
Abstract
Background:
Neurotrophic keratitis (NK) is a rare, degenerative disease of the cornea that arises from impaired trigeminal nerve innervation. The condition leads to progressive corneal anesthesia, epithelial breakdown, ulceration, and potential perforation. Cenegermin, a recombinant form of human nerve growth factor, is the first pharmacotherapy approved for this indication and operates through a disease-modifying mechanism that promotes corneal nerve regeneration.
Objectives:
To evaluate the therapeutic efficacy and safety profile of topical cenegermin (20 mcg/mL) compared with vehicle in adults with moderate to severe NK (Mackie classification stage 2 or 3) by quantitatively synthesizing evidence from randomized controlled trials (RCTs).
Design:
Systematic review and meta-analysis of RCTs, conducted in accordance with the PRISMA 2020 statement and the Cochrane Handbook for Systematic Reviews of Interventions.
Data sources and methods:
PubMed, Web of Science, and Cochrane CENTRAL were searched from inception through February 2026. Two double-masked, vehicle-controlled RCTs (the REPARO trial and the NGF0214 trial) enrolling 148 adults were included. Data were pooled using random-effects models (DerSimonian–Laird) and reported as risk ratios (RRs) with 95% confidence intervals (CI). Risk differences (RDs) and the number needed to treat (NNT) were also computed. Certainty of evidence was appraised using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework.
Results:
Cenegermin substantially increased the probability of complete corneal healing at 8 weeks, with a pooled RR of 1.84 (95% CI 1.34–2.52; z = 3.8; p = 0.0001) and minimal between-study heterogeneity (I-squared = 0%; tau-squared = 0.00). The model-based pooled RD was 0.42 (95% CI 0.24–0.60), yielding an NNT of 3 (95% CI 2–5). The crude pooled event rates were 72.6% in the cenegermin group versus 38.7% in the vehicle group. Regarding safety, the pooled RR for any adverse event was 1.07 (95% CI 0.64–1.78; p = 0.80), showing no significant difference between groups. The overall certainty of evidence was rated as moderate for both outcomes under the GRADE framework.
Conclusion:
Cenegermin is an effective and well-tolerated, disease-modifying therapy for moderate to severe NK. It nearly doubles the likelihood of complete corneal healing and represents an important addition to the therapeutic options available for this debilitating condition. Larger, independently funded trials with longer follow-up are warranted to confirm these findings and to establish its position within the treatment algorithm.
Trial registration:
PROSPERO CRD420251103148.
Plain language summary
Neurotrophic keratitis is an uncommon eye condition in which the nerves that supply the front surface of the eye (the cornea) become damaged. When these nerves stop working properly, the cornea can develop open sores that do not heal on their own, which may eventually lead to serious vision problems. Until recently, treatments for this condition were limited to protective measures such as lubricating eye drops, special contact lenses, or surgical procedures that did not address the root cause of the nerve damage.
Cenegermin is an eye drop medication that was specifically developed to treat this condition. It is a laboratory-made version of a natural protein called nerve growth factor, which helps repair and regenerate damaged nerves. By restoring nerve function in the cornea, cenegermin promotes healing of the damaged surface.
In this study, we combined the results of the two main clinical trials that tested cenegermin against an inactive eye drop (placebo) in patients with moderate or severe neurotrophic keratitis. Our findings show that patients treated with cenegermin were nearly twice as likely to achieve complete healing of their cornea compared with those who received the placebo. Importantly, cenegermin did not appear to cause more side effects than the placebo. The most commonly reported side effect was mild, temporary eye discomfort, which may actually reflect the recovery of corneal nerve sensation, a sign that the medication is working as intended.
These findings support cenegermin as an effective and well-tolerated treatment option for patients with this challenging eye condition.
Keywords
Introduction
Neurotrophic keratitis (NK) is a rare, progressive corneal disease that results from damage to the ophthalmic division of the trigeminal nerve, leading to partial or complete loss of corneal sensation. 1 The sub-basal nerve plexus of the cornea serves multiple protective and trophic functions: it triggers the blink reflex, stimulates lacrimal secretion, and sustains epithelial cell proliferation and turnover. 2 When this neural supply is compromised, the cornea becomes vulnerable to epithelial breakdown, persistent ulceration, stromal melting, and, in advanced cases, frank perforation. 3 The condition is classified into three clinical stages according to the Mackie grading system: stage 1 (punctate epitheliopathy with or without stromal scarring), stage 2 (persistent epithelial defect with smooth, rolled edges), and stage 3 (deep corneal ulcer with risk of perforation). 4 Etiologies include herpes simplex or herpes zoster keratitis, diabetes mellitus, multiple sclerosis, neurosurgical or maxillofacial procedures, and traumatic or iatrogenic injury to the trigeminal pathway.3,5
Management of NK has historically relied on a spectrum of supportive and protective interventions tailored to disease severity. In the early stages, treatment typically involved preservative-free artificial tears, therapeutic contact lenses, and autologous serum therapy. 6 For refractory or advanced cases, surgical approaches such as tarsorrhaphy, amniotic membrane transplantation, conjunctival flap procedures, and, as a last resort, corneal transplantation have been employed. 7 More recently, topical insulin has attracted interest as an emerging adjunctive therapy, with reported concentrations varying widely from 0.5 IU/mL to approximately 100 IU/mL (depending on formulation and whether dosing is expressed per milliliter or per drop) to promote epithelial healing and corneal nerve regeneration in small case series and pilot studies.8–10 Nevertheless, all of these strategies are fundamentally palliative or protective in nature and do not address the underlying neurotrophic deficit.
