
Abstract
Complementary and alternative medicine (CAM) practices have been widely adopted for thousands of years in the Eastern world. Integration of such approaches into the conventional medicine model has been limited, however, and there continues to be a paucity of data describing the extent of CAM usage in the US. The purpose of this investigation was to derive nationally-based estimates of CAM utilization among a large sample of adults who completed the 2022 National Health Interview Survey (NHIS). In this cross-sectional analysis, chi-squared tests and multivariate logistic regression models were used to identify factors associated with CAM use. Among 27 651 adults completing the survey, approximately 37% reported participating in at least one CAM activity in the past 12 months. CAM users were more likely to be of younger age, female sex, have obtained higher levels of education, have increased anxiety and report having better overall health. Meditation (18%), yoga (15%), chiropractic care (11%), and massage therapy (11%) were the most frequently reported modalities, while fewer than 5% of respondents visited an acupuncturist or naturopath or participated in art or music therapy. The main reason for CAM utilization was to improve overall health. Findings from this study indicate that approximately one-third of US adults engage in some form of CAM activity and that better health outcomes were associated with these practices. Additional research is needed to better understand the barriers and facilitators of CAM use and to further qualify which factors may influence the decision to (or not to) engage in such practices.
Keywords
Introduction
For thousands of years, people worldwide have practiced complementary and alternative medicine (CAM) approaches. These modalities are deeply ingrained in many healthcare therapies of Asia and the Middle East, where the models of care rely heavily on the use of herbal medicines, naturopathy, and homeopathic healing as the primary treatment strategies.1-3 Such Traditional Medicine (TM) practices are based on empirical methods and ancient wisdom, incorporating a holistic approach of healing the mind, body, and spirit to establish harmonization within the individual. This model of care focuses on treating the patient with the disease rather than focusing solely on the disease itself. Alternatively, Conventional Medicine (CM), often referred to as Western Medicine, utilizes an evidence-based, disease-focused approach to diagnose and treat illness, relying on scientifically proven methods to identify and address the underlying biological mechanisms responsible for the condition. 4 Given the foundational differences between the TM and CM systems of care, the two approaches have historically resulted in minimal overlap. Advances in integrative health in recent years have sought to bring together conventional and complementary approaches for whole-person health and to explore the barriers and facilitators to CAM, which has traditionally been underutilized by health care providers and patients. 5
Although it has been suggested that rates of CAM utilization appear to be increasing in the Western world, 6 there are limited reports describing national estimates of CAM use among adults living in the United States (US). Additionally, there remains a gap in the literature regarding comprehensive analyses that integrate multiple mind-body modalities with demographic and health-related correlates, as well as motivations for use. The purpose of this investigation is to provide population-based estimates of CAM utilization practices among US adults based on a large, nationally representative sample of individuals completing the National Health Interview Survey (NHIS) in 2022. The present study compares demographic and health characteristics of users and non-users of CAM and describes the extent to which selected approaches are being adopted in the general population. Factors associated with CAM utilization, as well as reasons for use, are also explored. These data provide descriptive insights into patterns of CAM use that may inform future research regarding integration of these practices into the framework of conventional care.
Methods
NHIS Study Design and Data Collection
The NHIS study is directed by the Centers for Disease Control and Prevention and aims to collect national longitudinal data on a range of health indicators, including (but not limited to) health status and behaviors, illness and chronic conditions, preventive services, and access to care. 7 The main survey is conducted annually to provide a cross-sectional representation of the nation's general overall health and is additionally used to assess trends in these domains over time. Each year, a variety of specialty topics are included in the survey to further explore conditions, practices, and other factors that are not represented in the main survey. In 2022, the questionnaire included a set of supplemental questions related to the use of CAM modalities. Information was collected on whether the following types of CAM were practiced within the past 12 months: acupuncture, chiropractic care, massage therapy, naturopathy, art therapy, music therapy, meditation, yoga, guided imagery or progressive muscle relaxation, and whether these activities were used to assist with pain relief and/or overall health. Beyond these latter two items, the survey did not inquire about other motivations for CAM use. Additionally, data were not collected regarding the extent and duration of use, nor how the modalities were practiced.
Population
The present investigation included all (n = 27 561) adult respondents who completed the NHIS 2022 survey.
Outcome Measures
Any CAM use was defined as a positive (“yes”) response to at least one of the listed practices in the NHIS supplemental survey within the past 12 months. As such, analyses were based on the set of restricted complementary approaches collected in the survey.
