
Abstract
Background
As calcitonin gene-related peptide (CGRP)-pathway-blocking therapies become more widely used, infrequent adverse events related to impaired compensatory peripheral vasodilation or to microvasculature regulation, such as Raynaud's phenomenon and alopecia, not observed in pivotal trials, have been described.
Case
We report a case of Raynaud's phenomenon exacerbation – with no serious consequences and that did not require treatment interruption – during fremanezumab treatment, in a patient suffering from chronic migraine and medication overuse headache living in a temperate climate zone in southern Brazil.
Conclusion
This case report shows that Raynaud's phenomenon does not seem to be an absolute contraindication to CGRP-pathway-blocking therapies but reinforces the need to assess prior peripheral vascular symptoms in individuals who are candidates for its use, even in temperate regions.
This is a visual representation of the abstract.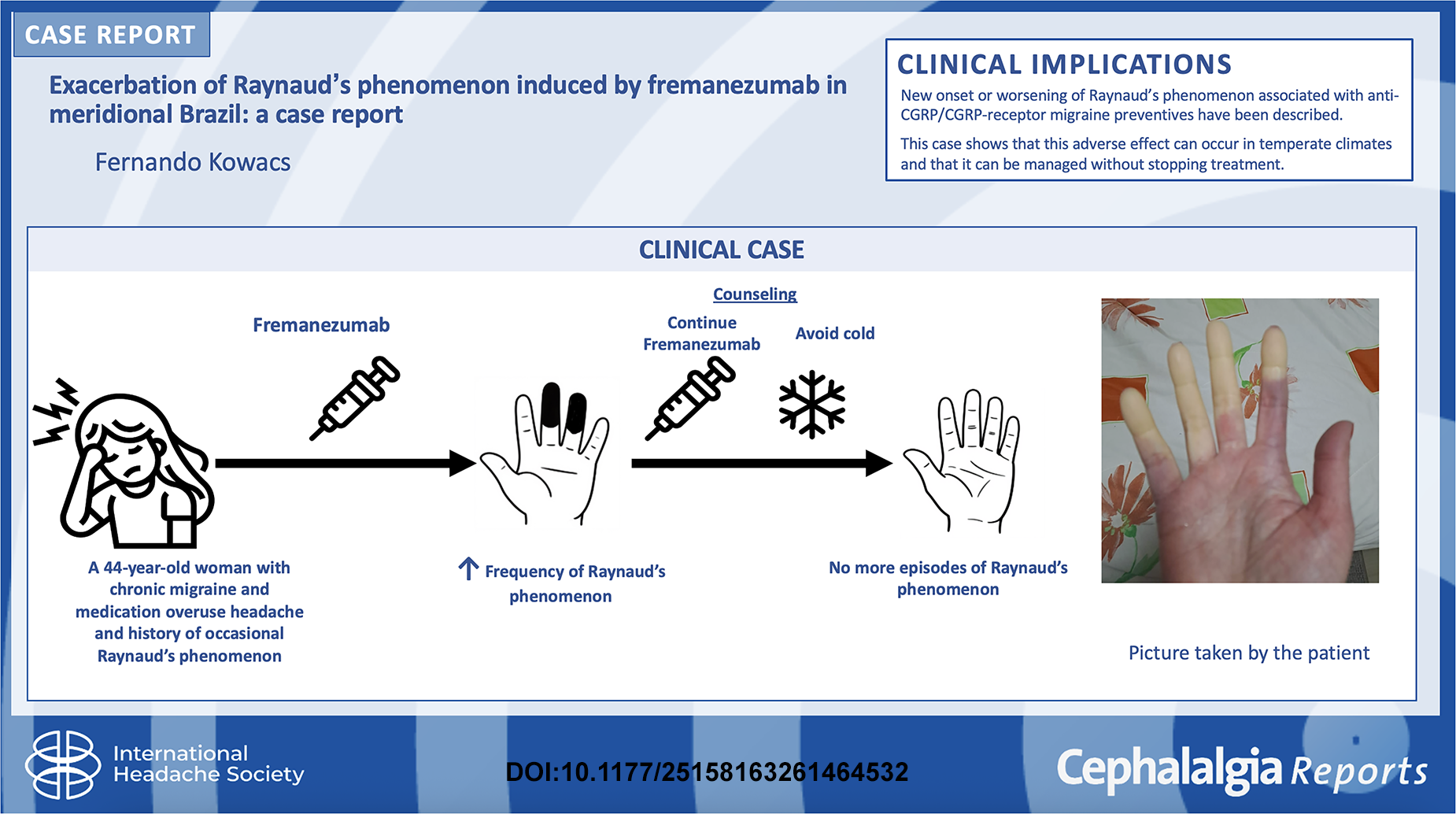
Introduction
Monoclonal antibodies that block calcitonin gene-related peptide or its receptor have expanded migraine preventive treatment options and, in spite of high cost and limited availability in many countries, are now recommended as a first-line choice both for episodic and chronic migraine. 1 Although the safety profile of these drugs was recently reaffirmed by results from both a systematic review 2 and a retrospective population-based cohort study, 3 their potential for impairment of physiological compensatory vasodilation in the context of tissue ischaemia is still a matter of concern. 4 Raynaud's phenomenon (RP) is considered a pathologic vasomotor response to cold stimuli, more prevalent in colder regions and also affecting women more frequently than men. 5 It is probably related to dysfunction of vascular adrenergic receptors, endothelial and/or regulatory neuronal/non-neuronal vascular pathways, and calcitonin gene-related peptide (CGRP) seems to play a protective role. 6 Recently, a few cases of new-onset or exacerbation of Raynaud's phenomenon associated with anti-CGRP or anti-CGRP receptor drugs have been described.7–9 In addition, a retrospective series from the Mayo Clinic showed that nine of 169 patients (5.3%) with migraine and RP developed microvascular complications during treatment with erenumab, galcanezumab or fremanezumab, varying from worsening of RP to distal digit gangrene, the latter occurring in only one patient. 4
