimens.71–73 As of late 2024, over 57 countries have adopted this simplified protocol, resulting in measurable reductions in logistical complexity and national program expenditures. Parallel to dose reduction, the programmatic landscape has been further bolstered by the validation of heterologous schedules. These mix-and-match approaches have proven safe and immunogenic, offering a pragmatic safety net for maintaining coverage during unforeseen supply-chain interruptions or brand-specific stock-outs.66,74 Ultimately, the success of these strategic shifts is contingent upon the implementation of targeted outreach and delivery innovations, which are essential to bridging the gap between vaccine availability and community acceptance.
Strategies to improve HPV vaccination coverage in LMICs
Achieving equitable vaccine coverage in low-income countries (LICs) necessitates a transition from generic immunization models to context-specific, innovative delivery strategies. While school-based programs remain a cornerstone of adolescent immunization, they often fail to reach the most vulnerable, out-of-school populations. Consequently, recent policy shifts have focused on diversifying delivery channels and optimizing healthcare resources to ensure sustainable, high-volume uptake. 66
Integration and hybrid delivery models
A primary catalyst for improving coverage is the adoption of the single-dose HPV vaccination schedule. By reducing the number of required clinical encounters, this approach minimizes logistical hurdles and lowers the opportunity costs for families, particularly in regions where compliance with multi-dose regimens is historically low. 75 To maximize the impact of the simplified schedule, hybrid delivery models are being deployed. These models combine school-based outreach with community-centric initiatives, such as mobile clinics, faith-based health days, and door-to-door campaigns. Integrating HPV immunization with other essential adolescent services, including deworming, menstrual hygiene management, and nutritional screening, has proven effective in normalizing the vaccine and streamlining resource utilization.67,76,77
Community empowerment and digital innovation
Strengthening last-mile delivery relies heavily on the empowerment of community health workers (CHWs). As trusted local intermediaries, CHWs are uniquely positioned to address vaccine hesitancy, counter misinformation, and mobilize caregivers. Training programs that focus on task-shifting enable CHWs to lead education efforts and facilitate follow-up for missed doses, thereby enhancing the resilience of local health systems. This human-centric approach is increasingly augmented by digital innovations. Electronic immunization registries (EIRs) and mobile health applications are being utilized to improve data quality and provide individualized tracking. Text-message reminders and digital scheduling tools have demonstrated significant success in reducing dropout rates and ensuring that catch-up campaigns reach the intended cohorts.76,77
Demand creation and economic sustainability
Sustainable coverage is also dependent on culturally sensitive communication strategies. Engaging religious and community leaders, alongside organizing parent-teacher forums, is essential for building public trust and countering the cultural stigma often associated with HPV. In some contexts, ethically designed incentive-based approaches, such as the provision of school supplies or health vouchers, have served as effective catalysts for participation in underserved areas.78,79 Finally, long-term viability in LICs is anchored in efficient cost management. Strategies such as pooled vaccine procurement through international alliances, task optimization within health workforces, and the integration of vaccination costs into national health insurance frameworks are vital for financial sustainability.61,80 By combining these operational advancements with ongoing equity monitoring, implementation programs can move beyond clinical efficacy toward the actualization of a cervical-cancer-free future.
Next-generation HPV vaccine candidates
As the global health community moves toward elimination targets, research is pivoting to address the limitations of current L1-VLP technology. While highly effective, existing vaccines are genotype-specific and primarily prophylactic. Next-generation candidates are being engineered to provide pan-genotype protection and to serve as therapeutic interventions for established infections. The minor capsid protein, L2, has emerged as a primary target for universal HPV vaccines. 81 Unlike the L1 protein, which varies across genotypes, the N-terminal sequence of L2 contains highly conserved epitopes. Preclinical and early clinical evaluations indicate that multimeric L2 constructs and mRNA-based L2 vaccines can induce cross-neutralizing antibodies against a diverse array of oncogenic types.82,83 In addition to these L2-based strategies, high-valency L1-based formulations are also expanding coverage. A notable candidate is SCT1000, a recombinant 14-valent VLP vaccine that covers five additional HR-HPV types (HPV-35, 39, 51, 56, 59) beyond those included in Gardasil 9. Currently in Phase III evaluation, SCT1000’s immunogenicity is being rigorously assessed using pseudovirion-based neutralization assays and Luminex total IgG immunoassays to confirm broad-spectrum efficacy (NCT06041061). 84 Complementing these efforts, the RG2-VLP vaccine utilizes a dual-component strategy to target both α-HPV and β-HPV types by incorporating L2 protective epitopes. 85 Collectively, these advanced approaches are vital for regions where diverse HR-HPV genotypes predominate, offering a more comprehensive solution than traditional VLP formulations.
