
Abstract
Infectious keratitis (IK) is a serious vision-threatening ophthalmologic emergency that can lead to irreversible complications such as blindness or corneal scarring. IK can be caused by various types of microorganisms, including bacteria, fungi, protozoa, and viruses, which can cause an inflammatory response and penetrate deep into the cornea, leading to perforation in addition to scarring and ulceration. Given the need for thorough and rapid evaluation of patients with IK, effective ophthalmic imaging techniques that provide both quantitative and qualitative information are essential clinician tools. In this narrative review, we outline the benefits of anterior segment optical coherence tomography as a noninvasive, quantitative and qualitative modality for the supportive assessment of IK and for the longitudinal monitoring of corneal abnormalities that may result from infection.
Keywords
Introduction
Infectious keratitis (IK) is a serious vision-threatening ophthalmologic emergency that can lead to irreversible complications such as blindness or corneal scarring.1,2 IK can be caused by various types of microorganisms, including bacteria, fungi, protozoa, and viruses, which can cause an inflammatory response and penetrate deep into the cornea, leading to perforation in addition to scarring and ulceration. 3 Although microbiological cultures performed by scraping are the gold standard for diagnosis, corneal stromal biopsies are an alternative method in negative cases.
Bacterial keratitis (BK) is the most common form of IK, which may be characterized on slit-lamp examination by conjunctival reaction, gray-white corneal infiltrate at the epithelial and stromal levels, and ciliary injections. The absence of any differentiating clinical signs made Gram and Giemsa stains more valuable for initiating treatment. Sensitivity and specificity were reported to be 56.6% and 97.8%, respectively, compared with culture for BK identification. 4
Clinical signs of fungal keratitis (FK) such as irregular feathery margins, stellate lesions, ring infiltration, and endothelial plaque may increase the clinical suspicion of the specialist, but additional testing is required for an accurate diagnosis. Therefore, corneal scraping is required for confirmation with direct microscopy as an initial step in diagnosis, using potassium hydroxide (KOH) wet preparation or Gram and Giemsa stain, followed with microbiological culture. 5 Despite cultures as the gold standard, culture of FK has shown low sensitivity compared to 10% KOH in which studies have reported 81% sensitivity.5–7
Herpetic keratitis (HK) is characterized by dendritic lesions, swollen margins, and infiltration of the epithelium. 8 In addition to clinical features, 12% of HK were detected by culture and 88% by polymerase chain reaction (PCR). 9 Although, PCR is consistently more sensitive and faster than culture, several factors can decrease PCR sensitivity such as prior topical antibiotic or antiviral treatment, early-stage infection, specimen type, rate of pathogen recovery, atypical lesion, and depth of infection.10–12
The overlapping clinical signs in the different types of keratitis, the dependence on expertise, the time-consuming procedures, and the importance of prompt diagnosis and treatment require a repertoire of tools to make better clinical decisions. To this end, various imaging methods such as in vivo confocal microscopy (IVCM) and anterior segment optical coherence tomography (AS-OCT) have emerged to assist in diagnosing and grading the severity of IK. 13
IVCM offers significant value for assessing severity and providing quantitative analysis of corneal layers, nerves, and cells and has been used in different types of keratitis such as bacterial, viral, and has been particularly valuable in fungal and Acanthamoebic.14–17 However, dependence on IVCM interpretation by specialists can be a drawback due to innate human errors. Other drawbacks include the requirement for skilled technicians, patient cooperation, limited ability to diagnose bacteria and viruses due to resolution constraints, high costs, and susceptibility to motion artifacts. 13 On the other hand, AS-OCT can precisely identify and outline the depth and scope of corneal ulceration, infiltrates, and haze. This capability aids in characterizing, quantifying, and tracking the progression of diverse corneal conditions, including both superficial and deep-seated IK.18–21
Given the need for thorough evaluation of patients with IK, this narrative review outlines the benefits of AS-OCT as a noninvasive, quantitative, and qualitative modality for the supportive assessment of IK, and the longitudinal monitoring of corneal abnormalities that may result from infection.
