
Abstract
Background
Patient safety is defined as the absence of preventable patient harm. Despite significant advances, enhancing the safety of pediatric patients is of particular importance. Thus, this study aimed to diagnose the current situation of patient safety and plan, implement, and evaluate patient safety initiatives in the emergency department (ED) of Ali Asghar Pediatrics Hospital.
Methods
Two action research cycles were conducted during 2023–2024 in the ED of Ali Asghar Hospital. Participants were nurses, physicians, and medical residents. In the first cycle, actions such as providing equipment and training in patient safety were carried out. In the second cycle, handoff standardization by I-PASS and continuing staff training were implemented. Data were collected using the Hospital Survey on Patient Safety Culture (HSOPSC), semi-structured interviews, and incident reports. Quantitative data were analyzed using the T-Test, and the Wilcoxon signed-rank test. Qualitative data were analyzed using content analysis.
Results
In the first cycle, the patient safety culture score was 48.1%. After training sessions, the patient safety test score significantly increased from 65.5% to 87.83% (P < .001). In the second cycle, according to interviewees’ opinion, handoffs and in-service training were improved. The patient safety culture score increased to 62.6%, and overall patient safety perception, communication openness, staffing, handoff, and nonpunitive responses to errors significantly improved (P < .05).
Conclusion
During this study, patient safety knowledge and culture among ED staff improved. Moreover, the standardization of handoff using the I-PASS tool improved the process by comprehensive information transfer, prioritizing critical patients, and reducing information loss.
Introduction
Patient safety is one of the most fundamental components of health care services worldwide and is defined as the absence of preventable harm to patients. 1 As is estimated, one in every ten patients experienced harm from healthcare services. This number is higher in developing countries where four patients out of every 100 patients lost their lives due to unsafe practices of healthcare services. 2
One of the primary sources of preventable harm to patients is medical error, which is the third leading cause of death in the United States. Reports show that approximately 400,000 hospitalized patients experience harm during their hospitalization, and more than 200,000 patients die annually due to preventable medical errors. In addition to human costs that result from medical errors, some experts estimate that adverse events cost 20 billion dollars annually for the healthcare system in the United States. 3
Due to the distinct features of pediatric patients, such as dependence on their parents for medical care and different features of medical conditions in this population compared to adults, there is paramount effort to study harm and errors in pediatric settings.4,5 As demonstrated in a study, 616 medication errors (5.7%) were on 10 778 orders of 1120 pediatric patient admissions.5,6 Another study also shows that 1 in every 100 hospitalized pediatric patients experience adverse events, which are preventable in 60% of cases. 4 These numbers are higher in pediatric emergency, intensive care, and anesthesiology departments. 7 Some studies show that the emergency department (ED) is a high-risk setting in pediatric care, in which reports show that the prevalence of therapeutic errors is between 10% and 31%.8,9
After the Institute of Medicine's publication in 1999, there have been paramount efforts to improve patient safety. Healthcare providers use different strategies in pediatric settings to reduce preventable harm. These strategies include active error detection, improving patient safety culture, simplification and standardization of systems, involving clinicians in quality improvement projects. 10
As a result, this research used the action research method to diagnose the current situation of patient safety and plan, implement, and evaluate patient safety initiatives in the emergency department (ED) of Ali Asghar Pediatrics Hospital.
Material and methods
The current study is an action research. During this study, from June 2023 to September 2024, two cycles of action research were conducted. After fact-finding and determining the current situation of patient safety challenges in the diagnosis phase, participants suggested solutions in each cycle's planning phase to improve patient safety in the ED of Ali Asghar Children's Hospital and solve the challenges. Then, in the action phase, selected strategies were implemented, and the results were monitored in the evaluation phase.
Study setting and participants
This action research was conducted in the ED of Ali Asghar Children's Hospital in Tehran. Based on the characteristics of action research, this research was not conducted on the sample population but with their cooperation and participation. The participants included nurses, physicians, and medical residents who have at least one year of work experience in the ED and give written consent to participate in the project. The number of participants was 30 people, including 18 nurses, 6 medical residents, and 6 physicians in the ED.
Study procedure
Cycle 1 of the action research
Diagnosis phase of Cycle 1
The first action research cycle began with a meeting between the research team and participants to determine and prioritize the stakeholders, understand the power relation between stakeholders, conduct force field analysis, and define role descriptions.
