
Abstract
Background
Therapeutic patient education (TPE) is a promising bio-behavioural adjunct to standard-of-care treatment to manage migraine. Evidence for its efficacy and optimal delivery, however, is limited.
Objective
To provide a comprehensive updated narrative review of the existing literature on the efficacy of TPE in managing migraine.
Methods
A preliminary PubMed search was conducted using a combination of MeSH and non-MeSH terms. Articles in English were screened through October 2025 based on titles and abstracts for relevance. Shortlisted studies were read in their entirety, and relevant findings were presented.
Results
The preliminary search yielded 257 studies, of which 37 were read in their entirety. Findings from 13 randomized controlled trials, eight non-randomized prospective studies and one retrospective study have been summarized in the present review. Despite methodological heterogeneity, results consistently demonstrate the efficacy of TPE for migraine management as an adjunct to standard of care. Various patient-reported outcomes, including quality of life, self-efficacy and pain catastrophizing, benefited particularly from TPE. TPE delivered through in-person group sessions may be superior to digital or written modes of delivery. Education provided by non-headache experts, including nurses, trained medical students and lay migraineurs, can also be effective when delivered by appropriately trained individuals. Preliminary analysis indicates reduced economic costs associated with TPE, though further studies are required.
Conclusion
TPE is a low-cost, accessible non-pharmacological intervention with evidence of efficacy in migraine management. This review provides a comprehensive summary of the literature, practical considerations and future research directions to optimize clinical utility.
This is a visual representation of the abstract.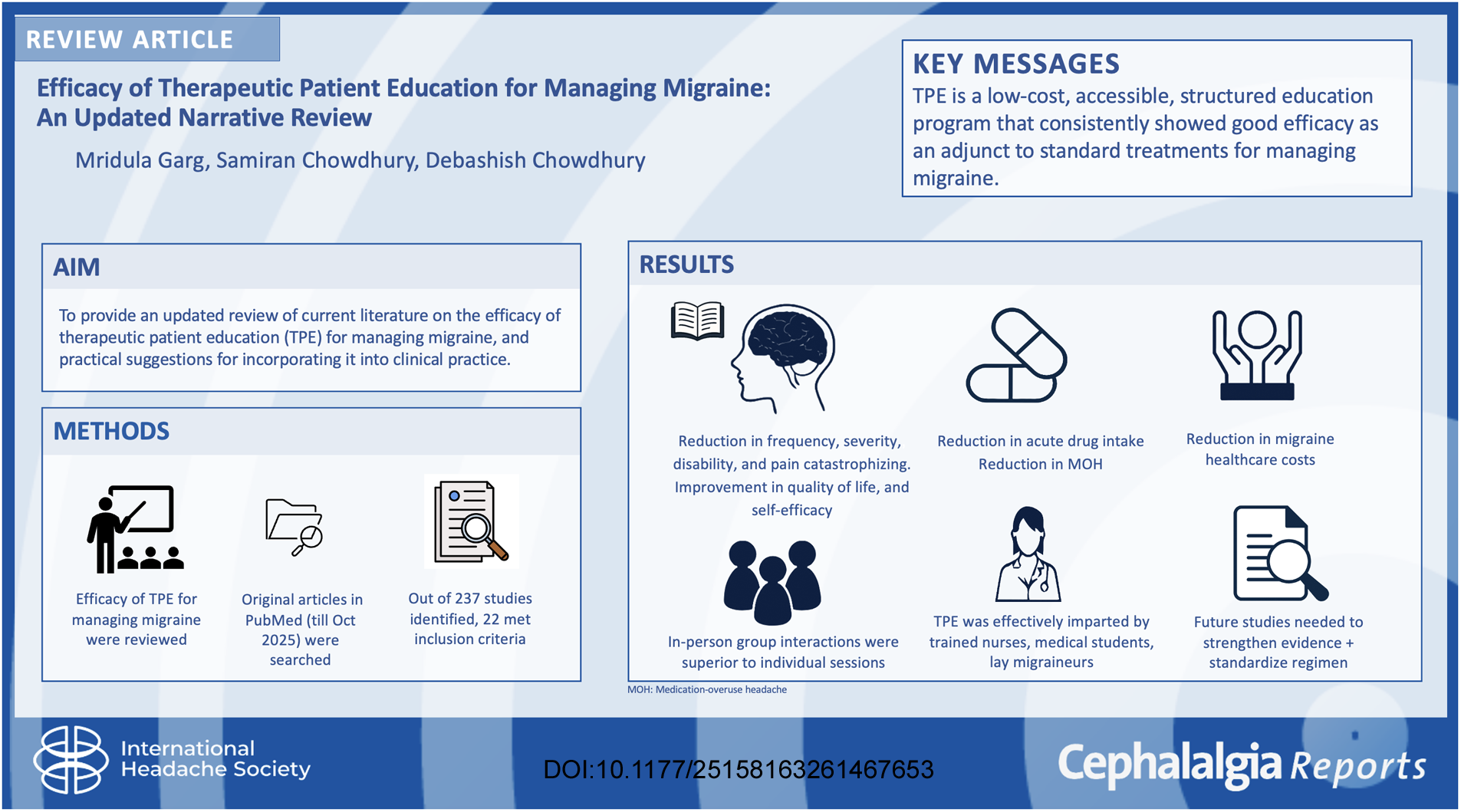
Introduction
Migraine is a highly prevalent1,2 primary headache disorder characterized by headache attacks lasting for 4–72 h that are of moderate to severe intensity, and frequently associated with nausea/vomiting and/or photophobia and phonophobia. 3 The prevalence of migraine peaks at 30–39 years of age, 4 with it contributing to an age-standardized rate of 541.9 years lived with disability per 100,000 population globally. 5 Thus, the disorder primarily affects the working population. Migraine is cited as the most common pain condition causing loss of productive time at work. 6 Roughly 8% of migraine sufferers are further diagnosed as having chronic migraine (CM), 7 defined as headache occurring for ≥15 days/month for 3 months, having features of migraine on ≥8 days/month. 3 CM is a highly disabling condition, 8 which is often complicated by medication overuse,8–10 increased risk of psychiatric comorbidities, 11 and severe headache-related disability. 7
Migraine often necessitates the use of both preventive and acute treatment modalities,8,12 despite which it can be difficult to treat, 13 especially by pharmacological modalities alone. 14 Thus, it is imperative to combine pharmacological as well as non-pharmacological interventions to treat migraine, 13 especially CM, optimally. Non-pharmacological interventions for migraine broadly include behavioural techniques, physical therapies, education and lifestyle modifications. 15 Multiple studies have shown the efficacy of various modalities in patient outcomes.15–24 In this review, we focus on therapeutic patient education (TPE) as an adjunct to pharmacological treatment for managing migraine. The World Health Organization defines TPE as ‘a structured person-centred learning process that supports individuals living with chronic conditions to self-manage their health by drawing on their resources, supported by their caregivers and families’. 25 The importance of TPE lies in the premise that patients make most decisions regarding their treatment independently, 15 including whether and when to undergo acute treatment, as well as behavioural changes such as weight reduction, regularizing sleep schedules and avoiding medication overuse.16,18,22 TPE thus shifts the locus of control to the patients, enabling them to make informed decisions about their health. 26
This review summarizes the latest evidence on the efficacy of TPE for managing migraine, elaborates on, and critically analyzes the various methods of delivering TPE studied to date, and provides practical suggestions for incorporating them into practice.