Methods
A structured literature search was conducted across four electronic databases (Scopus, Web of Science, Google Scholar, and PubMed) for articles published through October 2025. The search strategy combined keywords and controlled vocabulary (e.g., MeSH terms), including “optical coherence tomography,” “anterior segment OCT,” “keratitis,” “Acanthamoeba keratitis,” “herpes simplex virus keratitis,” “fungal keratitis,” and “infectious keratitis.” Reference lists of relevant articles were also manually screened to identify additional studies.
Eligibility criteria were defined a priori. Studies were included if they (1) evaluated AS-OCT in the setting of IK, (2) reported imaging findings, diagnostic utility, or monitoring applications, and (3) were original studies, case series, or clinically relevant case reports published in English. Studies were excluded if they (1) did not involve IK, (2) focused solely on non-OCT imaging modalities without relevant OCT correlation, (3) or lacked sufficient clinical or imaging detail.
All records identified through database searching were imported and duplicates were removed. Titles and abstracts were independently screened by two reviewers (MA and ZB) to assess relevance. Discrepancies were resolved through discussion and consensus relevant to the objective of the study. Full-text review was subsequently performed for eligible articles. In total, approximately 312 records were identified, of which 248 remained after duplicate removal. Following title and abstract screening, 96 articles underwent full-text review. Ultimately, 58 studies met inclusion criteria and were included in the qualitative synthesis.
Data extracted included study design, organism/infectious etiology, imaging modality, and relevant AS-OCT findings. A qualitative synthesis approach was used to summarize imaging characteristics and clinical applications across different types of IK.
Principle of anterior segment optical coherence tomography
Anterior segment optical coherence tomography is a noncontact optical modality that utilizes low-coherence interferometry to produce rapid cross-sectional images of corneal morphology and anterior segment structures in vivo.22,23 Image acquisition speed and resolution technology have recently improved. 22 In 2001, Bechmann et al reported for the first time the analysis of central corneal thickness using a time-domain (TD) OCT system. 24 In the same year, Radhakrishnan et al. presented the Fourier-domain (FD) OCT system designed for imaging the anterior segment of the eye that used 1310 nm and 8 frames per second instead of 830 nm wavelength. This high-speed, high-quality system depicted morphological structure in detail, accurate depth, and location, which is helpful for clinical applications. 25 The first OCT system was based on the TD technology, but its disadvantages, such as slower scanning speed, dependence on the mechanical movement of a mirror in the specimen arm, and lower sensitivity, made it less desirable.26–28
The independence of the spectrometer FD-OCT from any moving parts and the high-speed camera increases its applicability more than the first type. In 2008, the first swept-source device (SS) FD-OCT (Casia SS-OCT; Tomey, Nagoya, Japan) was introduced for three-dimensional imaging of the entire anterior segment of the eye. This device uses a 1310 nm SS laser as the light source for scanning the anterior segment of the eye. The scanning rate is 30,000 per second with a scanning area of 16 × 16 mm with a depth of 6 mm. It uses a narrow-bandwidth light source, resulting in an ultrafast system that can ignore motion artifacts and penetrate to a greater depth of the structure. All these features make it an important tool for clinical diagnosis.22,29
Different types of keratitis
Acanthamoeba keratitis
Acanthamoeba Keratitis (AK) is a severe, sight-threatening, worldwide eye infection. An Acanthamoeba is a protozoan that exhibits a 2-stage life cycle, alternating between an active trophozoite and dormant cyst form, as it lives in a variety of environments, including air, soil, and water. 30 Trauma and contact with contaminated water are the main risk factors. Contact lens wearers are affected in 85% of cases as contact lenses can trap the organisms and lead to subsequent keratitis. 31
Patients with AK may experience pain with photophobia, annular stromal infiltrates, epithelial defects, and eyelid edema. Diagnosis of AK remains difficult with the current use of cultures, corneal smears, and PCR to aid in identification of the protozoan. 30 Not only may diagnosis be limited by the fact that cultures may take several weeks to indicate a positive result, but the sensitivity of culture can also range significantly from 33% to 67%.15,32 As an alternative, PCR is a promising method, but its availability across laboratories may limit its use. IVCM also plays a role as a noninvasive method for the diagnosis of AK. Confocal imaging of corneas in suspected AK displays both the cyst and trophozoite forms of this parasite. The size of cysts is more suitable for detection by IVCM than that of bacteria and viruses. 15
Although microbiological methods and clinical presentation can be helpful in diagnosing Acanthamoeba, AS-OCT helped in visualizing the depth of the reflective bands of radial keratoneuritis and, in follow-up examinations, to monitor and demonstrate treatment success.33,34 Although radial keratoneuritis can be visualized very early in AK with AS-OCT, these patterns can be misdiagnosed as dendritic infiltration in HK.35,36 A comparison of AS-OCT in both AK and HK patients demonstrated that radial keratoneuritis occurred at different depths of the stroma in AK and disappeared after treatment. However, in HK, refractive lesions occur in the subepithelium without invading a deeper layer of the stroma, and in some cases, the epithelial layer is irregular. In a study by Park et al., reflective bands were observed in the corneal stroma corresponding to radial keratoneuritis in their patient cases. With appropriate AK treatment, the radial keratoneuritis resolved and the reflective bands disappeared. Corneal nerve bundles typically enter peripherally of the cornea and progress toward the center beneath the anterior third of the stroma. Reflective bands in this study aligned with this corneal nerve passage. However, AS-OCT could not identify AK cysts or trophozoites due to limited power resolution, making it unsuitable to replace tissue culture. 35 Studies that have used OCT in various types of keratitis were summarized in Table 1.
