
Abstract
Background
The use of medical technology may result in damage to patients. The aim was to determine which adverse events and adverse incidents related to medical–surgical devices were most frequently observed in patients seen at 65 health service providers, clinics and hospitals in Colombia.
Methods
Retrospective study describing reports of adverse events or incidents related to medical devices between 2014 and 2017. From the database of reports, all cases were identified and classified by the type of device, causes and time of identification of the event.
Results
The devices that were most frequently reported as having events or adverse incidents were those belonging to the vascular access category, with 45.2% of cases, followed by surgical equipment, with 20.2%. The causes of the events or adverse incidents were most often failures of the mechanical components, at 50.6%, followed by manufacturing defects, at 28.7%. The professionals who reported these issues most frequently were nurses, who did so in 33.1% of the cases. A total of 86.8% of the reports were non-serious adverse events, and the failure was identified at the time of device use in 72.8% of the cases.
Conclusions
Preventive approaches to events and adverse events related to medical devices can mostly be resolved through stricter quality control measures.
Introduction
Medical care today commonly involves the use of multiple medical technologies; however, the use of these products may result in some harm to patients.1,2 Despite this, the use of these technologies is crucial to the entire health care process, and the advances made positively impact the quality of life of patients and contribute to the development of society. 3 The design of medical devices must be done taking into account the ergonomics of health professionals, including the ethnographic differences that may exist. Proper design can reduce problems related to human factors. 4
Worldwide, approximately 4% to 17% of hospital admissions are associated with an adverse event (AE).2,5 One study in Latin America estimated that 10.5% of patients have AEs related to health care and that 60% of these are preventable. 6 Technosurveillance seeks to objectively determine the presentation of AEs or incidents resulting from the use of medical devices and is responsible for their identification, notification and implementation of preventive actions. 7 In Colombia, there is a Technosurveillance program led by the National Institute for Food and Drug Surveillance (Instituto Nacional de Vigilancia de Medicamentos y Alimentos, INVIMA), which establishes regulations for the use of medical devices and notifications of AEs. 8 AEs involve unintentional harm to patients or device operators, while adverse incidents (AIs) refer to potential harm. 9
In a study conducted in three hospitals in Colombia, a proportion of AEs of 7.9% was found, and those attributed to medical equipment or supplies accounted for 16% of them. 10 Another study in the country found that 22.8% of AEs were related to medical devices. 11 In some investigations, the causes of failures of equipment and devices have been attributed to different phenomena, including quality problems in manufacturing, incorrect use of the devices, clinical conditions of the patients, poor techniques, deterioration of the functions of the devices, among others.11,12
Given that this is a relatively new discipline and there is little information on the subject, it was established as objective to determine which AEs and AIs related to medical–surgical devices were most frequently observed in patients seen at 65 health service providers, clinics and hospitals in Colombia.
Methods
A retrospective study was carried out using all AE and AI reports related to medical devices from January 2014 to June 2017 in 24 cities in Colombia. This study utilized the database generated by the Audifarma Technosurveillance program, which is run by the largest company in the country that dispenses medicines, supplies medical devices to different clinics and hospitals, amounting to coverage of approximately 5800 patient beds.
All AE and AI cases recorded in the database of Technosurveillance program were collected; this included all the reports made by health personnel (pharmaceutical chemist, nurses, physicians, etc.) at the 65 health institutions to which Audifarma dispenses, supplies medical devices during the study period. The following variables were taken into account: Related to the AE or AI: initial diagnosis and harm caused; profession of the person making the report; description and classification of the event during which the product failure was detected: before, during or after using it; outcome; probable causes according to the norms established for Colombia; and corrective or preventive actions initiated.
8
Related to the institution: level of attention according to the complexity: from first to fourth. Related to the device: name, manufacturer, lot and model of the product.
The data were recorded in an Excel database for later analysis in the SPSS statistical package, version 24.0, for Windows (IBM, USA). Descriptive statistics used were averages, standard deviations, and minimum and maximum values for continuous variables and percentages for categorical variables.
This study was endorsed by the Bioethics Committee of the Universidad Tecnológica de Pereira in the category of “risk-free research”; personal data from patients were not used and the ethical principles established by the Helsinki Declaration were respected.