Methods
A preliminary search of the PubMed database was performed, incorporating the MeSH terms ‘Migraine’ and ‘Patient Education’. Additionally, terms such as ‘therapeutic patient education’, ‘behavioral intervention’, ‘behavioral treatment’, ‘chronic migraine’ and ‘quality of life’ were also searched. All types of studies, including randomized controlled trials (RCTs) and observational studies, were screened until October 2025. Some studies were also selected from citations in other articles, at the authors’ discretion, to ensure a comprehensive review. Only studies in the English language were included. The obtained studies were individually screened for relevance to the research question (the efficacy of TPE in migraine management) based on their titles and/or abstracts. Finally, the shortlisted studies were read in their entirety, and relevant findings are presented.
This study is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for this narrative review.
Although the review targets migraine headache specifically, studies that included primary headaches other than migraine were included if they provided separate data for migraine patients. Studies that additionally employed behavioural interventions beyond education (e.g., exercise, physical therapies, relaxation techniques) as part of their primary intervention were excluded from the review. Additional studies not specifically addressing the outcomes of TPE in migraine but instead focusing on its concepts, methods and mechanisms were also included to provide a comprehensive discussion.
Results
The initial MeSH search yielded 195 results, while the expanded search, including non-MeSH phrases, comprised 257 results. Initially, each study was screened for relevance to the research topic by examining the title and/or the abstract. Thirty-seven studies were thereby shortlisted and read in their entirety. Thirteen of these studies were RCTs – 11 used patient education as an active intervention while two employed education as a control intervention. Eight studies were recognized as non-randomized clinical trials, while one was a retrospective study. The PRISMA flow chart is shown in Figure 1.
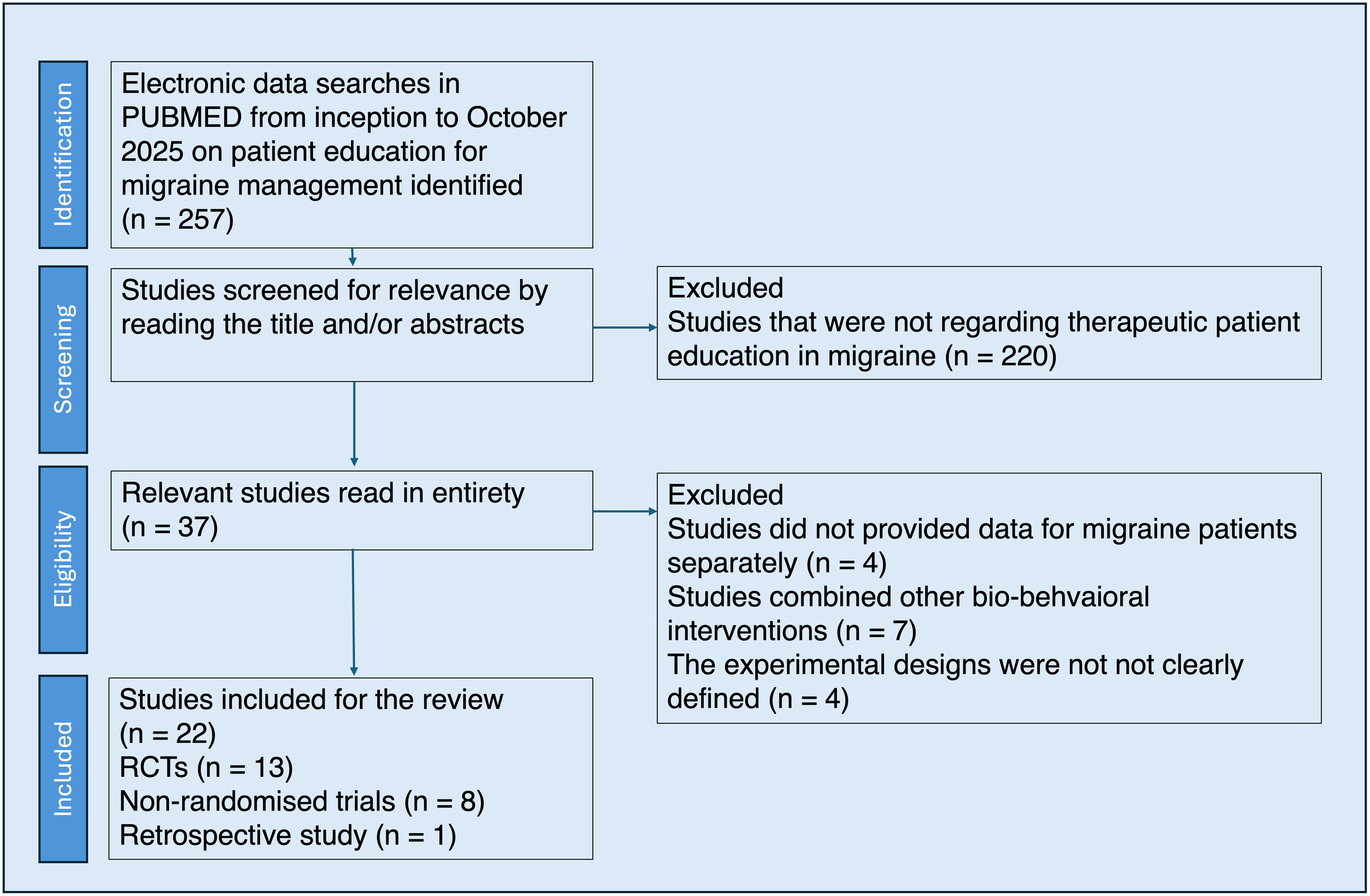
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart.
Randomized controlled trials
Salient features of the 13 RCTs have been summarized in Table 1. These studies are described briefly as follows: Bromberg et al. 4 conducted an RCT to assess the efficacy of a web-based educational intervention in patients with migraine. In total, 189 participants were given free access to a migraine education website named ‘painACTION’, which included informative articles on headache features and a headache diary, self-assessment tools and interactive pain tracker. They had to spend a minimum amount of time of eight 20-min sessions over 4-weeks on the website, with no limit on the maximum time. Significant treatment-by-time interactions were observed for depression (DASS subscale F = 4.86, p = 0.0028), stress (DASS subscale F = 4.07, p = 0.0079), self-efficacy (F = 10.99, p < 0.0001), positive coping strategies (like exercise and relaxation) (F = 7.18, p < 0.001) and all subscales of pain catastrophizing scale (PCS) (all p < 0.05). 27 Post hoc analysis also revealed lower depression, stress and PCS scores along with higher self-efficacy and positive coping strategies scores in the intervention group at 6-months follow-up.
Summary of randomized controlled trials.