Then, in the diagnosis phase of the first cycle, to reveal the patient safety challenges and understand the baseline status of patient safety in the ED, we used semi-structured interviews, a Hospital Survey on Patient Safety Culture (HSOPSC), and the hospital's voluntary error-reporting system.
Planning phase of Cycle 1
In the next step, during the planning phase, formal meetings were held between participants, hospital administration, nursing supervisors, and the research team to prioritize the existing challenges and provide strategies to correct them. Expert panels were held to prioritize the suggested strategies. Five interventions selected include providing necessary medical equipment, increasing nursing staff, patient safety education, standardizing inter-shift handoffs, and redesigning the hospital's error reporting system.
The first suggested intervention was providing necessary medical equipment for the ED. Based on the diagnosis phase, there was a shortage of medical equipment in the ED, including vital sign monitoring equipment, standard hospital beds, standard transport hospital stretchers, etc.
The second suggested intervention was increasing nursing staff. The diagnosis phase revealed a significant shortage of nursing staff in the ED, with the nurse-to-bed ratio at 1 to 6, highlighting the urgent need for more staff.
The third intervention was patient safety education for ED staff. As suggested by the nursing supervisors, e-learning methods, including online webinars, offline educational content (Infographics, documents, reminders, etc.), social media content creation, and face-to-face education were implemented.
The fourth suggested intervention was the standardization of inter-shift handoffs using I-PASS mnemonic forms and educational materials for pediatric residents and nurses.
The fifth suggested intervention was redesigning the hospital's error reporting system. Using new physical forms for error reporting and developing online electronic error reporting forms were suggested.
Providing the equipment, staffing, and patient safety training was chosen for the first cycle of action research, and an implementation plan was designed.
Action phase of Cycle 1
During the action phase, the Head of the ED, in companion with the hospital administration and the patient safety officer of the ED, determined the list of equipment needed by the ward. With the cooperation of the hospital management, the lack of medical equipment was solved. Also, the recruitment calls for new nursing staff for the ED were distributed in cooperation with the pediatric nursing department of Iran University of Medical Sciences, and six nursing staff were added to the hospital. Also, patient safety training with a new approach began with three 3-h online webinars about principles of patient safety. The first webinar covered subjects that included general aspects of patient safety, a review of existing ideas and theories on how errors occur, types of errors, root cause analysis (RCA), and systems theory on errors. The second webinar covered the principles of safe handoffs, I-PASS and ISBAR standards for handoffs, and principles of hospital infection control. The third webinar covered medication safety, medication administration steps, possible errors, and strategies to improve medication safety. Subjects of each webinar were announced one week before them, and a pretest evaluation was conducted before the start of training. After finishing the online webinars, offline content related to the webinar outline was distributed in health care providers’ groups in messengers and posted on the hospital's social media channels. Also, these contents were printed as posters and distributed in the ward.
Evaluation phase of Cycle 1
In the evaluation phase of the first cycle, which continued with diagnosis and planning phases of the next cycle, After finishing online and offline distance learning and face-to-face training of patient safety principles, a post-test evaluation was conducted, and the quality of virtual learning was assessed.
Cycle 2 of the action research
Diagnosis and planning phase of Cycle 2
During the meeting between the research team and participants, the measures taken were evaluated positively, and the possible obstacles to implementing the following steps were discussed and investigated. As a result, measures including training participants in patient safety principles focused on handoff and transitions continued. Standardization of inter-shift handoff and redesigning the patient safety incident reporting system were selected to be carried out in the next cycle, and an implementation plan was designed.
Action phase of Cycle 2
During the action phase of the second cycle, the standardization of medical resident inter-shift handoffs with I-PASS mnemonic printed forms was conducted, and handoff education for nurses and medical residents continued with online and offline virtual learning. The printed forms were available to medical residents, and an online group on social media was created to discuss the quality of handoffs and provide complementary educational information. Also, the chief resident of each shift should complete a checklist to give more details about handoffs.
The hospital's incident reporting system was redesigned, including introducing a new error reporting form format and providing an online electronic version of this form.
Evaluation phase of Cycle 2
Finally, in the evaluation phase of the second cycle, we used semi-structured interviews, the HSOPSC, and the hospital's voluntary error-reporting system. We also investigated the written forms of I-PASS and the self-reporting checklist for the quality assessment of handoffs.
Data collection
In the diagnosis and evaluation stages of both cycles of action research, data were collected by HSOPSC, the voluntary incident reporting system, semi-structured interviews, patient safety knowledge pre- and posttest, Questionnaire of Opinions about the quality of the virtual course, and a Checklist (I-PASS Handoff quality checklist).
