
Abstract
Background
Concern for the high prevalence and pervasive negative effects of clinician burnout has led to greater focus on clinician wellness programs, such as Mindfulness-Based Stress Reduction (MBSR). Our goal was to study MBSR feasibility and potential impact on clinician burnout, clinician–patient communication, and patient care and safety at a community hospital.
Methods
An eight-week MBSR program was offered for voluntary participation to clinicians at a community hospital. Pre–post surveys used validated scales and open-ended questions to assess participants’ levels of burnout, stress, mindfulness, communication behaviors, and perceived patient care and safety. T-tests were used to compare pre–post-program scale differences, and qualitative analysis identified themes from open-ended survey items.
Results
A total of 26 clinicians participated. Pre–post ratings showed significant improvements in personal burnout (p < .001), client-related burnout (p = .02), perceived stress (p < .001), and mindfulness (p = .01). Nearly all, 84% reported an improvement in self-care, 68% reported improved patient care, 50% reported improved patient communication, and 29% reported an increase in quality and safety of patient care. Qualitative analysis showed three themes of improvement in: emotional availability of the clinician, shared decision making and partnership with patients, and job satisfaction.
Conclusion
MBSR in a community hospital was feasible and suggests benefits related to reducing stress and burnout, as well as perceived improvement in clinician’s quality and safety of patient care. Given the serious negative effects of clinician burnout on patients, physicians, and the workplace, implementation of MBSR programs for clinicians should be considered.
Keywords
Background and objectives
Clinician well-being is of utmost importance in patient care. 1 However, many clinicians suffer from burnout, which may interfere with the quality of care they provide. 2 Burnout is more common among physicians than age-matched peers with similar education levels in the United States and peaks during training 2 as well as mid-career. 3 As a consequence of burnout, clinicians have reported substance abuse, marital/family discord, suicidal ideations, and stress-related health problems.2,4–6 In addition to personal problems, burnout has been linked to lower quality of care delivered to patients, such as reduced ability to express empathy, increased medical errors, and decreased patient satisfaction.7,8 Both individual-focused as well as institution-focused interventions may help decrease burnout among clinicians; however, more research is needed to determine which interventions are useful for specific populations. 9 It is agreed, however, that development of effective interventions for physician health and wellness is of great importance. 10 Mindfulness is one intervention that can address burnout and mental well-being of healthcare providers, 10 which in turn may have significant improvements on patient care.
Over the past 30 years, researchers have studied the impact of mindfulness-based practices on patient health outcomes. One of the most well-researched programs is Mindfulness-Based Stress Reduction (MBSR), which focuses on various mindfulness practices to effectively alleviate physical and emotional distress over a course of eight weekly, 2.5-h sessions, and a one-day retreat. 11 More recently, mindfulness-based practices have been extended to healthcare providers for well-being and improved patient care. As stated by Dr. Ronald Epstein, “This critical self-reflection (mindfulness) enables physicians to listen attentively to patients’ distress, recognize their own errors, refine their technical skills, make evidence-based decisions and clarify their values so they can act with compassion, technical competence, presence and insight.” 12 Indeed, studies reveal benefits for healthcare providers trained in mindfulness, including increased self-compassion, improved mood state, as well as reduced stress, burnout, distress, emotional exhaustion, anger, anxiety, and depression.13–18 Additionally, it has been posited that clinician mindfulness may reduce medical errors and enhance patient safety.12,19 Yet how mindfulness in healthcare providers may enhance patient care has not been well-studied. A recent systematic review examined 26 studies to determine if mindfulness-based interventions affected patient outcomes. 20 The review highlighted the following: significant data for healthcare provider reported patient improvements, moderate support for patient treatment outcomes (mostly looking at psychiatric patients), potential support but low-quality evidence for patient-centered care, potential support for patient safety improvements, and mixed support for patient satisfaction. The authors called for a more rigorous investigation on this topic using a theoretical framework of how mindfulness improves emotional competency, cognitive function and reduces burnout to lead to patient care outcomes.
