
Abstract
Background
Determining nurses’ attitudes and behaviors toward error reporting is important in providing safe, high-quality patient care. The current study aimed to test Turkish validity and reliability of the Incident-Reporting Attitude Scale for Staff in Long-Term Care Facilities.
Methods
This psychometric study was conducted in two stages with 395 nurses and nurse managers in long-term care at a university hospital between May 2021 and January 2022. First, the Turkish adaptation of the scale was performed. The scale's internal consistency was evaluated using Cronbach's alpha and corrected item-total score correlation. Content validity indices were used for content validity, and exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were used for construct validity. Discriminant analysis and internal consistency coefficient were used for reliability analyses.
Results
The results showed that the Turkish scale adaptation is adequate for language and content equivalence. According to CFA, the scale comprising 31 items and two subscales in the original version showed a significantly good fit in a 26-item and five-factor model. The Cronbach's alpha of the modified scale was 0.92; it was 0.88, 0.94, 0.82, 0.96, and 0.90 for the subscales, respectively.
Conclusions
The Turkish scale adaptation has consistently shown acceptable psychometric reliability and validity characteristics. It can be used by healthcare services and nursing managers to evaluate nurses’ attitudes toward incident reporting in healthcare facilities providing long-term care.
Introduction
Medical errors constitute an internationally important issue that threatens patient safety. The Institute of Medicine defines medical error as “an unexpected outcome caused by an unintentional disruption during the provision of medical care to a patient.” 1 The reporting of medical errors (incident-reporting) is seen as an important strategy in many high-risk industries as well as in healthcare and long-term care (LTC).2,3 The purpose of incident reporting, which indicates a positive safety culture, is to reveal incomplete or near-miss incidents, learn from mistakes, prevent future mistakes, and make the necessary arrangements.2,4 This is only achievable through adopting a positive safety culture and an appropriate reporting system. Developing a positive safety culture is essential in hospitals and LTCs since healthcare professionals in long-term care facilities face complex and difficult processes such as treating chronic diseases, rehabilitation, and palliative care. 5 And unfortunately, unintentional medical errors can occur too often during these processes.5,6 Reporting should be structured to encourage people to report errors and protect the reporting staff without revealing their identities or being punitive.2,4
In Turkey, the “Safety Reporting System” first started accepting active data voluntarily and anonymously on the 23 March 2016, and the first statistical report was published in 2017. This report indicated that 74,380 reports were submitted to the Safety Reporting System in 2016. Of these, 93.8% were laboratory errors, 1.5% were patient safety errors, 1.6% were surgical errors, and 3.1% were medication errors. 7 As can be seen from the report, the reporting of patient safety and surgical and medication errors is very low. However, the incidence rate of such errors is estimated to be higher in Turkey and has not been reported to the system. 8 More than half of the nurses in Turkey did not report any medical errors within a year.9,10 Measuring or determining nurses’ attitudes and behaviors toward medical errors can guide the arrangements to be made in reporting medical errors.
In Turkey, nurses’ attitudes and behaviors toward medical errors, the number of error reports, non-punitive responses to errors, feedback on error reporting, and hospital open communication were measured indirectly using the Patient Safety Culture Survey. 9 In Turkey, there are also national and international surveys and scales related to Patient Safety Culture.11,12 However, in these scales, medical errors were considered either under a single dimension or as a subscale of other dimensions. University hospitals in Turkey provide long-term care for chronic patients in addition to their research activities. Therefore, it may be more appropriate to use the Incident-Reporting Attitude Scale for Staff in Long-Term Care Facilities (IRA-LTC) to determine the medical error attitude of nurses and nurse managers in university hospitals in Turkey.
Nurses must report medical errors since they provide patient care services for long periods, one-on-one in complex processes, and frequently encounter errors. 13 Reporting of unwanted events by nurses reveals problems related to patient safety. Thus, the factors that cause errors to occur are identified. Efforts are made to eliminate them or prevent re-occurrence, which leads to a significant reduction in medical errors.13,14 Therefore, determining the attitudes and behaviors of nurses toward error reporting is critical in determining medical errors and taking the necessary precautions to provide safe and high-quality patient care. Accordingly, a reliable and verified instrument related to incident reporting is necessary to determine nurses’ attitudes toward reporting incidents in LTC facilities. Failure to accurately measure and identify nurses’ incident-reporting attitudes and behaviors may hinder the improvement of safety practices, patient outcomes, and staffing planning. 3
Measuring attitudes toward incident reporting is very important since it explains personnel perception, knowledge, motivation, and behavioral intention to report incidents.3,13 A positive attitude toward incident reporting can promote removing barriers to reporting errors among nurses. Therefore, this study aimed to evaluate the validity, reliability, and adaptation of the IRA-LTC developed by Lin et al. 3 in Taiwan in 2019 in a sample of Turkish nurses.