Statistical Analyses
For the present investigation, demographic factors included age, sex, race, ethnicity, level of education, marital status, and ownership of health insurance. Variables related to overall health and wellness included general health status, history of diabetes, hypertension, and hypercholesterolemia, body mass index, history of cancer, extent of anxiety and depression, tiredness, frequency of moderate physical activity, and number of hours of sleep per night. Unweighted descriptive statistics (N and %) indicating the distribution of each demographic factor and other variables related to overall health and wellness, stratified by any CAM use, are presented. Unadjusted chi-squared tests were performed to evaluate differences between users of CAM versus non-users with corresponding (two-sided) P-values <.05 considered to be statistically significant. Rates of utilization for each specific approach are presented, along with the overall prevalence of engaging in any CAM practice.
To account for the NHIS complex sampling design, additional analyses were performed in which survey weights were applied. Weighted prevalence estimates of CAM use were calculated and weighted logistic regression analyses were performed to assess associations between CAM use and demographic as well as health-related factors. Odds ratios (OR), 95% confidence intervals (95% CI) and Wald-statistic P-values are reported.
SPSS Version 21 (including the complex samples module) was used to conduct the analyses.
Results
The distributions of demographic characteristics among adult respondents of the NHIS 2022 survey are presented in Table 1. The data are stratified by those who reported utilizing at least one CAM practice within the past 12 months (n = 10 404) compared with those who did not (n = 17 247). Individuals who engaged in CAM activities were significantly younger, more likely to be female, less likely to be Black and Hispanic, and more likely to have higher educational attainment than non-users (P < .001).
The Distribution of Demographic Variables Stratified by CAM Use Among NHIS 2022 Participants.
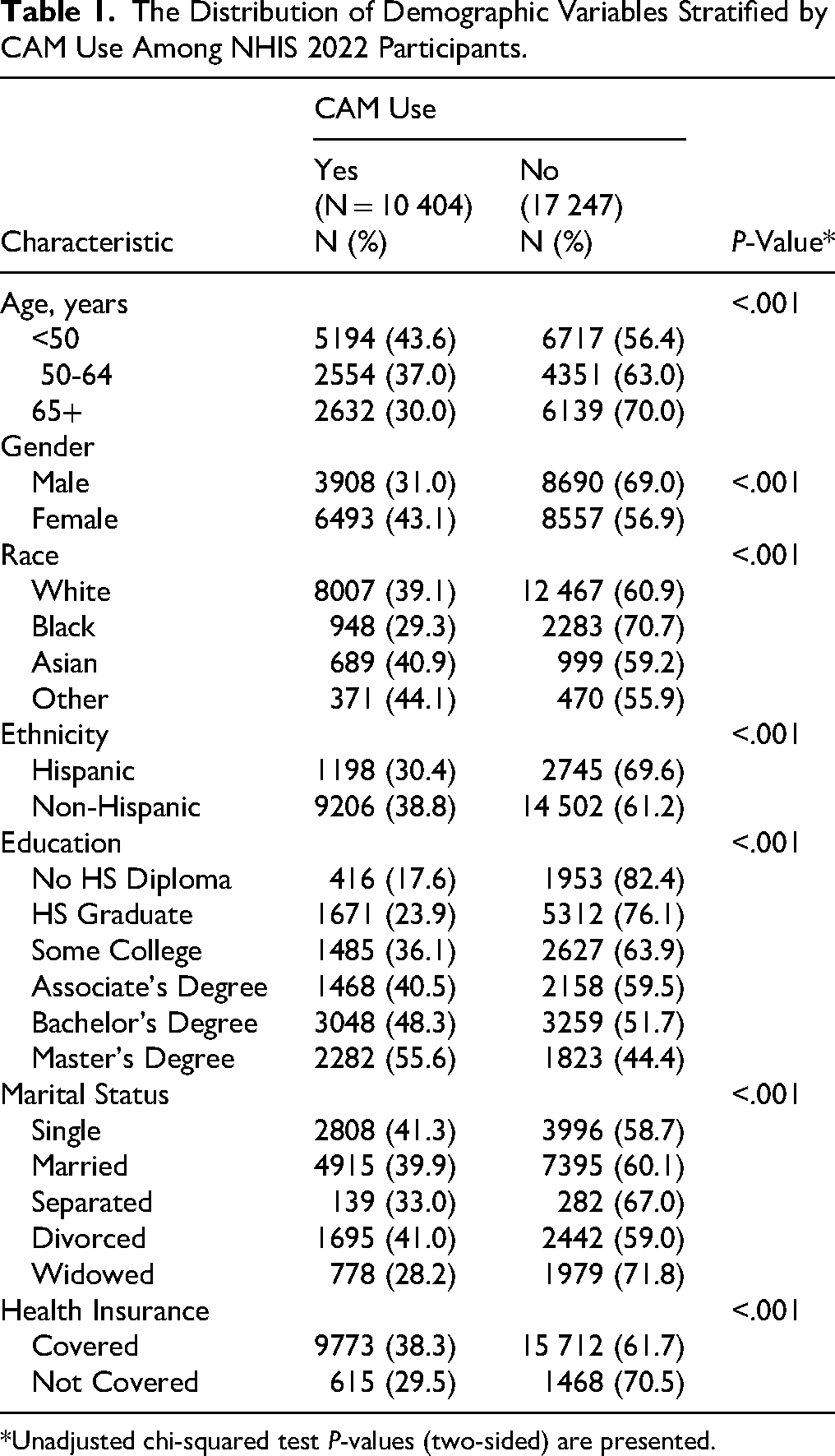
*Unadjusted chi-squared test P-values (two-sided) are presented.
