
Abstract
According to a study by Johns Hopkins, an average of 251,454 Americans die annually from medical errors. Medical error is the third leading cause of death in the U.S. after heart disease and cancer. Unintended retained foreign objects (URFOs) has been identified as the most common sentinel event by The Joint Commission. This paper proposes a proactive risk assessment framework to enhance patient safety in operating rooms by addressing the URFOs issue. This framework is developed by integrating the 10 traits of a positive safety culture, initially introduced by the nuclear industry and later adopted by other industries, with an accident investigation methodology called AcciMap, originally developed by Rasmussen.
The AcciMap is a hierarchical framework consisting of several layers: government and regulatory bodies, company (hospital), (surgery division) management, (operating room) staff, and work. Thirty main categories of socio-technical contributing causes of URFOs were captured across the AcciMap layers. Organizational factors were identified as the root cause of questionable decisions made by staff and management. Financial and budget constraints, inadequate training infrastructure, absence of a risk management infrastructure, and leadership failure are the most influential organizational factors contributed to URFOs.
Our mapping of the aforementioned positive safety culture traits on the AcciMap depicted that the four traits of Work Processes, Leadership Safety Values and Actions, Effective Communication, and Continuous Learning had the most influence on the URFOs issue. Associated recommendations to these findings are provided to contribute to reducing risks of URFOs instances.
Introduction
According to a study by Johns Hopkins, 1 an average of 251,454 Americans die every year from medical errors. This makes medical errors the third leading cause of death in the U.S., after heart disease (614,348 deaths per year) and cancer (591,699 deaths per year). Adding the financial cost to human tragedy, medical error easily rises to the top ranks of urgent, widespread problems.
High error rates with serious consequences are most likely to occur in intensive care units, operating rooms (ORs) and emergency departments due to the tightly coupled and interactively complex nature of their operations.2,3 Among different adverse events and medical errors in healthcare settings, unintended retained foreign objects (URFOs) has been identified as the most common sentinel event (any unanticipated event in a healthcare setting resulting in death or serious physical or psychological injury to a patient, not related to the natural course of the patient's illness) by The Joint Commission. 4 Therefore, this study will specifically focus on the analysis of URFOs in ORs.
Our extensive literature research identifies a vital need for the development of more robust proactive risk assessment frameworks to identify and analyze risks of failures in healthcare settings and improve the quality of care by preventing medical errors. Proactive frameworks contribute to predicting and in one step further, preventing errors and failures in a system. This study fills an important gap in proactive risk assessment in the healthcare industry. It specifically contributes to improving patient safety, as a major aim and aspect of quality of care, in ORs.
The proposed proactive risk assessment framework in this study has been developed by integrating the 10 traits of a positive safety culture, initially introduced by the nuclear industry and later adopted by other industries, with an accident investigation methodology called AcciMap, originally developed by Rasmussen. To our knowledge, this is the first study, not only in the healthcare industry but also other industries, that proposes such an integration to develop proactive characteristics.
There have been different developed methodologies to better understand and analyze accidents. Some examples of these methodologies include the Systems-Theoretic Accident Model and Processes (STAMP) by Leveson,5,6 Reason's model of organizational accidents 7 and Rasmussen's AcciMap framework. 8 The AcciMap framework is particularly useful for this purpose as it models different contributing factors of an accident, and their interactions, in a causal diagram across several layers that each represent a main group of involved decision-makers and stakeholders. This contributes to avoiding the unfair blame of front-line operators.According to the Health and Safety Commission, 9 safety culture is “the product of individual and group values, attitudes, perceptions, competencies, and patterns of behavior that determine commitment to, and the style and proficiency of, an organization's health and safety management”. Inadequate safety culture has been a significant contributing factor of sentinel events according to The Joint Commission. 10 Therefore, we believe that improving the culture of safety in healthcare settings and hospitals will contribute to enhancing the safety of operations and reducing instances of sentinel events, URFOs in this context.
Brief literature review
The healthcare industry has only recently applied risk assessment methodologies to enhance quality of care compared to many other safety-critical industries such as nuclear power, transportation sector, and oil and gas industry. Further, there are even fewer studies that proactively analyze and address the risks associated with healthcare delivery and more specifically, patient safety.
Some of the previous studies on proactive risk assessment primarily focus on hazards – or “risk factors” that increase the probability of errors or injuries in healthcare settings (e.g.11–16) In addition, there have been few studies on proactive risk assessment of surgical site infections in ambulatory surgical centers (e.g.17,18). However, to our knowledge, these studies have neither focused on patient safety in ORs (except Carayon, Xie and Kianfar 13 ) nor addressed the URFOs issue. The proactive characteristic of this framework will enable healthcare practitioners to enhance patient safety by identifying contributing and root causes of URFOs and analyzing and reducing risks of their occurrence.
Methods
The proposed risk assessment framework in this study is developed by integrating the 10 traits of a positive safety culture, initially introduced by the U.S. Nuclear Regulatory Commission (NRC) 19 and later adopted by the Institute of Nuclear Power Operations (INPO), 20 with an accident investigation framework called AcciMap, originally proposed by Rasmussen, 8 to proactively address and analyze risks of failures, issues and incidents (URFOs specifically) in ORs, which endanger patient safety. The proactive characteristic of this proposed risk assessment framework is through identifying weak instances of safety culture as well as those traits of a positive safety culture that have the highest influence on addressing the investigated contributing causes of URFOs. This will allow healthcare practitioners to enhance those aspects and traits of safety culture that best improve patient safety through reducing risks of URFOs in operating rooms. The workflow process in Figure 1 summarizes the main phases of developing our proposed risk assessment framework.

The workflow process showing the main phases/steps to develop our proposed proactive risk assessment framework.
In the first phase, we conduct an exhaustive literature search of existing studies that have analyzed the URFOs issue in order to identify a comprehensive list of socio-technical factors that contributed to this issue. We then develop an AcciMap framework to systematically analyze the contributing causes of URFOs and the role of different key involved players in causing them. In this phase, we also consult with subject matter experts to verify our captured factors in the AcciMap framework and also to make sure there are no missing factors.