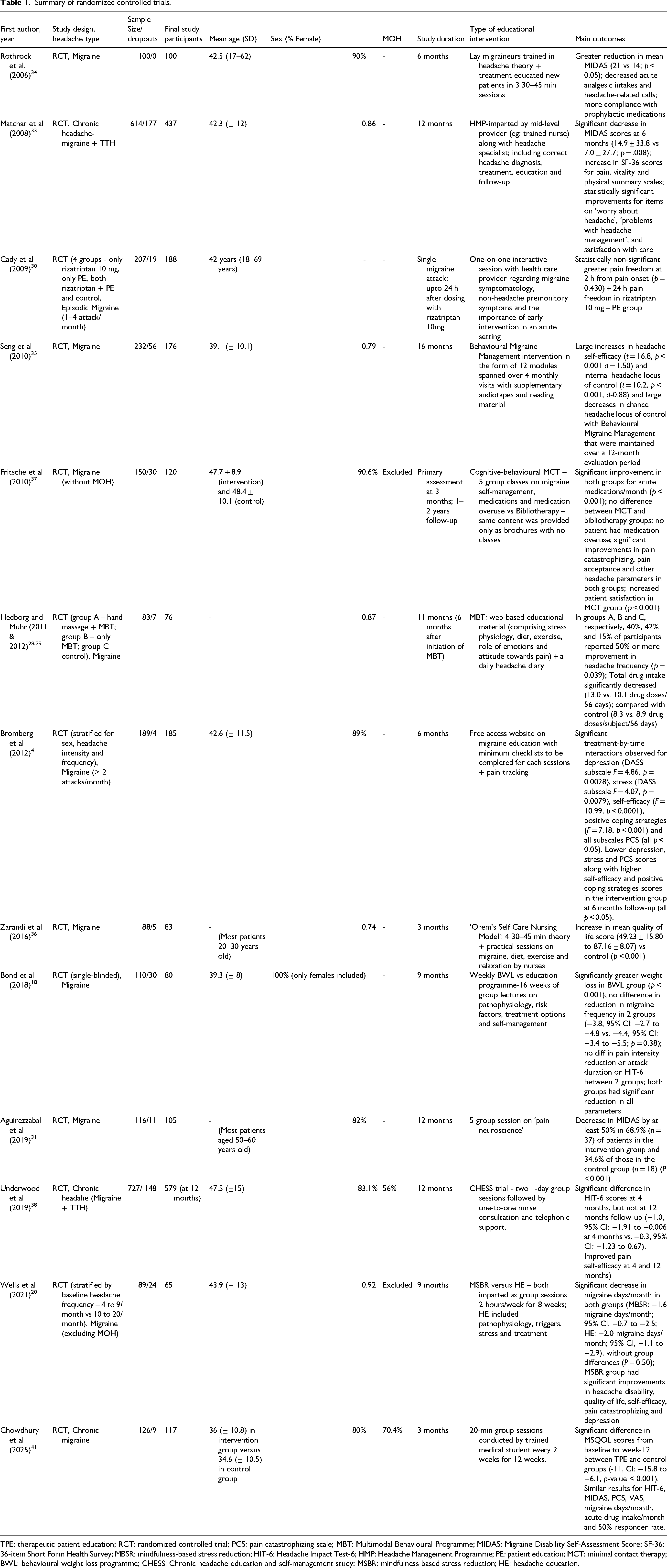
TPE: therapeutic patient education; RCT: randomized controlled trial; PCS: pain catastrophizing scale; MBT: Multimodal Behavioural Programme; MIDAS: Migraine Disability Self-Assessment Score; SF-36: 36-item Short Form Health Survey; MBSR: mindfulness-based stress reduction; HIT-6: Headache Impact Test-6; HMP: Headache Management Programme; PE: patient education; MCT: minimal contact therapy; BWL: behavioural weight loss programme; CHESS: Chronic headache education and self-management study; MSBR: mindfulness based stress reduction; HE: headache education.
Hedborg and Muhr28,29 employed a 6-month web-based Multimodal Behavioural Programme (MBT) to provide patients with education on stress physiology, physical activity, diet and thoughts; and to have them complete a daily headache diary. The intervention group (n = 55) was further divided into those who received an initial hand-massage intervention (n = 27) and those who did not (n = 28). A final analysis, performed 6 months after the introduction of MBT, showed that significantly more patients in the two intervention groups had at least a 50% reduction in headache frequency compared to the control group (p = 0.039). They also showed a greater reduction in the number of days of acute medication usage. Hand massage intervention, on the other hand, did not appear to affect patient outcomes.
Cady et al. 30 conducted an RCT on the efficacy of rizatriptan (10 mg) for treating early or mild headaches. A secondary objective of the study was to assess the role of patient education in treatment compliance. Out of the 207 participants studied, 46 comprized the group that received both early treatment and education, where the HCP assessed patient's awareness of their migraine symptoms and helped them identify possible premonitory symptoms from a pre-defined list. Greater percentage of patients with patient education reported pain freedom at 2 h (p = 0.430) and 24 h from pain onset, although the difference was non-significant. The finding was attributed to greater adherence to early intervention and higher patient satisfaction.
Aguirrezabal et al. 31 aimed to assess the impact of patient education at the primary healthcare level to decrease the burden on headache specialists and reach a wider subset of migraine patients who are unable to access specialist care. In total, 116 patients were enrolled, and those in the intervention arm were educated about pain neuroscience, including how the pain neuromatrix is activated by perceived threats to the body, how fear of pain positively correlates with headache severity, and how modifying beliefs and behaviours about the pain can alter headache outcomes. Four sessions were delivered weekly, with a fifth session given 1 month after the fourth session. The intervention group showed a significantly higher percentage of people with a 50% reduction in Migraine Disability Self-Assessment Score (MIDAS) (68.9% in intervention group vs. 34.6% in control groups, p < 0.001). 32
Matchar et al. 33 initiated a single-session ‘headache management program’ in three substantially different healthcare settings to provide 614 chronic headache patients (including both migraine and tension-type headache (TTH)) with accurate diagnosis, optimal pharmacological intervention, education and regular follow-up. At the 6-month follow-up, 437 patients completed the survey and the treatment groups showed significant improvement in MIDAS scores (14.9 ± 33.8 vs. 7.0 ± 27.7, p = 0.008), with increases in 36-item Short Form Health Survey (SF-36) scores for pain, vitality and the physical summary (all p < 0.05). In total, 387 participants also completed a repeat MIDAS survey at 12 months (6 months after the clinical intervention). The results showed a sustained response to intervention (6.8 points, 95% CI −0.3 to 13.92, p = 0.062) and an overall increase in patient satisfaction with their treatment.
Rothrock et al. 34 employed lay migraineurs to educate 50 new migraine patients (in the intervention arm) by rigorously training them in headache theory and treatment. Patients attended three educational sessions and were followed for 6 months. Analysis showed greater reductions in mean MIDAS scores (21 vs. 14, p < 0.05)), acute analgesic use (0% vs. 36%) and headache-related calls to physicians (mean 1.1 vs. 4.9 calls), as well as increased compliance with prophylactic treatment (96% vs. 58.5%) in intervention group compared with control. Authors described the methodology as an alternative healthcare-delivery system, given that a clinical setting, such as an overcrowded one-on-one outpatient setup, might not be ideal for educating patients.
