
Abstract
The diagnostic process is a complex and multifaceted journey that begins when patients first notice symptoms and seek advice from various sources, including family, friends, and digital platforms. To better understand this process, we introduce the concept landscape of diagnosis, which encompasses the diverse factors that influence diagnostic accuracy, timeliness, communication, and outcomes. Traditionally grounded in the biomedical model of health, the field of diagnostic safety is shifting toward a biopsychosocial approach that prioritizes community engagement. Yet, despite increased recognition of engaging patients, families and communities in safety practices, most interventions for reducing diagnostic error remain clinician and system focused, often failing to incorporate contributions of patients, families, and communities. We advocate for a paradigm shift in diagnostic safety practices, with impacts of social determinants of health addressed throughout the entire landscape of diagnosis. Community engagement strategies, including partnerships with local organizations and community health workers, can improve diagnostic accuracy and timeliness, particularly for underserved populations. We illustrate this with a hypothetical case showing how community health workers in partnership with community organizations can bridge gaps in follow-up care for geriatric patients with limited English language proficiency. Integrating community engagement strategies into diagnostic safety practices offers a promising path toward reducing diagnostic error and achieving more equitable health outcomes.
Keywords
Introducing the landscape of diagnosis
When does the diagnostic process begin? It depends on whom you ask. For patients, their diagnostic journey begins when they feel something out of the ordinary in their body. When they reach out to their family, friends, and elders about these changes. When they post a story on Instagram, try out a symptom checker, call a nursing line, or ask ChatGPT for help. The landscape of diagnosis refers to the broader, multifaceted context within which the diagnostic process occurs, encompassing the people, systems, technologies, and environments involved. This approach to diagnosis also acknowledges the important role of communities and culture in decision-making around diagnosis and subsequent actions. Patient and community engagement foreground the voices of those with lived experience, whose insight into healthcare challenges plays a pivotal role in advancing diagnostic safety. The landscape of diagnosis underscores the complexity of the diagnostic process, emphasizing the diverse factors—such as accuracy, timeliness, communication, and outcomes—that shape and are shaped by these influences. In this Commentary, we introduce a graphic visualization of the landscape of diagnosis (Figure 1) and explore pressure points within this landscape, where community engagement strategies can be integrated to reduce diagnostic error.