Rasmussen introduced a six-layer, hierarchical framework (Figure 2), known as risk management framework, in which, each layer represents a main group of involved decision-makers, players, or stakeholders in a studied system. 8 These six layers, from top to bottom, are: government, regulators and associations, company, management, staff, and work. The analysis of the framework includes assessing the activities of key players in each layer. More importantly, this framework captures the interactions between those key players within the stated layers. 21
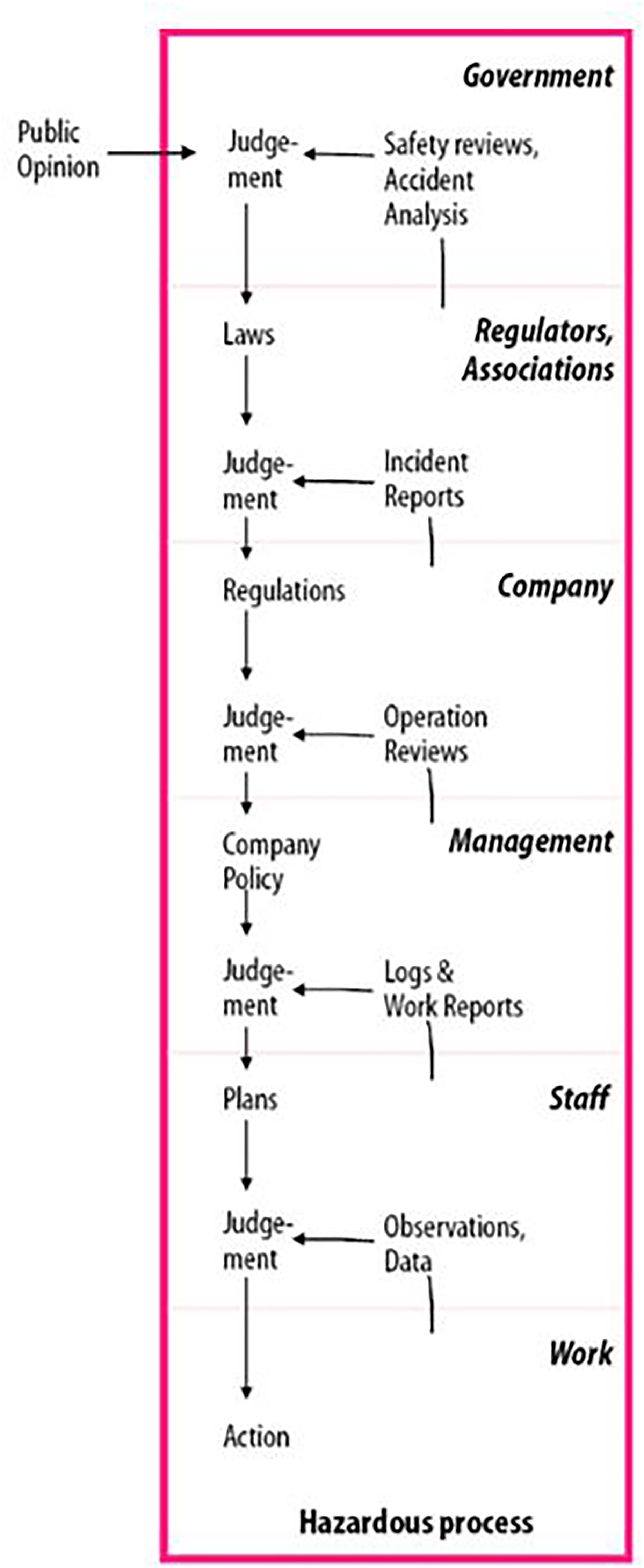
Rasmussen's risk management framework to capture the role of different involved key players in a studied system (Source of image: Rasmussen & Svedung 21 ).
The AcciMap methodology was developed by Rasmussen in 1997 in conjunction with his six-layer risk management framework, which is illustrated in Figure 2. This methodology captures the associated socio-technical factors of an incident/accident within an integrated framework and analyzes the contribution of those factors in causing the accident. This graphical representation is useful in structuring the analyses of hazardous work systems and in identifying the interactions between different levels of decision-makers, which shape the landscape in which accidents may “unfold” themselves. 21 This characteristic avoids the unfair blame of front-line operators, since it provides a big-picture perspective and background about events and conditions that led to accidents, and it systematically analyzes major causes of those accidents.
The AcciMap framework has been used as an independent accident investigation tool in different industries and domains, including transportation (e.g.21–24), aviation (e.g.25,26), gas pipeline transport, 27 chemical processing (e.g,28,29), gas production, 30 gas storage, 31 oil and gas drilling,32,33 electric power grid reliability, 34 public health (e.g. 35 ), and healthcare and medication errors. 36
In this study, we have customized the layers of the AcciMap framework to the context of a healthcare delivery system and more specifically operating rooms to investigate the URFOs issue. We have also combined the first two top layers and in the modified AcciMap framework, we have the following layers: government and regulatory bodies; company (hospital); management (surgery division management); staff (surgeons, nurses, anesthesiologists, OR technicians, and other related personnel); and work and processes in ORs. The identified socio-technical contributing causes of URFOs in the first phase of our study are mapped across the aforementioned layers of the AcciMap framework. In addition, the interactions between those captured factors and the layers they belong to are represented by connecting them using arrows.
The AcciMap, like other accident analysis frameworks provides retrospective analysis. Therefore, in the next phase, the 10 traits of a positive safety culture are integrated with (mapped into) each of the layers of our developed AcciMap framework to thoroughly investigate the influence of each trait on the captured contributing causes of URFOs in that layer. This also contributes to better understanding about the consequences of a weak safety culture in ORs operations, as a foundation to determine actions to improve this culture. To our knowledge, this is the first study, not only in the healthcare industry but also other industries, that proposes such an integration to develop proactive characteristics.
The NRC in its final Safety Culture Policy Statement 19 introduced nine traits for a positive safety culture: 1) Continuous Learning, 2) Problem Identification and Resolution, 3) Work Processes, 4) Environment for Raising Concerns, 5) Personal Accountability, 6) Effective Safety Communication, 7) Questioning Attitude, 8) Leadership Safety Values and Actions, and 9) Respectful Work Environment. The INPO 20 later added the tenth trait of a positive safety culture, which is Decision-Making. Although the nuclear power industry originally introduced these traits of a positive safety culture, they have been adopted completely or to some extent by other safety-critical industries, including offshore operations and pipeline and hazardous materials transport.
In the offshore industry, the Bureau of Safety and Environmental Enforcement (BSEE), which is an agency under the United States Department of the Interior and the lead agency in charge of improving safety and ensuring environmental protection relating to the offshore energy industry (mainly natural gas and oil) on the US Outer Continental Shelf, adopted the first 9 above-mentioned traits of a positive safety culture. In its published Final Safety Culture Policy Statement in 2013, 37 the BSEE states that those traits can be equally applied to the offshore industry, and the BSEE and the industry can greatly benefit from embracing these traits.
The Pipeline and Hazardous Materials Safety Administration (PHMSA) of the US Department Transportation has also recently (January 2021) published its Final Safety Culture Report 38 in which 5 principles of safety culture have been stated. Those principles are common with the NRC's and INPO's traits of a positive safety culture. They are leadership for safety, accountability and involvement, cooperation and communication, holistic and systematic approach, and continuous learning. Therefore, these traits, as it can be seen, are not industry-specific and we believe they can enable the evaluation and empowerment of safety culture in different safety-sensitive industries, including healthcare.
In the final phase, the most influential traits of a positive safety culture on the safety of operations and patients in ORs are identified by conducting some analyses on our developed framework. This provides necessary information to healthcare settings and ORs to focus on those positive safety culture traits that will most contribute to improving patient safety and reducing URFOs. For our model verification and validation, we have been able to refer to different credible references, based on an extensive literature search, as sources to capture contributing causes of URFOs and develop our described framework. We have also been able to communicate with subject matter experts for the purpose of model verification and validation. More details about this have been provided in the Results section, Model Validation and Verification sub-section.
There have been some studies in the context of healthcare industry focusing on safety aspects from behavioral and psychological perspectives. For instance, Edmondson and colleagues39–41 studied psychological safety in connection with team learning, leadership effectiveness, and hierarchy. In addition, Sexton and colleagues42–45 have identified a list of behavioral markers, which include information sharing, inquiry, teaching, workload management, environmental awareness, teamwork, and leadership of surgical teams, and their impact on patient safety. Furthermore, Sexton and colleagues have further investigated the role of teamwork and resilience on safety culture in one study 46 and the impact of leadership walk-rounds to improve patient safety culture through employee engagement. 47 The 10 traits of a positive safety culture in our proposed framework not only emphasize on the above-mentioned behavioral and psychological markers, but also call attention to other essential safety aspects to ensure patient safety in ORs. Therefore, based on this literature review and the above-explained reason about the generalizability of the 10 traits of a positive safety culture to the healthcare industry, we believe that not only are these traits inclusive of the existing studies in the healthcare industry that address safety culture, but also they are more comprehensive in capturing characteristics of a positive safety culture.