Hospital Survey on Patient Safety Culture
The HSOPSC was designed in 2004 by the Agency for Healthcare Research and Quality (AHRQ). This questionnaire measures composites of patient safety culture. The mean percentage of positive answers to each composite's items calculates the questionnaire's final scoring. The reliability and validity of the Persian version of HSOPSC were investigated, and Cronbach's alpha was found to be between .61 and .81. 11
Voluntary patient safety incident reporting system:
Reports were gathered and separated based on the site of occurrence and classified based on International Classification for Patient Safety (ICPS). 12
Semi-structured interviews
Individual interviews were conducted in the diagnosis phase of the first cycle to demonstrate patient safety challenges and in the evaluation phase of the second cycle to assess the effects of action research in ED. The topic guide for each interview was developed based on literature reviews and expert opinions.13–16 The interviews were recorded after the participants’ written consent and transcribed verbatim. We reached theoretical saturation after 12 in each interview.
Patient safety knowledge pretest and posttest:
The 20-question test was designed with the opinion of the hospital's research committee and patient safety experts before and after the patient safety webinars.
Questionnaire of opinions about the quality of the virtual course
After patient safety distance learning in the first action research cycle, a 12-question questionnaire with a 5-point Likert scale was used to measure the quality of education. The validity and reliability of the questionnaire were established earlier, 17 and although the reliability was calculated again, Cronbach's alpha was found to be .91.
Data analysis