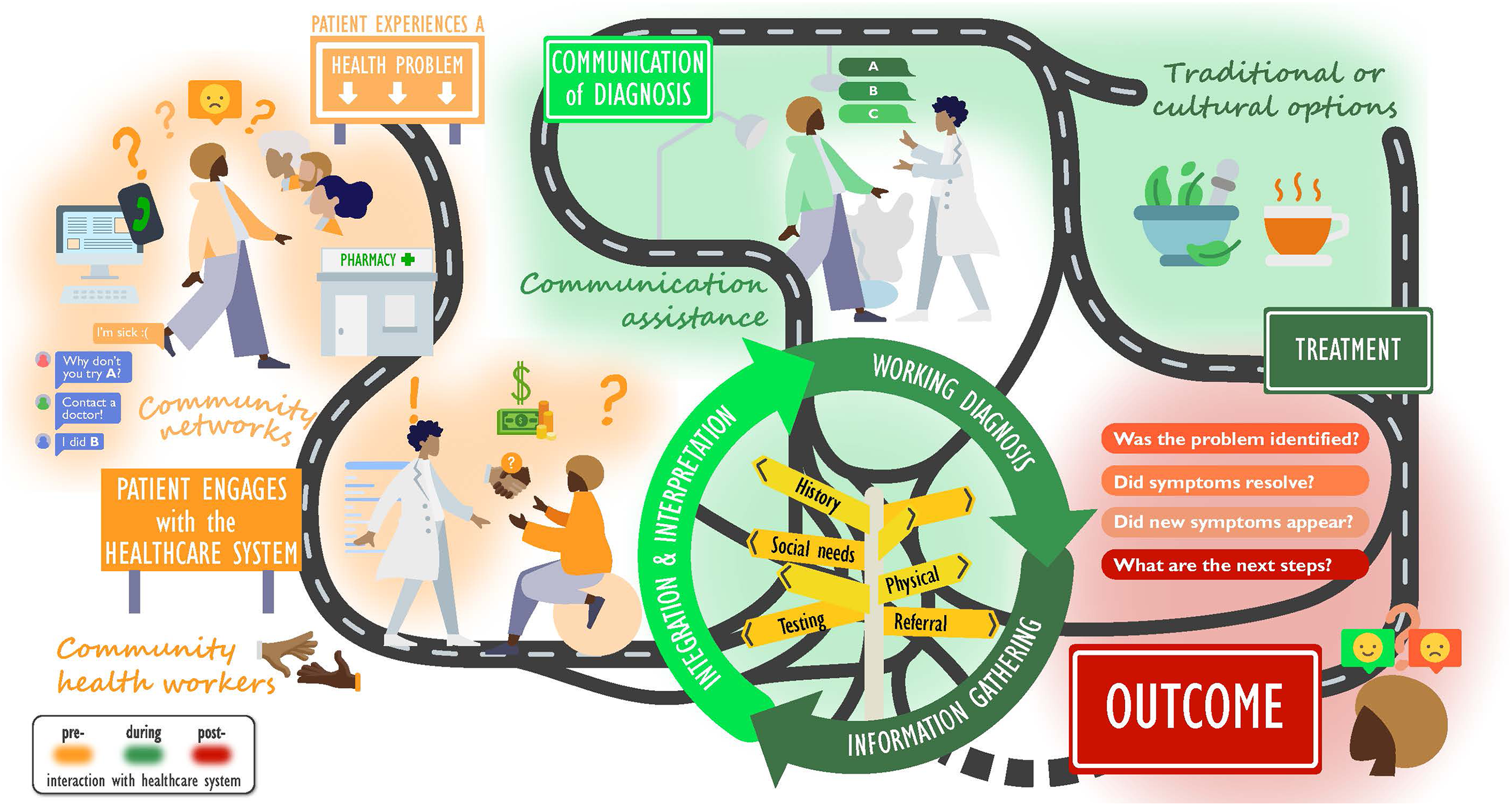
The landscape of diagnosis: A patient- and community-centered framework to the diagnostic process.
The field of diagnosis is historically shaped by the medical model and its biomedical focus on disease, which is reflected in the operationalization of key terms, proposed models, and frameworks to identify and understand steps and breakdowns in the diagnostic process. 1 However, a systemic movement towards more biopsychosocial approaches emerged in 2015, when the National Academies of Sciences, Engineering, and Medicine (NASEM) emphasized the importance of patient and family engagement in diagnosis. 2 Further, NASEM included “communication of a diagnosis to the patient” (p.4) in the formal definition of diagnostic error, along with “accuracy” and “timeliness”, 2 marking a shift towards recognizing diagnosis as a social and relational process shaped by communication, context, identity, and power.
Over the past decade, there has been an increasing awareness of the role patients and families play in patient safety practices.3,4,5 However, most patient and family engagement interventions measure perceptions of safety rather than involvement in safety activities, clinical outcomes, or patient safety events. 4 In the diagnostic error literature, interventions have predominately targeted clinicians and healthcare organizations. 6 A recent systematic review found that technique- and technology-based system strategies were the most-studied interventions, and that these were seen to be most effective in reducing diagnostic error. 6 Technique-based interventions covered changes in equipment, procedures, and clinical approaches targeting diagnostic performance. 6 Technology-based system interventions involved tools such as computer assistive diagnostic aids, decision-support algorithms, text message alerts and pager alerts. 6 Studies on effective educational interventions involved only clinicians, with no inclusion of patients, families, or communities. 6 Notably, none of 20 studies in the review reported on patient, family and community engagement or interventions targeting delays in patient presentation. 6 This gap reflects the need for a paradigm shift in the field of diagnostic safety, and we propose a two-fold iterative process to initiate the movement. The first step is to recognize that the diagnostic process extends beyond clinical settings into neighborhoods, community-based organizations, and online spaces. The second step involves a systematic synthesis of the evidence on efforts to engage patients, family, and communities in diagnostic safety. As an attempt to reimagine the diagnostic process through this lens, we present a visual landscape of diagnosis and explore pathways for integrating patient and community engagement to reduce diagnostic error.