Results
Accimap framework for the analysis of URFOs in operating rooms
As described in the Methods section, the illustrated workflow process in Figure 1 was followed to develop our proactive risk assessment framework. In the first step, we identified the socio-technical factors that have contributed to the URFOs issue and compromised patient safety through an exhaustive literature search of studies that have analyzed this issue as well as communication with experts. Those contributing factors were then mapped into (located across) associated layers of the AcciMap framework to create the building blocks of the framework. In the next step, we categorized the captured contributing causes across each of the AcciMap layers into main groups based on their similarities. This also enabled us to reduce the size of our developed AcciMap framework to help readers better comprehend it, as presenting more than 70 single contributing factors would have been overwhelming. As an example for this categorization, in the layer of Government and Regulatory Bodies, contributing causes of lack of standardized count policies,48–51 lack of descriptive homogeneity regarding definitions and collection of sentinel events,51–53 and lack of role clarity in the count process 48 were summarized under lack of policies and procedures main group.
Thereafter, the interactions between the layers and their associated contributing factors were captured using arrows. These arrows illustrate the causal relation between each two nodes (captured contributing factors) of the framework. To create these arrows, we investigated the impact of each and every captured category of contributing causes of URFOs (and its sub-factors) on other categories, both across its associated layer and other lower layers. The AcciMap framework for the analysis of URFOs has been illustrated in Figure 3. As it can be seen from this figure, not only does the AcciMap framework identify both internal and external (to a healthcare facility) socio-technical contributing causes of URFOs, which show the role and involvement of different key players and stakeholders, across its systematic, hierarchical structure, but also it captures (dysfunctional) interaction of those involved players.
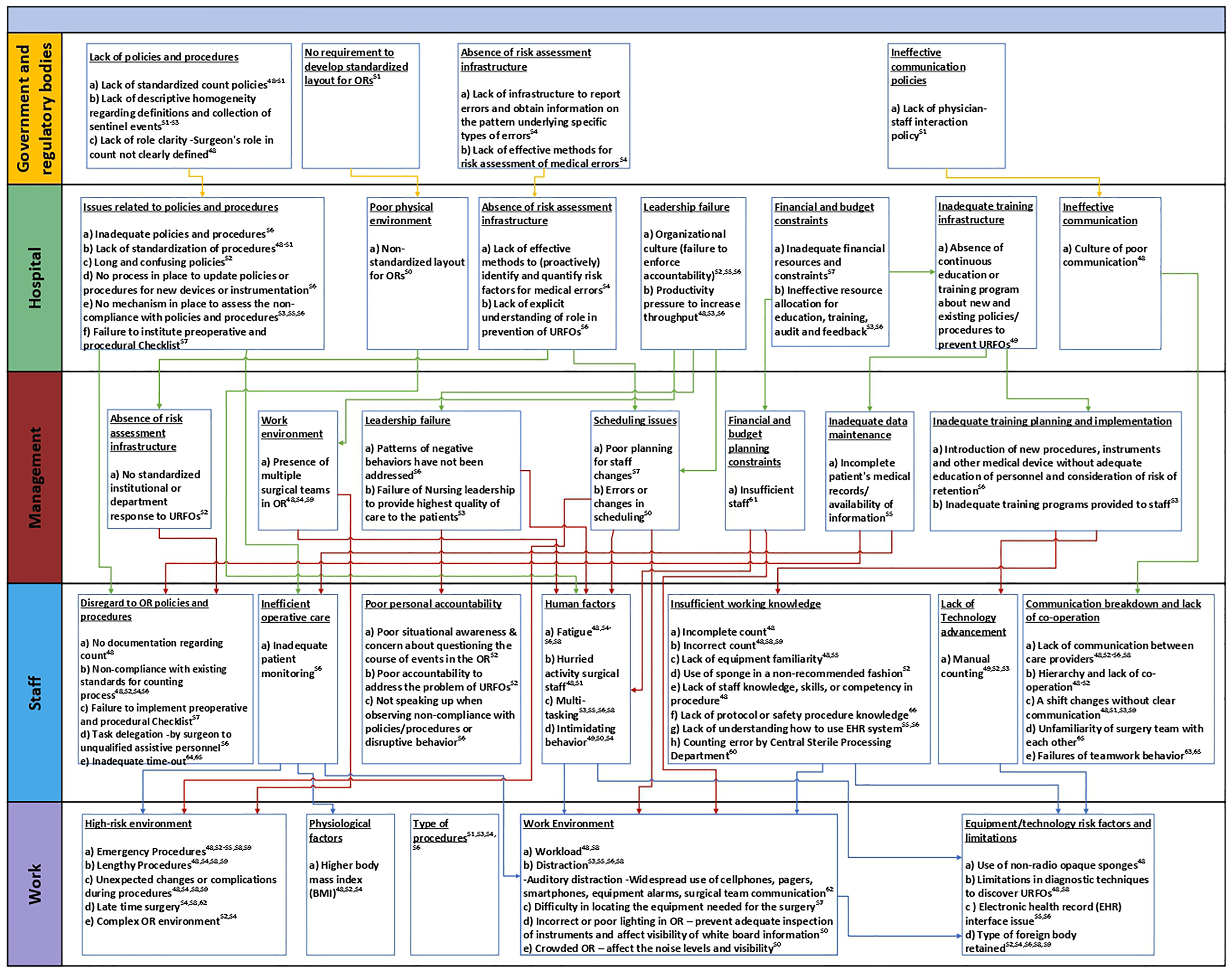
The developed AcciMap framework to analyze socio-technical contributing causes of URFOs and their interactions across the framework layers.
As stated before, we conducted a comprehensive literature review of existing studies and publications investigating the URFOs issue to capture its contributing causes. We conducted search on different sources and databases including ProQuest, PubMed, Medline, Scopus, and Google Scholar, up to the time of submitting this paper, to find related publications analyzing URFOs and their contributing causes. If you refer to our developed AcciMap framework in Figure 3, each of the captured contributing factors across the layers of this framework has different cited references, which are the results of our comprehensive literature search.
In addition to our comprehensive literature search, at this stage of our research and analysis, we consulted with different subject matter experts to validate the captured factors in our developed AcciMap framework and to also make sure there are no missing factors based on those experts’ experience and knowledge. We specifically communicated and held separate meetings with subject matter experts from the Office of Quality and Patient Safety at The Joint Commission and the University of Southern California's Keck School of Medicine. The name of these experts has been provided in our Acknowledgement section. After discussing our developed AcciMap framework with those experts, they confirmed the existence and impact of the captured factors. There were also few factors added to the framework; e.g. unfamiliarity of surgery teams with each other.
As stated before, in this study, we have combined the first two layers of Figure 2 into one layer and considered the impact of Government and Regulatory Bodies as a whole. Hence, the layers of our developed AcciMap framework in Figure 3, from top to bottom, are: Government and Regulatory Bodies, Company (Hospital), (Surgery Division) Management, Staff (e.g. surgeons, nurses, anesthesiologists, and OR technicians), and Work and Processes in ORs.
Layer 1: government and regulatory bodies
Government regulatory authority is in-charge of enacting new rules and policies as well as ensuring a quality of care and patient safety in operating rooms. In this layer, factors such as lack of a standardized surgical count policy48–51 as well as ineffective communication policy 51 are two of the contributing causes of URFOs. In addition, there is no mandatory nationwide system to report URFO cases causing death or serious harm. 54 The mandatory reporting may contribute to reducing medical errors and improve quality of healthcare. Lack of oversight from regulatory bodies to improve the physical environment of ORs by standardizing the layout of procedural areas, which prevents surgical teams from working in unfamiliar locations, is another contributing cause of URFOs in this layer. 50
Layer 2: company (hospital)
The lack of proactive safety culture of the hospital has been an issue in several instances; for example, leadership failure is a major contributing cause of URFOs. Organizational culture; e.g. failure to enforce accountability,52,55,56 and productivity pressure to increase throughput48,53,56 are the two captured factors under the main category of leadership failure in the Company layer.