Results
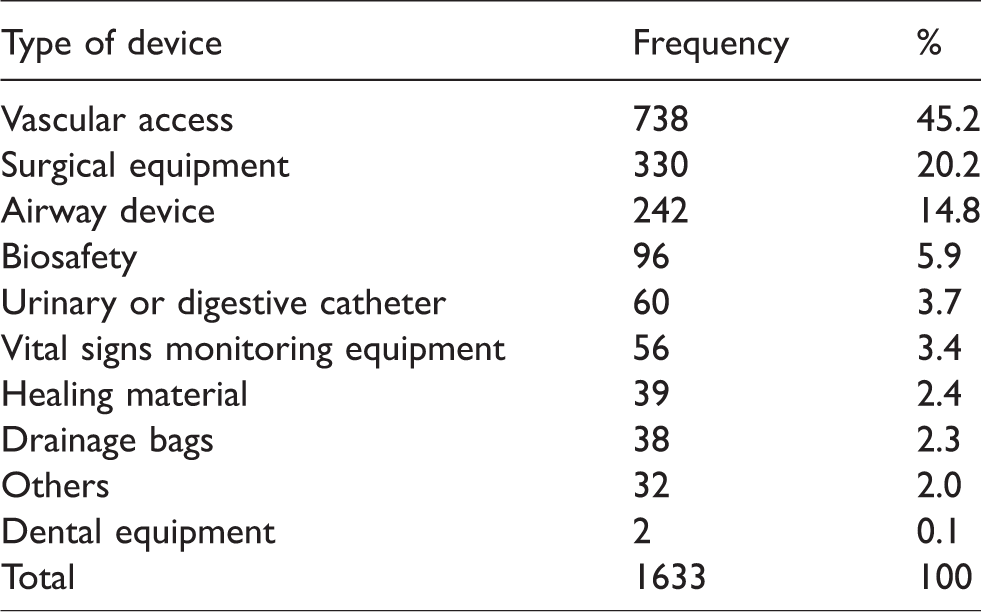
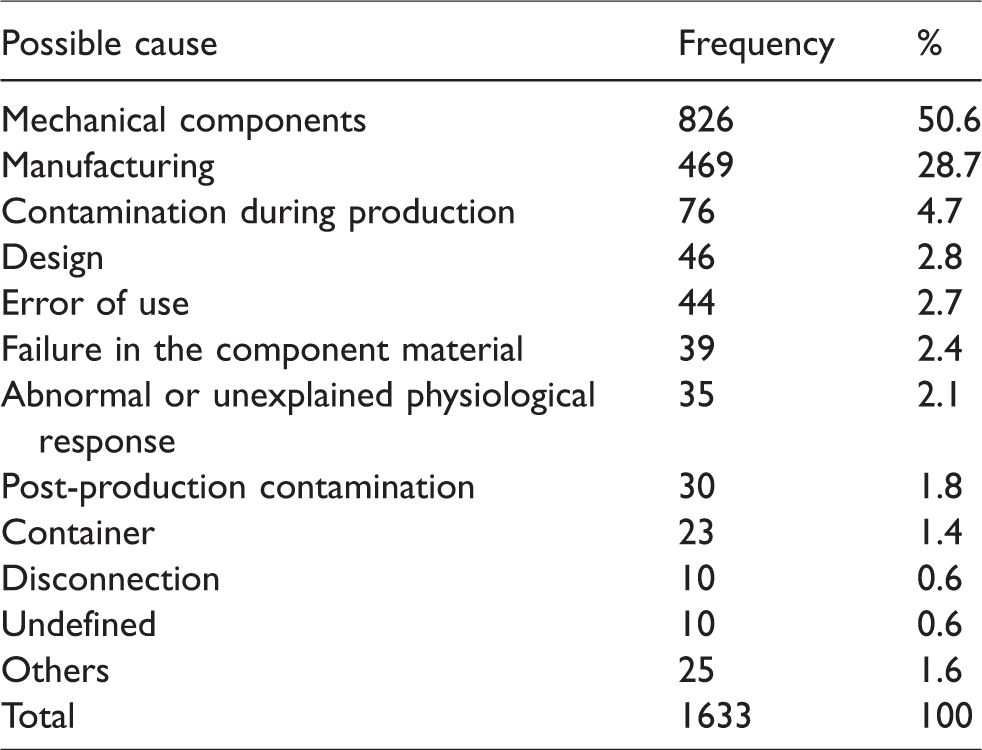
We identified 1633 (AE, n = 175, 10,7% and AI, n = 1458, 89,3%) reports in 65 health institutions in Colombia in the 42-month follow-up period. Devices for vascular access, surgical equipment and airway access were the ones most often involved in these types of events. The categories for medical devices can be seen in Table 1. Failures of mechanical components, manufacturing defects and contamination of the elements were the most common causes of AEs and AIs (see Table 2).