A pivotal advance came with the therapeutic application of nerve growth factor (NGF), an endogenous neurotrophin that plays a central role in neuronal survival, axonal growth, and regeneration. In the ocular surface, NGF contributes to corneal homeostasis by supporting sensory innervation, promoting epithelial repair, and stimulating tear production, functions that are characteristically impaired in NK. 11 The clinical relevance of this biological mechanism was first demonstrated in a landmark report showing that topical murine NGF could heal refractory neurotrophic corneal ulcers. 12 Building on this proof of concept, a recombinant form of human NGF (rhNGF) was developed and formulated as cenegermin. 13
Cenegermin (trade name Oxervate) represents a milestone in the treatment of NK. It is the first and, to date, only pharmacological agent approved by both the United States Food and Drug Administration (FDA) and the European Medicines Agency (EMA) specifically for the treatment of NK. 13 Unlike conventional therapies, cenegermin acts through a disease-modifying mechanism: it restores corneal neurotrophic signaling, facilitates sensory nerve regeneration, and promotes epithelial wound closure. 14
Two pivotal randomized controlled trials (RCTs) have individually reported the efficacy of cenegermin in patients with moderate to severe NK.15,16 However, no systematic review or meta-analysis has yet synthesized the data from these trials to provide a consolidated estimate of the treatment effect and its associated uncertainty. This systematic review and meta-analysis was, therefore, undertaken to quantitatively pool the available RCT evidence on the efficacy and safety of topical cenegermin in the treatment of NK, with the aim of informing clinical decision-making and identifying priorities for future research.
Methods
This systematic review and meta-analysis was designed, conducted, and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement, 17 the Cochrane Handbook for Systematic Reviews of Interventions (version 6.5), 18 and the AMSTAR-2 (Assessing the Methodological Quality of Systematic Reviews 2) guidelines. 19 The review protocol was registered prospectively in PROSPERO (CRD420251103148). Given that this study involved the analysis of previously published aggregate data, institutional ethics review board approval was not required. All procedures adhered to the tenets of the Declaration of Helsinki.
Eligibility criteria
We included RCTs that enrolled adult participants (aged 18 years or older) with a confirmed diagnosis of moderate or severe NK, corresponding to stage 2 or stage 3 of the Mackie classification. 4 The decision to restrict inclusion to stages 2 and 3 was based on two considerations: first, the two pivotal registration trials that formed the basis for regulatory approval exclusively enrolled patients at these stages; second, the primary endpoint of complete corneal healing (defined as a lesion smaller than 0.5 mm by fluorescein staining) is most meaningful in the context of frank epithelial defects (stage 2) or ulceration (stage 3), rather than the punctate epitheliopathy characteristic of stage 1. 4 The intervention of interest was topical cenegermin (rhNGF) at a concentration of 20 mcg/mL, administered six times daily for 8 weeks. Eligible comparators included vehicle (placebo) ophthalmic solutions. Trials were required to report at least one of the following outcomes: complete corneal healing, time to healing, corneal sensitivity, best-corrected distance visual acuity, disease recurrence, or adverse events. We excluded non-randomized studies, case series, single-arm studies, and RCTs that did not include a vehicle-controlled arm or did not isolate the effect of cenegermin.
Search strategy
A systematic literature search was performed across three electronic databases (PubMed, Web of Science, and Cochrane CENTRAL) from inception through February 2026, without language or publication date restrictions. The search strategy combined controlled vocabulary terms and free-text keywords including: “neurotrophic keratitis,” “neurotrophic keratopathy,” “nerve growth factor,” “cenegermin,” “rhNGF,” “efficacy,” “clinical trial,” and “randomized controlled trial.” The full electronic search strategy for each database is provided in Supplemental File 1. Duplicate records were removed using Zotero (version 6.0; https://www.zotero.org). Reference lists of included studies and relevant reviews were hand-searched to identify additional eligible trials.
Study selection and data extraction
Two reviewers independently screened titles and abstracts of all retrieved records for potential eligibility using the Rayyan web application (https://rayyan.ai). Full-text articles of potentially relevant studies were then obtained and assessed against the predefined eligibility criteria. Data extraction was performed independently by two investigators using a standardized form that captured study characteristics, participant demographics, intervention and comparator details, outcome definitions, and numerical results. Discrepancies at any stage were resolved by consensus or, when necessary, by consultation with a third reviewer.
Data analysis
All statistical analyses were performed in R (version 4.3; R Foundation for Statistical Computing) using the metafor and meta packages. The primary summary measure for dichotomous outcomes was the risk ratio (RR), calculated using the Mantel–Haenszel method under both fixed-effect and random-effects (DerSimonian–Laird) models. Risk differences (RDs) with 95% CI were also computed, and the number needed to treat (NNT) was derived from the pooled RD. Between-study heterogeneity was evaluated using Cochran’s Q statistic, the I-squared statistic, and the tau-squared variance estimate. It should be noted that with only two studies included, the power to detect genuine between-study heterogeneity is substantially limited, and an I-squared value of 0% should be interpreted with appropriate caution. 20 Forest plots were generated to display individual study estimates and pooled treatment effects.
The overall certainty of evidence for each outcome was assessed according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework, considering risk of bias, inconsistency, indirectness, imprecision, and publication bias. 21 Given the inclusion of fewer than 10 studies, funnel plots were not generated and formal statistical tests for publication bias (such as the Egger test) were not performed, as these methods lack adequate statistical power with so few data points. 22
Quality assessment
Two authors independently assessed the methodological quality of each included trial using the Cochrane Risk of Bias 2 (RoB 2) tool, which evaluates five domains: bias arising from the randomization process, bias due to deviations from intended interventions, bias due to missing outcome data, bias in measurement of the outcome, and bias in selection of the reported result. 23 Each domain was rated as “low risk,” “some concerns,” or “high risk” of bias, and an overall judgment was assigned for each study. Disagreements between raters were resolved through discussion with a third author.
