
Abstract
Background
Although there is a demonstrated need for peer support programs for healthcare workers like Resilience In Stressful Events, little is known about their utilization. This study evaluated awareness and utilization of Resilience In Stressful Events among nurses at one teaching hospital; perceptions of program benefits; and resilience, burnout, and job satisfaction among Resilience In Stressful Events users versus non-users.
Methods
Cross-sectional surveys of staff nurses and nurse leaders. Pearson Chi-Square tests and logistic regressions were used to establish significant differences.
Results
There were 337 responses (response rate 8.3%) from staff nurses. Awareness of Resilience In Stressful Events was 87%, but there was limited Resilience In Stressful Events activation for oneself (23%) or others (6%). Among recent users (n = 30), 47% reported that Resilience In Stressful Events improved their ability to work with confidence, 65% felt better after using Resilience In Stressful Events, and 70% found the program helpful. Among non-users, 39% wished they had used Resilience In Stressful Events and 34% wished they had activated Resilience In Stressful Events on behalf of a colleague. Nurses who used Resilience In Stressful Events reported more burnout and greater resilience than those who had not, but similar job satisfaction. There were 75 responses from nurse leaders (response rate 69%), 93% of whom were aware of Resilience In Stressful Events; 56% had activated Resilience In Stressful Events. Eighty percent reported Resilience In Stressful Events was personally helpful and 68% reported the program was helpful for their staff. Nurse leaders who activated Resilience In Stressful Events were more resilient than those who had not, but similar in burnout and job satisfaction.
Conclusions
Nurses indicated favorable perceptions of using Resilience In Stressful Events, and its utilization was associated with greater resilience but higher burnout in frontline nurses.
Introduction
Nursing is the largest healthcare profession in the US, with more than 3.8 million registered nurses nationwide. 1 Nurses are at the heart of patient care, which can be a high-risk enterprise for both patients and clinicians. Nurses often encounter unanticipated patient events, poor outcomes, death, and other tragic situations in healthcare settings.2,3 As a result, some become emotionally or psychologically traumatized, becoming second victims of the same events. 4 However, after psychologically distressing events, with appropriate support nurses can also experience post-traumatic growth (PTG). PTG theory posits that the nurse absorbs the secondary trauma and draws purposeful meaning from it. 5
The Resilience In Stressful Events (RISE) program was established at the Johns Hopkins Hospital in 2011 to support all healthcare workers. RISE is designed to provide timely peer support to workers who encounter stressful patient-related events, including medical errors and adverse events, as well as the day-to-day stresses of providing care. Consistent with the theory of the wounded healer, the premise is that support from a trained colleague promotes the opportunity to experience emotional and psychological healing. 6 As a result, a nurse may experience enhanced personal resilience, restored job satisfaction, and reduced professional burnout.
Evidence suggests that organizational support structures can prevent, minimize, or relieve distress among healthcare workers. 7 Quillivan et al. 7 found a significant positive association of peer support with safety culture in units that encounter high levels of stress. The costs of RISE are relatively low as it is delivered by trained volunteers, and a program such as RISE can be associated with substantial potential cost savings to a healthcare organization. 8 Peer support for second victims is recognized as a priority by the Joint Commission, which named RISE as a leading practice model. 9
Despite the demonstrated benefit of peer support programs such as RISE, awareness of the program’s existence and utilization of the service among healthcare workers remain relatively low.10–12 Utilization of second victim support programs may eliminate or reduce symptoms that have an adverse impact on nurses, such as dissatisfaction and burnout. 13 A gap in existing knowledge is understanding the relationship of personal resilience, which interacts with both burnout and job satisfaction,14,15 with peer support program utilization. This study aimed to evaluate awareness and use of RISE, perceptions of program benefits, and association of program use with resilience, burnout, and job satisfaction among RISE users and non-users.