The case of a Brazilian patient who presented an exacerbation of Raynaud's phenomenon while on treatment with fremanezumab is described, with the intention of emphasizing the need for an active search of previous vascular symptoms before starting a CGRP-pathway migraine therapy. This study is reported in accordance with the Case Report (CARE) guidelines for this case report.
Case presentation
A 44-year-old female complained of daily attacks of moderate to severe headache, with use of two naratriptan tablets per day, with incomplete response. She reported that for many years she had been experiencing headache attacks, which gradually became more frequent and intense and less responsive to simple analgesics. At least for 3 months before her consultation, the attack frequency exceeded 15 days per month. The headache was incapacitating if not treated, unilateral, pulsatile, worsened with movement and was accompanied by nausea (sometimes with vomiting) and intense photophobia, phonophobia and osmophobia.
The patient reported that more than one female cousin had incapacitating headache attacks with photophobia. She was using cyclobenzaprine every night, besides perindopril, rosuvastatin and levothyroxine for hypertension, dyslipidaemia and hypothyroidism secondary to radioiodine therapy for thyroid cancer, 7 years prior to the consultation. There were no significant abnormalities in the routine neurologic examination, and no papilloedema was detected. Diagnoses of chronic migraine and medication-overuse headache were established. Considering the high migraine-related impact at the time of the first consultation (Headache Impact Test-6 (HIT-6) score of 65), and previous treatment failures with a beta-blocker and anaesthetic nerve blocks, fremanezumab was prescribed (225 mg every 28 days, SC).
In the follow-up consultations, the patient recounted a remarkable effect starting in the second week after the first injection, with only mild and infrequent attacks reported. Her HIT-6 score fell to 56 after 3.5 months on treatment, and there were no tolerability issues at that moment.