Table 2 presents the distribution of health and wellness factors stratified by CAM use. The findings indicated an association between engaging in CAM practices and being in better general health, as well as having fewer comorbidities (eg, diabetes, hypertension, and hypercholesterolemia) (P < .001). Additionally, individuals with increased feelings of anxiety and depression reported a higher rate of CAM use than those who reported not feeling anxious or depressed as often (P < .001). Likewise, CAM use was higher among people who were more tired and those who tended to exercise more frequently (P < .001).
The Distribution of Health and Wellness Factors Stratified by CAM use Among NHIS 2022 Participants.
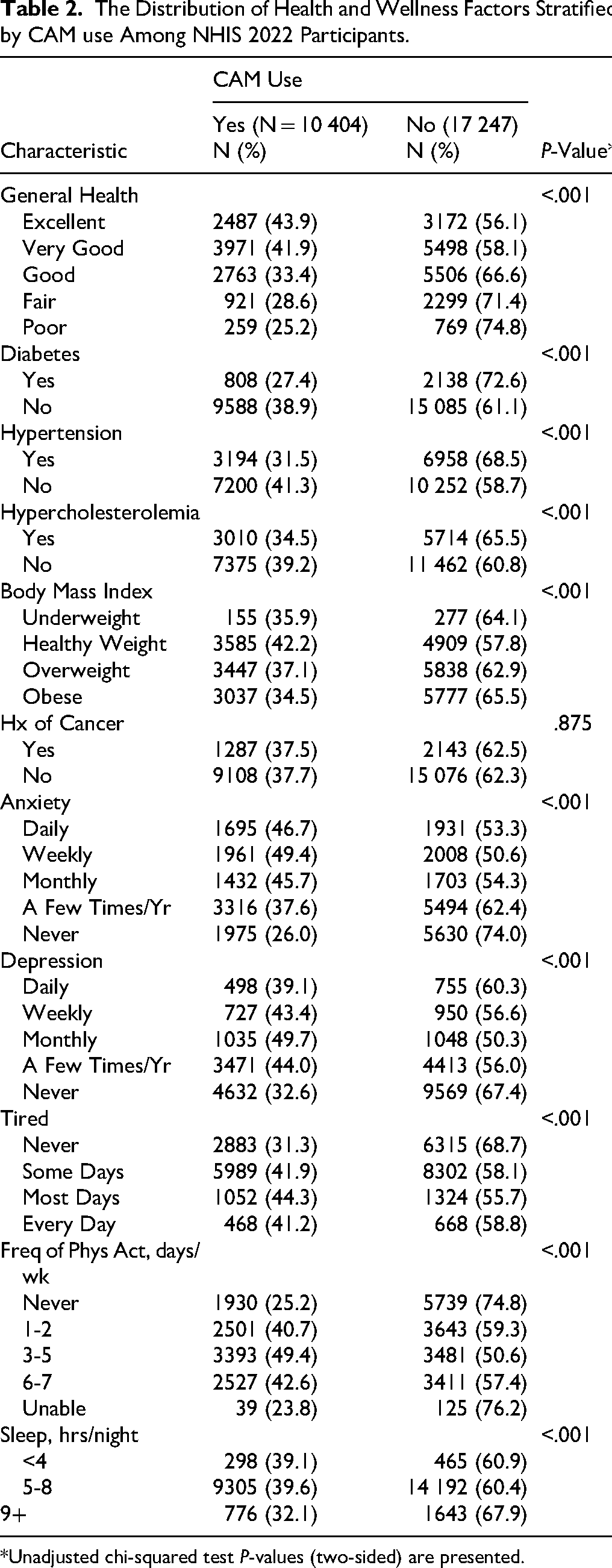
*Unadjusted chi-squared test P-values (two-sided) are presented.
While the rate of any CAM use among survey participants was 37.6%, the frequency of utilization of the various practices varied widely. Table 3 presents the percentage of participants who engaged in each modality within the past 12 months. Fewer than 5% of individuals visited an acupuncturist or naturopath or participated in art or music therapy in the prior year. Approximately 11% had seen a chiropractor or had received a massage, while 15.5% practiced yoga and 18% engaged in some form of meditation. Although a small percentage of individuals utilized these various modalities for the purpose of pain relief, the majority reported engaging in these practices for the goal of improving overall health.