Diagnosis in context: Addressing social determinants of health
As patient safety researchers, we must remind ourselves that only 20% of the modifiable contributors to health outcomes are influenced by quality of care. 7 Thus, 80% of our health is determined by factors and contexts outside the clinical setting, ranging from physical environment such as distance to healthcare providers to social connectedness, including civic participation. 7 Social determinants of health are closely linked to the diagnostic process. 8 Transportation, education, language, housing, and poverty are some of many factors impacting patient experiences and actions when symptoms arise. 8
The positivistic approach to medicine, in other words, reliance on objectivity, including testing, measurement and validity, has historically undervalued the importance of social determinants of health for patient safety. Growing involvement of patients and families in safety initiatives, along with increased focus on social determinants of health, has nevertheless generated momentum for redefining the scope and priorities of diagnostic safety. It is promising to witness the emergence of safety interventions that implement social needs screening in emergency departments, use bilingual patient navigators and integrate electronic health records into community referral platforms. 9 We encourage similar approaches for screening to be integrated into the diagnostic process. Especially, during the “information gathering, integration and interpretation phase” (Figure 1), social determinants of health screening can provide opportunities to identify and address unmet needs among medically disenfranchised patients. From a justice standpoint, patient harm due to diagnostic errors should not disproportionately affect certain patient populations. Yet, disparities in diagnostic error exist throughout the diagnostic process. 8 Women are less likely to receive a timely diagnosis of coronary heart disease, 8 Black/African American patients are more likely to be underdiagnosed with depression during a first primary care visit, 8 and patients living in rural areas have higher odds of late-stage breast cancer diagnosis. 10 COVID-19 highlighted in real time disparities in diagnosis for Black/African American patients, non-English speakers and people living in poverty. 11 The volume of research conducted in diagnosis and health equity as separate themes has increased significantly. 12 However, the intersection of these important areas has received less attention; and, thus, strategies to address disparities occurring throughout the diagnostic process remain sparse. 12
Integrating community engagement into the landscape of diagnosis
Community engagement is recognized as an essential element of achieving better health outcomes for all. 13 Over the past decades, research on a global scale has demonstrated the important role of community engagement in public health, 13 underscoring that health is more than just an outcome of biomedical interventions; social structures matter. Across disciplines, varying terminology is used to define community engagement reflecting different levels of inclusion and engagement. 13 In this Commentary, we operationalize community engagement as a continuum of activities involving community partners and members in the planning, design, implementation, and delivery of services that aim to ensure timely, accurate, and well-communicated diagnoses. 2 By empowering its core asset–the people–community engagement can reduce diagnostic error through not only identification of gaps in access to diagnostic services and barriers for patient safety, but also development of interventions supporting the quality of care through improved health outcomes, service delivery, and enhanced ownership and accountability.
The diagnostic process begins as the “patient experiences a health problem” (Figure 1), and symptom recognition is a crucial step towards timely diagnosis. Symptoms manifest in various ways and may be experienced differently across patient populations, and health literacy often impacts recognition of symptoms. 14 Engaging community members in design, development and information sharing of campaigns on warning signs and symptoms, especially in conditions with high disparity rates, can be the first step towards addressing unequal access to knowledge in communities with unmet needs. For instance, during the COVID-19 pandemic, local organizations and medical centers formed partnerships with Black/African American faith-leaders. 15 Through social media platforms, pastors disseminated culturally relevant COVID-19 messaging, which included African American colloquialisms, dialect and idioms. 15 Some churches also served as testing sites offering testing on a weekly basis. 15 These partnerships enabled sharing of culturally tailored information to church members, who were thought not to have access to accurate and reliable information, and also mitigated transportation barriers to testing. 15 Although these partnerships were perceived as successful, future community engagement interventions should include measures of testing uptake to document outcome effects on disparities. This case adds to the rich history of community engagement in public health programs including health education and disease prevention; we believe that safety interventions can benefit from such community engagement strategies as well.
Regarding “patient engagement with the healthcare system” (Figure 1), partnerships between hospitals and community health workers might improve access to diagnostic services among patient populations with unmet needs. There are documented sociodemographic disparities in diagnosis of autism spectrum disorder, in which children from families of low-income are diagnosed later than children from families of high-income. 16 Community health workers with personal experience and firsthand knowledge of beliefs and norms around health behavior can serve as intermediaries between patients, healthcare providers, and systems. For instance, pediatric primary care providers could refer families in need of support to community health workers, who can screen for patient barriers, connect to financial aid programs, assist with patient portal enrollment, and schedule follow-up appointments. Such assessments conducted by community health workers lay a foundation for knowledge exchange during the “information gathering, integration and interpretation and working diagnosis” pressure point in the diagnostic landscape (Figure 1), which in turn can improve timely diagnostic evaluation and early intervention access.