Results
Study selection
The systematic search across three databases identified a total of 64 records. Following removal of duplicates and clearly irrelevant records, 26 unique citations were screened by title and abstract. Of these, 17 reports were sought for retrieval, of which 2 could not be retrieved. The remaining 15 full-text reports were assessed for eligibility. After applying the predefined inclusion criteria, 13 reports were excluded for the following reasons: non-randomized study design, absence of a vehicle-controlled comparator arm, lack of relevant clinical outcomes, or reporting on populations outside the scope of moderate to severe NK. The literature search was updated through February 2026 and identified no additional eligible RCTs. Two studies were included in the final quantitative synthesis: the REPARO trial (Bonini et al., 2018) and the NGF0214 trial (Pflugfelder et al., 2020). The PRISMA flow diagram of the study selection process is presented in Figure 1.
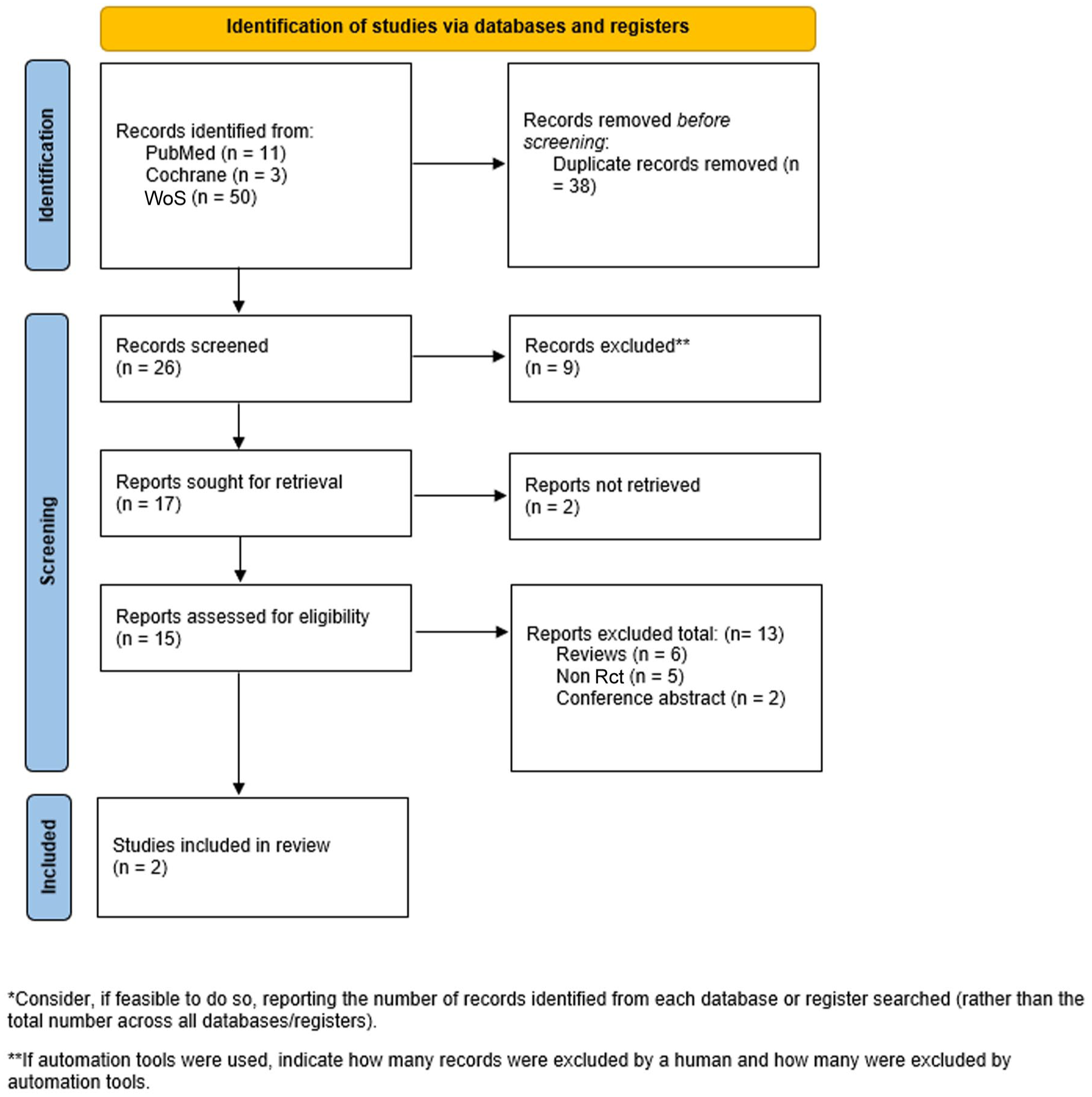
PRISMA flow diagram for studies’ selection process.
Characteristics of the included trials
A total of 148 participants were enrolled across the two trials, with 75 participants in the REPARO trial and 73 in the NGF0214 trial. Both were multicenter, double-masked, vehicle-controlled RCTs sponsored by Dompe Farmaceutici S.p.A. The REPARO trial was conducted across multiple European centers, whereas the NGF0214 trial was conducted in the United States. The study populations comprised adults with a mean age of 61–65 years, diagnosed with stage 2 or stage 3 NK per the Mackie classification. In both trials, the intervention consisted of cenegermin 20 mcg/mL ophthalmic solution administered as one drop six times daily (approximately every 2 h during waking hours) for a duration of 8 weeks. The comparator in both studies was an identical vehicle (placebo) ophthalmic solution administered with the same dosing schedule. Both trials defined complete corneal healing at 8 weeks (defined as a lesion smaller than 0.5 mm on fluorescein staining) as the primary endpoint. The detailed characteristics of the included studies are presented in Table 1.
Characteristics of included randomized controlled trials.
