
Abstract
Background:
Dry age-related macular degeneration currently lacks effective treatments for geographic atrophy. Cord blood platelet–rich (CB-PRP) plasma intravitreal injections are a novel therapy under investigation with promising ad interim results.
Objectives:
To describe the safety profile of cord blood platelet–rich plasma intravitreal injections (IVIs) in dry age-related macular degeneration (AMD) patients.
Design:
This prospective, randomized, sham-controlled, open-label experimental trial evaluated the safety of repeated intravitreal CB-PRP injections.
Methods:
The study, conducted from January 2023 to January 2025, investigated the safety and efficacy of CB-PRP IVIs to slow down the progression of geographic atrophy (GA). One eye of each patient was randomly assigned to the monthly, every other month, or every 3 months arm and received 0.05 mL CB-PRP, while the other eye underwent only a sham injection. Complete ophthalmological evaluations were performed at baseline, 3-, 6-, 12-, 18-, and 24-month follow-ups. In addition, slit-lamp and fundus examinations were performed the day after the injection to exclude any adverse effect.
Results:
In a total of 328 intravitreal injections, vitreous opacities were observed in the absence of other signs of infection or inflammation only in three cases. All of them showed progressive improvement without treatment, and complete recovery was observed within 2 weeks.
Conclusion:
Although the pathogenesis of the detected vitreous thickening was not completely clear, the most likely hypothesis was the coexistence of a slightly lower temperature of the CB-PRP sample and individual factors. This mild adverse event occurred only once in each patient involved, with no recurrence during subsequent intravitreal injections. The occurrence of this self-limiting finding after CB-PRP IVIs has not invalidated the safety profile of the procedure.
Keywords
Introduction
Age-related macular degeneration (AMD) is the principal cause of central vision loss in developed countries in patients older than 60 years, with the future forecast of significant increase in incidence worldwide. 1 Although the non-neovascular subtype (NNAMD), also known as dry AMD, is the most common, an adequate treatment to prevent or to slow down the progression to the end stage of the disease, the geographic atrophy (GA), is still not available. Recently, novel understanding of AMD pathogenesis has led to the development of new drugs, which act against the C3 and C5 factors of the complement system and reduce the atrophic growth of 20%.2–4 However, these molecules have not been approved by EMA in 2024, and the disease still lacks a reliable treatment.
Our group has given particular attention to the potential role of cord blood platelet–rich plasma (CB-PRP) in managing this condition. Rizzo et al. reported a mean gain of 5 ETDRS letters after 6 months and 2 letters after 12 months in dry AMD patients, who underwent subretinal injection of CB-PRP. 5 Furthermore, Savastano et al. evaluated a new therapeutic protocol based on intravitreal injections of CB-PRP, to assess the safety and the efficacy of repeated administrations. The primary outcome was overall satisfied, since no significant side effects were registered along 1 year of treatment. A longer follow-up, as well as a greater sample size with the ongoing project, will likely allow for the exclusion of even late adverse events. Moreover, we demonstrated that the annualized growth rate of GA, evaluated by enface optical coherence tomography (OCT), in the treated group was 14.5% smaller than in the sham arm. 6
The aim of this study was to report the safety profile of CB-PRP IVIs, describing a transitory, mild, and self-limiting finding that we observed in a small cohort of patients.
Materials and methods
The study, conducted at the Fondazione Policlinico Universitario Agostino Gemelli IRCCS, Rome, Italy, between January 2023 and January 2025, included patients over 65 years old, diagnosed with bilateral GA and best-corrected visual acuity (BCVA) between 35 and 65 ETDRS letters. The study employed a blinded, randomized, controlled, open-label, prospective, and non-profit experimental design. Ethical approval was granted by the Ethical Committee of the Fondazione Policlinico Universitario Agostino Gemelli IRCCS (ID number: 4995), and the study was registered on clinicaltrials.gov (NCT05706896). Written informed consent was obtained from each patient. The study was conducted in accordance with the 1976 Declaration of Helsinki and its later amendments. 7
Exclusion criteria included the presence of systemic or other ocular diseases in both eyes, such as glaucoma, amblyopia, diabetic retinopathy, uveitis, and a history of exudative or nonexudative macular neovascularization (MNV), and the presence of any significant optic media opacity that could influence the quality of images.