Categories of medical devices involved in adverse events or incidents related to medical devices in Colombia, 2014–2017.
Possible causes of adverse events or incidents related to medical devices in Colombia, 2014–2017.
In 2014, 449 AEs and AIs were reported (27.5% of the total reported, with an incidence of 3.66 AE/AI for every 1,000,000 devices delivered). In 2015, 488 were reported (29.9%, incidence of 3.38/1,000,000), and in 2016 there were 451 reports (27.6%, incidence of 2.67/1,000,000). Finally, in 2017, another 245 (15.0%, incidence of 2.56/1,000,000) were reported.
A total of 74.0% (n = 1210) of the reports came from 30 tertiary care hospitals, 24.9% (n = 407) came from 10 secondary care centers and 1% (n = 16) were from 25 primary care centers. More specifically, the highest number of reports came from 53 hospitalization services units (n = 782, 47.9%) followed by 37 operating rooms (n = 385, 23.6%), 27 intensive care units (n = 261, 16, 0%), 29 emergency services departments (n = 163, 10.0%), 11 outpatient services departments (n = 24, 1.5%), two hemodialysis rooms (n = 13, 0.8%), three procedure rooms (n = 3, 0.2%) and sterilization and imaging rooms, which had one report each (n = 1, 0.1%).
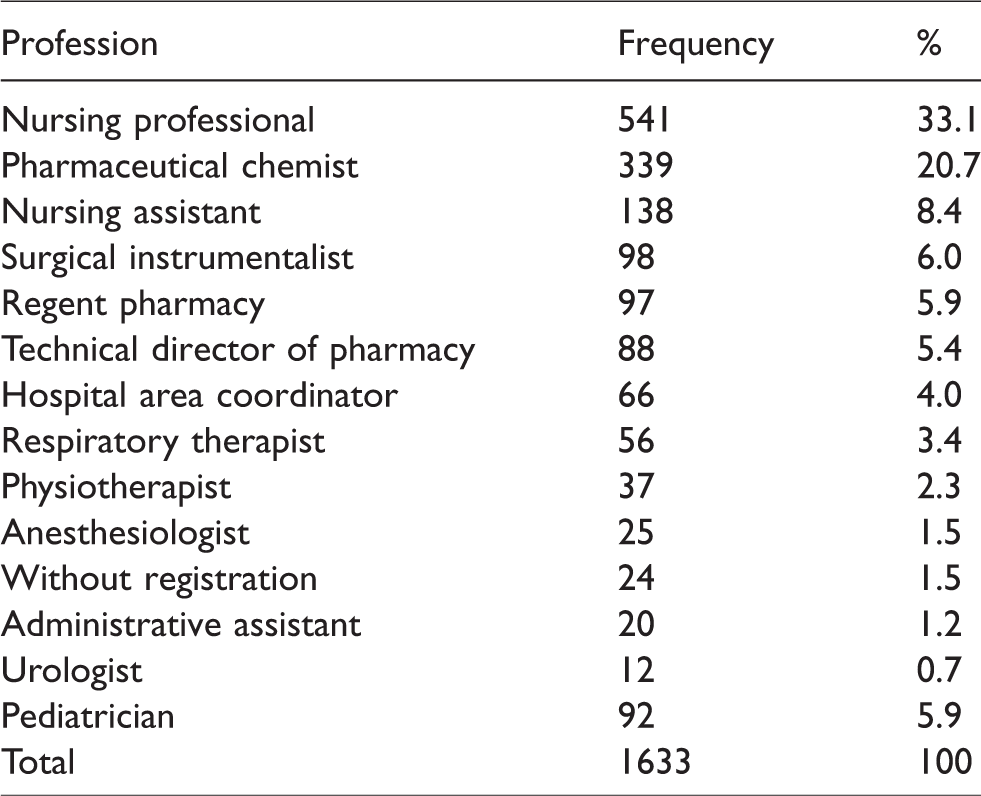
Nurses reported more AEs and AIs than other professionals followed by pharmaceutical chemists and nurse assistants (see Table 3). Most of the cases were identified during the procedures (n = 1189, 72.8%), but 26.9% (n = 439) were identified before the procedures, and finally a few after the use (n = 5, 0.3%).