To analyze the quantitative data descriptive and analytical statistics were used in SPSS (v.25), and interviews were analyzed by content analysis in MAXQDA 2022.
Comparing the results of HSOPSC before-and-after-action research, after evaluating the normality of the data with the Kolmogorov Smirnov Test in SPSS, the Wilcoxon signed-rank test was used. To compare the pretest and posttest results of patient safety knowledge, the T-test was used in SPSS(v.25).
Results
This study was two cycles of an action research project, with 30 healthcare providers participating from June 2023 to September 2024: 18 nurses, 6 medical residents, and 6 physicians participated.
Diagnosis phase of Cycle 1
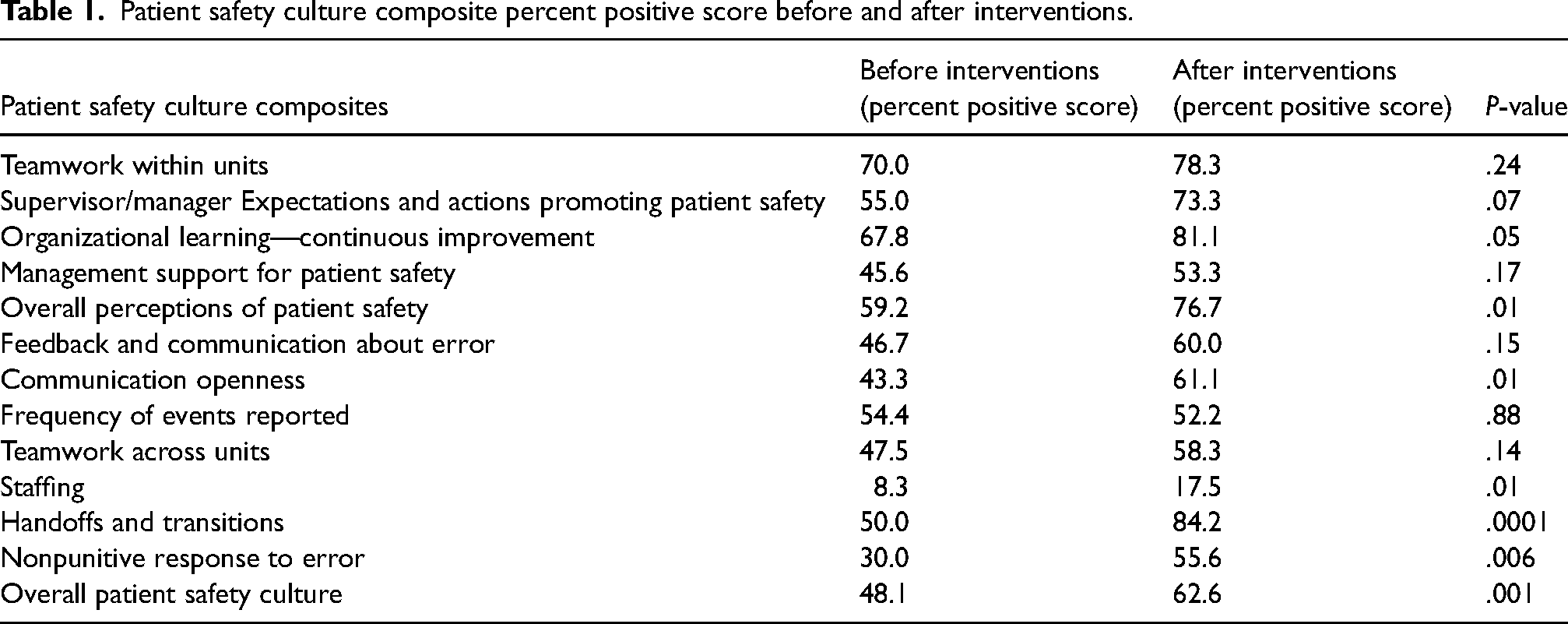
The final response rate of HSOPSC was 100%. After calculating the percentage of positive scores of each item and composite, the overall patient's safety culture score was also calculated. Among patient safety culture composites, staffing (8.3%), nonpunitive response to error (30%), communication openness (43.3%), management support for patient safety (45.6%), feedback and communication about error (46.7%), teamwork across units (47.5%), handoffs and transitions (50%) have lowest percent positive scores. The overall positive score of patient safety culture in the ED was 48.1%. (Table 1)
Patient safety culture composite percent positive score before and after interventions.
After analyzing the hospital's voluntary incident report system, 11 incidents were reported from June 2022 to May 2023. Based on ICPS classification, 10 medication/IV fluid incidents (83.33%) and 2 documentation incidents (16.66%) were reported.
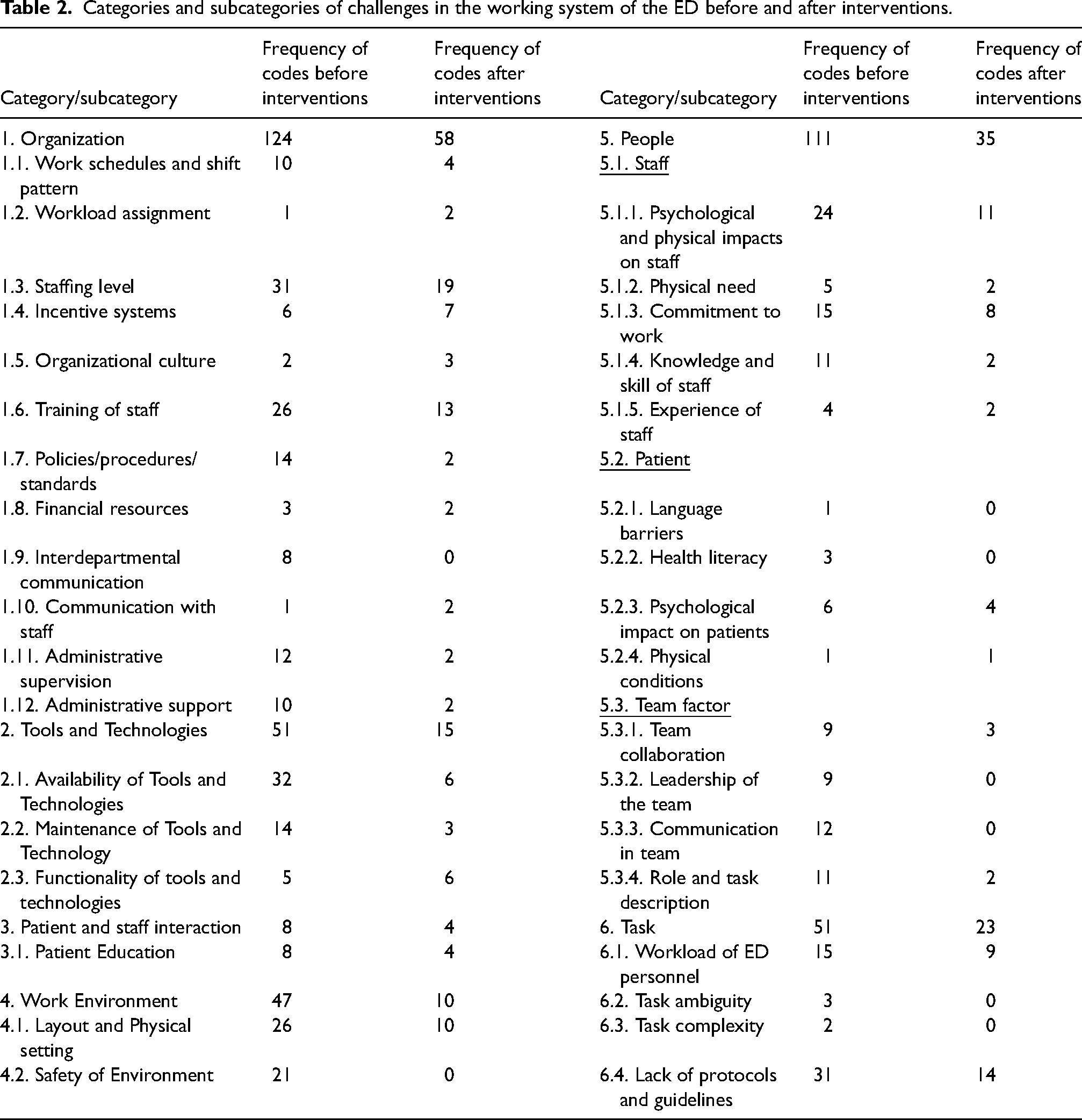