Given concern about mitigating burnout and the existing evidence for the benefits of mindfulness on provider well-being, we were interested in investigating provider well-being and the perceived effect on patient care. The objectives of our study were to assess the feasibility and acceptability of conducting a MBSR program at a private, community hospital and to explore the impact of the course on provider burnout, self-efficacy in communication with patients, and perceived effect on patient care and safety. We hypothesized that this program would be feasible and acceptable in a community hospital and would show potential benefits on outcomes of interest.
Methods
Study design and setting
We used a pre–post design, measuring participants’ levels of burnout, stress, mindfulness, and self-reported communication behaviors through validated self-report surveys. Participants were healthcare providers working in a private, community hospital located in the suburbs of Baltimore which serves the local community, with over 20,000 inpatient and 52,000 emergency visits annually. The participants of the study voluntarily enrolled in a MBSR course offered in the Fall of 2017 and Spring of 2018 by the hospital’s medical staff office. Participants were contacted prior to the start of the course and voluntary consent was obtained for study participation. This study (IRB00148928) was reviewed by the Johns Hopkins Medicine Institutional Review Board and qualified as exempt research under the Department of Health and Human Services regulations.
MBSR
The MBSR course was comprised of eight sessions. Each session was held from 5:00 p.m. to 7:30 p.m., and led by an experienced MBSR instructor trained at the University of Massachusetts School of Medicine Center for Mindfulness. The session activities included mindfulness meditation practices, yoga and body awareness training, and exploration of habits of thinking, feeling, and action. Additionally, the course included brief didactics on stress physiology, interpersonal communication, and implementing self-care. The group is asked to commit to a daily home practice, including bringing mindfulness into daily life (e.g. mindful eating, mindful walking, and formal practices of meditation). During the eight weekly sessions, participants were encouraged to cultivate an accepting and compassionate stance towards their thoughts, emotional states, body sensations, and impulses. In addition to the eight sessions, there was a full-day silent retreat to further practice the range of skills.
Data collection and measures
Pre- and post-intervention survey packets were emailed to participants and returned via email or in person to the study team. The survey packets included only initials of the participants’ names, to allow pre–post matching for analysis and limited identifying information. The pre- and post-course survey packets included four valid and reliable measures: Copenhagen Burnout Inventory (CBI), 21 Perceived Stress Scale (PSS), 22 Mindful Awareness and Attention Scale (MAAS), 23 and a Clinician Communication tool. 24
The CBI has three subdomains: personal burnout (six items), work-related burnout (seven items), and client-related burnout (six items), scored along a 5-point Likert-type scale that is normalized on a scale from 0 to 100, with higher scores indicating more burnout. CBI has been used in previous studies of clinicians, 25 and it is freely available.
The Perceived Stress Scale (PSS) is a widely used 10-item measure of stress, 22 asking about the frequency of perception of stress during the last month, with responses along a 5-point Likert-type scale. The PSS totals range from 10 to 50, with higher scores indicating greater stress (alphas 0.89 pre, 0.87 post).
The Mindful Attention and Awareness Scale (MAAS) is a 15-item instrument rated along a 6-point Likert-type scale used to measure mindfulness – whether an individual is non-judgmentally aware of the present moment. 23 Averages for each item are taken with scores ranging from 1 to 6 and higher scores indicate greater mindfulness.
The Clinician Communication instrument was a 13-item relevant sub-domain of a survey used to test physician confidence in using specific communication strategies. 24 Participants estimated the frequency with which they used each strategy, on a Likert-type scale from never to always.
In addition, at the completion of the course, participants were also asked to fill out a questionnaire developed by the authors. This questionnaire included demographics and questions regarding experience with the course, (rated as excellent, good, neutral, poor, or very bad) and whether the course led to differences in their self-care, patient-care, communications, medical care, and patient safety (rated as yes or no, with a request for a qualitative description). These questions were developed to explore the program’s potential impact on perceived self- and patient care. Not all items on this questionnaire were answered by all respondents; therefore, the denominators of the responses vary.