Seng and Holroyd 35 studied the impact of behavioural migraine management on headache self-efficacy and locus of control, reporting large increases in both parameters that were maintained over 12 months post-intervention. They provided education through 12 modules spanning four monthly visits, along with audio tapes and booklets for reference at home. Outcome was assessed by mixed models for repeated measures analyses (n = 176). Large increases in headache self-efficacy (t = 16.8, p < 0.001 d = 1.50) and internal headache locus of control (t = 10.2, p < 0.001, d = 0.88) were observed when behavioural migraine management was used as an adjunct to propranolol, and these effects were maintained over a 12-month follow-up period.
Zarandi et al. 36 employed a ‘supportive educative’ nursing model to deliver 35–40-min educational group sessions to migraine patients, covering topics such as migraine, diet, exercise and relaxation. They found that after 3 months of follow-up, patients in the intervention arm showed a significant improvement in quality-of-life scores (from 49.23 ± 15.80 to 87.16 ± 8.07) versus control (p < 0.001). In total, 84% of patients were able to employ dietary modifications (regular meals, avoidance of trigger foods) to manage their headache attacks.
Three RCTs approached TPE in different ways, with two using it as a control intervention.18,20 The third one compared the efficacy of two different forms of TPE (i.e., group sessions vs. information brochures). 37 Wells et al. aimed to assess whether mindfulness-based stress reduction (MBSR) improved migraine outcomes more than patient education. Both interventions lasted 2 h/week for 8 weeks, with headache education including instruction on pathophysiology, triggers, stress and treatment approaches. The study found that both interventions were equally effective in reducing migraine days per month (−1.6 vs. −2.0, p = 0.5) and headache frequency (−2 vs. −2.4, p = 0.52). There was a greater improvement in quality of life, disability, pain catastrophizing and depression scores in the meditation group. The authors noted that, contrary to their expectation, headache education also reduced headache frequency (as did mindfulness); thus, education was an active intervention and could be considered more of a comparator than a control.
Bond et al. studied the efficacy of behavioural weight loss intervention (≥ 7% weight loss goal) vs. migraine education (16 weeks of group lectures on migraine pathophysiology, treatment strategies and self-management) in obese female migraine patients. 18 While they reported significantly greater weight loss in the weight-loss arm, there was no difference in improvement in migraine-related outcomes, including reductions in mean migraine days (−3.8 vs. −4.4, p = 0.38), pain intensity (−1.5 vs. −0.7 p = 0.15), attack duration (−2.7 vs. −2.2, p = 0.89), or Headache Impact Test-6 (HIT-6) scores (−5.7 vs. −5.6, p = 0.94). These studies demonstrate the efficacy of TPE compared with other non-pharmacological interventions.
Fritsche et al. conducted a study comparing a ‘cognitive-behavioral minimal contact program (MCT)’ comprising five interactive sessions on headache management and medication use with providing bibliotherapy (brochures containing the same educational material as the MCT but without face-to-face interaction with educators) alone. 37 Results showed improvement in both groups (p < 0.001), with no statistically significant differences, on measures including the number of acute medications per month (5.9 ± 3.2 vs. 6.5 ± 3.2), medication overuse (no patients in either group), pain catastrophizing and pain acceptance. No participant in either group developed medication overuse over the 2-year study period. Interestingly, patients reported greater satisfaction with MCT than with bibliotherapy, even though the efficacy was the same, highlighting the value of a more interactive approach to educational interventions.
Underwood et al. 38 studied non-pharmacological educational and self-management interventions for people with chronic headache: the CHESS research programme, including an RCT in the UK between 2017 and 2019. The CHESS intervention consisted of two 1-day group sessions focused on education and self-management to promote behaviour change and support the use of learning strategies to manage chronic headaches. This was followed by a one-to-one nurse consultation and telephone support. The control intervention consisted of feedback from classification interviews, a headache management leaflet and a relaxation compact disc. They randomized 736 participants from 164 general practices. Nine participants (1%) had chronic TTH only. The main analyses were on the remaining 727 participants with migraine (376 in the intervention arm and 351 in the usual-care arm). The primary outcome was headache-related quality of life measured using the HIT-6 at 12 months. There was no between-group difference in the HIT-6 at 12 months (adjusted mean difference −0.3, 95% confidence interval −1.23 to 0.67; p = 0.56). However, at 4 months, there was a difference favouring the CHESS self-management programme on the HIT-6 (adjusted mean difference −1.0, 95% confidence interval −1.91 to −0.006; p = 0.049). Additionally, pain self-efficacy improved at 4 and 12 months. Subsequent exploratory papers identified three important factors for the negative results.39,40 First, attendance (‘dose received’) fell short of expectations, although 261/380 (69%) received at least the pre-identified minimum dose. Second, the authors suggested that the intervention's effect did not sustain over time in patients with chronic headaches. Third, the magnitude and durability of improvement in self-efficacy might be a key factor in achieving a better long-term quality of life for these patients.
Chowdhury et al. 41 provided TPE through group sessions led by a trained medical student. The sessions lasted 20 min, comprising information on migraine pathophysiology, trigger avoidance, medication and lifestyle modifications. The study reported significant improvements in their primary endpoint, change in Migraine-Specific Quality of Life score from baseline at 12 weeks (−11, CI −15.8 to −6.1, p < 0.001). Similar results were observed for other endpoints, including MIDAS, HIT-6, pain catastrophization scores, migraine, acute treatment frequency and 50% responder rates. The findings highlight the potential utility of non-expert-trained personnel for providing TPE, especially in low-income countries.
Non-randomized interventional studies
Salient features of the eight non-randomized trials have been summarized in Table 2. These studies are described briefly as follows:
Summary of non-randomized trials.