Therapeutic vaccines and immunotherapy
In contrast to prophylactic formulations, therapeutic vaccines are designed to stimulate cellular immunity against infected or transformed cells by targeting the viral oncoproteins E6 and E7. DNA vaccines, such as VGX-3100, have already demonstrated clinical efficacy in reducing CIN 2/3 lesions and clearing persistent HPV-16 and 18 infections. 86 Current research is exploring a variety of innovative platforms.
Peptide and liposomal vaccines
Synthetic long peptide vaccines like ISA101b have shown promise in Phase II trials, particularly when paired with anti-PD-1 therapies. 87 Similarly, the liposomal vaccine PDS0101 utilizes the Versamune platform to induce potent CD8+ T-cell responses. 88
Vector-based platforms
Viral and live-attenuated bacterial vectors, such as ADXS11-001, are being evaluated for their ability to promote tumor regression through enhanced antigen presentation.89,90
Synergistic combinations
A major breakthrough in therapeutic oncology is the combination of vaccines with immune checkpoint inhibitors, such as PD-1 blockade, which produces synergistic antitumor effects by revitalizing exhausted T cells within the tumor microenvironment.91,92 Furthermore, the early genes E1 and E2 have emerged as viable targets due to their high sequence conservation and ability to limit viral persistence. Multigene vaccine constructs incorporating E1, E2, E6, and E7 have demonstrated superior immunogenicity and tumor suppression in preclinical models, representing the next frontier in curative HPV interventions (Table 3).93–95
Therapeutic HPV vaccine candidates targeting HPV-associated disease.
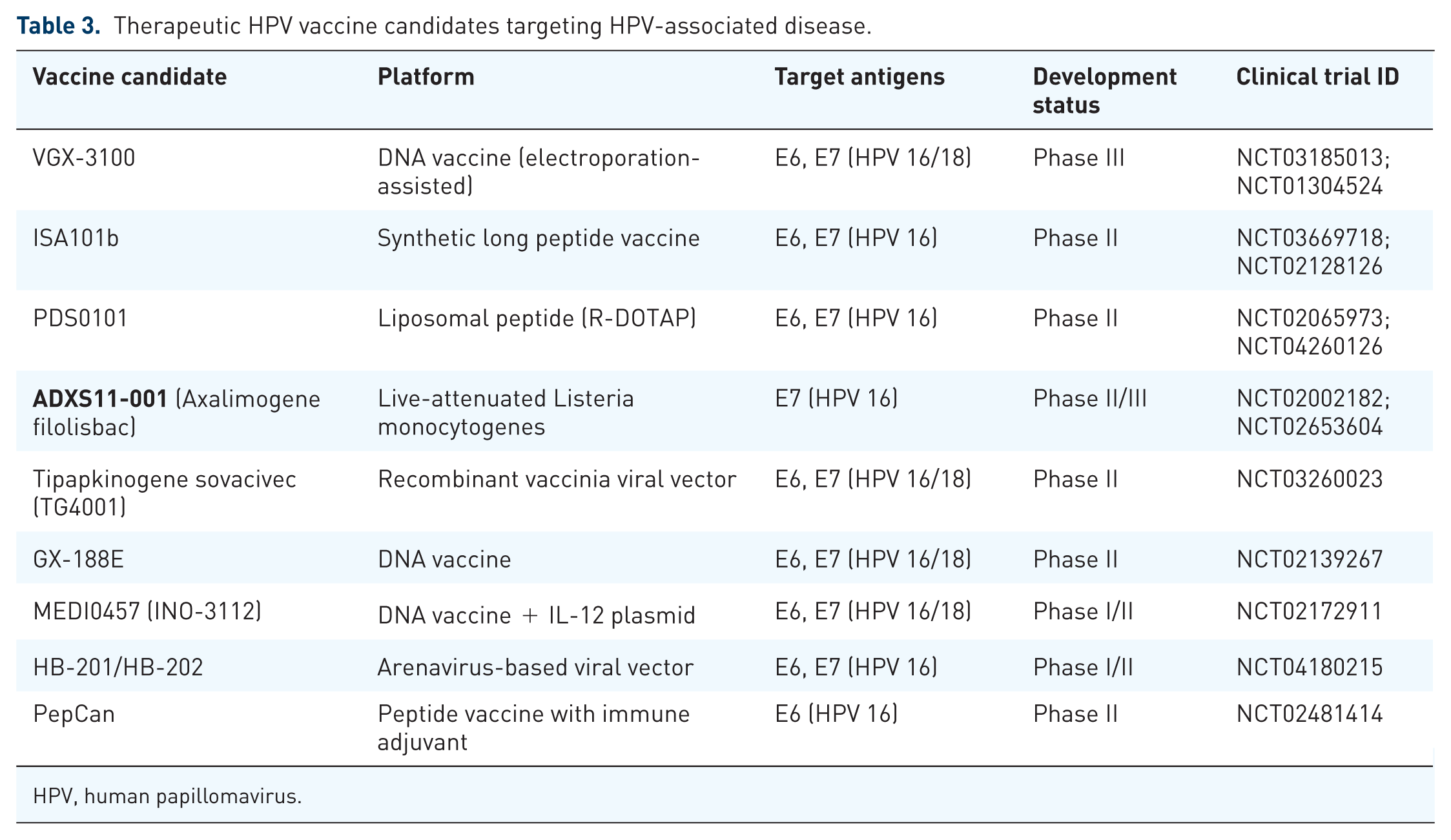
HPV, human papillomavirus.
Role of HPV vaccines in cervical cancer control
The implementation of HPV vaccination represents a pivotal advancement in preventive oncology. By targeting high-risk genotypes, specifically HPV-16 and HPV-18, widespread immunization, ideally administered prior to sexual debut, fosters robust herd immunity. 96 This has led to demonstrable, long-term reductions in HPV prevalence, the incidence of genital warts, and the burden of CIN.96,97 Nations that have successfully integrated high-coverage vaccination with systematic screening, such as Australia and the United Kingdom, have recorded precipitous declines in cervical cancer rates, with current trajectories approaching the WHO