Methods
Participants and setting
A cross-sectional design was used in this psychometric study. The study sample consisted of nurses (service nurses and unit charge nurses) working in a 722-bed LTC university hospital in the Mediterranean Region of Turkey. A total of 604 nurses work in the hospital. Of these, 513 nurses who met the inclusion criteria were invited to participate in the study online. The study sample was calculated based on the information that the sample size should be at least five or ten times the number of items in validity and reliability studies. 15 Accordingly, the original scale had 31 items, aiming to reach at least 310 samples. Data were collected from 395 nurses through the online data collection form using convenience sampling. In total, 22 data forms were invalid or incomplete, and 96 nurses still needed to complete the data form. The response rate was 76.9%. The inclusion criteria were to have been working in this institution as a service nurse and unit charge nurse for at least 30 days. In the study, nurses who had been working as a service nurse and unit charge nurse for less than 30 days, nurses on maternity leave or unpaid leave at the time of the study, and nurses in senior management (head nurse and their assistants) were not included.
Data collection
Due to the pandemic, the researchers collected data via WhatsApp between May 2021 and January 2022. After obtaining institutional permission and ethics committee permission, the nurses’ WhatsApp contact information was obtained from the hospital administration. Then, the Consent Form, Personal Information Form, and Turkish IRA-LTC scale were shared in the nurses’ WhatsApp groups. The nurses who agreed to participate in the study read the consent form, completed the forms and scales after agreeing to participate, and sent them back. Completion of the data collection tools took 8–10 min.
Instruments
Personal Information Form: It consists of six questions, including sociodemographic and occupational characteristics of nurses, such as age, gender, educational level, weekly working hours, and position in the institution. One question was whether they reported incidents in the clinic where they worked.
Incident-Reporting Attitude Scale for Staff in Long-Term Care Facilities (IRA-LTC): Lin et al. 3 in Taiwan developed the IRA-LTC version to determine nurses’ incident-reporting attitudes. The study was conducted between June 2013 and March 2014 using a proportional stratified random sampling method. A total of 251 head nurses, managers, nurses, nurse aides and administrative staff who had worked more than 30 days in 20 long-term care facilities were surveyed. All questionnaires were sent via email separately to LTC facilities. The original scale initially consisted of 32 items. One item was removed because its factor loading was low. As a result, the scale was created with 31 items and two dimensions: “Cognition and Intention to Report” and “Barriers to Report.” Items of the scale are rated on a 5-point Likert system as “5 = Strongly agree, 4 = Agree, 3 = Neutral, 2 = Disagree and 1 = Strongly disagree.” Seventeen items of the 32-item scale had negative items, and their ratings were calculated inversely. Higher scores indicate a more positive incident-reporting attitude. 3 The Cronbach's alpha of the original scale was found 0.94, while it was 0.97 for both subscales.
Translation and cultural adaptation of the instrument
The steps recommended in the World Health Organization (WHO) guide (Process of translation and interpretation of instruments) were followed to ensure language equivalence and cultural equality of the original scale. 16 The application of this method includes forward translation, expert panel, reverse translation, pre-test, cognitive interview, and final version. 16 In the first step of forward translation, the original English scale was translated into Turkish by four independent linguists who were well-versed in English and Turkish. The reason for choosing four translators was to increase consistency between translations. The native language of these specialists was Turkish, and they knew the English language and culture. Instead of a literal translation, instructions were given on using conceptually equivalent meanings of sentences. An expert panel of six people consisting of Associate Professors, Assistant Professors, Lecturers, and researchers was formed to examine the scale's prospective version in detail and identify inconclusive statements. All these specialists had experience in translation and scale development. By the recommendations of experts for preserving the content integrity, the item “I think that the incident-reporting procedure is inappropriate” was revised as “I think that the incident-reporting procedure is not useful,” the item “I’m afraid that the incident report I write may cause my colleagues to act differently toward me” was revised as “I’m afraid that the incident report I write may cause my colleagues to treat me differently.” “Reported incidents should be made anonymous before they are shared with employees” was revised as “Identity information should be removed before discussing written incident reports with employees.”
The research team, familiar with both languages, examined the original version of the scale and the Turkish translations. After the review, a consensus was reached on a single Turkish translation form. The Turkish translation agreed upon by the research team was reverse-translated into English. The reverse translation was carried out independently by two experts fluent in both languages and unfamiliar with the scale's original form. The research team compared the reverse translations and agreed on a single one. The agreed reverse translation was compared with the original version of the scale, and it was determined that the items maintained semantic integrity. The agreed English translation was returned to the scale owner, who asked to compare it with the original version. The developers stated that the reverse translation of the scale had the same content as the original scale.