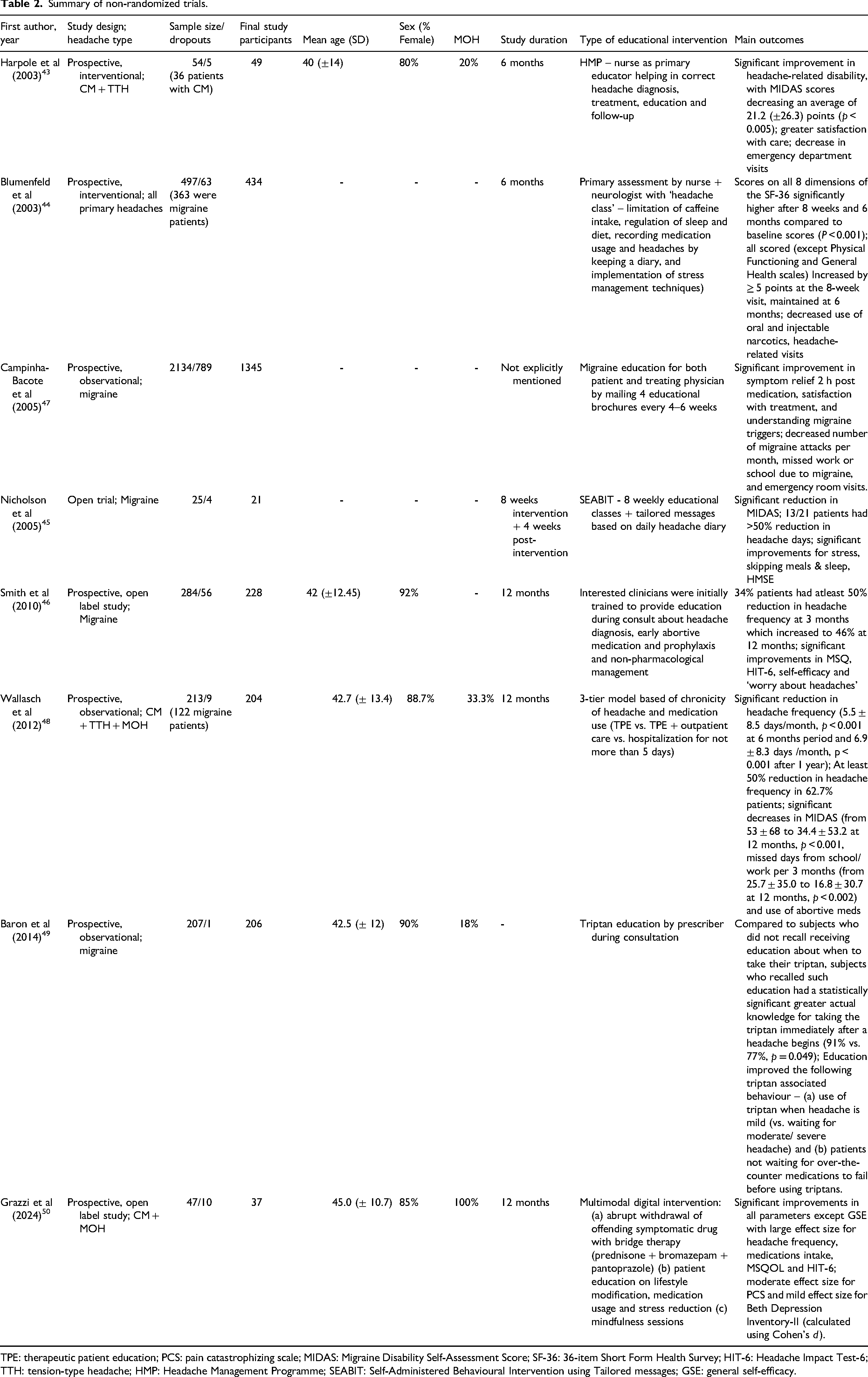
TPE: therapeutic patient education; PCS: pain catastrophizing scale; MIDAS: Migraine Disability Self-Assessment Score; SF-36: 36-item Short Form Health Survey; HIT-6: Headache Impact Test-6; TTH: tension-type headache; HMP: Headache Management Programme; SEABIT: Self-Administered Behavioural Intervention using Tailored messages; GSE: general self-efficacy.
Harpole et al. 42 conducted a study with 54 patients with CM and/or TTH by implementing a ‘Headache Management Programme’. In total, 36 patients had CM. Trained nurses served as the primary educators, assisting with the accurate diagnosis, treatment and education of patients through interactive group sessions followed for up to 6 months. Investigators found a significantly greater reduction in MIDAS scores (−21.2 ± 26.3, p < 0.005), increased satisfaction, and fewer emergency visits for headaches.
Blumenfeld and Tischio 43 also employed nurse educators in conjunction with neurologists to provide 497 primary headache patients (363 with migraine) with a ‘headache class’ covering topics such as regularizing sleep and diet habits, limiting caffeine intake, medication use, and keeping a headache diary. At the end of 8 weeks, results from the Migraine-Specific Quality of Life questionnaire (p < 0.001 for all three dimensions) and the SF-36 forms (p < 0.001 across all eight dimensions) showed significant improvements, and this trend was maintained at the 6-month reassessment. Usage of oral and injected narcotics also decreased after the intervention (p < 0.01). In total, 86% of the physicians who referred their patients to the programme were satisfied with the care.
Nicholson et al. 44 conducted an interesting study harnessing algorithms to send tailored messages to study participants based on their responses to an online daily headache diary. Additionally, eight weekly educational classes were also provided. The analysis of the 4-week post-intervention phase showed a significant reduction in the mean MIDAS score, and 13 of 21 patients had a greater than 50% reduction in headache days. The authors emphasized the importance of increasing self-efficacy as a key goal of effective behavioural interventions, and their study demonstrates a significant increase in self-efficacy from baseline to the post-intervention period.
Smith et al. created an educational programme for both physicians and patients, wherein interested physicians were educated on headache diagnosis, the benefits of early intervention, prophylactic drugs and non-pharmacological management. 45 Physicians then taught the same approach to 284 migraine patients, 46% of whom achieved at least a 50% reduction in headache days, along with improvements in self-efficacy, HIT-6 and MSQOL (all p < 0.001). Anticipation of an impending headache (and associated anxiety) can interfere with the efficacy of analgesics. Another study by Campinha-Bacote et al. 46 employed physician and patient education, reporting decreases in migraine high attack frequency (Migraine Treatment Assessment Questionnaire (MTAQ) subscale score from 35.6% to 31.2%, p = 0.02) and economic burden (MTAQ subscale score 60.6% to 47.7%, p = 0.006), as well as increased satisfaction with treatment (p < 0.0001).
Wallasch and Kropp 47 divided 213 headache patients into a 3-tiered headache care programme based on their headache frequency, analgesic use and psychiatric comorbidities. The least disabled patients only got education on self-management, while those with moderate severity also had regular outpatient care. Patients with severe headaches and/or psychiatric comorbidities were given hospital care. The intervention resulted in a significant reduction in headache frequency (5.5 ± 8.5 days/month, p < 0.001 at 6 months)), MIDAS scores (from 53 ± 68 to 34.4 ± 53.2 at 12 months, p < 0.001) and the number of school or workdays lost per 3 months (from 25.7 ± 35.0 to 16.8 ± 30.7 at 12 months, p < 0.002).
Baron et al. 48 provided triptan education to 207 patients, resulting in patients modifying their behaviour to practice early triptan use in acute settings (91% vs. 77%, p = 0.49) and to avoid waiting for over-the-counter medications to fail before using triptans (74% vs. 42%, p = 0.001). This study showed a direct relation between education and real-time behavioural modification.
Grazzi et al. 49 published a recent single-arm pilot study assessing a multimodal web-based intervention for patients with CM and medication-overuse headache (MOH). The intervention consisted of the immediate withdrawal of overused medicines, patient education on lifestyle modifications and mindfulness sessions. They report significant improvements in headache frequency (from 18.8 ± .1 to 6.9 ± 4,1, p < 0.001) and quality of life (from 50.2 ± 22.3 to 68.5 ± 18.6, p < 0.001)), among other parameters, over 12 months of follow-up; however, a high dropout rate (6 out of 47) occurred due to difficulty adhering to the intervention.
Ormond et al. 50 reviewed charts of 104 adolescent migraine patients who participated in a group education programme and found a significant reduction of 11.5 ± 11.9 headache days/month at 6 months follow-up (p < 0.001). The education comprised types of headaches, including dangerous headaches, trigger avoidance and pharmacological and lifestyle interventions.