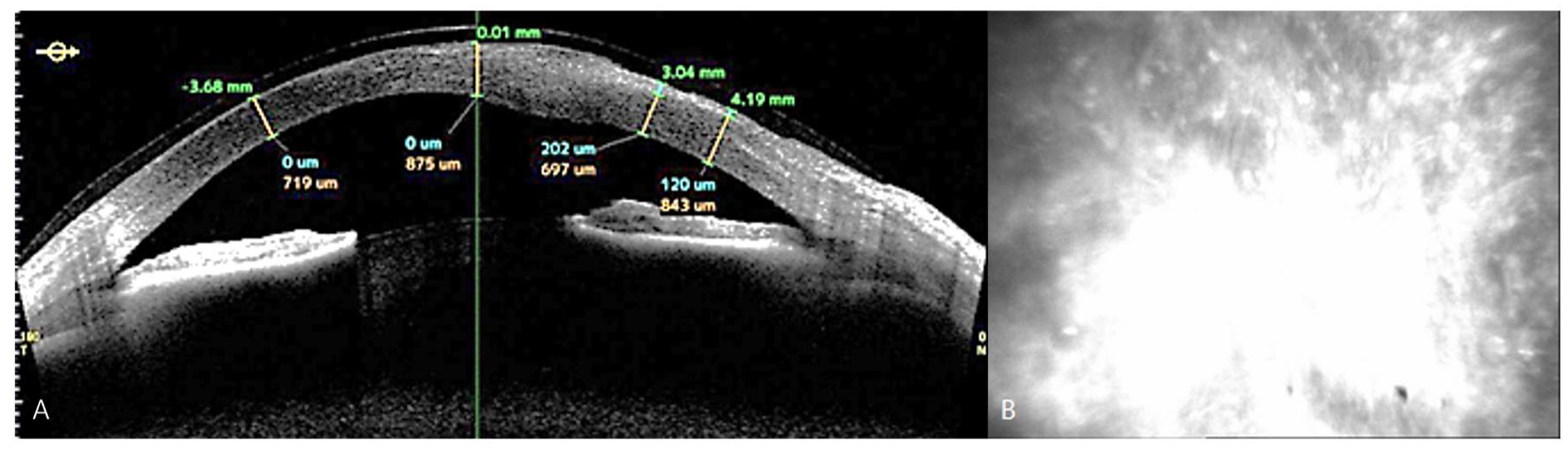
Studies using OCT in different types of keratitis.
Studies were included if they provided clearly described AS-OCT imaging findings, quantitative measurements, or comparative insights across infectious etiologies. Priority was given to studies with relevant imaging features or clinical relevance to enhance interpretability and educational value.
AS, anterior segment; CCT, central corneal thickness; CT, corneal thickness; HOA, higher-order aberrations; IT, infiltrate thickness; IW, infiltrate width; KP, keratic precipitates; OCT, optical coherence tomograph; OD, right eye; OS, left eye; SD, spectral domain; Spp., species.