One eye of each patient was randomly assigned to one of the three treatment arms: monthly, every other month (2-month interval between injections), or every 3 months, and received intravitreal injections of 0.05 mL CB-PRP. The fellow eye underwent only a sham injection. The eye with lower BCVA was injected. If visual acuity was the same, the eye to treat was chosen by randomization.
Patients underwent a comprehensive ophthalmological evaluation at baseline and at 3-, 6-, 12-, 18-, and 24-month follow-up, including BCVA assessment, slit-lamp examination, intraocular pressure measurement, dilated fundus examination, color fundus retinography (CFP), fundus autofluorescence (FAF), spectral-domain OCT (SD-OCT), enface OCT, and OCT angiography (OCTA).
The day after the injection, patients were scheduled for slit-lamp and dilated fundus examination to exclude potential side effects. If necessary, further imaging exams were performed.
Results
A total of 23 patients (46 eyes) were enrolled in the study. Twenty-three eyes underwent CB-PRP injections, and 23 received only the sham injection. Seven eyes were included in the monthly group, eight eyes in the every other month group, and eight eyes in the every-3-month subgroup. A total of 328 injections have been performed during the study, in particular 168 in the monthly group, 96 in the every other month group, and 64 in the every-3-month subgroup. Only 3 patients out of 23, throughout the study period, had mild complaints after the injection. The remaining 20 patients (43 eyes) did not experience any adverse event. In 3 out of 328 total injections, white vitreous opacities were observed at the fundus evaluation the day after the injection, with no signs of infection or inflammation, retinal detachment, vitreoretinal traction, or other vitreoretinal abnormalities. In all three cases, the anterior segment was silent, and the intraocular pressure was within normal limits. No pain was referred. In two patients, symptoms were referred after the first IVI, while in the third case, after the fifth IVI. In view of the absence of other critical signs, a close follow-up was scheduled at 3 days, 1 week, and 2 weeks after injection. In all cases, progressive improvement in the symptomatology as well as in the clinical sign was reported, until complete resolution of vitreous opacities within 2 weeks.
Other milder reported events were conjunctival hyperemia in four patients and subconjunctival hemorrhage in three patients, without any other signs of inflammation, and were considered likely related to the procedure of intravitreal injection and not to the CB-PRP.
Case 1
The first patient was a 66-year-old man, recruited in the monthly arm, who reported the onset of new symptoms in the left eye (LE) after the fifth intravitreal injection of CB-PRP, performed in accordance with the CORD-IV protocol. At the follow-up visit performed the day after injection, the patient complained of a dark spot in his visual field and visual acuity impairment. No pain was reported. BCVA of the LE was decreased from 30 ETDRS letters to counting fingers at 30 cm. The anterior segment showed slight conjunctival hyperemia, no corneal edema, an optically empty anterior chamber, and no signs of infection. The IOP was 18 mmHg. At fundus examination, a whitish vitreous floater was observed in the inferotemporal sector, close to the injection site (Figure 1(a)). There were no signs of infection, neither in the vitreous nor in the choroid or retina, nor evidence of vitreoretinal traction or retinal breaks. Infection or inflammation was excluded considering the absence of pain, corneal edema, endothelial precipitates, hypopyon, anterior chamber, and vitreous cellularity.