The scale was pretested with 25 nurses from the target population. Then, through in-depth individual interviews (cognitive questioning), their opinions were asked about whether the items were clear and understandable. As a result, “The institution must regularly supply knowledge about the reported incidents” was revised as “The institution must regularly provide information about the reported incidents.” These nurses were not included in the study sample. The final form of the scale was sent via email to the author who developed the original version to be evaluated for language equivalence. The author's approval was obtained for language equivalence.
To ensure the scale's content validity, the expert group's opinion in the nursing management field consisting of 11 people was applied. According to the technique proposed by Lawshe, 17 a minimum of 5 and a maximum of 40 expert opinions are required. All of the experts held a PhD, were well versed in Turkish (native speaker) and English, and had experience in scale validity. They were provided with information about the study. They were asked to measure the intelligibility of the items both in Turkish and English and to evaluate whether they were related to the concept and culturally consistent Item—Content Validity Index (I-CVI) and Scale—Content Validity Index—Average (S-CVI/Ave) were calculated to evaluate the content validity of the scale items and the overall scale. 18 Experts used a quadruple Likert type scale (1 = Not relevant, 2 = Slightly relevant, 3 = Relevant, and 4 = Very relevant) to evaluate the scale items. Polit and Beck determined the lower limit to be 0.78 for I-CVI and 0.90 for S-CVI/Ave. 18 As a result of the analysis, the I-CVI value of all items was calculated as higher than 0.80, and S-CVI/Ave was calculated as 0.98.
Ethical considerations
Permission was obtained from the author who developed the original questionnaire for Turkish adaptation. Institutional permission and ethics committee approval (Date: 17/02/2021; Decision no: 2021/133) were obtained to carry out the study. After the nurses were informed about the study via an online form, those who agreed to participate completed the survey after reading the consent form and checking the “I Agree to Participate in the Study” box.
Data analysis
The data were analyzed using Statistical Package for Social Sciences for Windows (SPSS) 26.0 and Analysis of Moment Structures (AMOS) 25.0 programs. The socio-demographic characteristics of the participants were summarized by descriptive analyses (number, percentage, average, standard deviation). The scale's internal consistency was evaluated using Cronbach's alpha and item-total score correlation. Content validity indices were used for content validity, and exploratory factor analysis (EFA) and confirmatory factor analysis (CFA) were used for construct validity. Discriminant analysis and internal consistency coefficient were used for reliability analyses. Principal component analysis and the varimax method were used in EFA. EFA and CFA are two types of factor analysis that can be used to identify the underlying factors or latent variables that explain the relationships between observed variables. EFA explores a variety of possible factor solutions without any prior assumptions, while CFA tests a specific factor model based on a hypothesis or theory. 19 In the EFA stage, for an item to be retained in the factor, the factor loading must be greater than 0.32. In addition, a difference of 0.20 between the primary factor and secondary factor loadings is expected. Items with insufficient factor loadings and items with a difference between the two factors were removed at this stage. 20 χ2/df, RMSEA, SRMR, TLI, and GFI were used for goodness of fit to evaluate CFA. Acceptable values for the goodness of fit values are χ2/df <3; RMSEA and SRMR < 0.8; TLI and GFI were taken as >0.9.21,22 Skewness–Kurtosis coefficients, and Kolmogorov–Smirnov test was used to check the normal distribution of the data. Accordingly, Skewnwss–Kurtosis coefficients vary between −1 and +1. The data show normal distribution since the Kolmogorov–Smirnov test is p > 0.05. Statistical significance was set at 0.05. In addition, “average variance extracted” (AVE) was calculated for the convergent validity of the items.