Percentages of adverse events or incidents related to distributed medical devices in Colombia according to the professionals who made the report, 2014–2017.
There was no harm to patients in 98.8% (n = 1614) of the reports, while in five cases (0.3% of the AEs), medical or surgical intervention was required; of which one patient needed a new prosthetic valve, another required additional suturing, another had a femur block plate replaced, another required removal of an epicutaneous catheter that broke and one had gingival bleeding that needed to be stopped. In two other cases (0.1%) in which a visible lesion was present, healing was achieved with improvement observed over time. Other outcomes found included desaturation, desaturation with sustained hypotension and bradycardia, hemodynamic and respiratory instability due to loss of the airway, phlebitis, pneumothorax, multiple punctures and nasal bleeding; for each of the cases, n = 8 (0.5%).
The corrective and preventive actions carried out after the AE or AI related to the medical devices were: (1) technical support and device review (n = 644, 39.4%); (2) provide recommendations for not using devices in case of visible damage of the package (n = 506, 31.1%); (3) training and personnel training (n = 300, 18.3%); (4) sent a no conformity to the manufacturer (n = 69, 4.2%); (5) Device review, quality filter increase and tracking (n = 56, 3.4%); (6) lot removal and follow-up (n = 20, 1.2%) and (7) replacement of reported units and technical support (n = 14, 0.9%).
Discussion
The identification of the highest number of AE and AI reports in the country was achieved in a large portion of health clinics and hospitals. Reports of AEs and AIs related to medical devices have increased in recent years with the advent of new technologies for health care and the development of Technosurveillance programs. 1
Several studies have shown that vascular access is widely used in hospitalized patients, but its use is associated with various complications, which can occur in 39.1% of patients.13,14 In a study conducted in Mexico, the main AEs were those related to patient care (n = 188, 34.8%) followed by drug effects (n = 113, 20.9%) and those related to vascular administration and access (n = 84, 15.6%); similarly other studies have reported a wide range of AEs related to vascular access as well, including phlebitis and thrombosis.15,16 In addition, it has been shown that vascular access is a risk factor for the development of infections. 17 It is important to highlight, despite the evidence, that phlebitis was only reported in one case, which may be related to device failure but not to the venous access procedure. Possibly many AEs could be prevented if in patients who do not require vascular access, their use is avoided and the medications will not be administered intravenously when there are oral alternatives with similar bioavailability.
A study carried out in Taiwan found that the defects in the most common devices were fluid leaks (12.7% of cases) and the presence of foreign material inside the devices (12.4%). This was in contrast to this report, which identified component failures (50.6%) as the first cause followed by manufacturing defects (28.7%), a situation that compromises the quality of the products and requires a review of manufacturing processes. 12 Both manufacturers and personnel who use surgical devices should ensure the quality of the products and the timely identification of quality problems.
A study carried out in Mexico showed that the location where most AEs and AIs were reported was in surgery (51.0%), while in this study, reports related to hospitalization services (47.9%) predominated, which is related to the types of institutions included, their care levels, numbers of beds and the reasons that led to the patient needing care in the health institution. 18 Many of the differences may be due to the health conditions of each region, the type of morbidities and even the traffic accident rates.