Issues related to policies and procedures is another main category of contributing causes of URFOs. There are several factors under this main category including inadequate count policies and procedures, 56 lack of standardized count policies,48–51 long and confusing policies and procedures, 52 no process in place to assess the noncompliance with policies and procedures,53,55,56 and failure to institute pre-operative and procedural checklists. 57 Moreover, absence of a risk assessment infrastructure; e.g. lack of effective methods to (proactively) identify and quantify risk factors for medical errors, 54 has contributed to URFO cases.
Furthermore, the three main categories of financial and budget constraints; e.g. inadequate financial resources, 57 inadequate training infrastructure; e.g. absence of continuous education or training programs regarding existing and new policies and procedures to prevent URFOs, 49 and ineffective communication; i.e. culture of poor coomunication, 48 have played a critical role in causing URFOs.
Layer 3: (surgery division) management
There are different contributing causes of URFOs that root in the Management layer. For instance, no standardized department response to URFOs 52 is a contributing factor that illustrates the absence of a risk assessment infrastructure. Furthermore, factors such as inefficient scheduling,50,57 inadequate data (e.g. patients’ medical record) maintenance, 55 and inadequate training planning and implementation53,56 are other main contributing causes of URFOs, which are related to the layer of Management. Captured factors in each layer have projection from the layer(s) above. For instance, captured factors in the Management layer influence decisions and actions of people in the Staff layer and contribute to issues, errors, and failures in that layer.
Layer 4: operating room staff (e.g. surgeons, nurses, anesthesiologists, and technicians)
Operating room staff; e.g. surgeons, nurses, anesthesiologists and technicians, are the key players whose actions and decisions immediately showcase themselves in the scope of influencing the layer of Work and Processes or by causing the final negative outcome/incident; a URFO in this context. The most frequent category of contributing causes at the Staff layer is human factors-related issues, which include fatigue,48,54–56,58 distraction,53,55,56,58 and hurried activities of surgical team.48,51 Operating room staff's disregard to policies and procedures and their noncompliance with existing procedures; e.g. counting process and time-out, is another main category of URFOs contributing causes.48,52,54,56,57,64,65
Moreover, staff's poor personal accountability and lack of a questioning attitude52,56 has contributed to URFO cases. Staff's insufficient working knowledge and errors made due to that48,52,55,56,58–60, 66 is another major contributing cause of URFOs, which has some roots from the above layer (layer of Management); mainly inadequate training.
Furthermore, communication breakdown and lack of co-operation is another main category of contributing causes of URFOs in the Staff layer. Captured issues in this category include: lack of effective communication and interaction between care providers,48,52–56,58 a shift change without clear communication,48,51,53,59 unfamiliarity of surgery team with each other, 65 and poor teamwork.63,65
Layer 5: work and processes in ORs
This layer is the last layer of the AcciMap framework that captures the role of work and processes in an operating room, utilized equipment and technology, as well as any related design and conditions in the OR. Our analysis of existing studies that investigated URFOs shows that physiological factors like body mass index (BMI)48,52,54 and operating rooms being a high-risk environment because of factors such as unexpected intraoperative events; e.g. complications during surgery,48,52–55,58,59 and procedure duration48,54,58,59 contribute to increasing the risk of URFOs. Risk factors related to OR equipment and used tools and devices and their limitations and issues; e.g. electronic health records interface issues55,56 and use of non-radio opaque sponges, 48 have also been identified as contributing causes of URFOs. In addition, an operating room work environment as far as its layout, ergonomics design, and concurrent events can cause human factors’ errors. For instance, incorrect or poor lighting in ORs can prevent adequate and effective inspection of instruments while conducting the count procedure, 50 or auditory distractions because of widespread use of cellphones, pagers, smart devices, and equipment alarms can cause errors in decision-making. 62
Another useful characteristic of the AcciMap is connecting the captured contributing causes of an investigated incident/accident across different layers of the framework to show how different involved socio-technical factors interacted with each other in causing the incident. The arrows in the AcciMap (Figure 3) illustrate the causal relationship between captured contributing factors across different layers and the way they are combined to produce the final outcome (an unintended retained foreign object in this case). In this way, an upward tracking by following the arrows from the lowest layer to the topmost one in the diagram enables us to uncover why each of the factors emerged 23 and how those contributing factors interrelated with each other. We will provide more details about this characteristic with an example in the Discussion section.
Mapping the traits of a positive safety culture on the acciMap framework
As described in the Methods section, after developing our AcciMap framework to capture and analyze the socio-technical contributing causes of URFOs across the layers of this framework, we mapped each of the ten aforementioned traits of a positive safety culture on the developed AcciMap framework. This was done by investigating the impact of each trait on each of the layers of the AcciMap framework and its captured contributing causes. This mapping has been illustrated in Figures 4(a) and 4(b). We needed to breakdown our whole framework into two pieces due to a size constraint. We have illustrated the mapping of the Work Processes, Leadership Safety Values and Actions, Effective Communication, and Continuous Learning traits on the AcciMap framework in Figure 4(a) and the mapping of the Environment for Raising Concerns, Problems Identification and Resolution, Respectful Work Environment, Questioning Attitude, Decision-Making, and Personal Accountability traits on the AcciMap framework in Figure 4(b). In these two figures, the layers of the AcciMap framework are represented in the rows, and each column depicts one of those 10 traits of a positive safety culture under which, all the contributing causes of URFOs that are influenced by that trait are captured. As an example to illustrate the stated mapping, consider the Effective Communication trait in Figure 4(a). We investigated the impact of Effective Communication trait on each and every captured factor in the AcciMap framework. After careful analysis, we determined that this trait influences the following contributing causes of URFOs: 1) lack of role clarity 48 (under the main category of lack of policies and procedures) and ineffective communication policies 51 from the Government and Regulatory Bodies layer, 2) ineffective communication; i.e. culture of poor communication 48 from the Company layer, 3) presence of multiple surgical teams in ORs48,54,59 (under the work environment main category) from the Management layer, and 4) communication breakdown and lack of co-operation48,51–56, 59,63, 65 from the Staff layer. Integrating the 10 traits of a positive safety culture with the AcciMap framework, which systematically captures and analyzes the contributing causes of URFOs across its hierarchical layers, enabled us to identify instances of violations across safety culture traits and understand the consequences of those violations on OR operations; i.e. creation of URFO cases. This integration and analysis has also allowed us to identify the most influential traits of a positive safety culture through which, we can improve this culture, enhance patient safety, and reduce risks of URFOs. The Discussion section provides more analysis of our developed framework in Figures 4(a) and 4(b).