Discussion
TPE must be distinguished from routine instructions given by the physician to migraine patients after each consultation regarding drugs, dosage and brief counselling about dos and don’ts. It is an organized, structured education programme that helps migraine patients self-manage their health by understanding the disease process, thereby motivating them to make the required changes. It should be viewed as an ongoing, continuous activity to be used as an adjunct to other therapeutic measures for a disease like migraine, which covers a large part of the lifespan of patients.
Efficacy of TPE
Our review showed that, despite methodological heterogeneity, including the content taught in the sessions, the teaching method, the instructor and the duration, results consistently showed a positive outcome with TPE compared to standard treatment for migraine management. Patient-reported outcome measures (PROMs), such as HIT-6, MIDAS and quality of life, showed more consistent favourable results than headache characteristics, such as attack frequency and severity. Other important outcome measures, such as self-efficacy, locus of control and pain catastrophizing, also showed significant improvements, suggesting their possible impact on PROM. Educating patients about optimal medication usage and overuse avoidance, along with strategies for self-management and lifestyle modifications, delivered by trained healthcare providers in interactive group sessions, shows most consistent evidence for efficacy for migraine outcomes.19,21,30,31,34–36,38,42 The mechanisms of action of TPE are summarized in Figure 2.
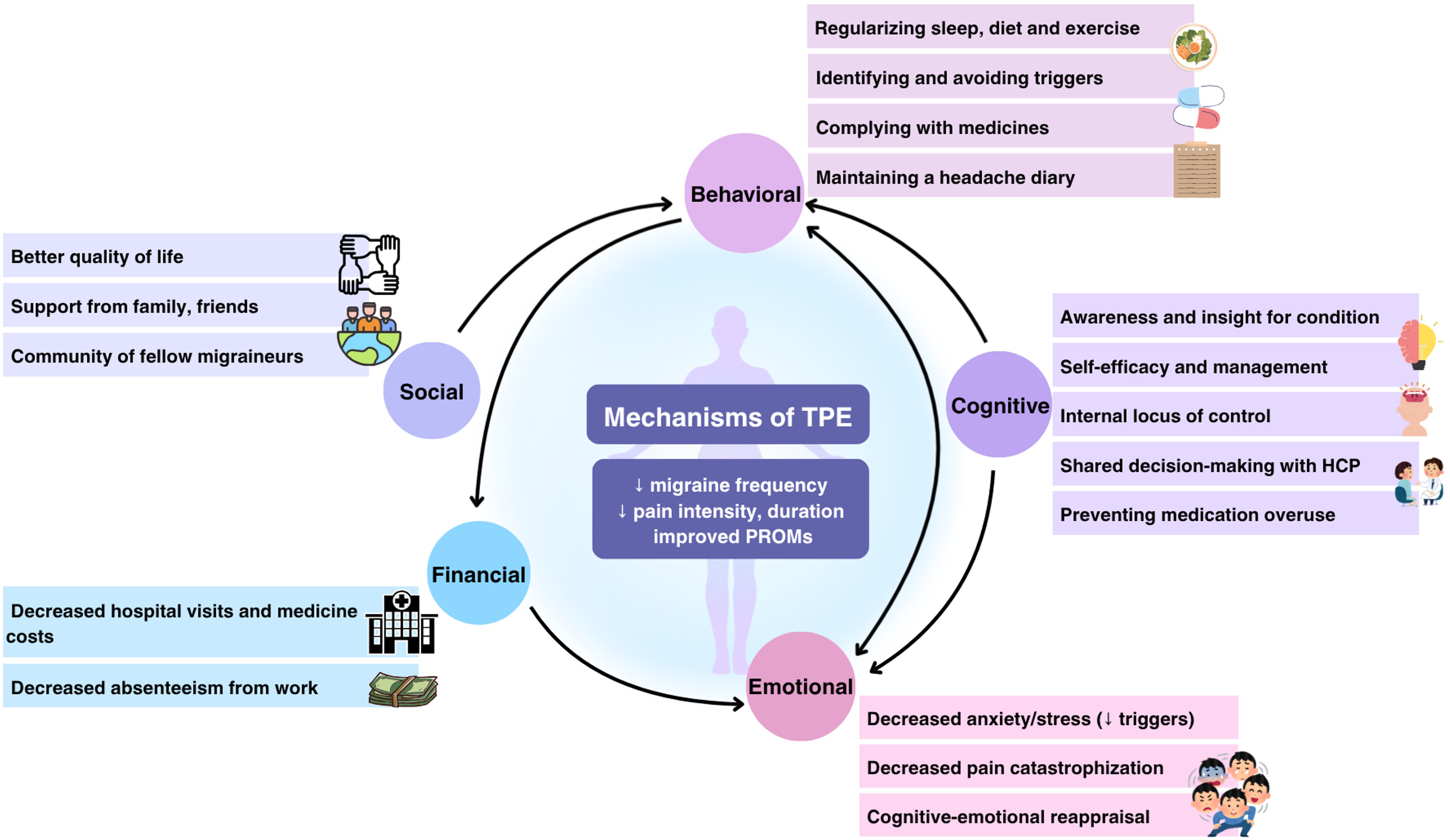
The mechanisms of action of therapeutic patient education (TPE).
Content of TPE
Based on our review an ideal TPE programme for migraine should preferably include following contents (a) define migraine and help patients identify migraine attacks as opposed to other headache types (b) explain in simple language the pathophysiology of migraine as a combination of genetic plus environmental factors with decreased pain thresholds (c) inform patients about non-headache symptoms that often precede headache (d) help patients understand and identify migraine triggers (e) drive home the role of both acute and prophylactic medications and responsible medication usage (avoiding medication overuse) (f) suggest lifestyle modifications including regularizing sleep and feeding habits, improving diet, weight loss (for obese patients), exercising, reducing stress and trigger avoidance (g) teach patients how to maintain a headache diary to keep track of their illness.
Most studies included at least some of these components in their educational curricula.4,18,20,28,33–35,45 Interestingly, many trials studied only one of these components and still reported significant results, suggesting that even minor changes in patients’ behaviour can impact therapeutic outcomes. Most studies focused on education regarding the appropriate use of medications.30,37,48 One study 31 specifically taught patients about pain science and how fear of pain worsens headache severity. They reported a 50% or greater reduction in MIDAS scores in 70% of their patients.
Method of imparting TPE
There are numerous ways of imparting patient education that have been studied in the literature. The most studied mechanisms were face-to-face group classes31,37,41,43,50 or one-on-one education during consultations.30,33,42,45 Some studies have reported good efficacy of web-based interventions,4,29 which offer the advantage of being perpetually accessible to patients, thereby facilitating better reinforcement through increased exposure to educational material at the patients’ convenience. It also helps reach patients who are unable to move around due to migraine disability. 4 Other methods that have been studied include audiotapes35,51 and messaging software. 44 While most educational programmes supplemented patient information with brochures, some studies used them as the primary mode of intervention.37,46 Both the group session and the information brochure method were found to be equally efficacious 37 in a non-randomized study. Cady et al. 51 found superior outcomes when nurses were actively involved in education. A recent pilot study by Young et al. 52 reported the efficacy of a mobile-app-based educational intervention, which resulted in fewer healthcare visits, reduced headache frequency and lowered MIDAS scores. They also reported a lower responder rate at 12-month follow-up, suggesting that human interaction (including telecommunication) may have a greater impact on positive action than virtual interventions.