The patient continued to use fremanezumab regularly and returned for a follow-up consultation after 8 months of treatment. On that occasion, she reported episodes of finger pallor followed by cyanosis and hyperaemia when washing her hands in cold tap water (Figures 1 and 2). At the initial consultation, she had not been asked about these symptoms and did not recall them spontaneously, but at that moment she described having experienced the same sequence of events in the past. Nonetheless, such episodes were milder and had occurred less than once a year, even under similar climatic conditions, and did not become more frequent until the first winter after she started fremanezumab. In that winter, temperatures fell to 37.6°F (3.1°C). Although it was not colder than three of the preceding five winters, 10 these transient episodes of finger pallor occurred many times, without sequelae. By then, naratriptan was no longer being used frequently and had not been taken on the specific days when the peripheral symptoms occurred. The patient was not taking any other drugs with vasoconstrictive effects.

Affected hand (picture taken by the patient).

Affected hand (picture taken by the patient).
The patient was referred to the vascular surgeon, who then ordered a Doppler study of the upper limbs that showed no abnormalities. Given the lack of clinical features suggestive of secondary RP caused by autoimmune disorder, laboratory tests or periungual capillaroscopy were not deemed necessary. General measures were recommended, and the patient opted to continue fremanezumab while taking precautions to avoid exposing her fingers to cold stimuli during the wintertime. Since then, although using fremanezumab regularly, the patient did not experience any further episodes of Raynaud's phenomenon. However, it is worth noting that she is still avoiding cold water when washing her hands and that, in cold environments, her hands become cold and pale more easily than they did before treatment. Written informed consent was obtained from the patient for publication. According to local regulations, ethics committee approval was not required for a single case report.
Discussion
A causal relationship between fremanezumab and the occurrence of Raynaud's phenomenon in this case can be assumed considering the marked increase in its frequency, from sporadic and mild to various more intense episodes (unfortunately, the patient did not provide a precise account of the number of episodes), with no change in the patient's exposure to low temperatures and cold water in comparison to previous winters. The fact that the episodes stopped occurring even with fremanezumab maintenance can be explained by the adoption of preventive measures after medical counselling.
The relevance of CGRP in the context of Raynaud's phenomenon pathophysiology has been emphasized by studies published during the 1990s that showed a diminished presence of CGRP-reactive neurons in the skin of the digits in patients with Raynaud's phenomenon in relation to healthy controls and that CGRP infusion was able to mitigate Raynaud's phenomenon in small controlled trials. 11 Abnormalities in the microvasculature of the digits have also been implicated in its pathophysiology, with some evidence pointing towards CGRP involvement12–14 and to a potential therapeutic effect of CGRP infusion.11,15 The receptor of adrenomedullin-1, another vasodilator peptide of the same calcitonin peptide family, also seems to be involved in Raynaud's phenomenon pathophysiology, at least when it is secondary to systemic sclerosis. 16 As CGRP can cross-activate the adenomedullin-1 receptor, 17 it could be expected that drugs that block the canonical CGRP receptor instead of the ligand itself, such as erenumabe and the gepants, would be less prone to cause or exacerbate Raynaud's phenomenon than the anti-CGRP monoclonal antibodies. Nonetheless, this was not observed in the Mayo Clinic retrospective study, in which erenumab was implied in RP exacerbation along with galcanezumab and fremanezumab. 4 A recent FAERS database analysis also suggested that this effect is common to all anti-CGRP pathway antagonists. 18
The occurrence of Raynaud's phenomenon associated with anti-CGRP/CGRP-R monoclonal antibodies and anti-CGRP-R small molecules has been described in the literature.7–9 Despite the fact that this patient did not develop any serious complication, as those described by Breen et al., 4 this new case of Raynaud's phenomenon exacerbation associated with a CGRP-pathway-blocking drug reinforces the need for active screening for peripheral vascular disorders, especially of this kind, in candidates for these drugs, even in temperate regions (this patient lives in the southernmost state of Brazil, at parallel 30°). Additionally, the fact that the patient was able to continue her effective migraine treatment after receiving appropriate counselling and adopting strategies to avoid cold exposure suggests that, particularly in regions with milder climates, Raynaud's phenomenon should not be regarded as an absolute contraindication to the use of CGRP-pathway-blocking drugs.