Results
Study group
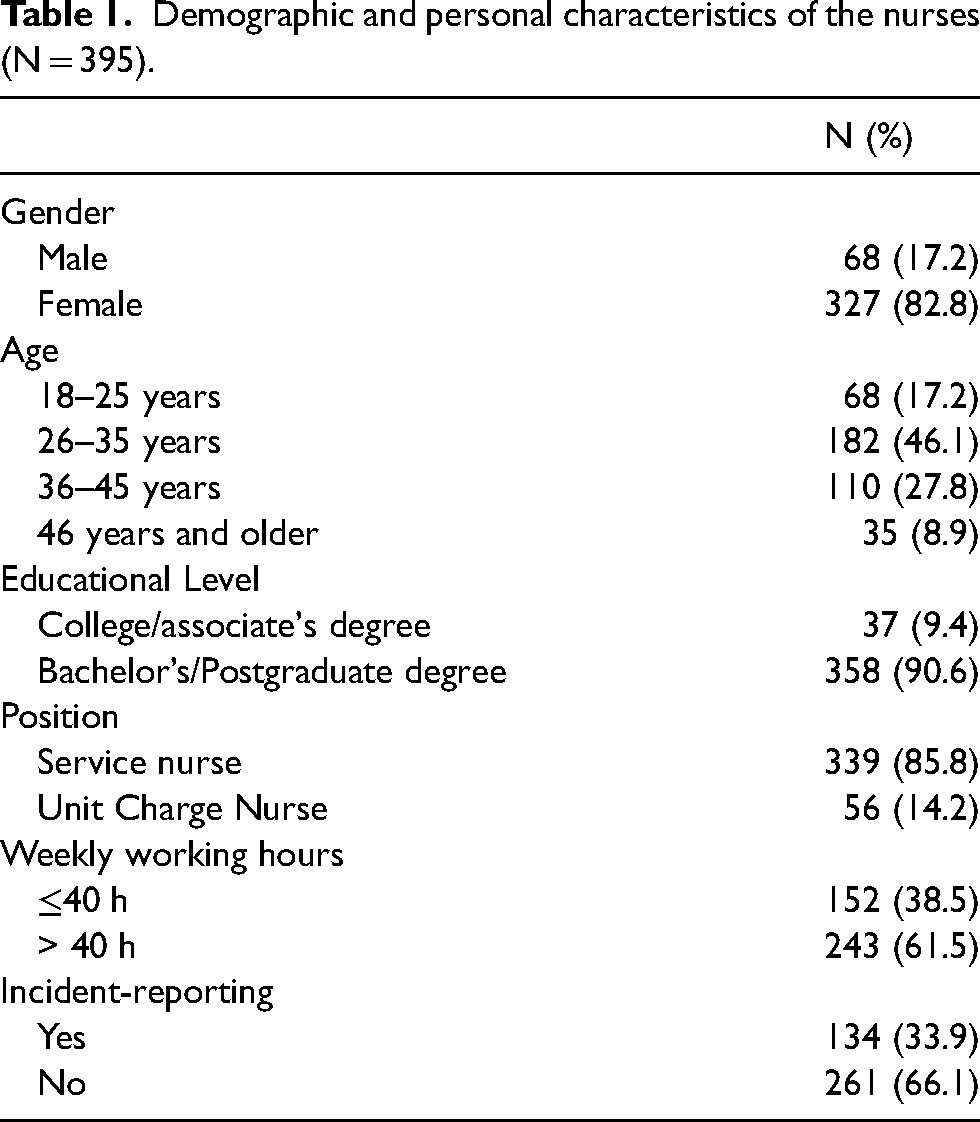
As seen in Table 1, of the 395 nurses who participated in the study, 82.8% were female, 46.1% were between the ages of 26 and 35, and 90.6% were undergraduates and postgraduates. It was found that 85.8% worked as a staff nurse, 14.2% worked as a nurse manager, and 61.5% worked more than 40 h a week. 66.1% were not found to report an incident in the unit where they were working.
Demographic and personal characteristics of the nurses (N = 395).
Validity analysis
Content validity indices were calculated to determine the content validity of the adapted IRA-LTC-TR. As a result of the analysis, all items’ I-CVI values were higher than 0.80, and S-CVI/Ave was calculated as 0.98.
Item analysis
A low correlation between an item and the item's total score indicates that the “item measures a different quality.” 23 As seen in Table 2, the corrected item-total correlation values of the scale varied between 0.53 and 0.90 (Table 2).
Cronbach's alpha coefficients and factor loadings of the IRA-LTC-TR (n = 395).
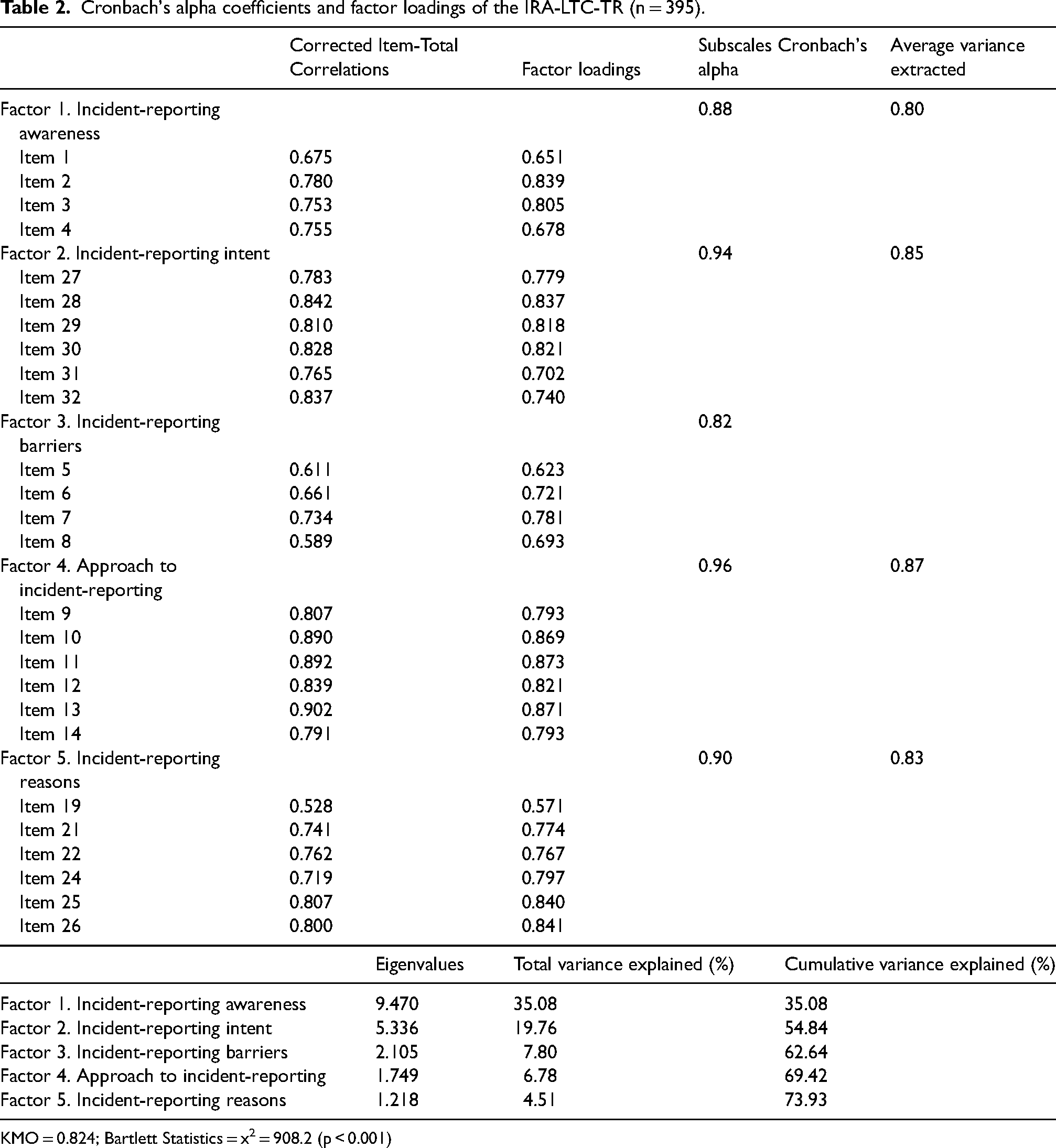
KMO = 0.824; Bartlett Statistics = x2 = 908.2 (p < 0.001)
Construct validity
Thirty-one items were included in the EFA phase. Regarding construct validity, the suitability of the data set for factor analysis is evaluated before factor analysis. 24 Accordingly, KMO and Bartlett's test was conducted to test whether the variables were correlated. As seen in Table 2, the KMO sampling adequacy test result of 0.82 indicated that the data set was suitable for EFA. Bartlett's test analysis in this study was x2 = 908.2 (p < 0.001), indicating that the sample was adequate and the data were normally distributed.