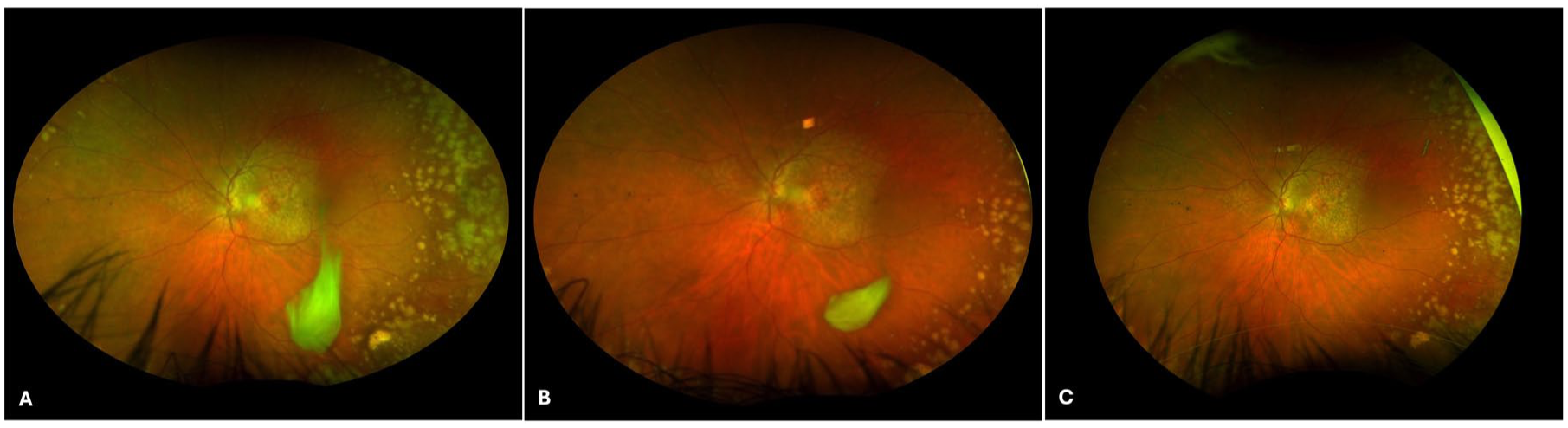
Ultra-wide-field CFP of the first case. (a) Ultra-wide-field CFP performed the day after the fifth injection of CB-PRP in the LE showed GA, peripheral drusen, and vitreous float in the inferotemporal sector close to the injection site. (b) Ultra-wide-field CFP 3 days after the injection showed a significant decrease in the vitreous float size. (c) Ultra-wide-field CFP showed complete reabsorption of the vitreous thickening at 2 weeks of follow-up.
Therefore, maintaining adequate hydration was suggested, and a new follow-up was scheduled. Three days after the injection, a new check was performed, reporting improvement in symptoms and signs. The anterior segment remained silent, and the vitreous floater had reduced in size (Figure 1(b)). At 2 weeks of follow-up, BCVA was restored to 30 letters ETDRS, the vitreous floater was completely reabsorbed, and symptoms were no longer reported (Figure 1(c)).
Case 2
A 76-year-old female patient, recruited in the quarterly group, reported the onset of symptoms after the first intravitreal injection of CB-PRP in the right eye (RE). In this case, the patient did not experience a decrease in vision, maintaining her BCVA of 32 ETDRS letters, but she complained about floaters.
There was no conjunctival hyperemia, corneal edema, anterior chamber abnormalities, or IOP rise. At fundus evaluation, the vitreous opacities were the only abnormalities found, and no retinal breaks, traction, or signs of infection were observed (Figure 2(a)). Adequate hydration was recommended with a close follow-up. Improvement of symptoms was reported during visits, and 2 weeks after the injection, the vitreous opacities were completely resolved (Figure 2(b)).