Data analysis
Basic descriptive statistics were tabulated for participant demographics and survey responses. There were two individuals who took the course in both fall and following spring. Only their initial (fall) survey responses were included in analysis. T-tests were used to determine differences in means pre- and post-course survey responses. Cronbach’s alphas were calculated for each scale total and for each CBI domain to assess internal consistency. Items related to perceived effects on self-care and patient care were only asked on the post-survey, so the authors present percentage of respondents answering “yes.” Statistics were computed using Stata 13 (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP.) Open-ended items on the post-course evaluation were reviewed as qualitative data by the first and last authors. Themes were identified by topic salience and frequency of similar responses. There were no disagreements regarding theme identification.
Results
The fall cohort had 17 participants and the spring cohort had 9 new participants and 2 participants who repeated the course. Of the 26 total participants, 26 (100%) completed the pre-course survey and 20 (76%) completed the post-course survey. Participants included 24 physicians, 1 nurse, and 1 chaplain. A majority (21/26, 80%) were women. Mean age was 55.9 years with a range of 28 to 71 (only 17 people provided their age). Ninety-five percent of participants attended five or more sessions. Ninety-five percent of participants rated the course as good or excellent.
Burnout, stress, mindfulness, and communication ratings
Pre–post ratings showed significant improvements in personal burnout (p < .001), client-related burnout (p = .021), perceived stress scale (p < .001), and mindfulness (p = .01) (Table 1).
Differences before and after MBSR intervention for providers.
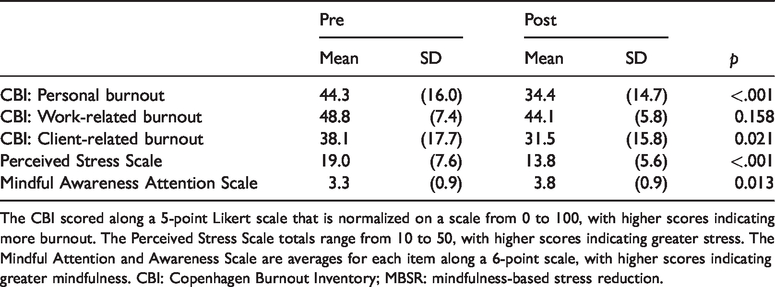
The CBI scored along a 5-point Likert scale that is normalized on a scale from 0 to 100, with higher scores indicating more burnout. The Perceived Stress Scale totals range from 10 to 50, with higher scores indicating greater stress. The Mindful Attention and Awareness Scale are averages for each item along a 6-point scale, with higher scores indicating greater mindfulness. CBI: Copenhagen Burnout Inventory; MBSR: mindfulness-based stress reduction.
Although not significantly different as a whole, individual communication items showed significant improvements (p < .05) for the following: “determining the psychological, emotional, and social needs of your patients” and “actively expressing understanding and empathy for patient’s problems” (Table 2). Cronbach's alpha across scales showed very good to excellent reliability, ranging from 0.77 to 0.90. Analysis of the questionnaire showed that a large majority of respondents (16/19; 84%) reported that the MBSR program changed how they care for themselves.
Differences before and after MBSR intervention for frequencies of performance of provider communication strategies.