elimination threshold of fewer than 4 cases per 100,000 women.98,99 The maturation of regional vaccine production, exemplified by Cecolin and Cervavac, has been instrumental in extending these benefits to LMICs where the disease burden is disproportionately high. Ongoing surveillance continues to affirm the sustained global impact of these formulations in reducing the incidence of HPV-related malignancies. 100
The emerging therapeutic landscape
While a licensed therapeutic HPV vaccine remains pending, the clinical pipeline is robust, with over 20 candidates currently in development.23,101 Meta-analyses of Phase II/III trials involving these candidates have reported promising clinical activity, with mean regression and clearance rates for CIN 2/3 lesions reaching 62.5% and 48.6%, respectively.102,103 Innovative platforms are demonstrating significant potential in early-phase trials.
Viral vector and oral platforms
The oral vaccine IGMKK16E7 and the viral vector-based Tipapkinogen Sovacivec have shown favorable safety and immunogenicity in patients with high-grade lesions.104,105
Immunotherapy synergies
Early findings for Vvax001 in HPV-16-positive CIN three patients highlight the feasibility of inducing targeted clinical benefits. 106 Evidence suggests that therapeutic vaccines can overcome local immunosuppression within the tumor microenvironment when combined with adjuvants or immune checkpoint inhibitors, such as anti-PD-1/PD-L1 antibodies.92,106
Future perspectives in curative strategies
The next decade of cervical cancer control will likely be defined by multi-modal integration. Combining vaccines with conventional radiotherapy, chemotherapy, or checkpoint blockade may synergistically enhance antitumor immunity and prevent disease recurrence. Furthermore, the application of CRISPR/Cas9 genome-editing tools to specifically target and disrupt E6/E7 loci has demonstrated potent tumor suppression in preclinical models, representing a potential curative molecular intervention.107,108 Strategies to augment immunogenicity through the use of nanoparticles, novel adjuvants, and co-stimulatory signals are also under active investigation. By aligning these biotechnological milestones with the WHO’s 2030 elimination targets, the global healthcare community is positioned to transition from disease management to the definitive eradication of cervical cancer as a public health threat.