Breakdowns in “communication of diagnosis” between providers and patients (Figure 1) have been identified as a pressure point, 17 where several barriers challenge the clinical encounter. 17 The use of medical jargon and complex terminology from providers and level of English language proficiency and health literacy among patients and caregivers are some considerations to include in strategies improving communication of diagnoses. 18 For instance, patients with limited English language proficiency, lower levels of health literacy and of disadvantaged socioeconomic position more often report lack of qualified translators, no healthcare provider speaking the patient's language, and not being able to understand the follow-up instructions as contributing factors to diagnostic error compared to their counterparts. 18
We present a hypothetical case that illustrates how healthcare systems, local community organizations, and community health workers can improve hospital follow-ups and thus facilitate safer diagnostic journeys for patients with limited English language proficiency.
Improving diagnosis in geriatric medicine: Lessons from a hypothetical case
At a safety-net healthcare system, the geriatric staff notices that there has been an increase in no-shows for referred patients. These patients have not been followed-up with a screening for cognitive impairment after discharge from the emergency department, despite concerns being noted in the medical records. The geriatric nurse practitioner reviews the electronic health records for demographic information and discovers that many patients have indicated a preferred language other than English. The nurse practitioner realizes that current standard practice for follow-up is a reminder phone call, a mailed letter and notifications on the patient portal, all provided in English only. This finding raises the concern that patients with limited English language proficiency are not adequately followed-up compared to English-speaking patients, which may result in delaying a potential diagnosis of cognitive impairment.
If we review the diagnostic landscape, this scenario demonstrates a breakdown in the diagnostic process; failures following-up in care. The geriatric nurse practitioner shares the concerns at a subsequent department meeting as to whether the current practice of outreach efforts is effective. The clinical case manager has some knowledge about the largest non-English-speaking geriatric community in the area, Latine patients. They initiate a community mapping process to identify organizations and stakeholders to partner with. Through this mapping, the clinical case manager identifies a recreational club for ageing Latines and a community-based organization that trains Spanish-speaking community health workers. The clinical case manager invites the two organizations to attend a department meeting to discuss concerns on current follow-up practices and share ideas to address this challenge. The representative from the recreational club emphasizes the negative impact of language barriers on healthcare utilization among ageing Latine patients. The community health worker recommends that information for this particular patient population be delivered in Spanish, written and oral. At a subsequent workshop, the community health worker collaborates with the geriatric department to create follow-up information in Spanish. The community-based organizations share their flyers in Spanish and English with the geriatric department, which intends to distribute them to patients during future encounters, bridging the hospital system with local community services.
With this case, we want to emphasize the importance of community health workers as cultural intermediaries between providers and patients. Besides language fluency, understanding of medical terminology and situational awareness, perhaps most significantly, community health workers occupy cultural knowledge and sensitivity that can be leveraged in clinical encounters. Partnerships between hospital systems, local community-based organizations and community health workers can address pressure points in terms of addressing specific barriers related to follow-up systems.
Conclusions
The progression of patient and family engagement in patient safety strategies and the increased focus on social determinants of health create momentum for rethinking the field of diagnostic safety. An approach based on social needs can help practitioners, policymakers, and researchers identify pressure points of potential error within the landscape of diagnosis. The integration of community engagement strategies holds promise to reach patients who suffer the most from diagnostic error. As patient safety professionals, we should be inspired by best practices from public health interventions in engaging community members to achieve safer diagnoses. Thus, the question remains: How can we systematically include community engagement in all our safety strategies? The journey of a thousand miles starts with a single step. We believe that the landscape of diagnosis must extend beyond the clinical setting to account for the importance of communities and culture in decision-making around diagnosis and subsequent actions. Inviting communities from margins to center may provide opportunities for patients and their communities to actively and meaningfully engage in safer care.
Footnotes
Ethical considerations
Ethical approval was not required for this Commentary article. Informed consent is not applicable to this Commentary article.
Author Contributions
The idea for this Commentary was conceptualized by AS and TDG. AS drafted the first version of the manuscript. TDG substantially revised the manuscript. The draft was edited and refined by AS based on recommendations from TDG through multiple rounds. All authors have read and approved the final version of the manuscript. TDG accepts full responsibility for the work and/or the conduct of the study, and controlled the decision to publish, as guarantor.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.