Group versus individual
A meta-analysis found that group interventions may be superior to individual sessions, as they improve confidence in self-management and facilitate social interaction. 14 Group therapy not only provides education but also allows for building a supportive community of migraine patients. One of the most concerning facets of migraine is the associated anxiety and ‘feeling of doom’ 53 that makes patients feel hopeless and less likely to adhere to their prescribed treatment. Interacting with fellow sufferers alleviates the perception of being alone. It also opens the possibility of ‘vicarious experiencing’-wherein patients can learn to duplicate behavioural change by listening to or following the experiences of other patients. 54 Evidence also supports the efficacy of group sessions in improving quality of life, 55 an important PROM in migraine management.
Who provides TPE
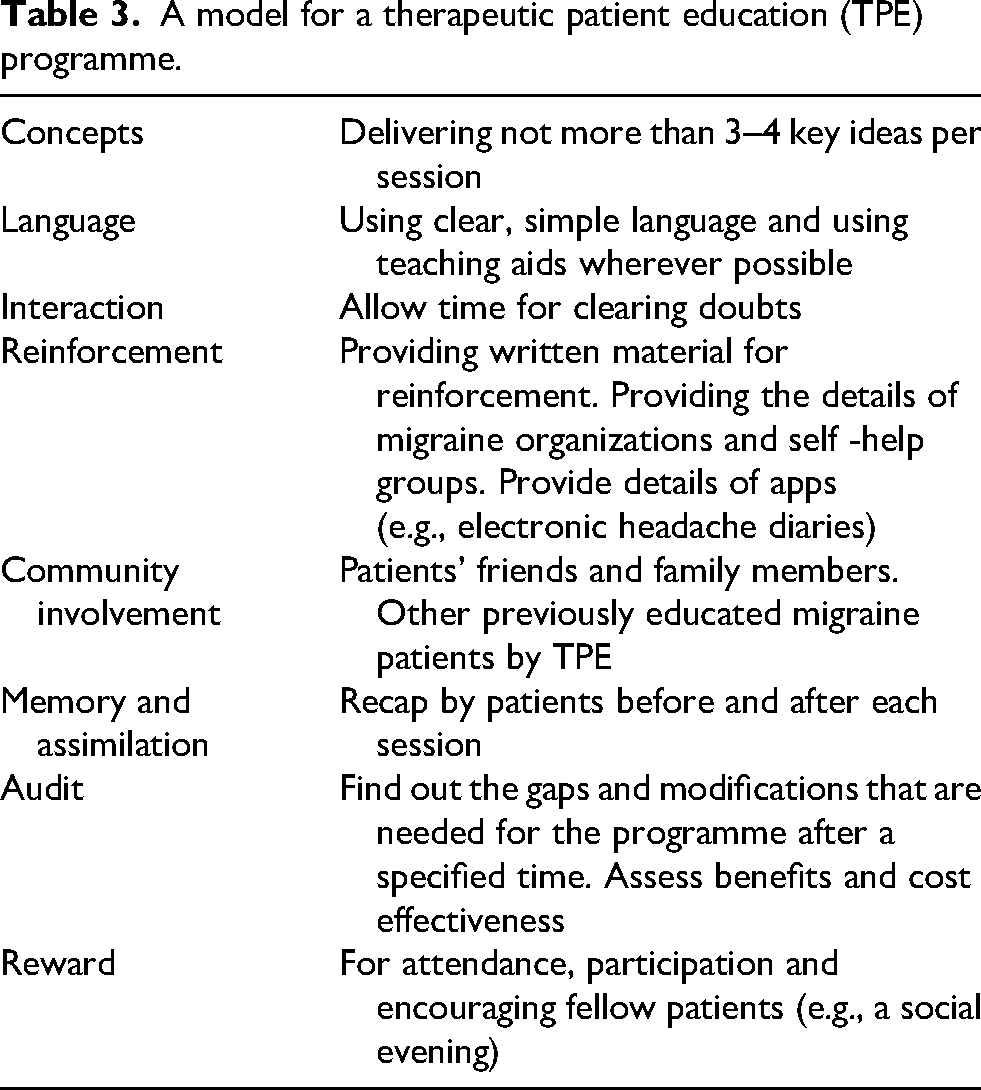
Among studies that used face-to-face educational interventions, there is considerable diversity in educators’ qualifications. Healthcare professionals, primarily doctors, provide TPE. 25 These may include headache specialists,20,30,48 trained junior doctors, or primary-care workers. Many studies have also shown evidence for nurse-based educational interventions, wherein 51 the burden of education is passed onto nurses since an outpatient setup might not be ideal for adequately informing patients.33,51 Importantly, in their meta-analysis, Probyn et al. 14 found no difference in outcomes between education provided by trained psychologists and other professionals. In fact, in a high-quality RCT, Rothrock et al. 34 demonstrated the efficacy of education provided by lay migraineurs trained in headache management. Such an intervention can have multiple benefits, not only alleviating the burden on healthcare providers but also helping to build strong communities of migraine sufferers and establish better support systems. Some preliminary data are also available on education imparted by pharmacists, but further formalized studies are required. 56 A plan for an ideal TPE programme is summarized in Table 3.
A model for a therapeutic patient education (TPE) programme.
Complementary role of TPE
The efficacy of TPE in most studies may be due to better medication compliance rather than the education itself. Indeed, TPE has been shown to improve patients’ adherence to their prescriptions, including timely (early) acute medication use, avoidance of medication overuse and increased compliance with preventive medications.30,34,54 However, recent studies have shown that educating patients about their disease and behavioural management techniques early in the course of their disease can significantly improve patient outcomes and reduce the overall burden of disease on both patients and the healthcare system. A recent study by Pack et al. 57 finds evidence for delayed or no communication about MOH with patients, with some patients reporting that they first heard about MOH as much as 5 years after their migraine diagnosis. Healthcare providers surveyed in the same study emphasize the importance of standardized educational materials to help them inform their patients about MOH early on. It is important to recognize that parameters such as acceptability, feasibility and ease of compliance are all crucial factors to consider when evaluating any intervention. In this regard, migraine pharmacological options have historically been suboptimal and the fact that TPE can improve these shortcomings is a testament to its utility as an adjunct. There is a growing body of evidence on the role of lifestyle modifications, such as adequate sleep, a healthy diet, weight loss and trigger avoidance, in reducing headache frequency and morbidity.18,19,22 Focusing solely on pharmacological intervention largely ignores these factors, resulting in subpar outcomes. TPE has demonstrated superior outcomes, even in RCTs that included both medically treated and non-treated migraine patients. 4
The role of TPE in increasing patients’ confidence in their ability to manage their disease (self-management) and in feeling in control of their health (self-efficacy) is well documented. Self-efficacy is directly correlated with the use of self-management behaviours. Likewise, patients who have an internal locus of control (headaches are caused by internal factors, such as stress or poor lifestyle) tend to mobilize more towards appropriate behavioural change. In contrast, those with an external locus of control (headaches occur due to fate or can only be cured by doctors/drugs) tend to make poor judgments and also have increased worry regarding their disease, which in turn adds to their likelihood of having a headache. 58 Seng et al. 35 found noteworthy correlations between self-efficacy and locus of control, in which patients with high chance locus of control scores before TPE showed larger increases in self-efficacy post-intervention. This can be attributed to the fact that patients who originally believed that they had no control over their disease benefited much more from the knowledge and behavioural skills taught to them than others.