CAM Practices Among NHIS 2022 Participants.
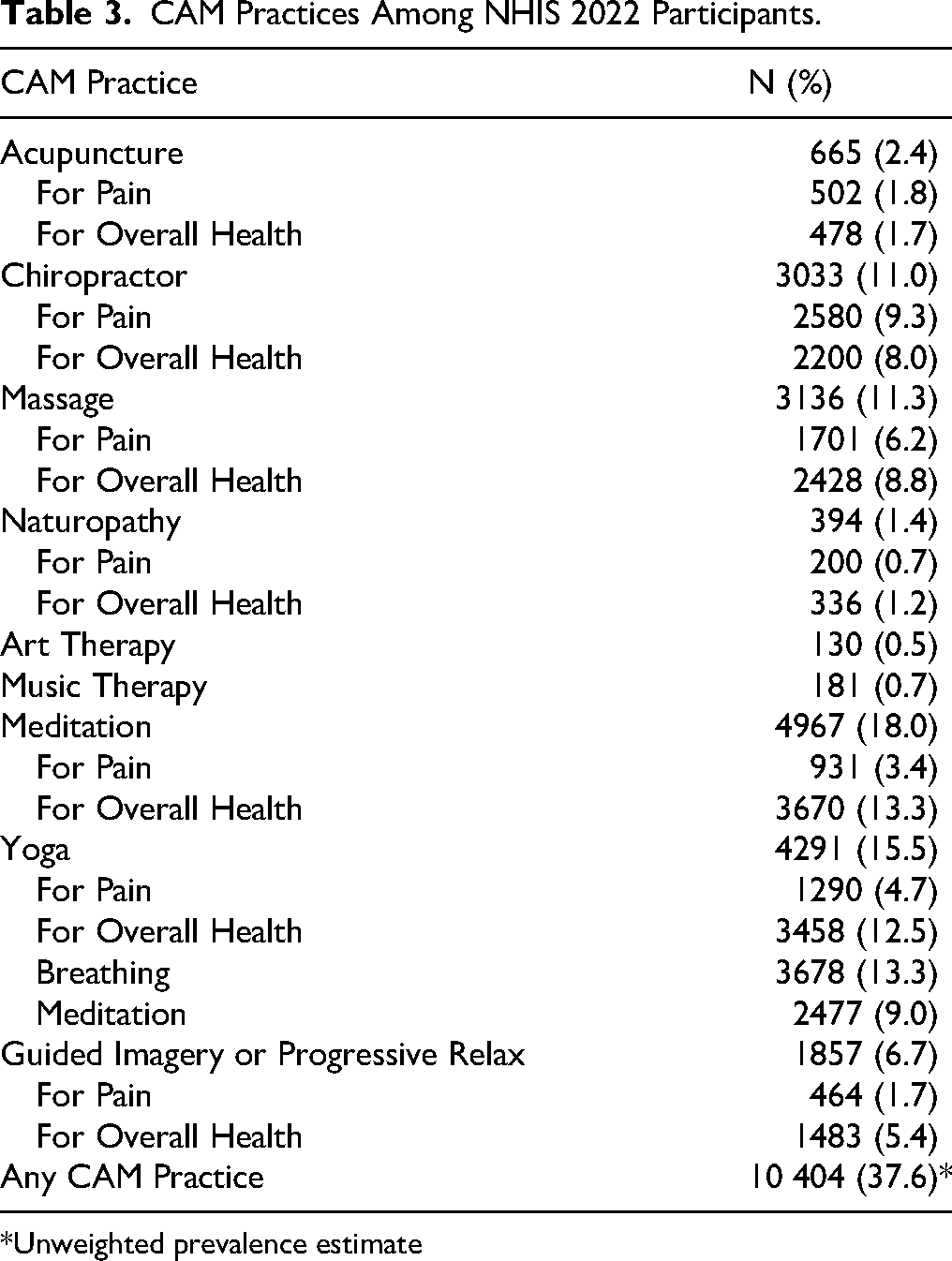
*Unweighted prevalence estimate
When applying weights to account for the NHIS complex sampling design, the estimated prevalence of CAM use was 36.6%. The weighted multivariable logistic regression models to evaluate associations between CAM use and demographic as well as clinical factors are presented in Table 4. The findings indicate that factors associated with CAM utilization include younger age, female sex, higher educational attainment, increased levels of anxiety, and self-reports of better overall health. While having insurance coverage was not found to be associated with CAM use (OR = 1.06 (0.92, 1.22), P = .412), individuals with a history of cancer were more likely to participate in these practices than those without such diagnosis (OR = 1.16 (1.04, 1.29), P = .008).
logistic Regression of Factors Associated with CAM use.