Fungal keratitis
FK accounts for a small percentage of all types of keratitis, and tropical climate is one of the most important predisposing factors.49–51 Pathogens include Candida species (spp.) and filamentous fungi such as Aspergillus and Fusarium spp. 52 Risk factors include long-term steroid use, ocular trauma with vegetative material, specific contact lens solutions, antibiotic use, immunosuppressive disease, and chronic ocular surface disease. 3 The clinical presentation of FK is nonspecific but may aid in diagnosis. FK usually has the following features: firm and dry raised hyphae extending to the normal cornea, multifocal granular infiltration, and satellite stromal infiltration. 51
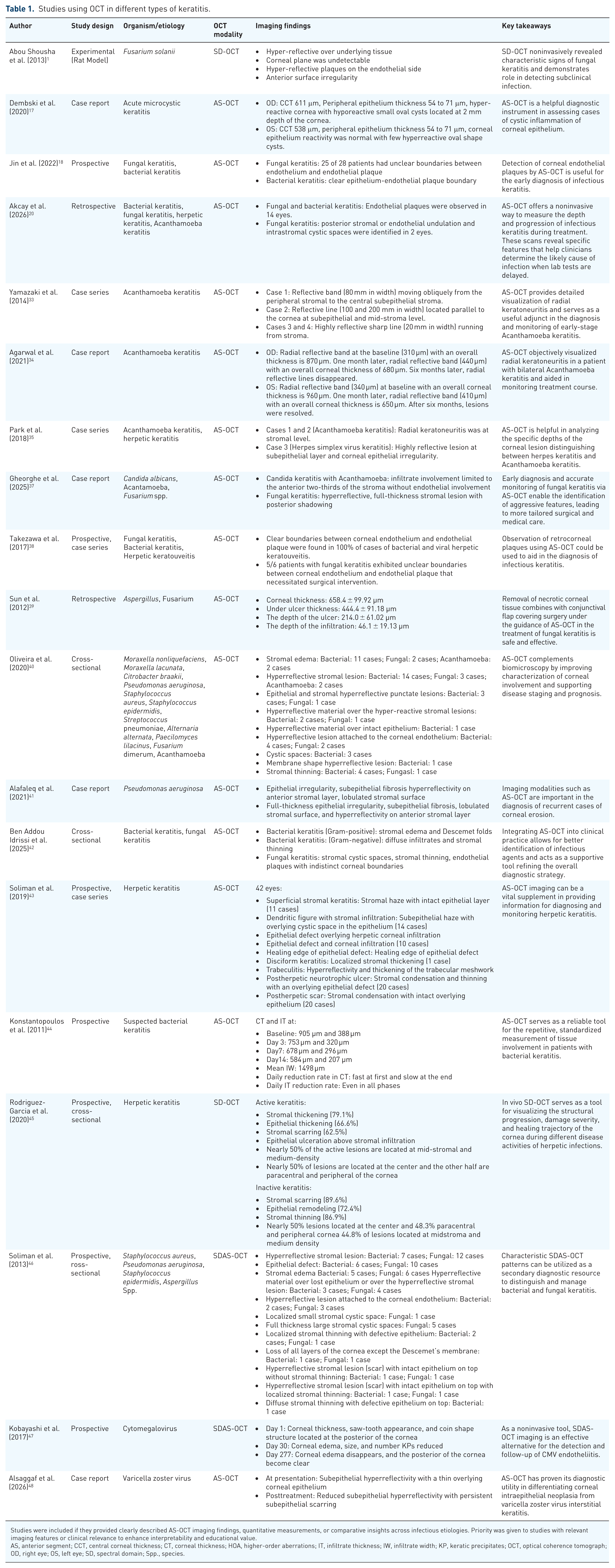
Generally, AS-OCT is a tool for early identification of fungal characteristics that have a poor treatment prognosis due to invasion of deep layers, so early diagnosis and treatment evaluation is critical.18,37 Endothelial plaques are often a feature of fungal infections and AS-OCT may assist in identifying features of endothelial plaques that may distinguish fungal plaques from bacterial and viral forms.38,53 Also, previous studies indicated that AS-OCT showed unclear boundaries between the endothelial plaque and corneal endothelial surface in cases of FK. 38 It has also been shown that removing necrotic corneal tissue alongside a conjunctival flap under the guidance of AS-OCT, is safe and efficient in treating FK.39,54 Therefore, this method can be used in assessing the diagnosis, management, and prognosis of this type of IK. 18 Figure 1 shows the use of AS-OCT and IVCM in a FK case.