Content analysis was performed to analyze individual interviews. An integrated approach was used to code the data. Developing categories and subcategories was done based on the system engineering initiative for the patient safety model (SEIPS) and Charles Vincent's framework.18,19 Based on each category and subcategory frequencies, the main work system challenges of the ED from the healthcare providers’ view were the availability of tools and technologies (32 codes), lack of protocols and guidelines (31 codes), staffing level (31 codes), training of staff (26 codes), and layout and physical setting (26 codes). (Table 2)
Categories and subcategories of challenges in the working system of the ED before and after interventions.
Evaluation phase of Cycle 1 and diagnosis phase of Cycle 2
After the distance learning of patient safety principles, the quality of the virtual course was measured, and participants’ patient safety knowledge was assessed by pretest and posttest to evaluate the actions taken and plan for the actions of the next cycle.
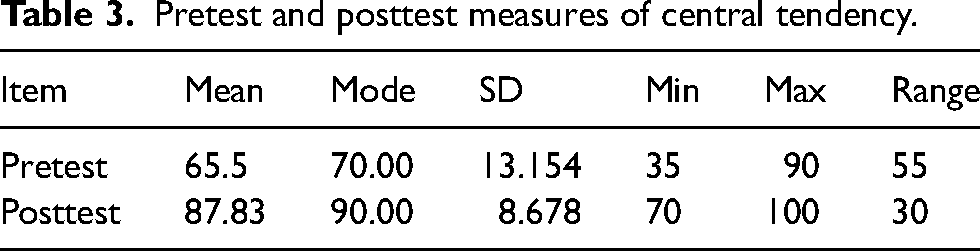
Patient safety knowledge mean score was increased from 65.5% in the pretest score to 87.83% in the posttest score (Table 3), which was significantly improved (P-value <.001).
Pretest and posttest measures of central tendency.
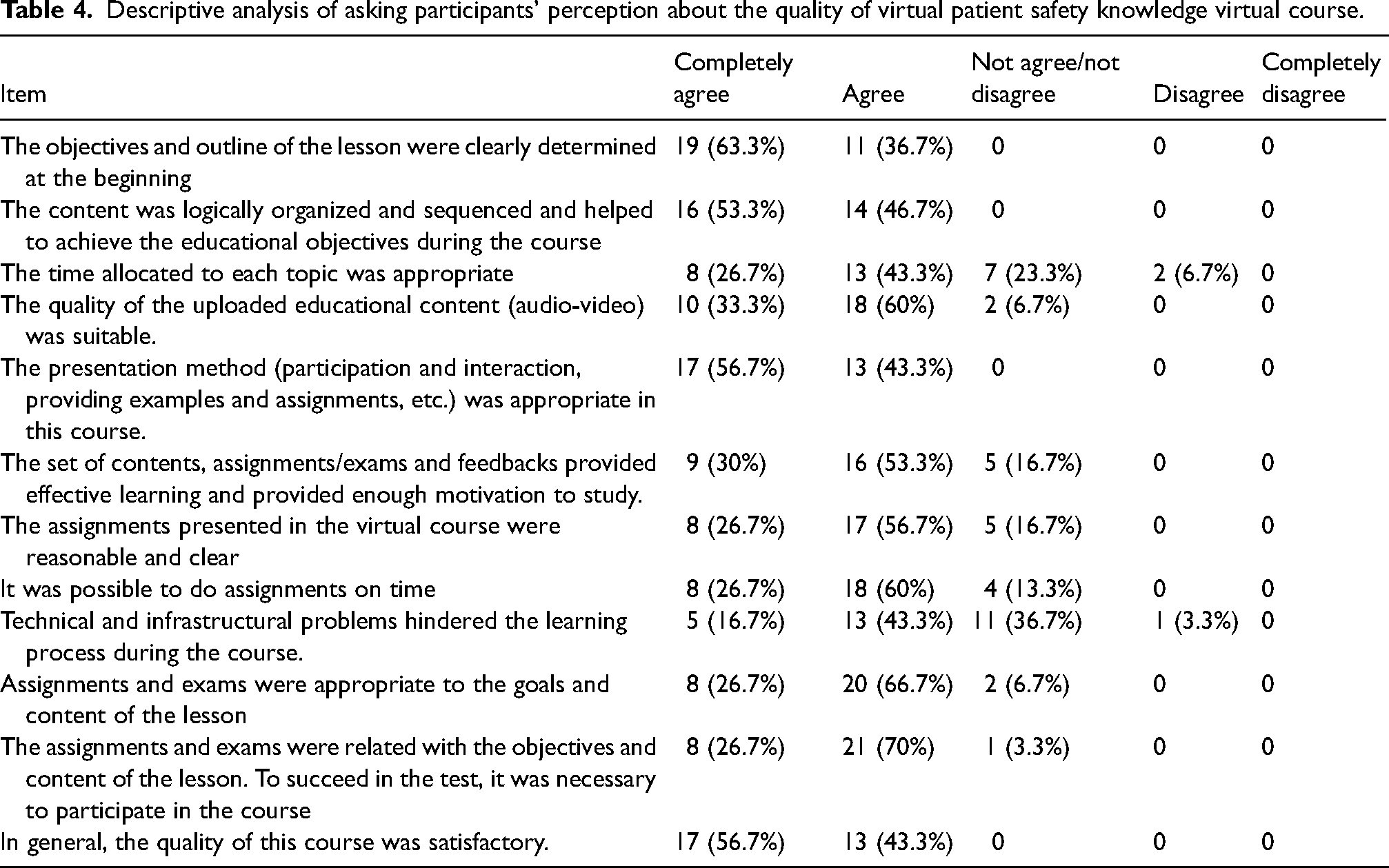
The attendance rate in each patient safety seminar was 93.33% for the first session and 96.66% for the second and third sessions. Based on the quality of the virtual course questionnaire, 56.7% of participants were very satisfied, and 43.3% were satisfied with the quality of the virtual course (Table 4).
Descriptive analysis of asking participants’ perception about the quality of virtual patient safety knowledge virtual course.