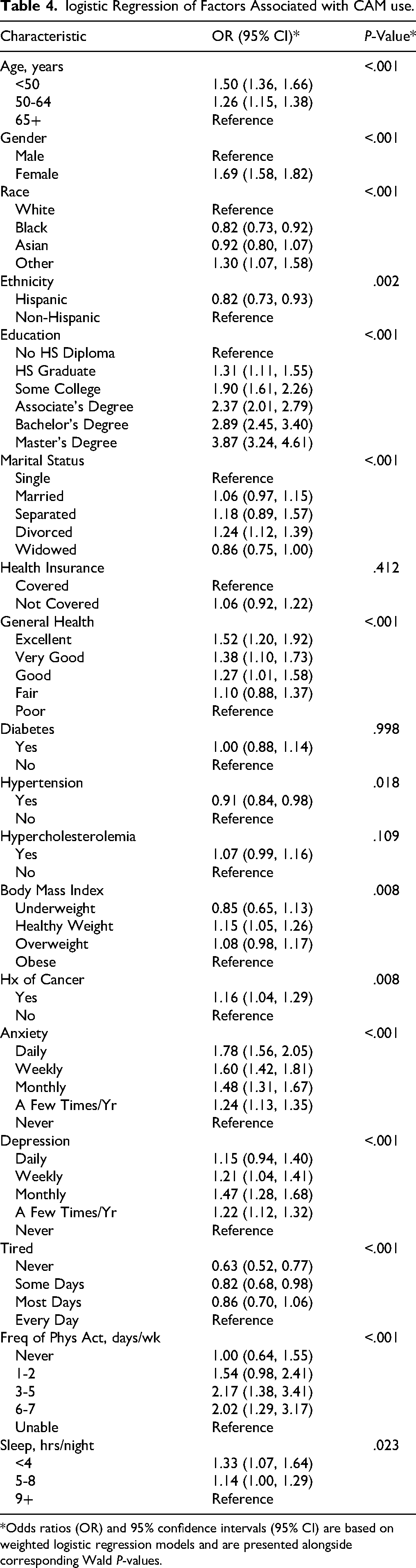
*Odds ratios (OR) and 95% confidence intervals (95% CI) are based on weighted logistic regression models and are presented alongside corresponding Wald P-values.
Discussion
CAM utilization rates vary widely, with recent publications estimating global usage ranging between 24% and 73%. 8 Higher rates tend to be more prominent in countries that follow TM approaches to healing and have cultural roots mainly originating in the Eastern world. 9 In contrast, the US continues to operate within a predominantly biomedical model of care, where treatment typically focuses on disease management through pharmaceutical, medical, or surgical interventions. Consequently, the integration of CAM modalities into routine clinical practice has historically been limited. Despite this dissimilarity, evidence suggests that CAM use in the U.S. has been increasing over the past two decades. 6 National estimates, however, have been sparse, and most reports describe usage among particular subgroups with personal motivations, such as those seeking symptom management and/or treatment of various health conditions. 10 Furthermore, motivations such as seeking greater control over personal health and aiming to improve well-being have been reported, 10 as have perceptions that conventional medicine is inefficient. 11 Taken together, these factors underscore the challenge of determining the true extent and magnitude of CAM use in the general population, which remains largely unknown. Existing estimates have been difficult to compare because of differences in study design, scope, and the practices being evaluated.
Findings from the present investigation indicate that in 2022, approximately 37% of US adults participated in at least one form of CAM within the past 12 months. Meditation and yoga were the 2 most commonly used practices, reported by 18% and 15% of the population, respectively, and these statistics represent more than a 2-fold increase in meditation and a 3-fold increase in yoga practice over the rates reported by the NHIS over the past 2 decades.6,8 Those who reported engaging in CAM activities tended to be younger, more highly educated, and in better overall health than those who did not practice, yet the directionality of these relationships remains unclear. It is yet to be determined whether healthier individuals are more inclined to use CAM practices or whether these modalities are improving health outcomes. Therefore, additional research is required to identify barriers and facilitators to CAM utilization and to clarify the complex and bidirectional relationships among demographic, psychosocial, and health-related factors that shape the adoption of these therapies. Personalized approaches to CAM adoption may be instrumental in assisting with the integration of such practices into conventional medicine. 12
National Prevalence Estimates of CAM and Associated Factors for CAM use
Although increases in selected CAM practices may suggest a rise in CAM use in the US, one cannot readily conclude that such increases equate to higher CAM rates in general. Additionally, although the reported estimates were based on data collected by the NHIS in 2012, 2017, and 2022, the questionnaires were not standardized, thereby making interpretation of the findings somewhat challenging.6,8 In 2012, the supplemental survey included approaches such as deep breathing exercises, meditation, and chiropractic and osteopathic manipulation, as well as product use (eg, dietary supplements and herbal preparations) within the previous 12 months. Using those metrics, the reported rates of any CAM use ranged between 32% and 36%.13-21 In 2017 and 2022, the study continued to collect information on mind-body practices but did not obtain data related to product use, therefore limiting the opportunity for direct comparisons of certain therapies, as well as evaluations of more general temporal trends.