Methods
The design was a cross-sectional survey including fixed-response and open-ended items collected from a convenience sample of staff nurses and nurse leaders at one academic medical center in late 2018. In general, staff nurses represent the primary users of RISE support services, whereas nurse leaders are most likely to refer nurses for support (activate) the Program. Institutional Review Board approval was received from Johns Hopkins Medicine and the University of Alabama. Participants provided informed consent, and all surveys were anonymous.
Survey domain identification
The survey battery was assembled based on an in-depth content review of literature on the theory of nurse as wounded healer, PTG theory, and factors that impact the ability to grow after trauma. 5 Five-point Likert-type scales were used to elicit responses in the domains of interest: professional burnout, job satisfaction, and personal resilience. Five items on professional burnout were adapted from the Emotional Exhaustion domain of the Maslach Burnout Inventory General Survey 16 which was available to the institution under a license agreement. Three items related to job satisfaction that addressed enthusiasm, satisfaction, and enjoyment were utilized with minimal modification from previously validated questions. 17 Six questions from the validated Brief Resilience Scale 18 and two questions from the Second Victim Experience and Support Tool 10 assessed personal resilience. The survey also included six demographic questions. Six experts in the field of peer support evaluated the surveys for content validity.
The survey asked if a respondent was aware of the RISE program, had used RISE, and if so, when and in what format: in person or by phone, individually or with a group. Users of RISE were asked to assess potential benefits such as return to work with confidence after using RISE, helpfulness of RISE support, and feeling better after receiving support. Participants were also asked if they considered leaving their job, took time off as a result of a stressful event, and if RISE reduced their intention to leave their current job. Finally, the survey asked if participants had used other professional support resources. Non-users were asked if they wished to use RISE in the future for themselves or to refer their colleagues. The qualitative portion of the survey asked about perceived benefits of activating RISE and the reasons why nurses would not, or did not, use RISE.
Recruitment and participation
Two groups of participants were recruited from nurses employed by the Johns Hopkins Hospital during the project period: staff nurses (users) and nurse leaders (activators). Staff nurses comprised nurses who primarily do clinical work at the bedside starting from novice nurses, Nurse Clinician I (NCI), and those subsequently advancing in their career, Nurse Clinician IM (NCIM), Nurse Clinician IIM (NCIIM), Nurse Clinician IIE (NCIIE), and Nurse Clinician III (NCIII) based on the years of experience and clinical ladder promotion. Nurse leaders included nurse managers, assistant nurse managers, nurse educators, advanced practice nurses, nurse directors, and assistant directors.
Staff nurses
Approximately 4055 staff nurses were asked to participate via an email message sent to an electronic nursing distribution list. The invitation went to all nurses employed by the hospital and included a link to the QualtricsXM survey (Qualtrics©, Washington, DC). The electronically administered survey used skip logic designed to be filled out regardless of RISE awareness or utilization of RISE. Additionally, the invitation suggested nurses who completed the nurse leader survey at an earlier point in time to opt out. The survey period was the month of December 2018.
Nurse leaders
The nurse leader survey was administered during a monthly hospital Nurse Leader Forum meeting in October 2018. Three versions of the paper survey were distributed to 109 attendees based on their awareness and use of RISE: (1) I am aware of RISE and have used RISE, (2) I am aware of RISE and have not used RISE, and (3) I am not aware of RISE.
Statistical analysis
Domain scores were calculated as summated rating scales across multiple questions for professional burnout, job satisfaction, or personal resilience.
Pearson Chi-Square tests were used to determine statistical differences using Stata 15 (StataCorp. 2018. Stata Statistical Software: Release 15. College Station, TX: StataCorp LP). We used logistic regressions to calculate the direction and strength of those associations.
For qualitative data, content analysis was conducted by two independent reviewers who developed and compared codes and identified emergent themes. Responses to questions about perceived RISE benefits were described, but differences in question frequencies were not tested for statistical significance.
Results
Staff nurse results
The response rate from the staff nurse survey was 8.3% (337 of 4055). The average age of respondents was 40 years (range 21–83). Mean nurse tenure was 13.4 years (0.25–62). Sixty-seven percent reported nursing as their first career and 32% indicated nursing as a second career.