A patient at presentation was shown to have a deep endothelial plaque. Gram stain analysis of the excised cornea demonstrated fungal hyphae infiltrating the corneal stroma and reaching the retrocorneal surface. (a) AS-OCT imaging revealed deep endothelial plaque and ill-defined separation between the corneal endothelium and the plaque. Clear contact lens was worn at the time of imaging (*). (b) In vivo confocal microscopy further supported the diagnosis by visualizing high-contrast linear structures consistent with fungal hyphae.
Bacterial keratitis
BK is a common visual-threatening corneal pathology with risk factors that include ocular surface disease, immunodeficiency, corneal trauma, contact lens wear, and ocular surgery. 55 Streptococci and Staphylococci are a common type of ocular flora that can cause ulceration if the eye’s natural protective barriers are compromised. 56 A higher prevalence of BK due to Gram-negative rods (e.g., Pseudomonas spp.) is observed in contact lens wearers. 57
In patients with BK, AS-OCT can be used as a tool to complement biomicroscopy and assist in early management through characterizing corneal involvement to help with staging and providing prognostic evidence.40,58 AS-OCT findings may include stromal edema, hyperreflective stromal lesions, punctate hyperreflective lesions in both epithelium and stroma, hyperreflective material over stromal lesions and intact epithelium, cystic spaces, membrane-shaped hyperreflective lesions, stromal thinning, and lesions attached to corneal endothelium.40,41
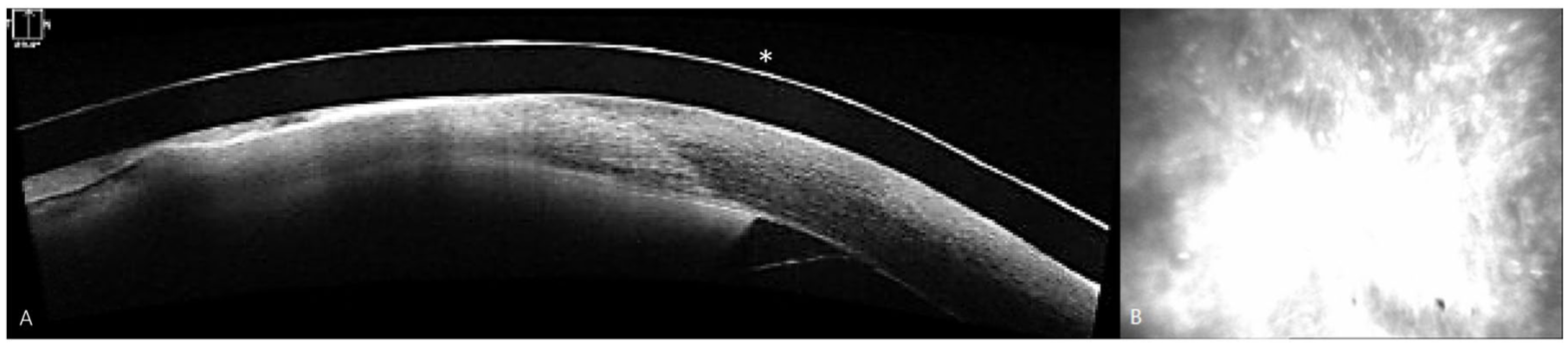
Oliveira et al. observed that a patient with BK due to C. braakii demonstrated corneal thinning and hyperreflective stromal lesion suggesting a severe inflammatory reaction and poor prognosis. 40 Additionally, clear epithelium-endothelial plaque boundary can be observed in patients with BK as an important finding in the AS-OCT.18,40 In a study by Ben Addou Idrissi et al., they demonstrated distinct AS-OCT patterns for BK. Gram-positive BK was associated with Descemet folds and stromal edema, while Gram-negative BK was associated with stromal thinning and diffuse infiltrates. Their study showed that diagnostic sensitivity improved to 66.7% for Gram-negative BK and 75% for Gram-positive when combining clinical findings with AS-OCT. 42 The use of AS-OCT aids in the diagnosis of BK and monitoring of bacterial progression. Figure 2 shows the use of AS-OCT and IVCM in a BK case.