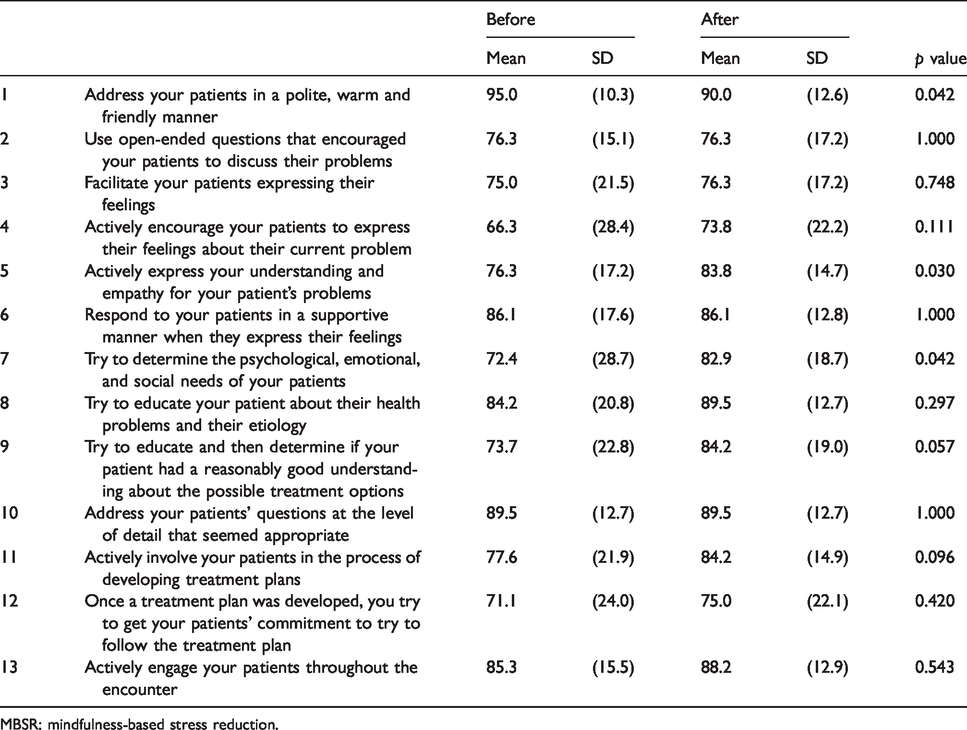
MBSR: mindfulness-based stress reduction.
Perceived impact on patient care
A majority of the responders, 68% (13/19) reported that it changed their patient care, 50% (9/18) reported that it changed their communication with their patients, 47% (9/19) reported that it changed the medical care they provide to patients, and 29% (5/17) reported that it changed the quality and safety of the care they provide.
Participant feedback
Fifteen out of 20 participants who completed the post-course survey offered additional comments related to the impact of the MBSR course on their work. Themes identified in qualitative analysis were: Improvement in emotional availability of the provider, improvement in shared decision making and partnership with patients, and improvement in job satisfaction. A sample of these responses included: “(a) more quality time with patients, looking at them and focusing;” “(b) active listening reduced repetitions;” “(c) less reactive to patient’s short-comings;” “(d) feel less rushed, with a slower pace;” “(e) more present;” “(f) learned to travel side by side with patient predicaments instead of taking it on my shoulder;” “(g) rekindle the joy of patient relationship;” “(h) attentive to patient needs;” “(i) less impatient;” “(j) better able to answer questions and address concerns;” “(k) stay with patient instead of being way ahead in my own head during the encounter.”
Discussion
In this pilot study, we investigated if mindfulness-based-training for healthcare providers is feasible in a typical community hospital setting, could reduce burnout and/or, lead to improved patient care as perceived by the clinician. The participants were majority female, middle age, and well-educated, which is consistent with the general demographic of participants interested in mindfulness training. 26 We discovered that participation in MBSR was feasible for this group: there was significant interest and enrollment in the course, and attendance was excellent, as more than 95% attended the majority of sessions. Additionally, 95% of the group rated this course as good or excellent.
Consistent with previous studies,9,15,27 clinicians reported a statistically significant reduction in personal burnout, client-related burnout, and perceived stress. The average score for personal burnout from the PUMA study was 39.5 including workers from all sectors. 21 In our study, the baseline score of 44.3 approaches the cut-off of 50 for moderate burn-out and decreased post intervention to 34.4 suggests a meaningful change for our participants. Additionally, the perceived stress scale 22 has a range from 0 to 40 with scores greater than 14 considered moderate perceived stress and scores greater than 27 considered as high perceived stress. Our participants’ scores improved from moderate stress to low stress at the conclusion of this intervention, reflecting a significant and meaningful difference. We also set out to investigate whether MBSR had a perceived effect on the care clinicians provide for their patients. In a systematic review of 46 studies, Hall et al. 28 showed that the clinicians’ burnout and poor well-being were associated with poorer patient safety in the majority of cases. In another study, increased length of recovery post hospitalization in a group of students in a large southern university was linked to clinicians that reported burnout. 29 These studies suggest a link between burnout and patient care. In our sample, 50% of participants perceived improvement in patient care, post-program. The participant feedback includes comments that point to being more focused, more fully present, listening more attentively, and feeling less judgmental toward patient’s behaviors. Additionally, in the communication survey, there were a number of significant changes post intervention that suggest improved patient care through better communication. Specifically, addressing patient in a warm and friendly manner, expressing empathy toward patients, trying to determine psychological, emotional, and social needs of patients. Cultivating attitudes of empathetic presence has been encouraged by Kabat Zinn 30 and others as a way of broadening an individual's practice of mindfulness. Kee et al. 31 studied 125 cases of patient complaints regarding their doctors in a hospital in Singapore and found that the highest reason for patient complaints was determined to be lack of empathy in their communication with the patient.