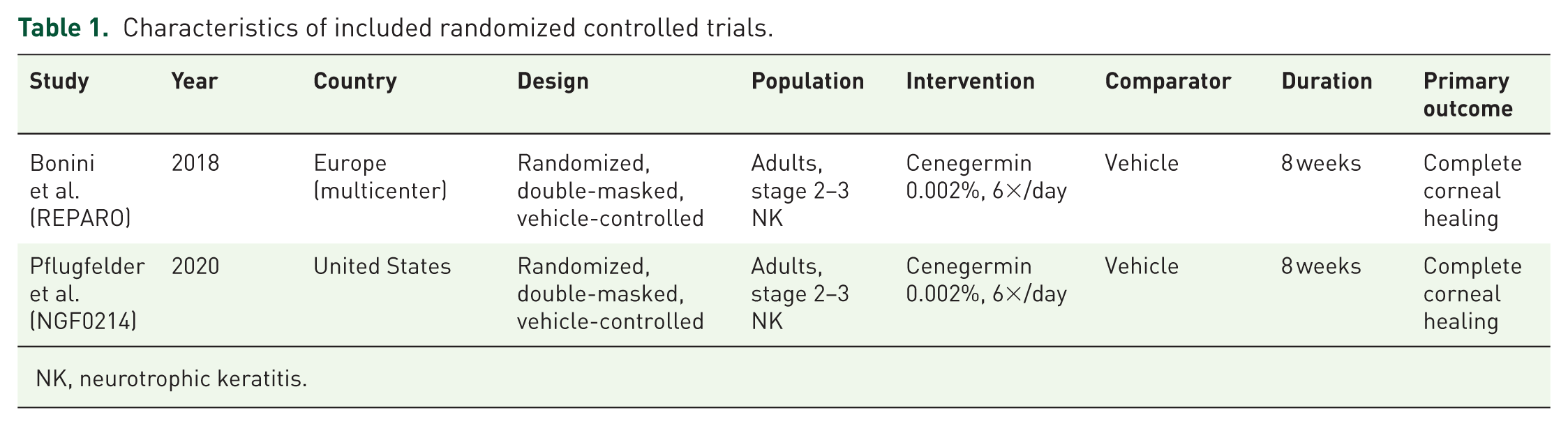
NK, neurotrophic keratitis.
Risk-of-bias assessment
The results of the risk-of-bias assessment are presented in Figure 2 (traffic-light plot) and Figure 3 (summary bar plot). Both trials demonstrated low risk of bias in the domains of randomization, allocation concealment, and attrition. Some concerns were identified in the domain of blinding of participants and personnel: although both studies were described as double-masked and used matching vehicle formulations, the possibility of unmasking due to subtle differences in the physical properties of the solutions (e.g., viscosity) cannot be entirely excluded. Outcome measurement was considered to be at low risk of bias because the primary endpoint (corneal healing) was assessed objectively through fluorescein staining by masked examiners. Selective outcome reporting was judged as low risk, as both trials reported all prespecified outcomes. The overall risk of bias for both studies was rated as low to moderate.

Risk-of-bias traffic light plot (ROB 2).

Summary bar plot of risk-of-bias domains.
Primary efficacy outcome: Complete corneal healing
In the REPARO trial, 37 of 50 evaluable patients (74.0%) in the cenegermin group achieved complete corneal healing at 8 weeks compared with 22 of 51 (43.1%) in the vehicle group (between-group difference 30.9%; 95% CI 10.6–51.1%; p = 0.002). In the NGF0214 trial, complete healing was observed in 16 of 23 patients (69.6%) receiving cenegermin versus 7 of 24 (29.2%) receiving vehicle (between-group difference 40.4%; 95% CI 14.2–66.6%; p = 0.006).
The meta-analytic pooling of these two trials under a random-effects model (DerSimonian–Laird method) yielded a pooled RR of 1.84 (95% CI 1.34–2.52; z = 3.8; p = 0.0001), indicating that cenegermin nearly doubled the likelihood of achieving complete corneal healing relative to vehicle (Figure 4). Between-study heterogeneity was minimal (Q = 0.71; df = 1; p = 0.40; I-squared = 0%; tau-squared = 0.00). A fixed-effect analysis produced an identical pooled estimate (RR = 1.84; 95% CI 1.34–2.52), confirming the robustness of the finding (Figure 5).
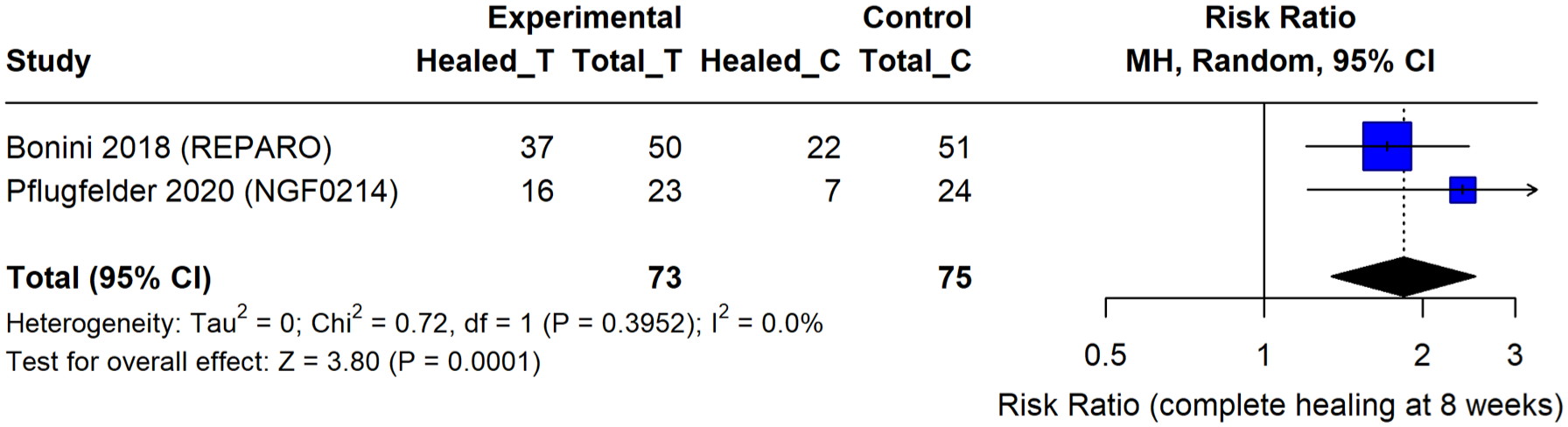
Forest plot showing pooled risk ratio for complete corneal healing (8 weeks).