In addition to the noted difficulties with evaluating CAM use trends over time, utilization rates have mainly been based on investigations that have included only a small subset of modalities, most of which did not provide detailed information pertaining to particular therapies, extent of practice, or motivations for use. The majority of existing studies have collected information on modality categories rather than individual products and/or practices. To complicate matters further, there is variability in how individual investigations define “CAM use” in terms of time frame and type of engagement. For example, some surveys inquire about “ever” using CAM, whereas others assess only practices used within the past 12 months. Furthermore, some capture information about “consulting” with a practitioner, whereas others define use as personally engaging in a self-care practice or receiving the therapy from a provider.17,18,20 Each of these nuances may substantially influence reported rates of CAM use and ultimately makes it difficult to compare estimates across studies.
The inclusion and exclusion of particular practices are also likely to significantly influence estimates of CAM utilization. 8 For example, studies that include prayer have reported increased rates compared to those that do not consider spiritual practices. 22 Similarly, some investigations may consider osteopathic care as a CAM practice, while others may not, 23 thus inflating or deflating the estimates accordingly. Likewise, certain groups may be more or less inclined to use CAM practices than others, although the directionality of such factors is not always clear. For instance, in a recent systematic review, individuals in the US without health insurance were reported to be 50% more likely to seek care from a CAM provider, 8 whereas findings from the present study indicate that health insurance coverage was not associated with CAM utilization. These findings suggest that adoption of such practices is likely to be multi-factorial and shaped by a constellation of factors, including motivation for use.
Intention is a key component to consider when evaluating CAM utilization. Strong motivating factors for exploring these approaches include disease, symptom management, and improving well-being and overall health. As such, a number of smaller studies have examined rates of CAM use among sub-populations, particularly those who have been diagnosed with cancer. In one multi-institutional analysis of 749 patients in the US, 77.8% reported using at least one of ninety listed CAM options for their cancer care. 24 The three main goals of CAM use were management of symptoms (42.2%), treatment of cancer (30.4%) and assistance with mental health challenges (11.8%). In a second study of 658 patients with cancer, the prevalence of twenty-one CAM approaches was 66.11% with prayer and spirituality reported as the most commonly practiced CAM modalities. 25 It remains unclear whether the higher rates of utilization in the two aforementioned studies compared to those reported for the general population are a result of the added sequelae experienced by individuals with cancer, the wider variety of CAM therapies included in these investigations compared to the national surveys, or a combination of these and other factors influencing the outcomes.
So, while the number of studies aimed at assessing both prevalence and effectiveness of CAM utilization practices continues to grow, interpretation of the findings has been hampered by several challenges, including (but not limited to) the heterogeneity of approaches, varying outcome measures, participation and selection biases, and often limited sample sizes. Additionally, even among investigations assessing the same CAM modality, the specific elements vary widely. Yoga, for example, has several different styles of practice and countless variations of poses, breathing exercises, and mindful awareness activities.1,26 Given the variability in movement type, intensity, and duration of practice; differences in breathwork exercises; diversity of mindfulness-based techniques; and the extent to which each of the mind-body components are incorporated into the sessions, it becomes increasingly difficult to compare efficacy within and between practices.
How is CAM Currently Defined?
The present “definition” outlined by the National Center for Complementary and Integrative Health (NCCIH) subdivides CAM practices into three general categories that may overlap. 5 These incorporate nutritional, psychological, and physical approaches, which represent therapies related to natural products, as well as mind-body practices. Nutritional therapies may include (but are not limited to) pre- and probiotics, phytochemicals, plants and botanical drugs, herbs and spices, dietary supplements, and food/diet regimens. While mindfulness, spiritual practices, and psychotherapy are mainly considered psychological practices, manual therapies (eg, chiropractic and osteopathic), as well as heat/cold therapies, are generally classified as physical practices; many mind-body techniques combine elements from both domains. Additionally, the lines between what might be considered conventional medicine and CAM are not always clearly delineated. There is considerable subjectivity in determining which practices may be integral components of the conventional health care model (eg, psychotherapy, osteopathy, etc) and which may more likely be classified as non-Western CAM activities (eg, yoga, tai chi, etc). This “gray” zone can significantly impact estimates of CAM use. 8
In an effort to better estimate the true prevalence of CAM use in the general population (and in particular subgroups), it is necessary to begin by developing standardized data collection protocols that clearly delineate the types of therapies, along with measurable outcomes that will more accurately quantify use and facilitate meaningful comparisons across studies. Operational definitions must be developed to not only provide a well-defined list of approaches but also specify time frames for practice (eg, ever, 30 days, 12 months, etc), duration of practice (eg, number of times per week, length of time per session, etc), and details related to the specific practice modality. It is important, for example, to differentiate factors such as whether one is receiving care or engaging in self-practice and provide the details within a given therapy, as there may be a significant number of variations within the same practice. Likewise, with regard to nutritional supplements and botanicals, the dose and mechanism of ingestion (eg, pill, injection, cream, suppository) should be considered, along with dietary intake. Additionally, it is important to identify the intention for use (eg, health promotion, disease prevention, treatment, relief of symptom burden, etc), as these factors will likely influence or dictate the extent to which the products are adopted.