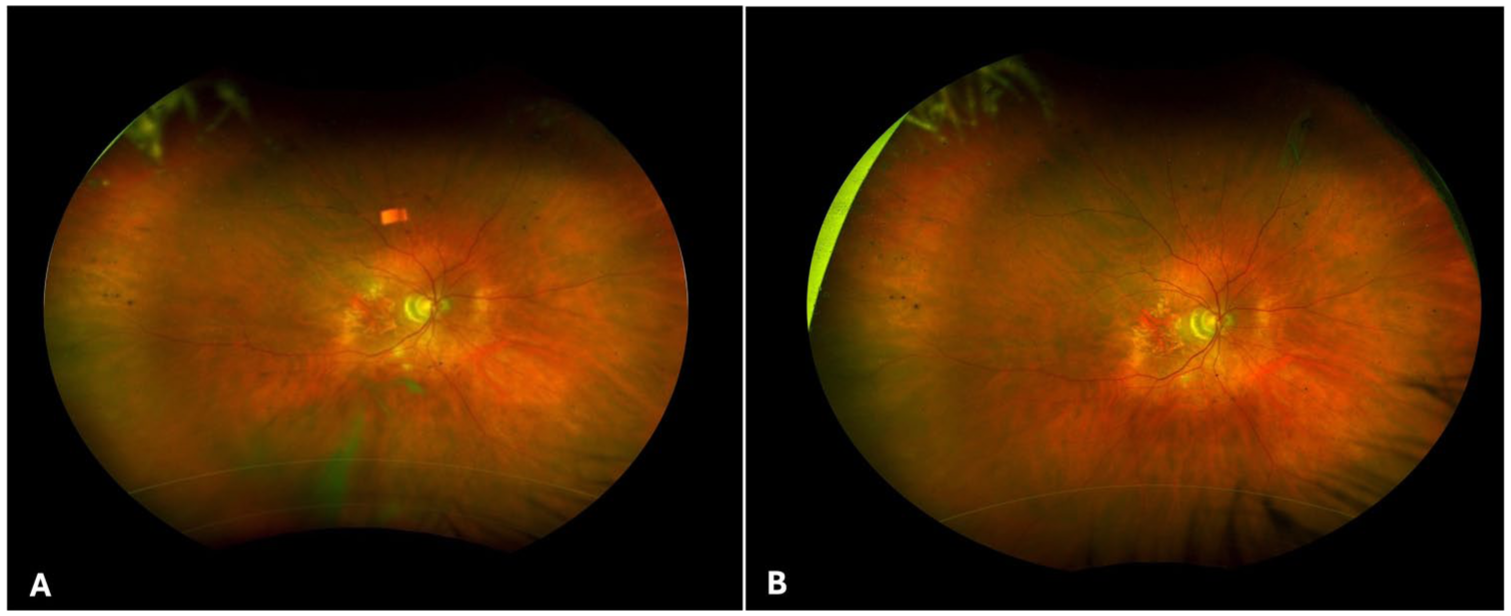
Ultra-wide-field CPF of the second case: (A) The CFP, performed the first day after the first intravitreal injection of CB-PRP, showed GA, normal optic disk and vascular architecture, vitreous opacities in the inferior sector, and no retinal breaks or traction. (B) Ultra-wide-field CFP showed complete reabsorption of the vitreous thickening after 2 weeks.
Case 3
The third case was observed in an 86-year-old male patient after the first CB-PRP intravitreal injection in RE of his monthly regimen. During the scheduled follow-up the day after injection, he complained of a dark spot in the superior quadrant of his visual field, but not about vision impairment. His BCVA was stable at 31 ETDRS letters. The anterior segment was normal, with only a slight subconjunctival hemorrhage in correspondence with the injection site, but clear cornea, normal anterior chamber, and IOP. The fundoscopy showed a big vitreous opacity in the inferotemporal sector, associated with other little ones at the posterior pole, but no retinal breaks, traction, or signs of infection (Figure 3(a)).
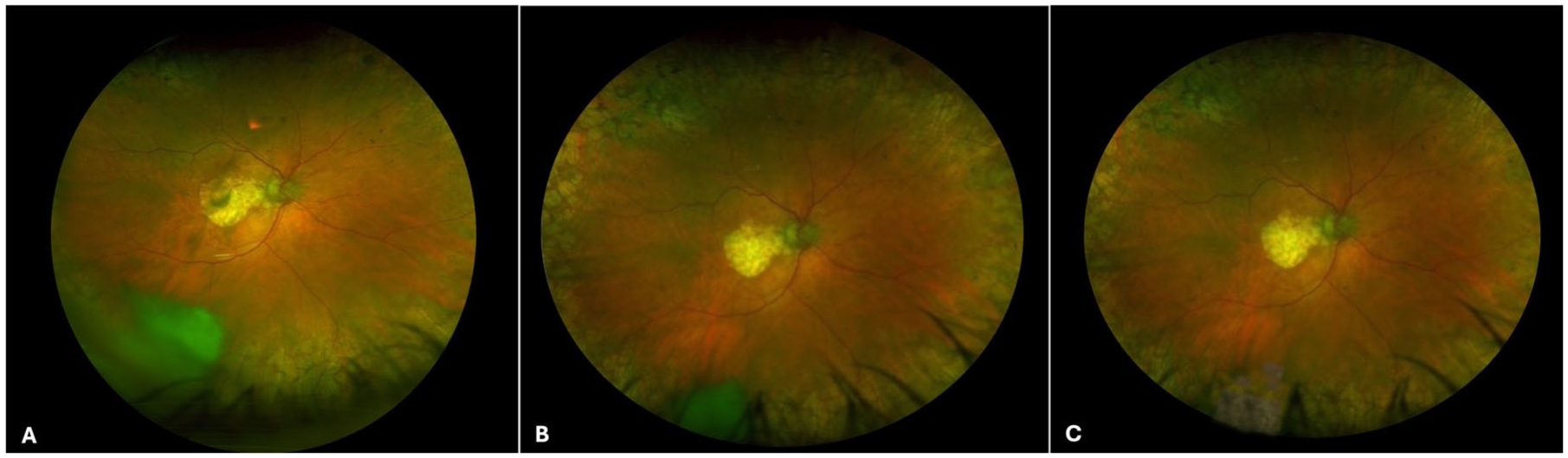