Another related effect of TPE is the shift in patients’ perspective from being a victim of their condition to feeling empowered and in control of their health. 59 Victimization is closely linked to an external locus of control, wherein patients feel their illness is ‘happening to them’ and there is nothing they can do about it. This belief of hopelessness is often solidified in clinical practice as patients are prescribed daily preventive medications for an indefinite amount of time, making them believe that ‘something is wrong with them’. Intervening at this stage with sensitively imparted knowledge about the true nature of their diagnosis, the rationale behind their prescription and their ability to influence their treatment through lifestyle modifications can drastically shift patients’ focus from self-pity to self-management.
Cost-effectiveness of TPE
Chronic diseases such as migraine have a high economic toll, not just on the patient but also on society at large. Migraine is among the leading contributors to patients’ healthcare costs. This includes both direct costs, such as hospital and medicine bills, as well as indirect economic losses, including absenteeism from work or school and/or reduced productivity at work. An estimated $13 billion is lost in the United States annually owing to migraine. 60 Families of migraine patients have 70% more healthcare costs compared with non-migraineur families. 61
According to the economic analysis presented by Aguirrezabal et al., 31 patients in the TPE arm of the study spent €12.33 on migraine treatment, compared with €45.53 (€53.91 including preventive medication) spent by patients in the control group. They estimated that €92 could be saved for each additional patient whose MIDAS score was reduced by 50%. Other studies have also demonstrated that TPE is a low-cost intervention with a significant impact on headache disability and consequent work absenteeism.4,31,47,62
Timing of TPE and predictors of good outcome
Ideally, TPE should be initiated at the time of the first visit when migraine diagnosis is confirmed. However, the patient's acceptability and the logistics of its delivery can be challenging. It can be helpful to visualize migraine patients along a continuum of motivation over the course of their disease, as described by Prochaska and DiClemente. 63 Some patients may be in the pre-contemplation stage, where they do not even think about changing their behaviour; therefore, simply prescribing daily prophylactics without addressing the underlying beliefs might not be effective. As patients slowly move towards the other end of the spectrum, they initially acknowledge the importance of change and eventually take appropriate actions until it becomes a habit. This progression is often not linear, and it is here that TPE can prove highly efficacious by catalysing movement towards active change and long-term habit formation. Secondly, the health literacy of migraine patients also matters. Studies have shown that patients with inadequate health literacy have a strong association with a low socioeconomic position, poor health status, inactivity and overweight. 64 Appropriate early institution of TPE can thus become even more significant in this population.
Artificial intelligence for TPE
As we enter an era of unprecedented enthusiasm for artificial intelligence (AI), it is logical to anticipate its expansion into patient education and healthcare. More and more people are seeking (at the very least) preliminary medical advice from AI chatbots. An interesting study by Li et al. 65 found 83–97% accuracy in responses from five different AI Large Language Model Chatbots to common migraine-related queries, including its definition, management and prognosis. While promising, it is pertinent to note that when asked about the surgical options for treating migraine, the Chatbot responses were deemed ‘poor’, with ChatGPT 3.5 proposing hemicraniotomy as an option for severe migraine. The healthcare community would be remiss to underestimate the inevitable impact and implications of publicly accessible AI tools on patients’ overall health-seeking behaviour. Rather, we must be quick to adapt to the changing landscape and get involved (as medical experts) in determining the scope of such tools vis-à-vis clinical management. Such studies are necessary to prevent any undue harm to patients resulting from unsound medical advice.
Limitations
We acknowledge the limitations of this review in recommending TPE, given the heterogeneous nature of the studies. Many questions remain unanswered about content, methodology and outcome parameters. Behavioural interventions are also culture-dependent, which poses a challenge for devising a uniform protocol for a diverse patient population. One of the biggest impediments to interpreting the available data on behavioural interventions, such as TPE, is the lack of an ideal ‘behavioural placebo’ that can help reduce bias from the Hawthorne effect – that is, patients changing their behaviour because they are aware they are being studied. Most studies compare TPE to standard medical care alone, which can result in differences in time and attention received by the two groups, potentially leading to bias. However, studies that use TPE as a control with a parallel intervention arm still showed comparable results in both study groups.18,20
Scope for future research
While the current literature includes some interesting, high-quality trials, many RCTs employ multiple behavioural interventions simultaneously (e.g., cognitive behavioural therapy, relaxation techniques, biofeedback), which can diminish the outcomes of particular interventions. Future research should focus on studying these non-pharmacological interventions individually, and in comparison, to different comparator interventions. Given the heterogeneity in methodology, different TPE methods can also be compared, such as whether a web-based or AI-based intervention is as effective as group sessions. Another pertinent question is regarding the optimal dosing of TPE. Some studies incorporated a one-time educational intervention, while others emphasized the importance of reinforcement and repeated exposure. The existing literature does not adequately address this issue, and there is a need for focused research. Behavioural interventions require a learning and implementation curve, which often takes time. While most studies follow patients for 3- to 12-month periods, longer follow-up may be warranted to better capture the fluctuating nature of the disease and sustained effects of the behavioural intervention. Lastly, future cost-benefit analyses will better help guide clinicians in incorporating TPE in everyday practice.
Conclusion
To conclude, TPE is a low-cost and accessible non-pharmacological intervention with emerging evidence supporting its efficacy, and it presents as a promising avenue for further research in migraine management. TPE is not as straightforward as optimizing drug dosing but involves a multitude of psychosocial elements that require more thorough assessments than mere statistical data from a few outcome measures. This review provided a comprehensive overview of the current literature and offered considerations for the practical application of the intervention.
Clinical implications
TPE is a structured programme empowering migraine patients toward self-management and behavioural change.
Evidence shows TPE with standard treatments outperforms standard treatments alone, with in-person group sessions proving superior to digital or written formats.
Effective delivery of TPE does not require headache experts; trained nurses, medical students and lay migraineurs can successfully facilitate it.
Footnotes
Ethical approval
Not required for a retrospective narrative review.
Consent for publication
The authors agree to publish with Cephalalgia Reports, if the manuscript is accepted.
Author contributions
Mridula Garg: Review of literature, critical analysis of the existent data, synthesis of the existing data, draft of the manuscript.
Samiran Chowdhury: Review of literature, Tables and figures, draft of the manuscript.
Debashish Chowdhury: Conceptualization, critical analysis of the draft and final structure of the review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used for this article may be obtained from the authors with a reasonable request.