To accurately measure CAM use and enable valid cross-study comparisons, it is not only imperative to develop standardized definitions and reporting guidelines to detail the practices, knowledge, geographical and cultural influences, and other factors that may impact utilization of these modalities but also to ensure that data collection instruments include items designed to assess one's healthcare goals, personal beliefs in the efficacy of conventional care, and motivations for use/non-use of CAM, since these factors are likely to influence the willingness to integrate CAM approaches into healthcare decisions. If the desired outcome, for example, is solely to cure disease and there is a strong belief that existing therapeutic agents and procedures will effectively do so, the inclination to engage in CAM practices may be lower than if one is additionally seeking symptom control or a more general sense of overall wellness. 27 As such, assessing motivation is pivotal to understanding why CAM therapies may or may not be considered beneficial, particularly among those who primarily rely on a conventional healthcare model.
Integration of CAM in Medical Practice
A worldwide systematic review of 231 publications indicated that the top 3 reasons for using CAM modalities were (1) an expectation of benefits; (2) dissatisfaction with CM; and (3) perceived safety of CAM therapies. 11 The main motivations for use were treatment of illness, symptom relief, mitigating side effects of CM, preventing disease, and maintaining overall well-being. This study also noted that satisfaction with CM was a significant factor for not using such practices and that the existing literature included significantly more publications of CAM use among “condition-specific” groups such as those diagnosed with high blood pressure and stroke, for example. 28 While some studies have explored CAM utilization in primary care, 29 the largest number of studies to date have been conducted among patients with and survivors of cancer, particularly those with breast cancer. Reports indicate that patients with a diagnosis of cancer may be more willing to try CAM approaches than other condition-specific populations, particularly to address the unpleasant side effects of chemotherapy and other cancer-related treatments.11,25 In a multi-institutional analysis including 749 patients with cancer, 77.8% reported utilizing at least one CAM modality, and more than 90% of patients used these therapies in addition to (not in place of) conventional treatment. 24
As a result of the growing interest in CAM's potential therapeutic benefits for disease management in recent years, many cancer treatment centers in the US have established integrative health care programs to assist with addressing early and late effects related to cancer treatment and to aid in the management of related symptoms such as fatigue, insomnia, anxiety and depression, pain, and issues with mobility. 28 These “integrative” models of holistic care have aimed to coordinate conventional and complementary approaches in various combinations to address the needs of the whole person. In 2017, a systematic analysis of NCI-designated Comprehensive Cancer Centers indicated that 45 centers had developed websites related to integrative medicine. 30
Although organizations such as the Society of Integrative Oncology (SIO), 31 the American Society of Clinical Oncology (ASCO) 32 and the National Comprehensive Cancer Network (NCCN) 33 have led the way in the past decade by developing frameworks for implementing CAM approaches alongside more evidence-based practices, physicians who practice CM typically do not receive a formal education related to CAM during their medical training. This void results in a lack of provider knowledge about such practices, which may subsequently contribute to reduced communication about CAM use with their patients.24,34,35 One study found that fewer than 20% of patients report that their cancer physicians are a source of information related to CAM. Instead, family/close friends (53%), distant friends (28.5%), social media (26%), and websites (25%) are the main sources for obtaining information related to their health. 24 Not surprisingly, there is a significant amount of circulating misinformation, with an estimated one-third of cancer treatment social media posts containing incorrect messaging and three-fourths of these posts providing potentially harmful information.36-40
Although it has been shown that engaging in dialogue with oncologists tends to improve patient safety and treatment efficacy, as well as patient trust,24,41-43 27%-50% of patients reportedly do not disclose their CAM practices to their oncologists.24,27,44-46 Common reasons for non-disclosure are beliefs related to a provider's lack of interest and knowledge regarding these practices, anticipation of the practitioner's disapproval, and perception that CAM is irrelevant to conventional care.27,47-52 From the provider perspective, there are concerns about potential interactions and toxicities when CAM therapies are used alongside oncology treatments, as well as possible impacts on the effectiveness of conventional treatment practices (eg, potential delays in seeking care).24,45,53-55 Such concerns likely contribute to provider hesitancy to discuss or recommend CAM therapies. So, while results from the National Ambulatory Medical Care Survey indicated that 50% of US office-based physicians recommended at least one CAM practice to their patients, 29 there appears to be greater hesitancy reported among oncologists, 27 reflecting the specialized concerns and risk perceptions in cancer care. This highlights the need for enhanced communication, provider education, and evidence-based guidance to support safe and informed CAM discussions in oncology.