A 42-year-old woman with soft contact lens use for high myopia presented with a two-week history of ocular redness. Examination revealed a superficial corneal infiltrate with an active leading edge and central punctate lesions arranged in a wreath-like pattern. Gram stain identified gram-positive bacteria with beaded branching morphology identified as Nocardia spp. (a) AS-OCT imaging demonstrated increased corneal thickness corresponding to the mid-stromal infiltrate. (b) In vivo confocal microscopy revealed multiple short, thin, beaded, bright filamentous structures with right-angled branching.
Herpetic keratitis
HK is another common cause of IK and can lead to impaired vision. The most common manifestation is the dendritic ulcer, which exhibits a branching appearance when visualized with fluorescein dye. In neurotrophic keratopathy, corneal ulceration and punctate epithelial erosions result. 53 Another category of HK, stromal keratitis, which may also be referred to as necrotizing stromal keratitis, occurs less commonly but with more significant destruction of the tissue, leading to opacification with thinning and perforation of the cornea. In endotheliitis, the resulting inflammation of the corneal endothelium during the course of ongoing or recurrent keratitis causes endothelial dysfunction, promoting stromal edema and opacification.43,59,60 Herpetic corneal infiltrates seen on imaging typically appear as a spindle-shaped area or lentiform with increased reflectivity in the stroma, which can be localized or diffused. 43
Notably, there is no published consensus addressing the confocal diagnostic criteria for viral keratitis and the resolution of the available confocal imaging systems precludes visualization of any potential viral particles.16,61 Further large studies are needed to standardize its characteristics for elucidating the use of IVCM in the diagnosis. 16 Alternatively, Park et al. demonstrated the utility of AS-OCT in distinguishing features of and aiding in the diagnosis of HK, noting subepithelial hyper-reflective lesions and occasional corneal epithelial irregularity. 35 Moreover, AS-OCT can be performed in cases of endothelial, stromal, and epithelial keratitis to obtain pachymetry and epithelial thickness mapping to track corneal edema resolution and assess treatment efficacy.59,62
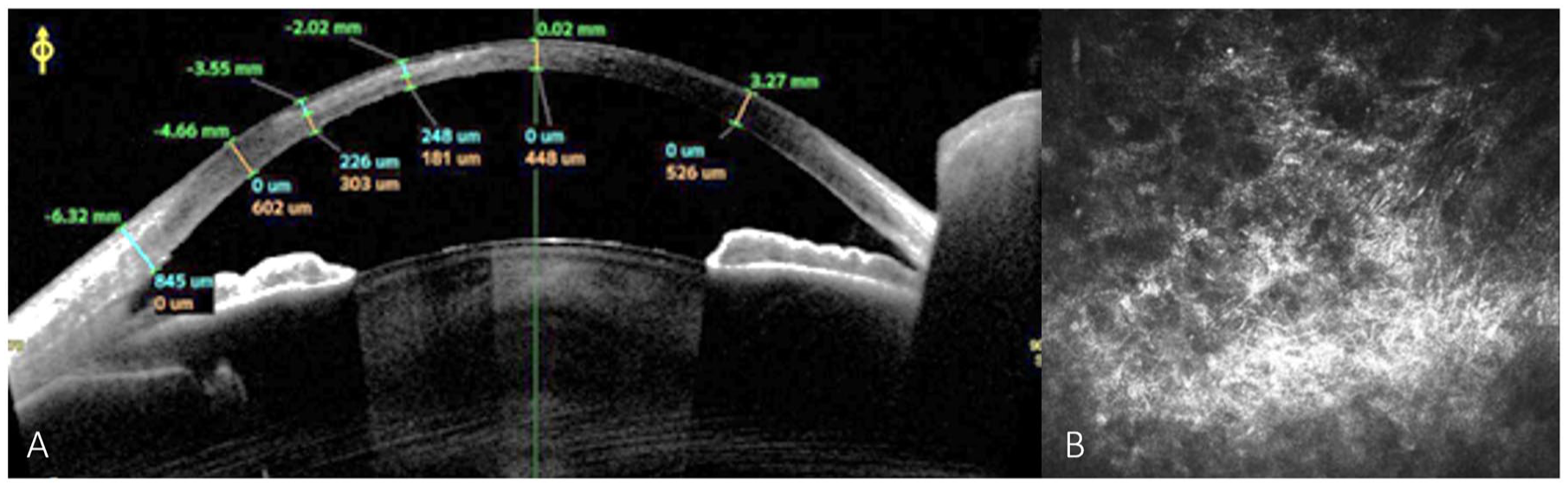
AS-OCT imaging aids in distinguishing between active infiltrates and stromal scarring. Active HK is characterized by considerable stromal and epithelial thickening, whereas inactive disease displays epithelial remodeling in areas of stromal thinning due to scarring. Though, this can be challenging during the healing phase when both may be present. Necrotizing keratitis is distinguished by a deformed corneal structure, extensive stromal inflammatory infiltration, and corneal thinning. 58 In line with its use in the detection of other forms of keratitis, AS-OCT may be an appropriate method for detection, management, and follow-up of HK. 63 Figure 3 shows the use of AS-OCT and IVCM in a HK case.