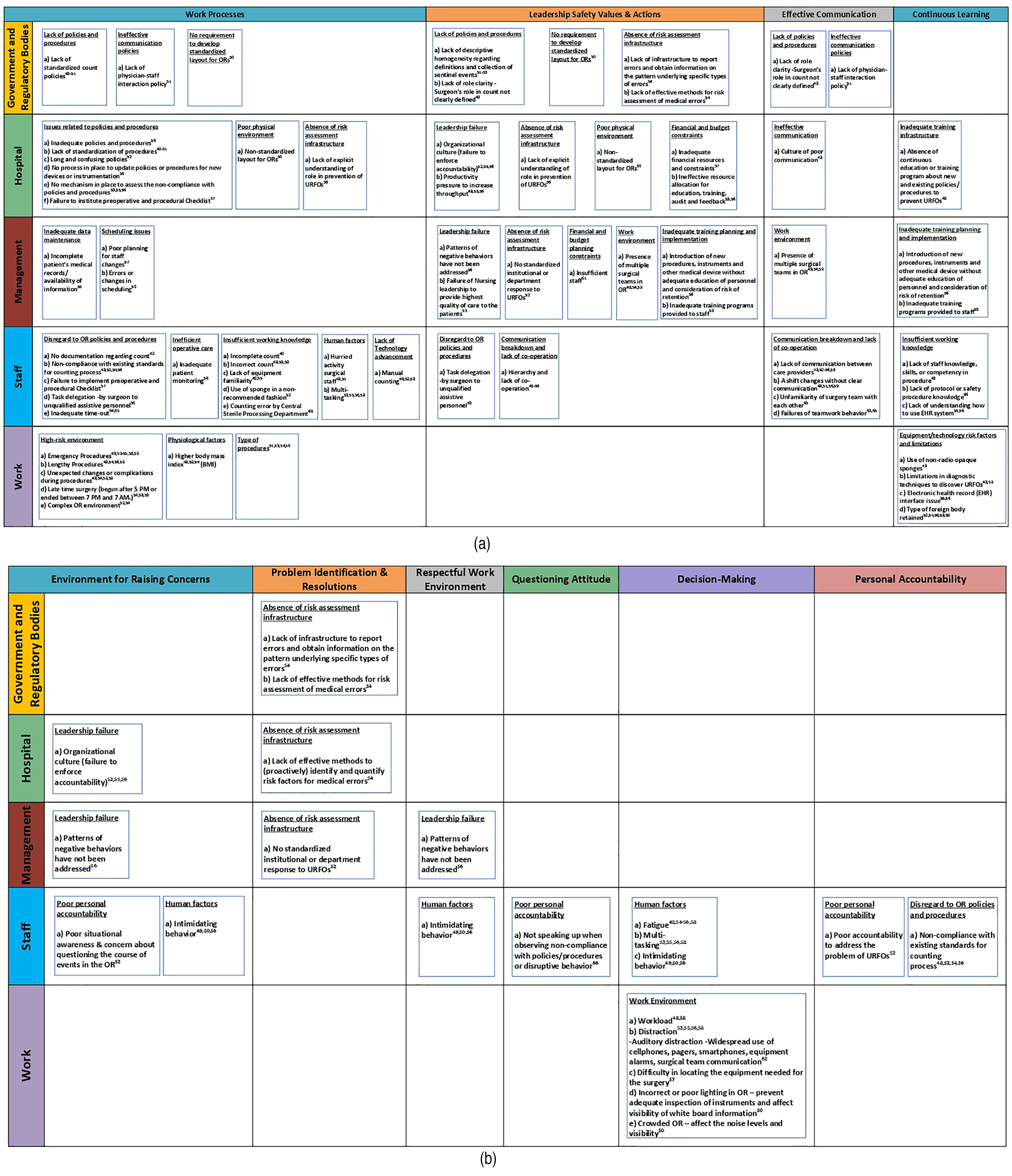
The developed framework to integrate the 10 traits of a positive safety culture with the AcciMap and the captured contributing causes of URFOs across its layers (a) This figure shows the mapping of the first four traits into the AcciMap framework. (b) This figure shows the mapping of the last six traits into the AcciMap framework.
Model verification and validation
The purpose of validation studies is to corroborate our findings and to ensure correct and effective solution to improve patient care and safety by minimizing the risk of URFOs. As far as verification and validation of our methodology and conducted analyses, firstly, all the captured factors in our developed frameworks are endorsed by at least one (in many cases, by several) credible reference(s), as we conducted an exhaustive and comprehensive literature search to review existing studies in the literature that analyzed URFO cases. A summary of our extensive literature search was provided in the beginning of the Results section. As stated before, if you refer to our developed AcciMap framework in Figure 3, each of the captured contributing factors across the layers of this framework has different cited references, which are the results of our comprehensive literature search.
Moreover, after first developing our AcciMap framework and later mapping the traits of a positive safety culture to the AcciMap framework, we consulted with different subject matter experts to seek their opinion regarding those developed frameworks and our research findings. As stated before (in the Results section), we held meetings with subject matter experts from the Office of Quality and Patient Safety at The Joint Commission and the University of Southern California's Keck School of Medicine. The captured socio-technical factors across the layers of the AcciMap framework were verified by those subject matter experts. There were few controbuting causes that were added to the AcciMap framework as well; e.g. unfamiliarity of surgery team with each other.
Moreover, we consulted with subject matter experts to validate our findings after mapping the traits of a positive safety culture to the AcciMap framework. More details regarding this consultation have been provided in the Discussion section after we completed the mapping process and identified the most influential traits of a sportive safety culture.
Discussion
We explained the process of integrating the traits of a positive safety culture with the AcciMap framework with the purpose of enhancing patient safety in operating rooms through monitoring and eliminating the sources and contributing causes of failures and issues; URFOs specifically, in healthcare settings. This integration has enabled us to not only systematically investigate and identify the socio-technical contributing causes of URFOs across the layers of the AcciMap framework, but also to determine what traits of a positive safety culture impact those identified contributing causes the most and by improving the culture of safety in healthcare settings; i.e. hospitals, through enhancing the determined traits, we can increase the safety of operations and reduce risks of failures and issues; URFOs specifically, which leads to increasing patient safety.
It is noteworthy that the developed AcciMap framework in this study (Figure 3) and its captured contributing causes of URFOs as well as our identified most influential traits of a positive safety culture are based on our comprehensive literature review of studies that investigated this medical error and our consultation with subject matter experts. Hospitals, however, can follow the described and illustrated roadmap/Workflow process in Figure 1 and develop their own customized and context-specific methodology based on need (e.g. if there are other factors to consider in their context compared to the ones captured in this paper) to assess their own strengths and weaknesses and later create and execute interventions to positively impact those traits of a positive safety culture that have influenced them the most. Furthermore, it is important to note that culture is not a discrete binary ‘on-off’ variable; rather a continuous variable with wide variation across settings and contexts.
As described before, the AcciMap framework, through its graphical representation, provides a big-picture to illustrate the context in which an accident occurred as well as the interactions between different levels of a socio-technical system that resulted in that event; i.e. accident. A total of 74 contributing causes of URFOs were first identified across the layers of the AcciMap framework. These contributing factors were further categorized into 30 main groups, as it can be seen in Figure 3.
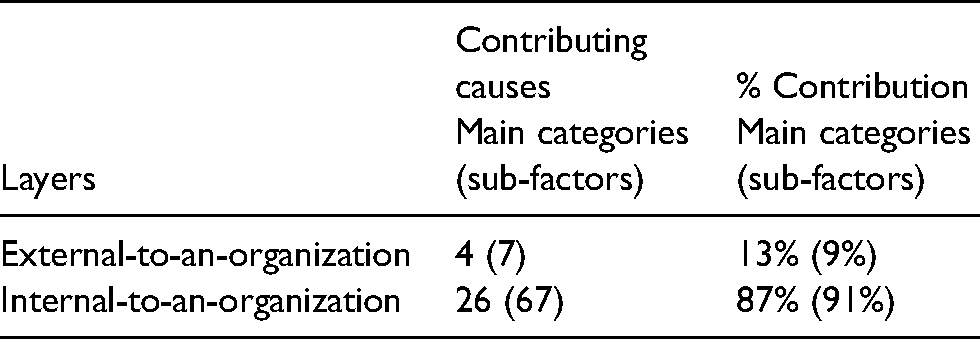
The AcciMap framework highlights the involvement of key players and stakeholders both external- and internal-to-an-organization; a hospital in the context of our analysis. We assessed the impact of external factors and players; i.e. government and regulatory bodies, in the first layer of our developed AcciMap framework and the internal (to-an-organization) factors in the layers of Company, Management, Staff, and Work. Since we did not have access to any data regarding instances of URFOs in hospitals and the investigation of each instance and its contributing causes to run any statistical analysis, we assumed that all the captured contributing causes in our AcciMap framework have a similar importance weight. Further statistical analysis upon receipt of data is one of the future directions of this study. Based on this assumption, our analysis of the developed AcciMap framework in Figure 3 depicts that most of the contributing causes of URFOs have been identified in the internal-to-an-organization layers (Table 1). As Table 1 shows, 26 out of 30 captured main categories of contributing causes of URFOs are related to internal-to-an-organization factors. The numbers in parentheses indicate the number of sub-factors (before the categorization process). The sub-factors of each main category can be found listed inside the box of that main category in Figure 3.