The number of factors was determined by considering the percentages of variance explained by the factors and their eigenvalues. Factors with eigenvalues above 1 were taken as the basis for interpretation, 24 and the eigenvalues of 5 factors were found to be greater than 1.25,26 The 5-factor structure with eigenvalues greater than 1 was explained with a total variance of 73.93%. An explained variance higher than 0.50 indicates the scale has “adequate” validity. 27 In the instrument, Factor 1 measured 35.08%, Factor 2 measured 19.76%, Factor 3 measured 7.80%, Factor 4 measured 6.78%, and Factor 5 measured 4.51%. A higher variance explanation indicates a better-measured concept and a stronger factor structure. 28
As a result of EFA, rotated item factor loadings were analyzed using the Varimax rotation method. In the Varimax method, rotation maximizes factor variances with fewer variables. 29 Therefore, whether the scale items were included in the expected subscales and whether they overlapped with other factors (high loading on more than one factor) was examined. Items 15, 16, 17, and 18 were removed due to multiple factors’ low factor loading difference. Item 23 (factor loading < 0.32) was removed from the scale because it indicated insufficient factor loading.
After the factor analysis stage, Factor 1 was named “Incident-reporting awareness,” Factor 2 “Incident-reporting intent,” Factor 3 as “Incident-reporting barriers,” Factor 4 was “Approach to incident-reporting,” and Factor 5 “Incident-reporting reasons” the literature. 30
As shown in Table 2, the factor loadings of the five-factor model of the Incident-Reporting Scale range from 0.57 to 0.87. The factor loading of the first factor, Incident-reporting awareness, ranges between 0.65 and 0.84 for the second factor; incident-reporting intent ranges between 0.70 and 0.84; of the third factor, Incident-reporting barriers range between 0.62 and 0.78, of the fourth-factor Approach to incident-reporting ranges between 0.79 and 0.87, and of the fifth factor Incident-reporting reasons ranges between 0.57 and 0.80.