A 38-year-old woman presented with a keratitis characterized by a white-yellow stromal infiltrate with indistinct borders, stromal edema, hypopyon, and a retrocorneal plaque. PCR testing confirmed herpes simplex virus type 1 infection. (a) AS-OCT imaging demonstrated a distinct interface between the corneal endothelium and the plaque. (b) In vivo confocal microscopy revealed a network of hyper-reflective keratocytes and inflammatory cells within the corneal stroma; however, no atypical organisms were visualized.
Discussion
The four main types of keratitis are Acanthamoebic, fungal, bacterial, and herpetic. In AK, superficial keratitis may migrate to the deep layers over time. The pseudodendritiform epitheliopathy in these patients may be misdiagnosed as the dendritic patterns that occur in HSV patients if clinicians fail to appreciate differences in the corneal layers affected. 35 Additionally, while multifocal stromal infiltration in AK and FK would exhibit the same pattern in both causes of infection, the primary difference can be seen in the proclivity of AK to cause perineural stromal infiltration.64,65 This pattern of similarity between different types of microorganisms can lead to misdiagnosis, delay in diagnosis, and poor prognosis. 38
In addition to the overlapping clinical signs, the time-consuming culturing and dependence on clinical suspicion have led researchers to introduce image-guided diagnosis such as IVCM and AS-OCT. These are rapid imaging modalities that inform us about the structure and characteristics of the lesion in detail. 13 For example, IVCM diagnosed atypical IK (AK and FK) with a sensitivity of 85.3% and a specificity of 100%. 16 Additionally, AS-OCT detected different depths and orientations of radial keratoneuritis in patients with AK and distinguished between AK and HK according to the depth of invasion.33,35 In BK, there is a tendency to evaluate treatment response based on corneal thickness, infiltrate thickness, and infiltrate width, suggesting that it plays a role in both treatment evaluation and diagnosis. 44 In FK, both IVCM and AS-OCT have been used to evaluate the disease, identifying numerous hyperreactive and dendritic cells in the epithelial layers and hyperreactive filaments and oval bodies in the stromal layer. 17 In addition to illustrating the corneal edema and an uneven corneal surface that may occur in FK, AS-OCT highlighted infiltration of anterior stroma and diffuse edema of the stroma, underlining specific findings that may assist in early diagnosis of infection.66,67
AS-OCT may serve a critical role not only in detection and identification of features that distinguish various forms of keratitis but also in prognosticating postinfection visual acuity and monitoring changes in higher-order aberrations and scarring.68–70 By identifying features of fungal endothelial plaques that may indicate a future need for surgery, AS-OCT may assist clinicians as they determine the direction of care as well as improving the efficiency and quality of care. 38 In particular cases of FK that may lead to devastating vision loss, AS-OCT may allow for early and improved detection of fungal pathogens and preservation of vision for patients. 18 Similarly, AS-OCT captured changes in higher-order aberrations (HOA) for patients before and following treatment, indicating improvement in corneal aberrations after medical intervention.59,69 Pretreatment HOA helped to predict posttreatment visual acuity and, therefore, AS-OCT can be used to assist clinicians in setting expectations for patients as they seek care.
AS-OCT presents a promising modality for the detection, management, and monitoring of IK, differentiating between potential etiologies, indicating improvement with treatment, and prognosticating outcomes following intervention.