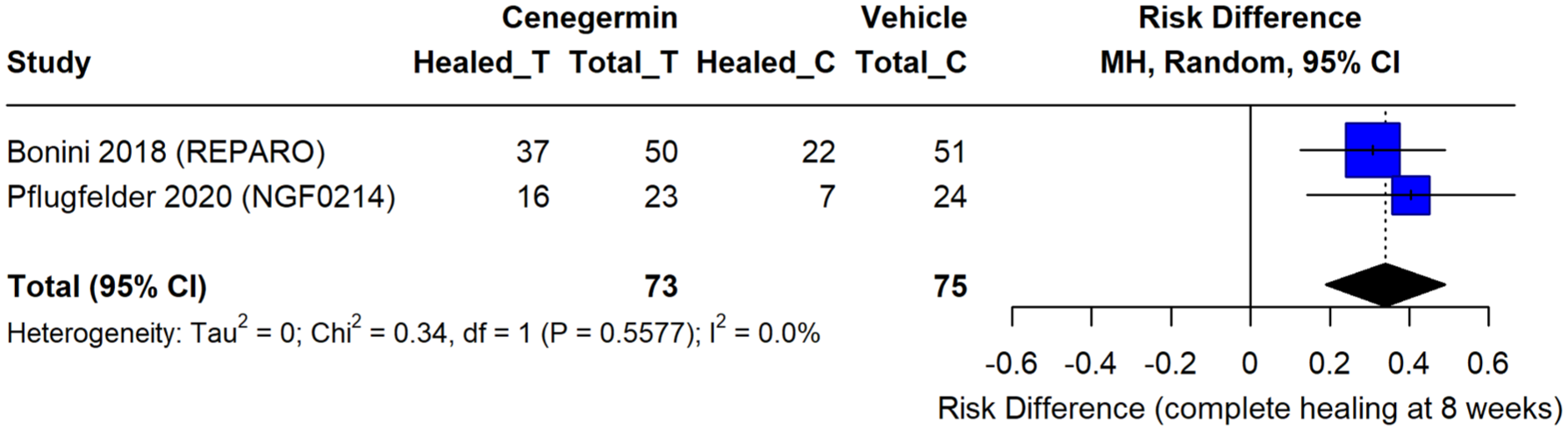
Forest plot showing risk difference summary.
The crude pooled event rates were 72.6% (53 of 73 evaluable patients) in the cenegermin arms and 38.7% (29 of 75) in the vehicle arms, yielding a crude absolute difference of approximately 34 percentage points. However, the model-based pooled RD, which accounts for the inverse-variance weighting of each study, was 0.42 (95% CI 0.24–0.60). This discrepancy arises because the smaller NGF0214 trial, which demonstrated a larger treatment effect (40.4%), receives different weighting under the random-effects model compared with its contribution to the crude pooled rates. The corresponding NNT derived from the model-based RD was 3 (95% CI 2–5), meaning that for every three patients treated with cenegermin, one additional patient achieves complete corneal healing beyond what would be expected with vehicle alone. The overall certainty of evidence according to the GRADE assessment was deemed moderate for complete corneal healing at 8 weeks (Table 2).
Quality and certainty of evidence (GRADE assessment).

CI, confidence intervals; GRADE, grading of recommendations assessment, development and evaluation; RCTs, randomized controlled trials.
The individual study results and pooled estimates are summarized in Table 3.
Primary outcome: complete corneal healing at 8 weeks.
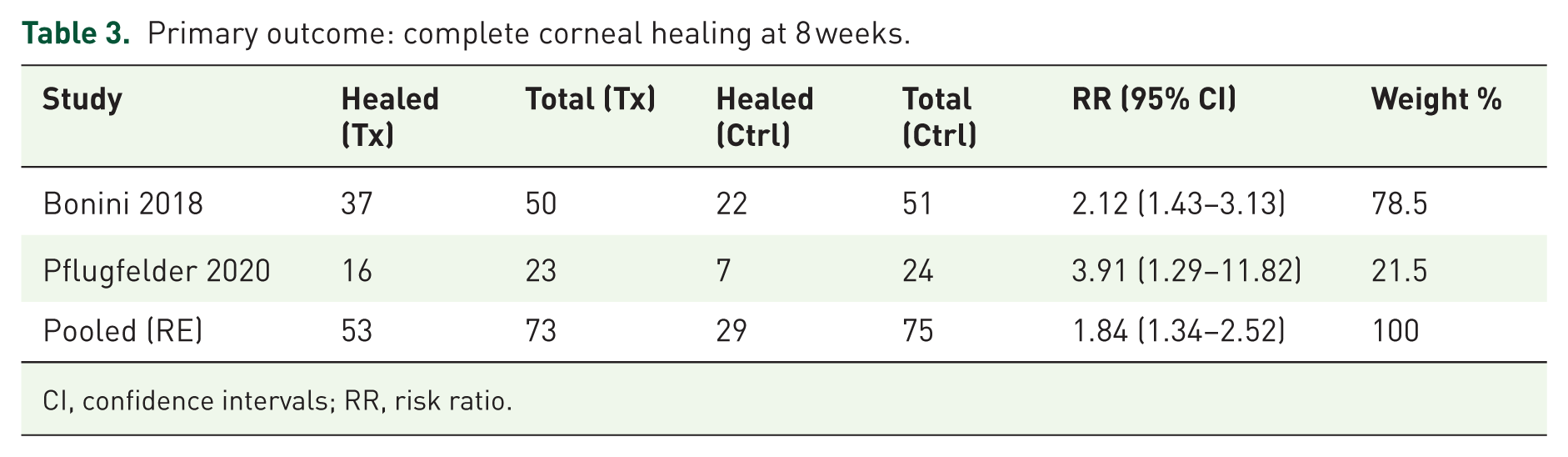
CI, confidence intervals; RR, risk ratio.