CFA is applied to support the construct validity of the scale whose factor number is determined in the EFA stage and to test the appropriateness of the results. 28 To test whether the results obtained in EFA adequately explain the model, CFA was conducted using the SPSS AMOS Program.
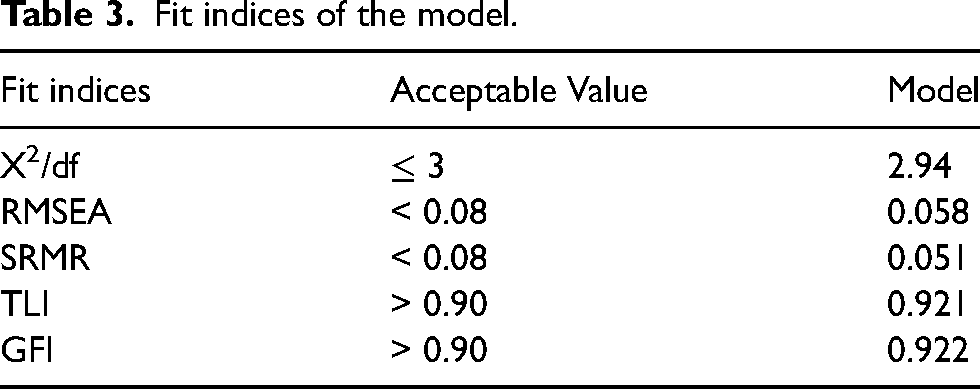
Table 3 shows the compliance indices of the IRA-LTC-TR. According to CFA results, while x2/df = 2.94, RMSEA = 0.058, and SRMR = 0.051 were found to indicate an acceptable fit, TLI = 0.921, and GFI = 0.922 were found to indicate a good fit. There was a good relationship between the items and subscales. Error variances in the subscales of IRA-LTC-TR are at acceptable levels. Covariance was not performed between the items since the correction indices were not found to be at significant load (par change < .10) (Figure 1). When the CFA results of IRA-LTC-TR are evaluated according to these criteria, 24 it can be concluded that the model indicates a good fit.
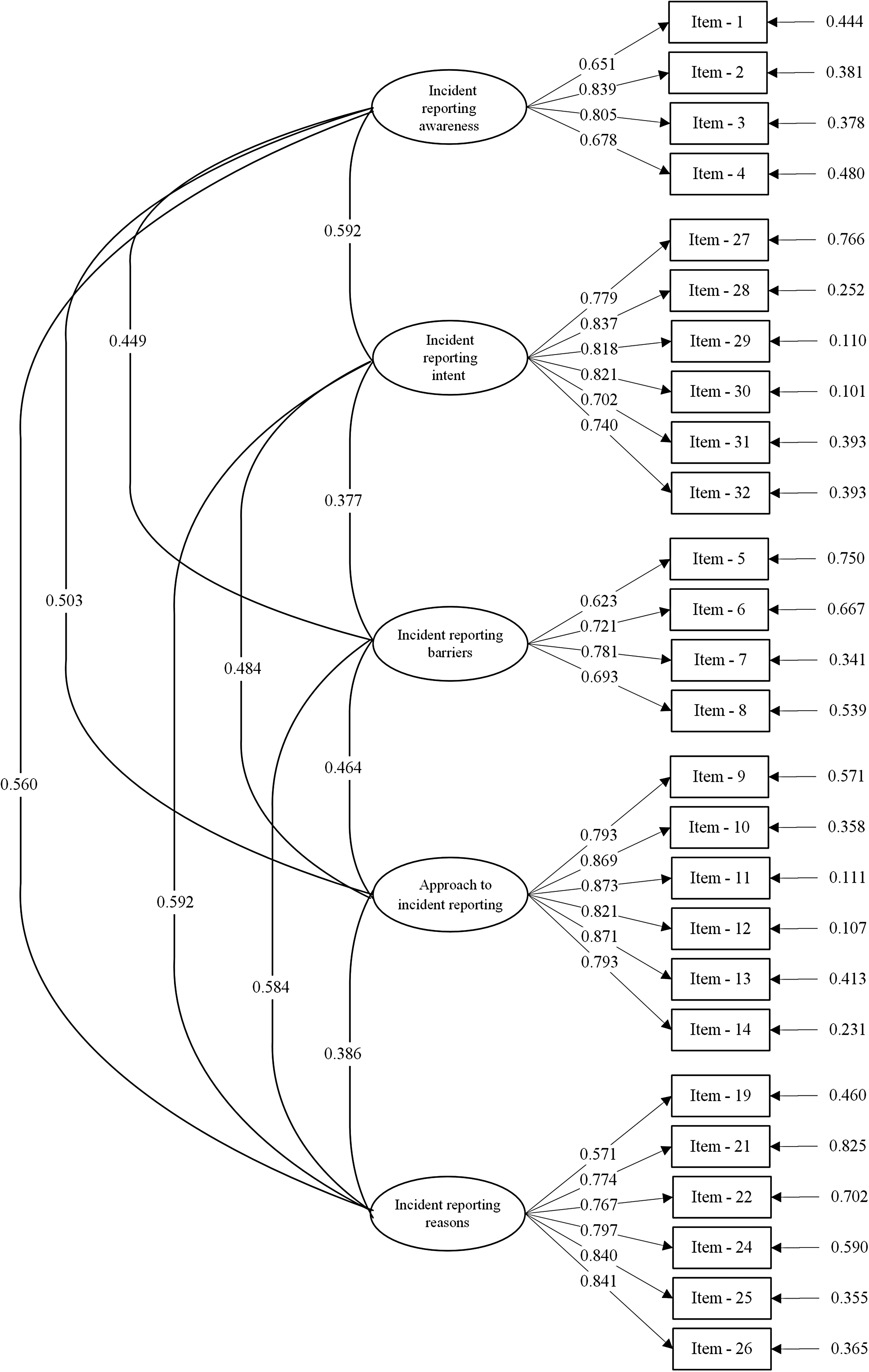
Final factor structure of IRA-LTC-Tr.