Among staff nurses, 87% (n = 274) were aware of RISE, and 19% (n = 63) had met with RISE. In addition, 13 had activated RISE for a colleague but not for themselves, and 12 both used RISE for themselves and activated for a colleague (Table 1). On average, staff nurse participants had used RISE 15.2 months prior to the survey distribution (0.1–60, SD = 18.4). Thirty-five percent of users had used RISE less than six months prior and 48% less than one year prior (n = 30). Of all who had met with RISE, 27% had considered leaving their job, and 22% felt that RISE reduced their thoughts about leaving their job. Eighty-four percent of participants who met with RISE did not subsequently take any time off from work due to the stressful event. Among staff nurse respondents who met with RISE, 4 were NCI, 15—NCIM, 18—NCIIM, 6—NCIIE, 15—NCIII, and 5 have not disclosed their stage in the clinical promotion ladder.
Awareness, use, and perceived benefits of RISE among staff nurses (N = 337 out of 4055 surveyed).
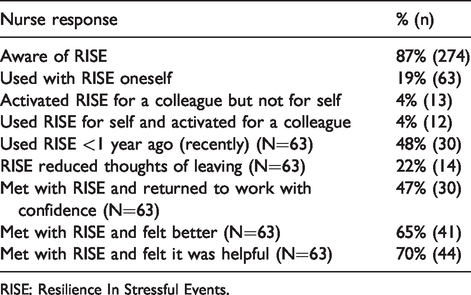
RISE: Resilience In Stressful Events.
Among those who had used RISE, 47% agreed or strongly agreed that RISE helped them return to work feeling confident in their ability to do their job. Overall, of those who met with RISE, 65% reported that they felt better after meeting with RISE, and 70% reported that RISE had been helpful (Table 1). Among participants who had not used RISE, 39% wished they had used RISE for themselves and 34% wished they had activated RISE for a colleague.
A total of 80% indicated some degree of professional burnout. Among those who had used RISE recently, 93% indicated at least some burnout. Among those who had never used RISE 67% indicated some burnout. This difference was statistically significant (p = 0.038) (Table 2). The odds that a staff nurse indicated some level of burnout was 4.3 times greater for nurses who had recently used RISE compared to nurses who had never used RISE (p = 0.048).
Burnout, satisfaction, and resilience among staff nurses and nurse leaders.
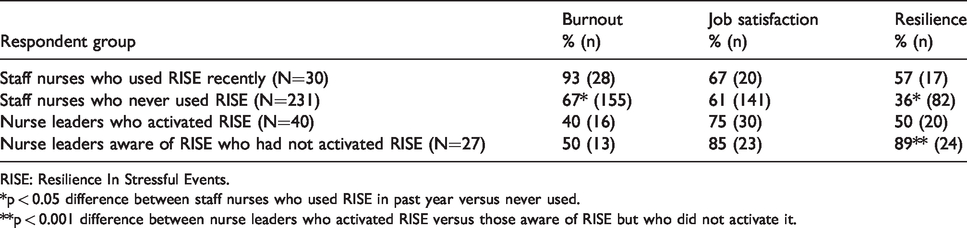
RISE: Resilience In Stressful Events.
*p < 0.05 difference between staff nurses who used RISE in past year versus never used.
**p < 0.001 difference between nurse leaders who activated RISE versus those aware of RISE but who did not activate it.
Overall, 39% reported their personal resilience as strong by responding affirmatively to the battery of the relevant survey questions. Those who had used RISE in the past year were significantly more likely to report resilience (57% versus 36%, p = 0.025) (Table 2).
Overall, job satisfaction was reported as 60% (n = 203). There was no difference in job satisfaction assessment between staff nurses who had used RISE recently and those who had not (67% versus 61%, p = 0.45) (Table 2).