In addition, in the formal meeting between the research team and participants, the overall perception of healthcare providers about the action research project and the effect of interventions in the first cycle was positive. Based on the positive overall effect of interventions, the participant decided to continue the action research cycle by standardizing inter-shift handoffs and redesigning the hospital's incident reporting system. Training in patient safety principles also continued as it was recommended by the participants with minor adjustments.
Evaluation phase of Cycle 2
After implementing the I-PASS bundle for inter-shift handoff standardization and redesigning the hospital's incident reporting system, the HSOPSC questionnaire was redistributed 12 months after the first assessment. (3 months after finishing the interventions) After every shift, the chief resident completed a self-reporting quality checklist of medical residents’ handoffs. Semi-structured interviews were conducted to evaluate intervention effects from the participants’ view and find remaining patient safety challenges in ED.
Reassessing patient safety culture 12 months after measuring baseline scores with a 100% response rate revealed that staffing, frequency of events reported, management support for patient safety, nonpunitive response to error, teamwork across units, feedback, and communication about error have the lowest percent positive scores. The overall positive scores for patient safety culture significantly increased to 62.6%. (P-value = .001) Also, overall perceptions of patient safety (P-value = .013), communication openness (P-value = .017), staffing (P-value = .017), handoffs and transitions (P-value < .001), and nonpunitive response to error (P-value = .006) were significantly improved (P-value <.05) (Table 1).
From June 2023 to May 2024, 21 patient safety incidents were reported in the ED, 15 medication/IV fluid incidents, and 6 documentation incidents. Compared with the same period before starting the project, the number of reported incidents increased by 90.9%.