Distribution of contributing causes of URFOs across the AcciMap layers; division into internal- and external-to-an-organization categories.
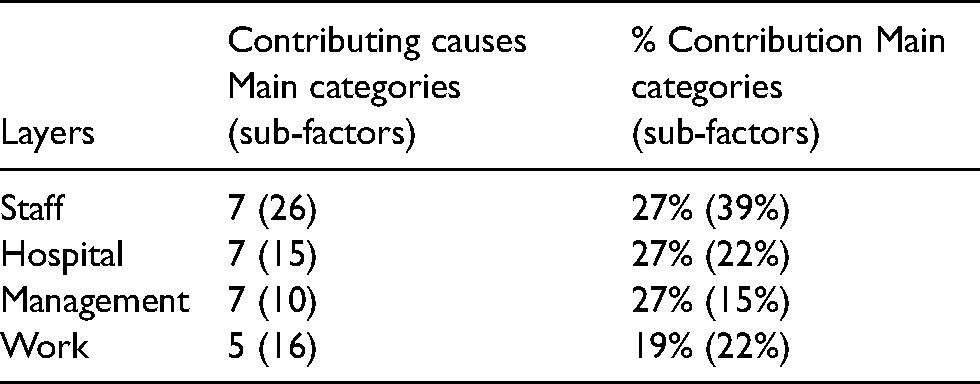
Our further analysis shows that among the internal-to-an-organization layers, the most contributing causes of URFOs have been identified across the Staff and Hospital layers (Table 2). This is based on considering a combination of the number of main categories and sub-factors.
Distribution of contributing causes of URFOs across the internal-to-an-organization layers of the AcciMap framework (layers are listed based on percentage of contribution).
From another perspective, it is noteworthy that although the number of captured factors across each layer of the AcciMap framework implies the complexity of socio-technical, including cultural, issues at a given layer, that number might not be 100% correlated with the overall contribution of the key player(s) associated to that layer. For example, external-to-an-organization layer may have fewer number of contributing causes (Table 1), but targeting just one of them (e.g. national URFO reporting requirement) may have a larger overall impact than targeting multiple of the causes at a lower layer. Some adjustments from government and regulatory bodies’ side could drive multiple improvements at the hospital level as well. Furthermore, (cultural) improvements made in the hospital level can impact and improve plans of management as well as actions and decisions of all personnel.
Another important characteristic of the AcciMap framework is illustrating the interactions between different involved key players, which are represented in the layers of the framework. Captured factors in each layer project on lower layer(s) and the arrows in the AcciMap framework (Figure 3) illustrate the relationship between captured contributing causes and the way they are combined to produce the final negative outcome. In this way, following the arrows upward in the diagram enables us to uncover why each of the factors emerged 25 and how those contributing causes interrelated with each other. The described upward tracking depicts several paths through which, captured contributing causes are connected together from the lowest layer of Work to the topmost layer of Government and Regulatory Bodies. For instance, one of the contributing causes of the “equipment/technology risk factors and limitations” in the Work layer is “insufficient working knowledge” from the Staff layer. That factor itself is under the influence of “inadequate training planning and implementation” from the Management Layer. This issue can be caused due to “inadequate training infrastructure” in the Company (Hospital) layer, and one of the reasons of inadequate training infrastructure could be “financial and budget constraints” in the same layer.
It is noteworthy that some of the decisions or actions of the Staff layer could directly contribute to a URFO case without impacting the layer of Work, as those decisions can be immediate triggers of the negative outcome. For instance, inadequate time-out, under the main category of disregard to OR policies and procedures, can be an immediate contributing cause of an unintended retained foreign object.
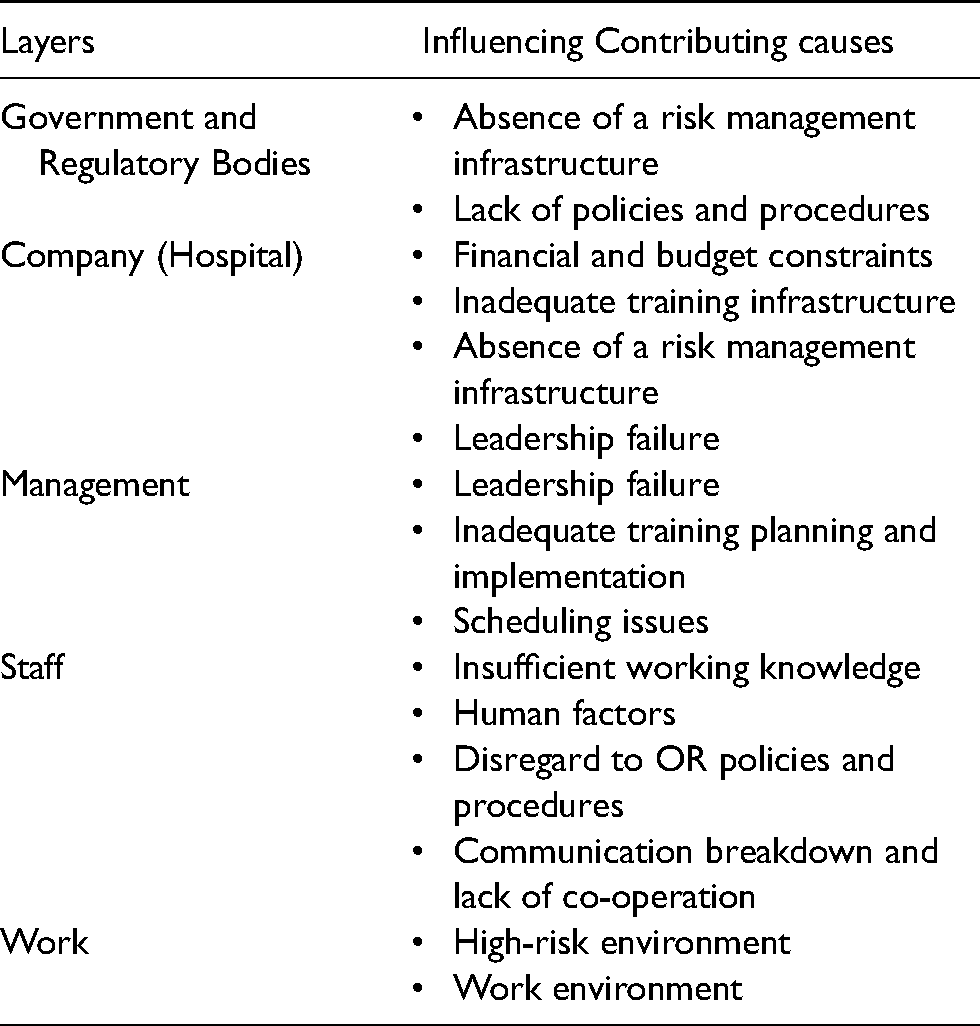
We performed the described upward tracking analysis for the entire developed AcciMap framework in Figure 3 to identify the most influential contributing causes of URFOs across each layer of the framework. In this analysis, the number of outgoing arrows from each node (captured factor) as well as its indirect impact on lower-level elements through intermediate nodes is a representation of the node influence. In the layer of Staff, since as discussed above, Staff-related decisions and actions can either directly or through impacting the layer of Work contribute to URFO cases, only considering the number of outgoing arrows from each node in this layer can be misleading. Therefore, we considered a combination of the number of outgoing arrows from each node in the Staff layer and the number of sub-factors captured under each main category (node) in this layer. Finally, for the layer of Work, as it is the lowest layer, there are no outgoing arrows from those factors captured in this layer. Hence, we only considered the number of captured sub-factors under each main category. We also asked our subject matter experts regarding the critical status of each captured factor. The stated results in Table 3 depict the most influential contributing causes of URFOs in each of the five illustrated layers of the developed AcciMap framework.