Ultra-wide-field CFP of the third patient. (a) Ultra-wide-field CFP, performed the day after intravitreal injection of CB-PRP, showed geographic atrophy, normal vascular architecture and optic disk, paving stone degenerations on 360°, vitreous thickening in the inferotemporal sector, and some smaller vitreous opacities at the posterior pole. (b) One week after injection, the inferotemporal vitreous opacity was significantly decreased in size, and the central ones were reabsorbed. (c) CFP at 2 weeks of follow-up showed complete reabsorption of the vitreous opacity.
We recommended adequate hydration and follow-up. One week later, at fundus examination, it was possible to appreciate a significant decrease in vitreous thickening size and reabsorption of central vitreous opacities (Figure 3(b)). After 2 weeks, no symptoms were reported, and the inferior vitreous thickening was completely resolved (Figure 3(c)).
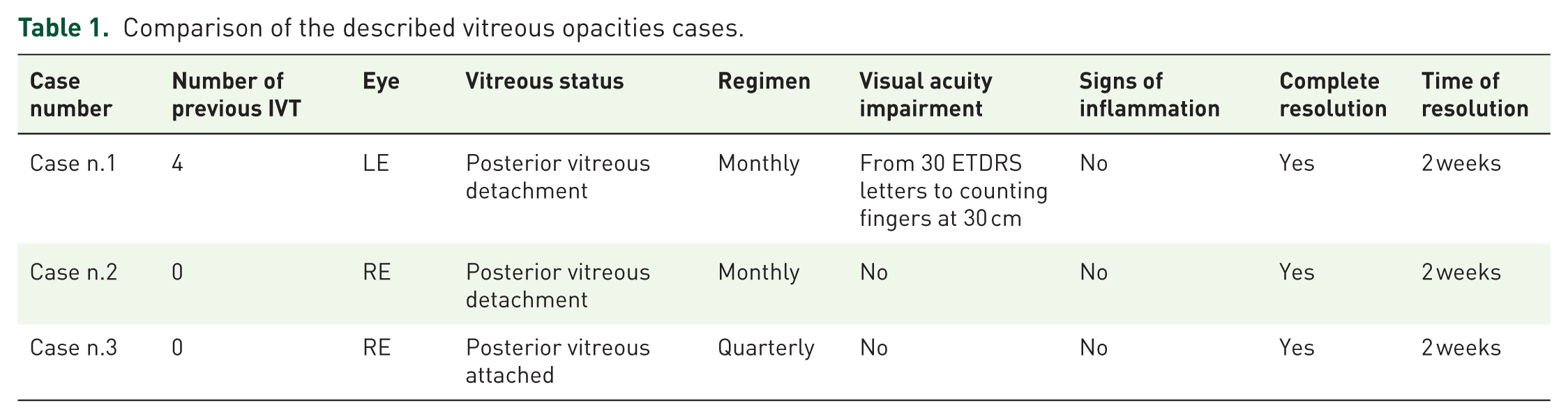
Table 1 shows a comparison of the vitreous opacities found in the three cases.
Comparison of the described vitreous opacities cases.
Discussion
Nowadays, intravitreal injections represent the main approach to treat several retinal diseases, such as exudative AMD, diabetic retinopathy, and vascular occlusions. The major concern related to the procedure is the risk of endophthalmitis, followed by lens damage and retinal detachment.