Safety and adverse events
The pooled RR for any adverse event under the random-effects model was 1.07 (95% CI 0.64–1.78; p = 0.80), indicating no statistically significant difference in the overall incidence of adverse events between cenegermin and vehicle groups (Table 4 and Figure 6).
Pooled safety outcome: any adverse event.
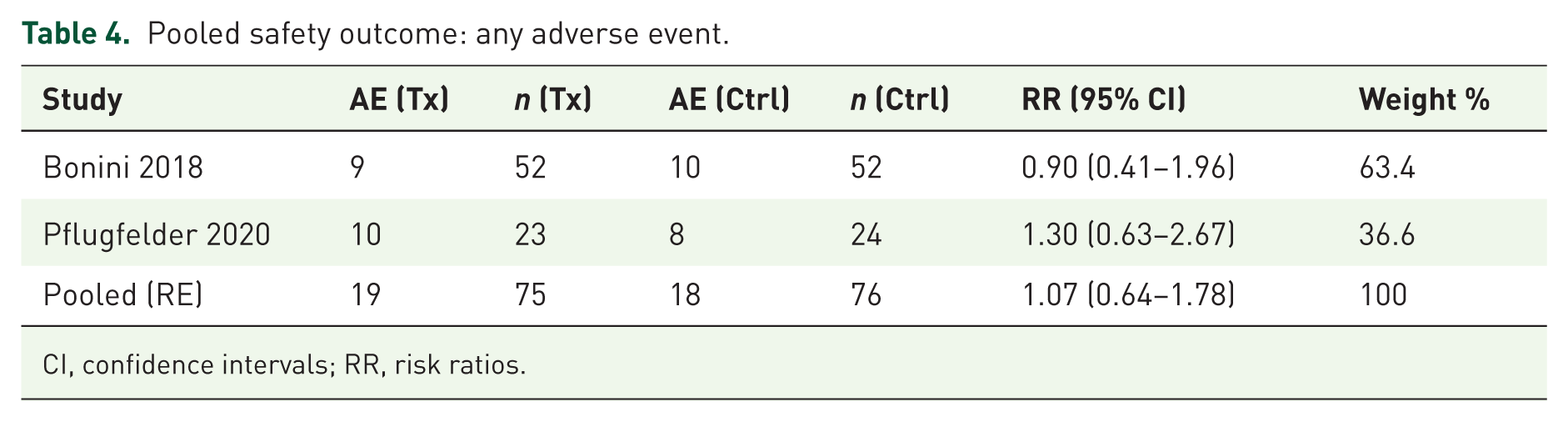
CI, confidence intervals; RR, risk ratios.
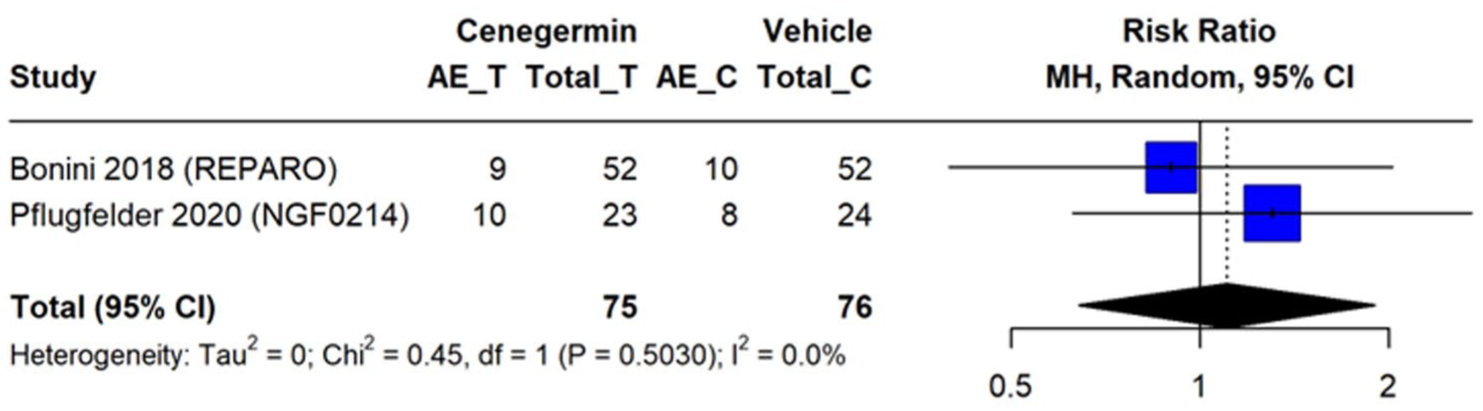
Forest plot for any adverse events.