Most influential contributing causes of URFOs across each of the acciMap layers.
Furthermore, the analysis of the AcciMap framework indicates that organizational factors, among internal factors, were the root contributing causes of URFOs. Organizational factors such as personnel management issues; i.e. inadequate training infrastructure, economic pressure (trade-off between safety and production), procedural issues, and issues in communication have also been identified as major contributing causes of accidents in other safety-critical industries such as nuclear power, aviation, and transportation sectors. For instance, inadequate communication was stated as one of the main contributing causes of the Three Mile Island nuclear meltdown.67,68
As described in the Results section, for the development of our proactive risk assessment framework, we integrated the 10 traits of a positive safety culture with the AcciMap framework, which systematically captured and analyzed the contributing causes of URFOs across its hierarchical layers. This integration, which was illustrated in Figures 4(a) and 4(b), enabled us to identify instances of weak safety culture and understand the consequences of that on OR operations. We also evaluated the level of influence of each of the 10 traits of a positive safety culture based on the number of contributing causes of URFOs that it has impacted, i.e. the number of captured factors under the column of each trait in Figures 4(a) and 4(b). Our analysis shows that the most instances of violations were identified across four safety culture traits: Work Processes, Leaderships Safety Values and Actions, Effective Communication, and Continuous Learning. The details of this analysis have been presented in Table 4. This provides necessary information to healthcare practitioners to focus on those traits that contribute the most to improving safety culture, patient safety, and reducing instances and risks of URFOs.
Distribution of the contributing causes of URFOs across the 10 traits of a positive safety culture.
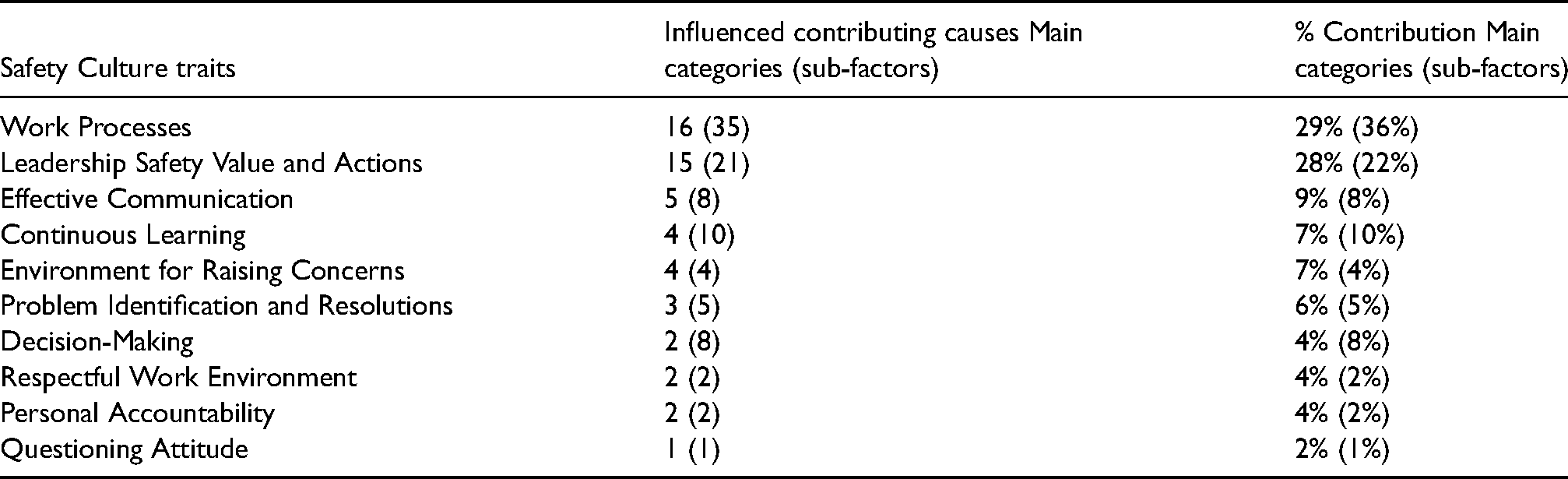
As Table 4 shows, the first two traits of Work Processes and Leaderships Safety Values and Actions had a much higher impact compared to the next two listed traits. We first had the intention to identify the three topmost influential traits of a positive safety culture. However, since the two traits of Effective Communication and Continuous Learning were very close as far as the amount of influence, we listed four traits instead of three. On the other hand, we stopped at listing the first four traits even though the fifth traits of Environment for Raising Concerns was also close to the third and the fourth ones for the purpose of more concentrated recommendations based on fewer identified traits with the highest influence. Some of our recommendations, however, have addressed the other traits of a positive safety culture (e.g. the sub-section "Recommendations to improve leadership safety value and actions" provides recommendations to create an environment in which raising safety concerns is possible).
In this phase of our analysis, we also consulted with our aforementioned subject matter experts to verify our findings as far as the identified most influential traits of a positive safety culture in our context. There were agreements as far as the first two identified traits; especially the essential role of leadership in creating and promoting safety culture was emphasized. In addition, the critical role of effective communication and creating an infrastructure to reduce disconnects, unclarities and miscommunications, as a leading cause of medical errors, was highlighted. To our experts, several of the other traits including continuous learning, environment to raise concerns, personal accountability, and questioning attitude were all important. Therefore, since we wanted to list the four topmost influential traits, we decided to follow our analysis based on the number of URFOs contributing factors that were influenced by each trait, as described before and listed in Table 4. However, as stated before, some of our developed recommendations in the next section have also addressed the other traits of a positive safety culture.
Based on all the stated analyses in this section, we have developed some recommendations to improve the safety of operations in the healthcare industry, enhance patient safety, and reduce risks of URFOs in operating rooms.
Recommendations
The stated recommendations in this section can be categorized into two main groups: 1) recommendations to regulatory agencies, as external factors outside the boundary of a hospital and 2) recommendations to hospitals, which are categorized as internal factors. Based on our analysis in the previous section, we realized that Work Processes, Leaderships Safety Values and Actions, Effective Safety Communication, and Continuous Learning are the most frequently violated traits among the 10 aforementioned positive safety culture traits in the URFO cases investigation. We have a separate sub-section for each of these four traits of a positive safety culture including recommendations to both government & regulatory bodies and hospitals to improve the status of that trait.
Recommendations to improve work processes
There is a need to improve regulatory infrastructures in the healthcare industry. One of the aspects of this improvement is related to more established policies and procedures. Government and regulatory bodies need to develop standard protocols for critical procedures, such as counting of surgical instruments. In addition, they need to develop requirements for standardized layout of operating rooms. From the hospitals perspective, they need to improve work processes and its root contributing organizational factors. A major area in this regard is improving procedural issues by establishing standard operating procedures, such as count policies, and uniform documentation of the count process across all procedural areas.