Cases of vitreitis without signs of infection were reported after intravitreal injections of different drugs, including bevacizumab, ranibizumab, and aflibercept. In the reported case series, a decrease in visual acuity was reported in association with ocular pain. 8
In our CB-PRP experience, only one patient reported impairment in visual acuity, while pain was always absent. Furthermore, the vitreous condensation was located in the inferior sector, while, as reported in scientific literature, non-infectious vitreous inflammation was typically diffuse. In addition, in our patients, no signs of inflammation were observed in either the anterior segment or the posterior one. These findings may be supportive of excluding an inflammatory reaction in the three reported cases, which moreover resolved spontaneously in 2 weeks.
However, from a pathogenetic point of view, the origin of the vitreous thickening in our sample was not entirely clear.
The protocol followed to prepare the CB-PRP units had not been modified during the study, as confirmed by the blood transfusion center. At the same time, the injection procedure has not been changed. It was usually performed by expert ophthalmologists, choosing the infero-temporal quadrant for the injection at 3.5 mm from limbus in pseudophakic eyes and at 4 mm in phakic ones. 9
In view of the high number of injections performed during the study (328 IVIs) and the detection of only three cases of vitreous opacities, it could be supposed that particular conditions of the injected units played a significant role in the onset of these events. One of the most likely hypotheses was represented by a slightly lower temperature of the CB-PRP unit than other cases, which may have favored the condensation of the material once injected into the vitreous chamber.
The contemporary presence of unknown individual co-factors may have exerted an influence, although other similar events were no longer reported in the same three patients.
Furthermore, we were confident to exclude a previous sensitivity since, in two out of three patients, signs and symptoms occurred after the first injection. Therefore, even an immune reaction could be unlikely to be responsible.
After the detection of these findings, a slight modification was made to the procedure, consisting of thawing the CB-PRP sample 45 min before the injection time instead of 30 min. Since the protocol change, we performed 212 injections, and we did not observe other similar cases, suggesting that the lower temperature of the units may have played a crucial role in the onset of vitreous opacities.
The study had some limitations. The main one was represented by the small sample size, although the number of performed injections was significantly high. Recently, the Ministry of Health has awarded a grant according to the National Recovery and Resilience Plan (PNRR-MCNT2-2023-12377045) for this project that included two other study centers, enabling us to enlarge the number of included patients. Another limit was the relatively short follow-up, which may not allow for the definitive exclusion of late onset side effects. Thus, the enrolled patients will continue to be examined for the following year after the end of the study.
In conclusion, we reported temporary and completely self-limiting events after CB-PRP intravitreal injections, which have not invalidated the safety profile of the procedure. Quite the opposite: in view of the high number of performed injections, we could consider the CB-PRP IVIs a safe procedure.
Supplemental Material
sj-pdf-1-oed-10.1177_25158414261462410 – Supplemental material for Transitory vitreous opacities after CB-PRP intravitreal injections in dry AMD patients
Supplemental material, sj-pdf-1-oed-10.1177_25158414261462410 for Transitory vitreous opacities after CB-PRP intravitreal injections in dry AMD patients by Claudia Fossataro, Maria Cristina Savastano, Mattia Cusato, Valentina Cestrone, Francesco Mottola, Lorenzo Hu, Giorgia Campaniello, Gianmarco Oreste, Federico Giannuzzi, Emanuele Maiola, Giulia Mastropietro, Alfonso Savastano, Caterina Giovanna Valentini, Claudio Pellegrino, Luciana Teofili and Stanislao Rizzo in Therapeutic Advances in Ophthalmology
Footnotes
Acknowledgements
Rafforzamento e potenziamento della ricerca biomedica del SSN, finanziato dall’Unione Europea – NextGeneration EU – CODICE PROGETTO: PNRR-MCNT2-2023-12377045; CUP: C53C23001160007. The authors would like to thank Università Cattolica del Sacro Cuore for publication support.
Author Note
All authors attest that they meet the current ICMJE criteria for Authorship.
Declarations
Supplemental material
Supplemental material for this article is available online upon reasonable request to the author.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.