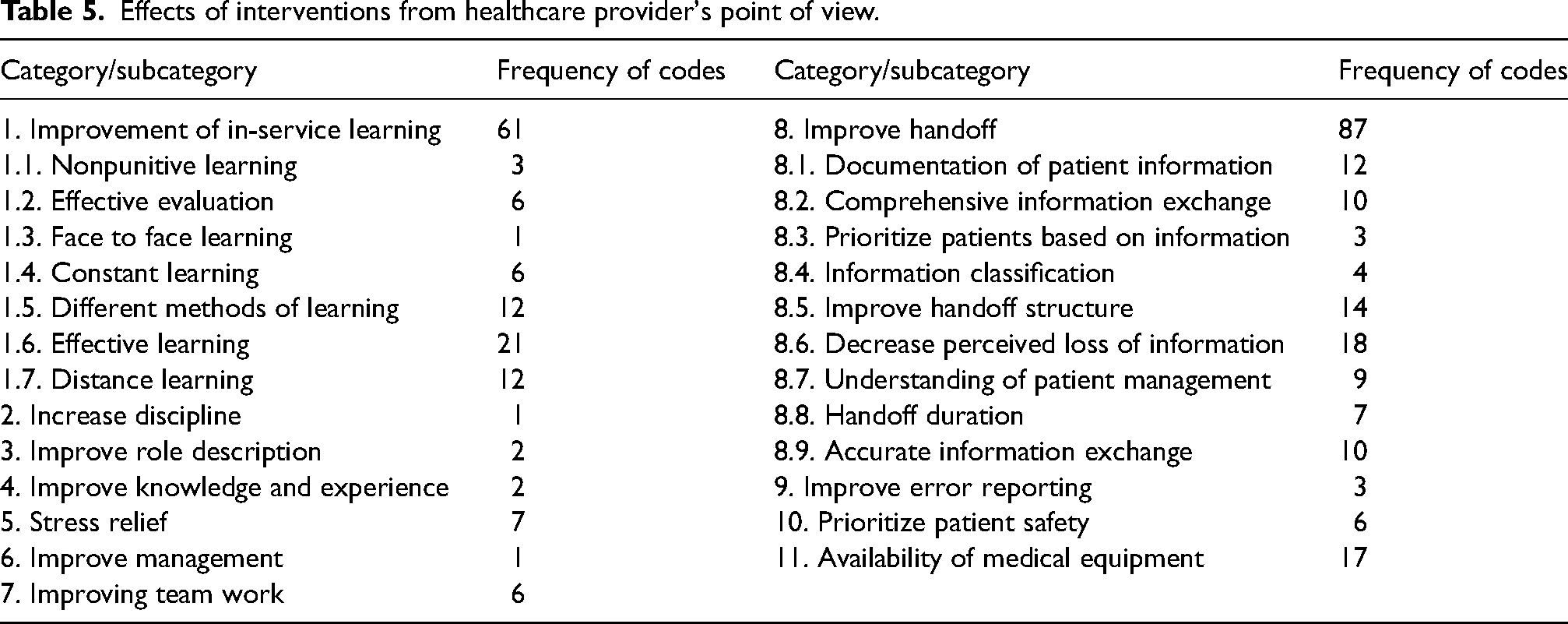
After content analysis of interviews, In order to determine intervention effects, main categories were assigned. Improve inter-shift handoff (87 codes), improve in-service learning (61 codes), availability of medical equipment (17 codes), and stress relief (7 codes) were the main effects of interventions in healthcare providers’ view. Effective in-service learning (21 codes), decreased perceived loss of information (18 codes), improved handoff structure (14 codes), use of different learning methods (12 codes), and documentation of patient information (12 codes) were major subcategories of the intervention's effects. (Table 5)
Effects of interventions from healthcare provider's point of view.
Also, the SEIPS model and Charles Vincent framework were used to determine categories and subcategories to find the remaining patient safety challenges in the ED. Low staffing level (19 codes), lack of protocols and guidelines (14 codes), staff training and education (13 codes), psychological and physical factors (11 codes), and the physical environment of the ED (10 codes) were the main remaining challenges (Table 2). Also, the overall perception of interviewees of the action research project was positive.