It also suggests that, consistent with real-world evidence, these adverse events may be under-recognized and may be noticed more frequently as the use of CGRP-pathway-blocking drugs is becoming a standard migraine treatment. 19 A parallel can be traced with alopecia, another microvascular regulation-related adverse effect not present in the pivotal trials. 20 In addition, comorbidity between migraine and Raynaud's phenomenon, suggested recently by a retrospective, cross-sectional, population-based study, reinforces this potential trend. 21 It is worth mentioning that this case occurred in a country where a much smaller number of patients are exposed to these drugs, as the only available CGRP-pathway-blocking drugs are fremanezumab and galcanezumab, both of which were launched in 2022 (erenumab was available from 2020 to 2022), which are not provided by the public health system or most private insurers. Even if symptom exacerbation appears to occur in only a small proportion of patients with Raynaud's phenomenon who receive these drugs, it can rarely progress to severe complications such as distal digit gangrene; this reinforces the need to include prior episodes of Raynaud's phenomenon in the routine anamnesis of patients with migraine, particularly those who are candidates for CGRP-pathway–blocking drugs.
Conclusion
As preventive treatment of migraine with drugs targeting the CGRP pathway becomes more widely used, adverse reactions not observed in pivotal trials may be encountered more frequently. We report a case of marked wintertime worsening of Raynaud's phenomenon in a patient receiving fremanezumab in southern Brazil.
In this case, no persistent adverse consequences were observed, and the benefits of treatment appeared to outweigh the risks. Nonetheless, this report underscores the need to actively elicit a history of peripheral vascular symptoms or signs in patients with migraine – such as prior cold-induced colour changes, numbness and/or digital ulcers – particularly when considering initiation of CGRP-pathway-blocking preventive treatment, even in a temperate region. This will help ensure that at-risk patients receive appropriate counselling on how to prevent and monitor for the occurrence of peripheral vascular dysfunction during treatment, with the aim of averting more severe complications.
Clinical implications
CGRP-pathway monoclonal antibodies may impair peripheral compensatory vasodilation.
This case adds to reports of Raynaud's phenomenon worsening after fremanezumab initiation.
Raynaud's phenomenon should not be regarded as an absolute contraindication to CGRP-pathway monoclonal antibodies, but prior vascular symptoms should be actively screened and monitored.
Footnotes
Acknowledgements
Use of Artificial Intelligence: ChatGPT (OpenAI, San Francisco, CA, USA) was used to improve readability without adding any AI-generated content. A permission release document signed by the patient, authorizing the publisher to include and publish the patient's photographs, is being submitted as a separate signed document. Although the document refers to another journal to which the manuscript had previously been submitted, the author confirms that the patient's authorization applies to publication in Cephalalgia Reports and assumes responsibility for its use in this submission.
Ethical considerations
According to local regulations, ethics committee approval was not required for a single case report.
Consent to participate
Written informed consent was obtained from the patient for publication.
Consent for publication
The author agrees to publish the case report with Cephalalgia Reports if accepted.
Author contributions
The author solely conceived and designed the study, collected and analysed the data, interpreted the results and wrote and approved the final manuscript.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The author declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: Fernando Kowacs has received speaker and/or advisor fees from Abbott, AbbVie/Allergan, AstraZeneca, Dr Reddy's, GSK, Janssen, Lilly, Lundbeck, MSD, Novartis, Neurodiem, Omifarma, Pfizer and Teva and invests in an equity mutual fund that may hold shares of Eli Lilly stock (indirect exposure only).
Data availability statement
Data sharing is not applicable to this article, as no datasets were generated or analysed during the current study.