Sixty percent (n = 202) of survey participants reported that they had not used other professional support resources. Among those who had used RISE recently, 80% had not used other resources, while among those who had never used RISE, 70% had never used other resources. Similar proportions of those who had and had not recently used RISE reported they were supported by close friends and family after a stressful situation (90% versus 76%, p = 0.079) and that the love received from their close friends and family helped them get over stressful occurrences (90% versus 77%, p = 0.095).
Staff nurse qualitative responses
Staff nurses who had used RISE reported that the program was helpful because RISE opened a safe, non-judgmental space where they could share their experience, process their feelings, and discover strategies to help them move forward. One nurse reported: “Just having someone for my colleague to talk to and normalize/validate feelings was so helpful.” Few nurses indicated that they had not used RISE because of either time constraints or not understanding the program’s expectations of RISE. Even fewer nurses reported not trusting in the confidentiality of the program.
Nurse leader results
The response rate among nurse leaders was 69% (75 out of 109 surveys were returned completed). Awareness of RISE among nurse leader respondents was 93%, and 56% indicated that they had activated RISE for a member of their staff. Among those who had activated RISE, 80% agreed that the support had been helpful to them and 68% agreed that the RISE support had been helpful to their staff (Table 3). Of the 40 who had activated the program, 20% had also used other professional support resources.
Awareness, use, and perceived benefits of RISE among nurse leaders (N = 75 out of 109 surveyed).
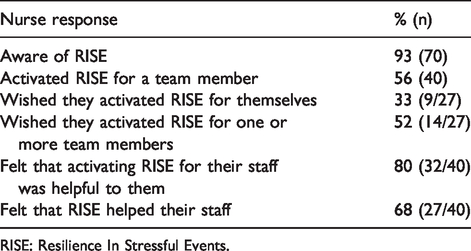
RISE: Resilience In Stressful Events.
Among nurse leader participants who had not activated but were aware of RISE, 33% indicated that they wished they had used RISE for themselves, and 52% wished they had activated RISE for one or more members of their team (Table 3). Among those who had not activated RISE, 55% had used other resources.
Responses regarding professional burnout revealed that 40% of nurse leaders who had activated RISE reported at least some burnout versus 50% of nurse leaders who had not activated RISE. This difference was not statistically significant (p = 0.42) (Table 2).
Regarding personal resilience, nurse leaders who had not activated RISE reported significantly higher resilience compared to those who had (89% versus 50%, p = 0.001) (Table 2). The odds that a nurse leader indicated a strong resilience was 0.12 times less for nurse leaders who had activated RISE compared to nurse leaders who had not activated used RISE (p = 0.002).
There was no difference in job satisfaction between nurse leaders who had and had not activated RISE (75% versus 85%, p = 0.315) (Table 2).
Nurse leader qualitative results
Nurse leaders activated RISE primarily due to death, traumatic events, or workplace violence. They reported that trained, neutral, non-judgmental, readily accessible responders who were available to provide a safe space for staff relieved them of the responsibility to provide that support themselves. For example, one leader wrote: “knowing there was a qualified person available was supportive and took something off my plate.”
Nurse leaders also noted that the RISE program provided a listening supportive presence for staff nurses, allowed nurse leaders to promote support in a different way, and felt that support was more effective from RISE than compared to support from themselves. To illustrate, another nurse leader wrote: “RISE offered a type of support that I wasn’t sure I could offer.”
Most nurse leaders could not think of any reason not to use RISE and wrote that RISE was a great resource. However, some felt that lack of available time or support timing were issues that may have prevented RISE activation and use. Others felt that they could have managed without support. Among nurse leaders who had not used RISE, most had not felt the need and some were not sure how to activate the Program.
Discussion
In this hospital survey of staff nurses and nurse leaders at a single academic medical center, the large majority of responders were aware of the hospital’s RISE peer support program and the perception of the program among users was positive. However, only a minority had used the program themselves or activated a call on behalf of colleagues. Staff nurses who had used RISE reported significantly more burnout and greater resilience than those who had not, but similar levels of job satisfaction. Nurse leaders who had not activated RISE were significantly more resilient than those who had, but similar in burnout and job satisfaction.