Establishing a robust risk assessment infrastructure by hospitals is another area that can contribute to improving work processes in healthcare settings. Developing a system-based risk management program to holistically assess the safety of operations in hospitals, operating rooms specifically, is of paramount importance. This program needs to be equipped with effective methods to (proactively) identify and evaluate risks of medical errors, URFOs specifically. This will also contribute to improving the Leadership Safety Values and Actions aspect/trait of a positive safety culture.
Recommendations to improve leadership safety value and actions
Government and regulatory bodies need to develop a systematic risk management infrastructure to effectively assess risks of medical errors and improve safety of operations in the healthcare industry. Moreover, regulatory authorities need to improve regulatory effectiveness through incorporating regulatory reviews and approvals of safety critical points into their risk management infrastructure. This system has to enable and require reporting of medical errors and obtaining information on the patterns of underlying types of errors.
Hospitals could also improve their leadership toward safety values. Cultivating organizational culture plays a critical role in this improvement. Hospitals need to play a leading role in committing to prioritize patient safety and make that visible through their every day actions. They must commit to creating and maintaining a culture of safety. This commitment is as critical as allocating resources to generate revenue and improve productivity. Economic pressure, the productivity pressure to increase throughput, has always been an issue and a challenge in profit-making organizations. This issue can lead to compromising the safety of operations, which is even more critical in the healthcare industry as it endangers patient safety, if there is no existing balance between safety and productivity. Establishing the discussed balance can be created and/or maintained by for example incorporating equivalent number of performance measures for safety achievements compared to production and cost saving accomplishments. Maintaining a culture of safety also requires leaders to consistently and visibly support and promote those safety measures. Hospitals could provide and allocate sufficient resources to ensure that equipment and personnel are adequate to employ those safety measures. Furthermore, defining rewarding systems for safe operations can contribute to improving safety; e.g. patient safety.
Leadership toward safety values can also be improved through encouraging hospital staff to have questioning attitude regarding safety issues and by creating an environment where staff feel comfortable to raise safety concerns. This attitude can be improved if hospitals and their management create an environment that staff can work as a “team of equals”. Moreover, encouraging reporting of medical errors and implementing a system-oriented approach to conduct root cause analysis can lead to improving the safety of operations in the healthcare settings; operating rooms in this specific context. Adverse events and even near-misses need to be seen by hospital leadership as providing “information-rich” data for learning and systems improvement. In fact, a reporting culture in which people report errors and near-misses is one of the main elements of a safety culture according to James Reason. 7
Finally, hospitals and their executive managers need to allocate enough budget and financial resources to provide their personnel with not only technical trainings but also non-technical trainings; e.g. teamwork and safety culture.
Recommendations to improve effective communication
Government and regulatory bodies need to incorporate effective communication policies and procedures to ensure quality of patient care in ORs. Lack of role clarity, in the count procedure in this context, as well as lack of a clear and well-defined interaction policy between surgeon and staff in operating rooms have contributed to communication issues. Therefore, there has to be clear policies and protocols defined by regulatory bodies in this regard to ascertain effective communication of staff in ORs.
From the hospitals perspective, they need to define clear lines of communication to reduce instances of communication breakdown, which can contribute to increasing the risk of URFOs. Defining clear lines of communication during shift changes is one of the instances that is very critical. In addition, there have to be clear guidelines as far as interaction and co-operation when there is more than one surgery team in an operating room.
Designing standardized communication policies and procedures to improve interdisciplinary communication to prevent URFOs is also of paramount importance. Moreover, hospitals could design and implement standard and well-understood reporting infrastructures and protocols to reduce the risk of ineffective communication and interaction. Incorporating appropriate rewarding systems for reporting near-misses is another policy to reduce issues in communication. Finally, hospitals could develop training programs to improve operating room staff's teamwork skills to decrease instances of communication breakdown, increase co-operation among staff, reduce medical errors (URFOs in this context), and enhance quality of care including patient safety.
Recommendations to improve continuous learning
Continuous learning is a critical element to improve safety of operations and quality of care. It is also a crucial trait to improve safety culture and consequently, reduce risks of URFOs and enhance patient safety in ORs. A learning culture is also another main element of safety culture that Reason 7 introduces. In this context, providing specific trainings to personnel who deal with complex operations such as surgical count is one the involved aspects that needs to be highlighted. These trainings have to be continuously updated based on new developed policies and guidelines; e.g. to prevent URFOs. In addition, personnel need to receive training in a routine basis. Auditing trained personnel by experienced experts to make sure that they have achieved a proper level of expertise in their training is also critical to prepare them for handling complicated situations. Furthermore, integrating trainings on non-technical skills, such as human factors engineering and safety culture, into workplace procedures is another fundamental strategy that ensures continuous learning.
Not do only personnel need to receive continuous education and training, but also the acquired technology and equipment in ORs have to be updated to support medical errors reduction (URFOs in this context). For instance, the use of radio opaque sponges can help tremendously to reducing risk of URFOs, as sponges are one of the most common retained foreign objects. Moreover, hospitals can acquire more efficient diagnostic techniques to discover URFOs.
Conclusion
In this paper, we analyzed the contributing causes of the URFOs in ORs by utilizing Rasmussen's AcciMap framework, as a systematic accident investigation methodology. This methodology enables analysts to identify high-level contributing factors, which are related to organizational, governmental, and regulatory practices as well as direct contributing causes of an analyzed incident, by investigating all of the stated factors within the scope of its hierarchical structure in distinct layers. The AcciMap Methodology is a powerful tool to analyze the main contributing causes of an accident as well as the interactions of key involved decision-makers and stakeholders.
We then created an integrated proactive risk assessment framework by integrating the 10 traits of a positive safety culture, originally introduced by the nuclear industry, with our developed AcciMap methodology. The analysis of this developed framework depicted that most instances of violations were identified across the four following positive safety culture traits: Work Processes, Leaderships Safety Values and Actions, Effective Safety Communication, and Continuous Learning. This provides necessary information to healthcare practitioners seeking to focus on those traits that will contribute the most to improving patient safety and reducing instances and risks of URFOs. Finally, we belive that although this risk assessment framework was developed for the analysis of URFOs, it can be generalized and used to analyze any sentinel events in the healthcare industry.
Future Research
One of the main future research directions for this study is to perform statistical analyses (upon receipt of data) to derive more informed results as far as the importance weight for each of the captured contributing causes of URFOs in our developed AcciMap framework as well as our traits mapping on the AcciMap. At the current stage, we have assumed that all captured contributing causes have a similar importance weight. As an example to access pertinent data, certain states and insurance companies have mandated the reporting of URFOs. If those reports can be accessed, the analysis of their reported cases and their contributing causes can be used as a source to develop frequency rates and importance weights for captured factors in the AcciMap framework. Moreover, we plan to contact other healthcare facilities and hospitals to pursue a possibility to implement research findings, as a whole or in the scope of a pilot study.
Footnotes
Acknowledgement
We would like to convey our extensive gratitude to four individuals from the Office of Quality and Patient Safety at The Joint Commission: Dr Raji Thomas, the Director; Dr Edward Pollack, the Medical Director and a Patient Safety Officer; Ms. Lisa Buczkowski, the Associate Director; and Ms. Erin Lawler, a Human Factors Engineer, for their advice and guidance. In addition, we would like to graciously thank Dr Carol Peden, the Director of the Center for Health Systems Innovation at the University of Southern California's Keck School of Medicine, for her time and provided feedback. This work, however, should not necessarily be construed as their representative positions or be endorsed by them.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.