Fit indices of the model.
Reliability analysis
Reliability
Discriminant analysis was performed based on the difference between upper and lower group averages, one of the internal consistency criteria. 31 One of the lower or upper 27% groups is expected to be positive toward the attitude the scale wants to measure, while the other group is expected to be negative. For any item, both groups are expected to provide different mean scores, and this difference should be statistically significant (p < 0.001). Accordingly, the Student's t-test was used to compare the upper and lower groups. There was a significant difference between the lower group (n = 110) and the upper group (n = 110) (p < .001) for average scores of each item.
The Cronbach's alpha coefficient was found to be 0.88 for the incident-reporting awareness subscale, 0.94 for the incident-reporting intent subscale, 0.82 for the incident-reporting barriers subscale, 0.96 for an approach to incident-reporting subscale, 0.90 for the incident-reporting reasons subscale. The Cronbach's alpha coefficient was 0.92 for the overall scale. It can be seen that the internal consistency of the IRA-LTC-TR's subscales and the overall scale are highly reliable. 32 The AVE coefficient was found to be 0.80 for the incident-reporting awareness subscale, 0.85 for the incident-reporting intent subscale, 0.80 for the incident-reporting barriers subscale, 0.87 for an approach to incident-reporting subscale, and 0.83 for the incident-reporting reasons subscale. AVE coefficient of 0.5 and above indicates that it provides sufficient convergent validity. 33
Discussion
Healthcare institutions that provide LTC are vulnerable environments for medical errors since they provide service for patients with complex and chronic diseases, and multiple medical errors may occur.2,3 Determining the attitudes and behaviors of nurses and nurse managers working in these institutions toward error reporting is extremely important in identifying medical errors and taking the necessary measurements, thus providing safe, quality, and cost-effective patient care. 4 This study aimed to determine whether the IRA-LTC is an appropriate, valid, reliable, and adaptation instrument to assess the error-reporting attitudes of Turkish nurses.
The literal translation of a scale needs to be improved for use in different linguistic and cultural structures. Therefore, WHO's recommendations on the translation and adaptation of instruments have been adopted. 16 The I-CVI and S-CVI/Ave values calculated using the expert evaluations of the IRA-LTC translated into Turkish were high. In addition, the clarity and comprehensibility of the scale items were tested through pre-test application and in-depth individual interviews. The nurses did not report any serious problems with the comprehensibility of the items in the Turkish version of the scale. Only a few minor word changes were made. These results supported the successful translation process, and the IRA-LTC-TR had adequate content validity. In this study, we conducted an EFA using the IRA-LTC data from a sample of Turkish service nurses and unit charge nurses to confirm whether the original Taiwanese IRA-LTC putative factor structure applies to Turkish nurses. However, the EFA failed to confirm the original factor structure for our sample. Therefore, we modified the original scale and specified the model most appropriately for Turkish nurses.