Discussion
The transition to a single-dose HPV vaccination schedule represents a pivotal evolution in immunologic strategy, moving away from rigid multi-dose frameworks toward high-impact, evidence-based flexibility. As demonstrated by the KEN SHE, DoRIS, and ESCUDDO trials, the comparable efficacy of a single dose against persistent HR-HPV infection provides a robust scientific mandate for the WHO’s updated guidelines.71,109 This shift is not merely a clinical convenience but a structural necessity; the adoption of simplified protocols by over 54 countries, including expanded national rollouts across sub-Saharan Africa, underscores a global appetite for interventions that minimize logistical friction and optimize resource allocation in resource-constrained settings.
Innovations in next-generation vaccines are further addressing the limitations of current L1-based VLPs. While L1 VLPs are highly immunogenic, they provide largely type-specific protection, necessitating complex multivalent formulations to cover diverse oncogenic strains. Emerging candidates targeting the minor capsid protein (L2) utilize highly conserved N-terminal epitopes to induce broad-spectrum, cross-neutralizing antibodies. Although L2 antigens are naturally less immunogenic than L1 VLPs, new delivery platforms, such as bacteriophage VLPs and mRNA-based L2 scaffolds, are overcoming this by presenting these conserved epitopes in highly repetitive, immune-engaging arrays. These advancements suggest a future where a single, low-cost vaccine could provide near-universal protection against both mucosal and cutaneous HPV types.
Furthermore, the integration of heterologous schedules and thermostable formulations, such as those utilizing controlled temperature chain (CTC) strategies, bolsters supply-chain resilience. 110 By establishing that mixed-vaccine regimens are safe and immunogenic, public health systems can mitigate the risks of manufacturing shortages and delivery interruptions. Ultimately, the success of these strategic shifts is contingent upon bridging the last-mile gap through targeted community outreach and school-based programs. These strategies address the sociocultural determinants of vaccine hesitancy, ensuring that the theoretical benefits of simplified dosing and broader valency translate into sustained, equitable vaccine coverage and the global elimination of cervical cancer.
Limitations
This review is subject to several limitations inherent to its narrative design. Unlike a systematic review, the qualitative synthesis of literature may be susceptible to selection bias, focusing primarily on high-impact, English-language trials. Methodologically, the absence of a quantitative meta-analysis precludes a statistical comparison of effect sizes across the diverse global cohorts studied. Clinically, while the evidence supporting single-dose efficacy and heterologous schedules is robust, long-term longitudinal data exceeding 15 years are still required to confirm the duration of protection relative to multi-dose benchmarks. Furthermore, data remains sparse regarding the immunogenicity of simplified protocols in immunocompromised populations, particularly those living with HIV. Finally, the long latency between HPV infection and malignancy means the definitive impact of these recent policy shifts on cervical cancer mortality will not be fully measurable for several decades.
Conclusion
The HPV vaccination landscape is shifting toward evidence-based programmatic flexibility, supported by the validation of single-dose efficacy and heterologous schedules. These advancements, alongside the clinical maturation of L2-based and mRNA platforms, provide a transformative toolkit to overcome historical barriers to vaccine equity. However, realizing the full potential of these innovations requires bridging delivery gaps through localized and school-based interventions. Future research should prioritize long-term effectiveness of emerging vaccine platforms, durability of single-dose protection across diverse populations, and implementation strategies that improve uptake in low-resource settings. By aligning technical breakthroughs with sustained political commitment and context-specific evidence, the global community can achieve the WHO 2030 targets and eventually eradicate cervical cancer as a public health threat.