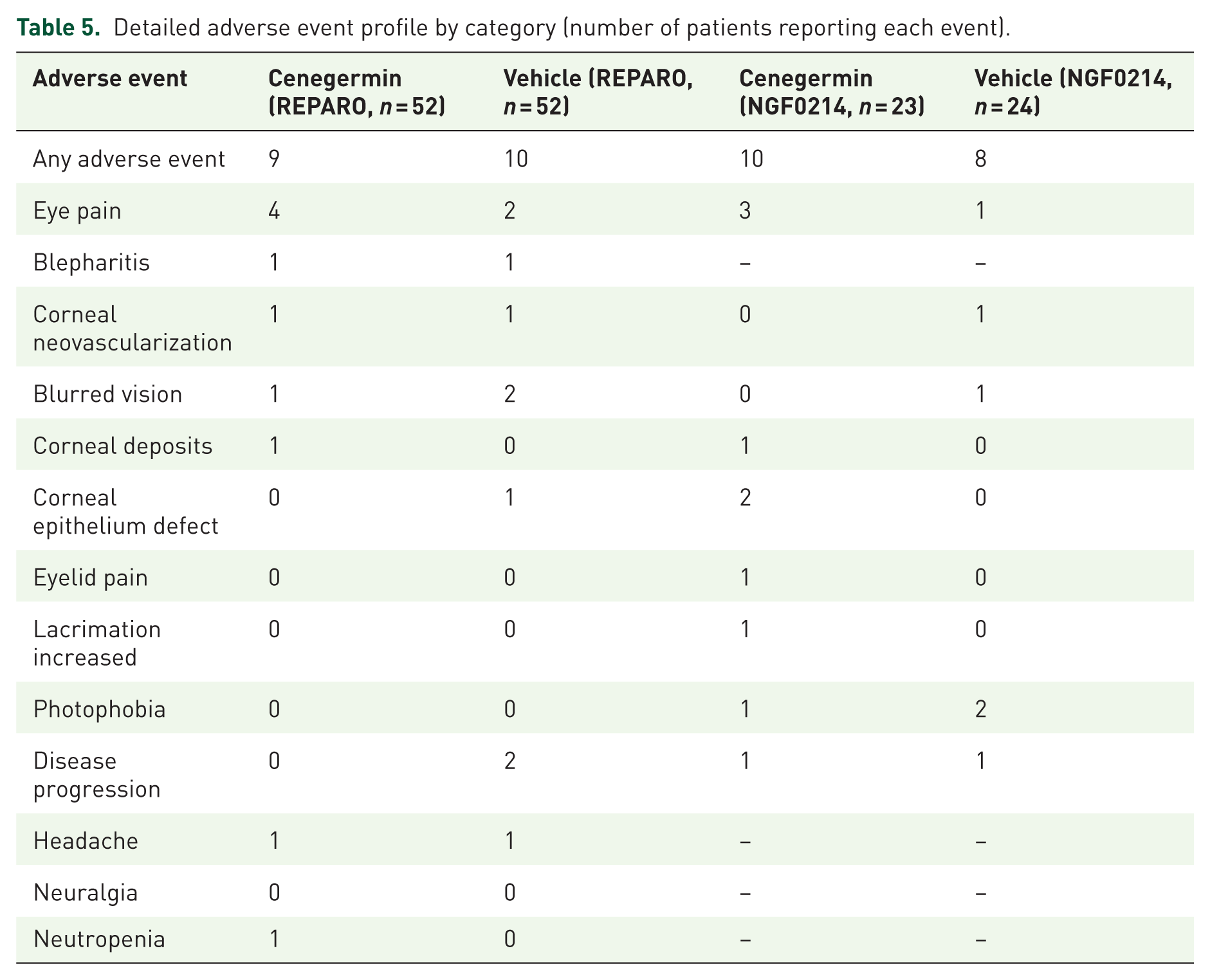
A more detailed analysis of specific adverse events across both trials is presented in Table 5. Eye disorders were the most frequently reported category of adverse events in both the cenegermin and vehicle groups. Specifically, ocular pain was the single most common adverse event associated with cenegermin, reported in 7 of 75 treated patients (9.3%) across both trials compared with 3 of 76 patients (3.9%) in the vehicle groups. Other reported ocular adverse events in the cenegermin arms included blepharitis (one patient), corneal neovascularization (one patient), blurred vision (one patient), corneal deposits (two patients), corneal epithelium defect (two patients), eyelid pain (one patient), increased lacrimation (one patient), and photophobia (one patient). In the vehicle groups, ocular adverse events included blurred vision (three patients), conjunctival hyperaemia (one patient), dry eye (one patient), eyelid edema (one patient), and corneal neovascularization (two patients). Disease progression was reported in one cenegermin-treated patient and three vehicle-treated patients. Non-ocular adverse events were infrequent in both groups and included headache (one cenegermin patient vs one control patient), neuralgia, neutropenia, and cardiac arrhythmia (each in one cenegermin-treated patient in the REPARO trial only).
Detailed adverse event profile by category (number of patients reporting each event).
Discussion
This systematic review and meta-analysis provides, to the best of our knowledge, the first quantitative synthesis of RCT evidence evaluating the therapeutic efficacy and safety of cenegermin in moderate to severe NK. The pooled findings demonstrate that cenegermin nearly doubles the probability of achieving complete corneal healing at 8 weeks (pooled RR 1.84; 95% CI 1.34–2.52), with a model-based absolute RD of 42% and a corresponding NNT of three. These results indicate a treatment effect that is not only statistically significant but also of clear clinical relevance.
The consistency of the treatment effect across the two included trials is noteworthy. In the REPARO trial, 74.0% of cenegermin-treated patients achieved corneal healing compared with 43.1% in the vehicle group, whereas in the NGF0214 trial, the respective rates were 69.6% and 29.2%.15,16 Despite these studies being conducted in different geographic settings (Europe vs the United States) with distinct patient populations, the direction and magnitude of the treatment effect were remarkably consistent, as reflected by the absence of statistical heterogeneity (I-squared = 0%). That said, it is important to acknowledge that the power of heterogeneity tests is substantially limited when only two studies are available, and an I-squared of 0% in this context should not be taken as definitive evidence of homogeneity. 20
The clinical significance of these findings becomes apparent when cenegermin is placed in the context of the existing therapeutic landscape for NK. Conventional management strategies, including preservative-free lubricants, autologous serum therapy, therapeutic contact lenses, tarsorrhaphy, and amniotic membrane transplantation, provide supportive or protective benefits but do not address the neurotrophic deficit that underlies disease progression.6,7 Topical insulin has recently emerged as a potential adjunctive option, with preliminary reports suggesting that concentrations ranging from 0.5 IU/mL up to 100 IU/mL (depending on whether expressed as IU/mL or IU/drop) may promote epithelial healing and nerve regeneration in small series of patients with persistent epithelial defects and neurotrophic keratopathy.8–10 However, randomized controlled evidence for topical insulin remains limited. Cenegermin, by contrast, operates through a fundamentally different mechanism: as a recombinant form of human NGF, it directly restores neurotrophic signaling, facilitates sensory nerve regeneration, and promotes epithelial wound closure.13,14 The NNT of 3 observed in our analysis compares favorably with many therapeutic interventions in ophthalmology and underscores the substantial absolute benefit of this treatment.