The current study is the first to perform an EFA based on the original Taiwanese factor structure in a relatively large Turkish sample. Due to the cultural and healthcare system differences, the results suggest certain variances in the factor structures of the IRA-LTC scale between the Turkish and Taiwanese samples. Since the 5-factor and 26 items IRA-LTC-TR created by EFA shows good fit values, it should be better understood by Turkish nurses in the incident reporting process, and it will allow nurses’ attitudes toward incident reporting to be accurately determined. Since the incident reporting attitude in the new scale is discussed in five sub-dimensions as “incident-reporting awareness, incident-reporting intent, incident-reporting barriers, approach to incident-reporting, and incident-reporting reasons,” it becomes more advantageous compared to the original scale with two sub-dimensions. Because the five subscales measure different aspects of incident reporting attitude in more detail. In addition, detailed determination of nurses’ attitudes toward incident reporting with this new scale in hospitals providing long-term care will shed light on the regulations to be made in this field.13,14 The construct validity of the scale was evaluated using CFA. CFA is a model of the structural equation that indicates the relationships between items and factors. 34 According to CFA results, x2/df, RMSEA, and SRMR values indicated an acceptable fit, while TLI and GFI values indicated a good fit. 35 As stated in the method section of this study, the criteria for model fit indices are more liberal than in the previous study. 3 Therefore, we claim that there is a good model fit in this scale study. There was a good relationship between the items and subscales. Covariance was not performed between the items since the correction indices were not found to be at significant load. 23 According to the factor analysis of IRA-LTC, which consists of 31 items and two factors, “Intention to report” and “Barriers to report,” IRA-LTC-TR was confirmed to be a 5-factor structure with 26 items. 36 Items 15, 16, 17, and 18 were removed from the scale since they were overlapping, and item 23 (factor loading < 0.32) was removed due to indicating an insufficient factor loading. Subscales of the IRA-LTC-TR, named incident-reporting awareness, incident-reporting intent, incident-reporting barriers, approach to incident-reporting, and incident-reporting reasons, were created by the researchers regarding the meaning of the items by reviewing the relevant literature. 30 Written permission was obtained via email from the authors who developed the original scale for necessary changes.
The factor loadings of the five-factor model of the Incident-Reporting Scale are above 0.57. It is stated that the factor loadings for each item should be greater than 0.32.3,37 In addition, discriminant analyses have shown that each item can distinguish between those obtained the highest and lowest scores. In addition, the convergent validity results of the scale are at an acceptable level. 38
IRA-LTC-TR showed good internal consistency reliability with a Cronbach's alpha value 0.92. Values for incident-reporting awareness, incident-reporting intent, incident-reporting barriers, approach to incident-reporting, and incident-reporting reasons subscales were found to be 0.88, 0.94, 0.82, 0.96, and 0.90, respectively.
The Cronbach's alpha of the original scale was slightly higher than that of the current study, with a value of 0.94. For both dimensions of the original scale (barriers to report an intention to report), the Cronbach's alpha coefficient was 0.97. 3
Item-to-total correlation is considered for the reliability of the scale. In other words, it is calculated to what extent the item is related to the value for a measurement and the sum of all items (for each measurement). Item-to-total correlation should be above 0.5. 39 In this study, the corrected item-total correlation coefficient was above 0.5.
The current study has several limitations. The first is that IRA-LTC-TR is a self-reporting instrument. In this study, conducting EFA and CFA on the same samples can be considered a disadvantage. The inability to collect data from a second sample due to pandemic conditions constitutes the limitation of this study. Collecting information through self-reporting has limitations. People are often biased when they report on their own experiences. That is, they are more likely to report experiences that are considered to be socially acceptable or preferred. 40 However, it is widely used since it allows researchers to collect data from a wide sample in a relatively short period. Another limitation is that the sample comprises nurses in a LTC university hospital. Accordingly, the study's results cannot be generalized to other hospitals in Turkey. Future studies should further examine the factor validity of IRA-LTC-TR in other samples and a different validity and evaluate convergent validity with additional measures.
Conclusion
The current study has indicated that IRA-LTC-TR is a valid and reliable instrument for evaluating the incident-reporting attitudes of nurses working in long-term care institutions. Establishing a positive attitude toward incident reporting can help to decouple the barriers to reporting errors among the staff. IRA-LTC-TR will help Turkish healthcare organizations and nursing managers determine, evaluate, and examine nurses’ attitudes toward incident reporting. IRA-LTC-TR indicates consistently acceptable reliability and validity inferences in a sample of Turkish nurses. In this context, IRA-LTC-TR is a practical and applicable instrument that can reveal the incident-reporting attitudes of nurses in detail. In addition, to develop programs aimed at creating a positive attitude toward incident reporting and safety culture, administrations of healthcare institutions and nursing managers can use IRA-LTC-TR to identify the current situation.
Footnotes
Acknowledgment
The authors sincerely thank Shu-Yuan Lin, Hui-Ching Yang, Hui-Ying Chiang, and Shu-Li Lee for authorization to use and modify the IRA-LTC. They would also like to thank all the nurses, nurse managers, and senior management who made the study possible. This study was conducted in the first author’s institution.
Authors contributions
Study conception and design were contributed by AY, AYK, SD, and MY. Data collection by AY, AYK, and MY. Analysis and interpretation of data by AY and MY. Drafting the article by all authors. Critical revision of the article by AY and SD.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.