Analyzing Self-report forms of inter-shift handoffs showed that, in 45 days, clinical information of 283 patients was recorded on I-PASS written handoff forms. In 82 shifts (91.11%), I-PASS handoff tools were used besides verbal handoff. The mean handoff duration was 24.77 min (SD = 3.16). Handoff quality, in the opinion of medical residents, was very good in 63 inter-shift handoffs (70%) and good in 15 inter-shift handoffs (16.66%).
Discussion
This study was conducted from June 2023 to September 2024. As results indicated, after implementing interventions including a patient safety education course, providing medical equipment for ED and standardization of inter-shift handoff with the I-PASS tool, patient safety knowledge of ED healthcare providers, and patient safety culture in ED were significantly improved. Also, overall perceptions of patient safety, communication openness, staffing, handoffs and transitions, nonpunitive response to error were significantly improved. In the participants’ view, effective in-service learning decreased perceived loss of information, improved handoff structure, used different learning methods, and documented patient information, which were major effects of the project on their daily work.
Prior studies established the effect of patient safety educational programs on the patient safety culture of healthcare providers. Agbar et al., in a systematic review, evaluated the cumulative effect of patient safety educational intervention on healthcare professionals’ overall patient safety culture. They showed that 4–36 months after educational interventions, the mean score of overall patient safety culture and the mean percentage of positive responses were improved significantly. 20 Also, Lassoued et al. showed that after educational interventions, including self-learning content and workshops on patient safety and quality improvement for obstetric unit providers, eight dimensions of patient safety culture were improved significantly. 21 Jamshidi et al. also demonstrated in a randomized clinical trial that problem-based learning education in eight sessions can significantly improve knowledge, attitudes, and perceptions of the nursing students about patient safety. 22 These results are consistent with the results of the current study which show that educational interventions can improve patient safety knowledge and culture.
The handoff structure improved after using the I-PASS handoff tool for medical residents, and there was a significant decrease in perceived loss of critical information during handoff in the medical residents’ opinion. This tool was used in 91.11% of inter-shift handoffs, and after finishing the project, using the tool became routine for medical residents. In a quality improvement project at a tertiary oncology hospital, Franco et al. demonstrate handoff improvement by implementing the I-PASS tool. After using I-PASS as a standardized tool for inter-shift handoffs, the usage rate of I-PASS increased from 23% to 72%, significantly improving. In the healthcare provider's opinion, handoff efficiency, quality, and effectiveness of the tool were satisfactory. 23 Soares et al. also showed in a prospective intervention study that educating healthcare providers with online sessions about the I-PASS tool and using it in order to standardize handoffs, improve relevant information delivered, and lead to attention and focus during handoffs and improve objectivity and efficiency of handoffs 24
Despite paramount efforts to improve the staffing level of the ED and recruit six new nurses in a hospital, from the healthcare provider's view, Low staffing level and high workload are the most critical remaining patient safety challenges that this project can only solve partially. As demonstrated by Banda et al., in nurse's opinion, a high nursing workload negatively affects the quality of care to critically ill patients and affects patient safety. 25
Due to the nature of the action research method, the research results are limited to where the research was conducted (ED of Ali Asghar Pediatrics Hospital). Other researchers can use the research method of this study to improve patient safety in their departments. Also, because of the time limitation of each cycle, patient safety challenges, including staffing level, lack of protocols and guidelines, psychological and physical factors of staff, and the emergency department's physical environment, remain the emergency department's main challenges. It is recommended that other researchers use this method to solve remaining challenges and diagnose probable existing challenges that were missed in this research.
Conclusion
According to this research, training on patient safety principles improved patient safety knowledge among ED staff and promoted a culture of patient safety. Also, from the participant's point of view, standardizing the patient handoff process using the I-PASS tool led to an improvement in information transfer and classification.
Due to the nature of the action research method, the research results are limited to where the research was conducted (ED of Ali Asghar Pediatrics Hospital). Other researchers can use the research method of this study to improve patient safety in their departments.
Footnotes
Acknowledgments
We want to thank the Iran University of Medical Sciences and Ali Asghar Hospital staff for contributing to this action research.
Consent to participate
All participants provided written informed consent prior to participation in the study. Also, respondents gave written consent for review and signature before starting interviews.
Consent for publication
Not applicable.
Data availability
The data that support the findings of this study are on request from the corresponding author. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
This study was approved by the ethics committee of the Iran University of Medical Science with the following number IR.IUMS.REC.1402.383, and all methods were carried out with the research ethical codes of the Iran National Committee for Ethics in Biomedical Research.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.