Regarding safety, our pooled analysis demonstrated no statistically significant increase in overall adverse event rates among cenegermin-treated patients (pooled RR 1.07; 95% CI 0.64–1.78). The most commonly reported adverse event was ocular pain, which occurred in 9.3% of cenegermin-treated patients compared with 3.9% of vehicle-treated patients. This observation warrants interpretation within the unique pathophysiological context of NK. Because the condition is defined by reduced or absent corneal sensation due to trigeminal nerve dysfunction,1,2 the emergence of pain during treatment with a neurotrophic agent may paradoxically reflect the intended pharmacological action of rhNGF, namely, neural regeneration and the restoration of corneal sensory function. 13 As sensory nerve fibers regenerate and corneal sensitivity returns, patients may experience transient discomfort that is, in effect, a marker of therapeutic neural restoration rather than a conventional adverse drug reaction. Other specific adverse events, including corneal deposits, blurred vision, and eyelid pain, occurred at low frequencies and were generally mild and self-limiting in both groups.
Several emerging studies further support the clinical utility of cenegermin, although they did not meet our eligibility criteria for formal inclusion. The DEFENDO trial (Hamrah et al., 2024) was a phase IV, open-label, uncontrolled study that evaluated cenegermin in patients with stage 1 NK and reported corneal epithelial healing in 84.8% at 8 weeks and sustained improvement in corneal sensitivity. 24 Although this trial lacked a vehicle comparator and therefore could not contribute to pooled efficacy estimation, it provides valuable evidence that cenegermin may also benefit patients at earlier disease stages. Similarly, Li et al. (2025) conducted a phase IV, open-label study in Chinese patients with stage 2 or 3 NK, reporting corneal healing in 84.6% at 8 weeks with a durable effect maintained in over 90% of responders at week 56. 25 This study extends the evidence base to an East Asian population and provides reassuring long-term follow-up data. In addition, Arboleda and Ta (2022) reported encouraging results with cenegermin in a small prospective cohort of patients with limbal stem cell deficiency associated with NK, observing significant improvement in corneal epithelium and sensitivity. 26 While these studies are observational and cannot establish comparative efficacy, they complement the RCT evidence by suggesting broader applicability and consistent therapeutic benefits across diverse clinical settings.
The methodological rigor of this review merits comment. Both included trials employed double-masked, vehicle-controlled designs with identical intervention protocols (cenegermin 20 mcg/mL, six times daily for 8 weeks) and outcome definitions, which facilitated valid pooling. The primary endpoint of complete corneal healing was assessed objectively through fluorescein staining by masked examiners, reducing the potential for detection bias. Fixed-effect and random-effects models yielded identical pooled estimates, further confirming the stability of the results.
Nevertheless, several limitations must be considered when interpreting these findings. First, the quantitative synthesis is based on only two RCTs enrolling a combined total of 148 patients. Although meta-analysis of two studies is methodologically permissible and provides a summary of the best available evidence, the statistical precision of pooled estimates is inherently constrained, and the generalizability of findings to populations beyond those studied (predominantly White, mean age approximately 63 years) remains uncertain. Second, both included trials were sponsored by the same manufacturer (Dompe Farmaceutici), which introduces a potential sponsorship bias. Although the study designs were rigorous and outcome assessment was performed by masked investigators, it is well documented in the methodological literature that industry-funded trials tend to report outcomes more favorable to the sponsor’s product. 27 We have accounted for this concern in our GRADE assessment by downgrading for risk of bias. Third, the primary endpoint was assessed at 8 weeks. While this timeframe is clinically meaningful for evaluating epithelial closure, it does not address the long-term durability of the healing response, the potential for disease recurrence after treatment discontinuation, or the sustained impact on visual outcomes. Fourth, heterogeneity and publication bias could not be adequately assessed given the small number of included studies: the I-squared value of 0% has limited interpretive value with only two data points, and funnel plot analysis or formal tests such as the Egger regression require substantially more studies to be informative.20,22
Future research should prioritize independently funded, multicenter RCTs with larger sample sizes and extended follow-up periods that capture long-term corneal integrity, visual acuity trajectories, disease recurrence rates, and cost-effectiveness. Head-to-head trials comparing cenegermin with other emerging therapies such as topical insulin or autologous serum therapy would be particularly informative for establishing an evidence-based treatment algorithm. Additionally, confirmatory RCTs in stage 1 NK, building on the preliminary findings of the DEFENDO trial, 24 and in geographically and ethnically diverse populations are needed to define the full scope of cenegermin’s clinical utility.
Conclusion
This systematic review and meta-analysis demonstrate that cenegermin is an effective and well-tolerated disease-modifying therapy for moderate to severe NK. It nearly doubles the probability of complete corneal healing at 8 weeks compared with vehicle, with a clinically meaningful NNT of three and no significant increase in adverse events. The certainty of evidence was rated as moderate under the GRADE framework. While these findings are consistent and statistically robust, they are derived from only two industry-sponsored RCTs with a combined population of 148 patients. Therefore, cenegermin should be regarded as an important addition to the therapeutic armamentarium for NK, but larger, independently funded trials with longer follow-up are needed to establish its definitive position within the treatment algorithm for this rare and debilitating corneal disease.
Supplemental Material
sj-docx-1-oed-10.1177_25158414261460347 – Supplemental material for Therapeutic efficacy of cenegermin in the management of neurotrophic keratitis: a systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-1-oed-10.1177_25158414261460347 for Therapeutic efficacy of cenegermin in the management of neurotrophic keratitis: a systematic review and meta-analysis of randomized controlled trials by Zainudheen Faroog, Abdul Rehman Zia Zaidi and Sehar Tejani in Therapeutic Advances in Ophthalmology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.