Two of the other questions with borderline statistical significance also pointed to an improvement in partnership with patients: actively involving patients in the process of developing treatment plans, and educating and determining if patient understands the treatment options. These findings coupled with comments such as: “learned to travel side by side with patient predicaments instead of taking it on my shoulder,” “stay with patient instead of being way ahead in my own head during the encounter,” and “better able to answer questions and address concerns” describe improvement in shared decision making and partnership with patients. Changes that lead to this partnership between clinician and their patients have been shown to lead to an improved quality of care and safety.32,33 Further, 29% of the participants stated they perceived improvement in patient safety and quality. These results are consistent with other studies34,35 where through the use of recording clinician–patient encounter, followed with Rotor Interaction Analysis System (RIAS), researchers concluded that mindfulness was significantly associated with high quality of care provided to patients. In one study, 34 it was noted that providers that score higher on MAAS showed more positive emotional atmosphere, and more time for rapport building during clinician–patient encounters. In another study, 35 it was noted post MBSR clinicians spoke less, the patient spoke more, and agreement and mutual understanding increased. This mutual agreement and understanding is the bases of the partnership that leads to patient-centered care.
Limitations of this study include its small sample size, no control condition or randomization, single site, and largely female participants. Another limitation was the inability to obtain direct patient feedback to determine potential improvements in patient care following completion of the MBSR course by clinicians. Furthermore, self-reported improvements are subject to response bias. Finally, since the group of clinicians who participated were volunteers for this intervention, there may have been a bias toward a desire and readiness for improvement.
Conclusion
Overall, the findings of this pilot study were favorable for the feasibility and acceptability of MBSR for clinicians at a community hospital, as well as decreasing their burnout and perceived stress. Additionally, there was evidence for perceived improvement in communication, patient care, and self-care among the participants. As communication and clinician–patient partnership are key components of safe and effective care, this program has the potential to enhance not only clinician quality of life but also to improve patient care and safety. Although attention has been brought to the negative consequences of burnout on clinicians and their employers, future research should explore the impact of effective clinician interventions to combat burnout, such as MBSR, on meaningful clinician and patient outcomes.
Footnotes
Acknowledgements
The authors thank Dr. Theresa Nguyen of Greater Baltimore Medical Center (GBMC) for contributing data from the clinicians in the Mindfulness Based Stress Reduction (MBSR) Course at GBMC.
Authors’ contributions
Dr. Sheila Hofert: Made a substantial contribution to the design of the work, participated in acquisition, and interpretation of data, drafted the article and revised it critically for important intellectual content. Dr. Sean Tackett: Provided the analysis and interpretation of the data and made a substantial contribution to revisions of the paper drafted by the first author. Dr. Neda Gould: Made a substantial contribution to the revision of the paper. Dr. Erica Sibinga: Made a substantial contribution to the concept and design of the work, helped with interpretation of data, made a significant contribution to the revision of the paper and approved the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval/patient consent
This manuscript has not been published elsewhere and will not be submitted elsewhere while under consideration by your journal. All authors are responsible for the reported research and have participated in the concept and design, analysis and interpretation of data, drafting and/or revising the manuscript, and have approved the manuscript as submitted. No patient consents were needed for this submission
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank Dr. Melissa Sparrow, Chief of Staff at GBMC for supporting the program to provide MBSR training for the clinician in GBMC.