These findings are important because they contribute to the limited literature on the utilization and usefulness of hospital second victim support programs. These programs are difficult to evaluate because of the sensitive nature of many of the situations that led healthcare workers to call for peer support, which can include medical errors or patient-adverse events. There is an ethical conflict between the program’s mission to provide confidential, timely peer support, and the ability to collect data directly from users. For this reason, we elected to survey the entire nurse staff at the medical center.
Although 9 out of 10 staff nurses and nurse leaders were aware of RISE, a minority had used or had activated the support program. These findings are consistent with previous findings which evaluated RISE awareness and utilization, as well as findings from other programs.11,12,19 It appears that it is important to conduct program awareness activities on a continuous basis. It is possible that the kind of benefits reported by staff and leader nurses could be used to encourage the use of the peer support by others. In addition, healthcare professionals’ perception of support is associated with positive perceptions of safety culture 7 and may indirectly serve to improve patient safety as a whole. Sharing positive perceptions of RISE and actual benefits experienced through the program could influence safety culture, and peer support may be requested more often.
Staff nurses who had used RISE reported greater resilience but more burnout than those who had not. The meaning of latter finding is unclear. The level of burnout may be explained by self-selection. Our data did not allow us to identify level of burnout in recent RISE users before they utilized the service. For resilience, it is possible that peer support promoted PTG in some nurses or allowed them to increase awareness of their own resilience in the face of crisis. However, it is also known that less resilient people may experience certain factors to a greater degree than others, and that each nurse is likely to experience the process differently. 20 Further research is needed to determine the effectiveness of peer support to improve resilience and reduce burnout.
Interestingly, nurse leaders who had not activated RISE also reported a stronger sense of personal resilience. If those nurses observed (or assumed to have) similarly high levels of group or individual resilience in their staff nurses, this could be one reason why they did not activate RISE.
It is concerning that a majority of staff nurses indicated some degree of burnout. Several factors are known to contribute to burnout, including excessive workload, insufficient control or authority, lack of appropriate reward, lack of community, lack of fairness and mutual respect, and mismatched values of the organization and practice. 21 However, the level of burnout reported in this study could be explained in part by self-selection. Future research should be conducted utilizing a prospective, longitudinal approach in a larger sample to better understand what factors influence the use of peer support and how peer support may be beneficial to any member of the healthcare team.
Although staff nurse users reported having many personal, rather than professional support resources, support from a peer or someone who can directly relate to their experience and who has specialized training might be preferred if positive outcomes can be firmly established.10,11 According to the theory of nurse as wounded healer, receiving peer support may allow nurses to build on resilience and have a positive impact on care they provide.
Finally, it is worth noting that most of participants who met with RISE did not take time off from work after the incidents they requested support for. These findings could be used to corroborate the study by Moran et al. 8 which suggested the cost benefit of peer support.
This study had some limitations. The most important was the low response rate among staff nurses. The survey was distributed to all hospital nurses in an effort to maintain anonymity of those who had used RISE. However, this type of mass email survey distribution generally results in lower response rates. The survey was designed to elicit responses regardless familiarity with RISE. The response rate among the nurse leaders was higher and non-respondents were those who left the forum session early and thus were unable to complete the survey. Finally, because data collection was observational and cross-sectional it was not possible to establish causal relationships between the use of RISE and individual characteristics such as personal resilience and burnout.
In conclusion, in this study of nurses at an academic medical center, there was a high degree of awareness of the RISE program, favorable perceptions of the benefits of using RISE, and a desire for increased use. There was an association between staff nurse utilization of the program, greater resilience, and more burnout, but further studies are needed to investigate causation. Nonetheless, the study provides evidence to support the positive effects of a hospital peer support program. Internal marketing describing desirable features of the program,11,19 such as being confidential, timely, delivered by peers, and accessible in various forums, as well as positive benefits experienced by the users, could increase willingness to utilize a service among hospital staff. The results of this and related studies could help to persuade hospital leaders to embrace a culture of support within their organizations.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.