A recent international cross-sectional survey among oncology researchers and clinicians indicated that 93% reported that CAM practices lacked scientific evidence for safety and efficacy, and almost 20% were skeptical about their effectiveness. 27 Additionally, 41% were unsure if body-based practices were safe, 35% were unsure if such practices should be integrated into mainstream medicine, and 31% reported not being comfortable counseling patients about whole medical systems (defined as including Ayurvedic medicine, traditional Chinese medicine, acupuncture, homeopathy, and naturopathic medicine). A total of 39% believed that clinicians should receive formal training, and half of those surveyed favored the need for supplemental education. This survey underscores the need for additional research to understand the clinical utility of CAM modalities, as well as their safety and effectiveness, in order to better facilitate an evidenced-based approach for integration of these therapies into conventional medicine practice.
Study Limitations
While the NHIS is one of the largest nationally represented studies available to date describing CAM use in the US, the data are limited to a small subset of modalities that were not well-defined. The data set of this investigation did not include metrics related to the specific components of CAM modalities, their frequency, duration, or user motivations. As such, findings from the present investigation should be interpreted in this context along with the caveat that statistical significance does not necessarily equate to clinical significance. Additionally, the survey focused mainly on mind-body practices but did not include nutritional, psychological, and other potentially prevalent CAM therapies, such as prayer and spiritual practice. Of further note, the total household response rate for the NHIS 2022 survey was 49.6% and the final interview completion rate for sample adults was 47.7%, thereby introducing the potential for selection, reporting, and other biases which may limit generalizability of the findings. Despite these limitations, however, the NHIS data add to a growing evidence base describing CAM use among adults in the US and highlight the need for further exploration of these practices both in the general population and in condition-specific subgroups.
Integrative medicine is an emerging person-centered approach to healthcare that aims to combine complementary therapies and conventional medicine with the goal of improving overall health of mind, body, and spirit. This model emphasizes holistic, evidence-informed care to prevent disease, manage symptoms, and promote overall well-being. Given the high rate of trust in physicians that has been reported by patients receiving conventional care, particularly in oncology, 24 an opportunity exists for providers to discuss the benefits and potential safety concerns of CAM use with their patients.41-43 For these conversations to be effective, it is not only important for physicians to be well-informed and receptive about speaking with patients about CAM modalities but also for patients to likewise feel comfortable communicating openly with their doctors about the therapies they are using. As CAM utilization continues to grow in the US, it is important to i) educate both patients and providers on the benefits and limitations of these therapies; ii) establish a scientifically proven evidence base to fully elucidate the potential advantages, as well as concerns, of each practice; iii) understand the intentions and expectations for use; iv) evaluate factors that influence adoption or hesitancy of utilization; and v) determine which specific modalities (individually or in combination) may be most appropriate for a patient's personalized needs. Addressing the aforementioned considerations will likely not only improve the patient experience but also advance our understanding of how best to integrate CAM practices into the CM model of care to optimize overall health outcomes.
Conclusions
In this study, approximately one-third of survey respondents participated in at least one CAM practice, mainly for the purpose of improving their health. To date, there remains limited national data regarding knowledge, perceptions, and the extent of adoption for CAM practices in the US. Future research is needed to more fully explore the motivations, facilitators, barriers, rates of utilization, and efficacy of individual modalities to discover which practices may be most beneficial for one's individual needs. Well-designed, large-scale studies using standardized operational definitions and data collection tools/instruments, with multivariate analyses, are necessary to enable rigorous comparisons across studies and to more accurately quantify the potential psychological and biological effects that may be influenced by these practices.
Footnotes
Ethical Considerations Statement
This study was exempt by the Stony Brook Committee on Research Involving Human Subjects Institutional Review Board, as the study utilized a publicly available, de-identified dataset.
Consent to Participate Statement
Not applicable.
Consent for Publication Statement
Not applicable.
Author Contributions
Barbara Nemesure – conceptualization, methodology, formal analysis, writing – original draft
Chitra Thakur - conceptualization, data interpretation, writing – review and editing
Linda Mermelstein - conceptualization, data interpretation, writing – review and editing
Sylvia K. Wood - conceptualization, data interpretation, writing – review and editing
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this research are publicly available.