It is striking that the vast majority of reports were made by nursing staff and pharmaceutical chemists, while only a small number were made by physicians, which is in agreement with the findings of another study conducted in Australia. 19 It has already been established that professionals who avoid carrying out AE and AI reports do so for cultural reasons or because they consider them unnecessary or useless, and they should be the target of educational activities aimed at encouraging this activity.20,21 Emphasis should be placed on the education of physicians and nurses on the importance of reporting all AI and AE, since it can help reduce the problems associated with its use and can create a culture of reporting.
The identification of the AEs and AIs occurred mostly at the time of the procedures (n = 1189, 72.8%), which suggests that the situations associated with cases of Technosurveillance, both those that have to do with the use of the device as well as those related to factors in the manufacturing process, distribution and enlistment, can be identified only after the medical device is removed from the primary packaging and its use is attempted. Regarding the cases associated with the use of the devices, it is worth noting that a lack of adherence to patient safety protocols has been found in studies, where general safety guidelines are only followed in 31% of cases, 22 or devices have been reused 23 or have been misused. 24
The corrective and preventive actions implemented after the identification of the most representative cases of Technosurveillance are the use of technical support and reviews of the devices by the manufacturers, as well as providing necessary advice so that staff are trained in the correct use of devices and identification of the possible damage that AIs and AEs can generate. 25 Medical and surgical devices should be designed according to the ergonomics of health professionals from different regions of the world using ethnographic field research and the regulatory agencies of each country should keep vigil that the necessary adaptations are made to ensure the safety of the patients. 26 A study conducted in Colombia proposed different strategies that can contribute to reducing AIs and AEs related to the manipulation and maintenance of medical devices, 11 the implementation of such strategies can help explain the reduction in the incidence of AE/AI throughout the follow-up. Some recommendations that may be useful to reduce AEs and IAs include to reevaluate the performance and competencies of maintenance service providers, to require device providers to use simulators to demonstrate the perfect operating conditions and improve communication between the doctor and the patient during the presurgical evaluation. 11 There should be stricter quality controls and health authorities would have to monitor their compliance by verifying in the industries that manufacture the medical devices or in the plants of those who import and market them.
This work presents some limitations, such as the lack of review of the clinical history of each patient involved and its observational nature, which is subject to the reports made, rather than it being an active search for AEs and AIs. Nor is there certainty in some cases if the AE or AI was due to mechanical failure or misuse of the device. It is also a record of spontaneous reports, so there may be some underreporting. Although we believe that professionals knew how to use surgical devices, we do not know the level of training they had on their use, so it is possible that some events are also due to misuse. The results show an overview of the AE and AI presented in these health institutions, but cannot be extrapolated to other population because population data are not available and also AE and AI were considered without being individualized. It also has some strengths, such as the rigor in the collection of information from the reports made, the broad coverage of clinics and hospitals and the volume of AEs and AIs registered. Technovigilance reports are relatively new, and this is the largest AEs and AIs record in the country.
With the described findings, it can be concluded that the majority of AIs and AEs in this group of institutions occurred in hospitalization services, and the majority were related to devices such as syringes and peripheral catheters for vascular access followed by surgical equipment and airway management devices. The most common causes were failures in the mechanical components and manufacturing defects, they were most often reported by nurses and pharmacists, and after the problems occurred, technical support and reviews of the devices were pursued. It is necessary to carry out new studies that assess preventive and corrective measures for the appearance of these types of events, and educational strategies should be created that focus on promoting the submission of AE and AI reports by all participants in patient care. Preventive approaches to events and AEs related to medical devices can mostly be resolved through stricter quality control measures. The creation of post-marketing surveillance program for medical devices is essential. 25
Footnotes
Acknowledgements
The authors thank John Alexander López and Carlos Tovar for their support to obtain the database.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the Bioethics Committee of the Universidad Tecnologica de Pereira, Code: CBE-SYR-162016. Date: 9 October 2017.
Funding
The author(s) disclosed receipt of the following financial supportfor the research, authorship and/or publication of this article: This study received funding from the Universidad Tecnológica de Pereira (www.utp.edu.co) and Audifarma S.A. (![]() ).
).
Guarantor
JEMA.