
Abstract
Background
The communication of bad news in healthcare is a critical factor in patient care and workplace safety. Ineffective communication can contribute to emotional distress and aggression toward healthcare professionals. Despite its importance, many professionals lack the necessary training to manage these conversations effectively, increasing the risk of conflict. This study investigates the relationship between communication breakdowns and workplace violence in healthcare settings.
Methods
This retrospective observational study analyzed incident reporting data from two major Local Healthcare Authorities in Southern Italy (2019–2023). Reports of aggression toward healthcare professionals were categorized by type (verbal or physical), triggering event, location, severity, and aggressor identity. Chi-square tests and linear regression models were used to identify trends and associations.
Results
A total of 248 reported incidents were analyzed, with 85.1% classified as verbal aggression and 14.9% as physical aggression. The primary trigger was disagreement over clinical management (57.4%), followed by perceived delays in care (25.5%) and denial of assistance by family members (11.7%). Most incidents occurred in community-based healthcare services (42.6%) and emergency departments (25.5%). Family members were the primary perpetrators of physical assaults (64.3%), while patients were responsible for most verbal aggression (55.3%).
Conclusions
Poor communication strategies contribute to workplace violence. Improving healthcare professionals’ communication skills through structured training, implementing conflict management strategies, and strengthening security measures in high-risk areas are crucial for reducing aggression. Future research should explore additional risk factors and assess the effectiveness of targeted interventions.
Keywords
Background
“The failure of a relationship is almost always a failure of communication”. 1 Among the “emotionally intense” relationships, the one between healthcare professionals and patients certainly stands out. Communication in healthcare refers to the process of exchanging information, thoughts, and feelings between healthcare providers and patients in verbal, non-verbal, and written forms. It can be considered a “transaction” in which messages are created and exchanged.2–6 Nowadays, also thanks to incentives provided by jurisprudence in Italy and worldwide, communication time in healthcare plays a fundamental role. Consider, for instance, informed consent, patient and caregiver involvement in decision-making regarding therapeutic settings, etc.
Nevertheless, the communication of bad news remains a significant challenge for healthcare professionals. This complex and multifaceted process profoundly impacts both patients and professionals, who often have to manage intense emotional reactions while providing practical information.7–9
In the past, medical and healthcare education placed little emphasis on communication skills compared to technical competence. 10 As a result, healthcare professionals were—and still are, to some extent—often unprepared to face the communicative complexity and emotional intensity of delivering bad news.11,12
Bad news in healthcare can be defined as any information that negatively affects a person's opinions or expectations about their present or future. 13 It is not limited to a diagnosis or prognosis but includes any information that significantly alters the patient's perception, such as test results, reduced functional abilities, changes in treatment plans, or end-of-life transitions.11,14 The severity of bad news is also influenced by patient expectations, current health status, and awareness, 14 as well as their psychophysical conditions.
Delivering bad news or life-changing information is one of the most challenging tasks healthcare professionals face. Breaking bad news has psychological effects on both the patient and the professional. 15 Nonetheless, studies have shown that patients need and want to know the truth about their condition, even if it is hard to understand. 16 In reality, the situation is complex, and patients and their families often receive more favorable assessments from optimistic rather than honest physicians. Healthcare professionals may experience stress in delivering bad news, fearing emotional reactions from patients or being blamed, which can lead them to withhold information, delay disclosure, or present an overly optimistic prognosis. However, this approach can create significant confusion for patients about their condition.17,18 Therefore, it would be appropriate for healthcare professionals to recognize this need on the part of patients and to ensure that the information provided is complete and truthful—possibly delivered gradually, in order to help the patient come to terms with the truth. From the patients’ perspective, receiving distressing news significantly impacts quality of life, coping strategies, psychosocial adaptation, and openness to treatment compliance. Patients may react in various ways, including violent outbursts, expressions of shock, fear, and helplessness, anger and a sense of injustice, gratitude toward the professional, or feelings of depression.19,20 Patients most frequently responsible for violent acts are those affected by conditions such as intoxication, psychosis, delirium, or dementia, which significantly increase the risk of aggression toward healthcare personnel.21–23
Other contributing factors include workplace context and the specific tasks of healthcare professionals, which can make them more exposed to patient aggression, particularly in emergency departments, internal medicine wards, and psychiatric units. The situation is further aggravated by shift management, especially during night shifts, which are often characterized by an insufficient number of staff relative to patient needs.24,25
The way healthcare professionals communicate bad news significantly influences how patients and their families receive, interpret, and cope with it.14,26
Inadequate communication can cause confusion, long-term distress, and resentment in patients. 27 Breaking bad news is thus a complex process that must be managed skillfully, as it not only profoundly impacts the patient's emotional well-being but also affects the relationship with the caregiver and the patient's future decisions.26,28
However, research has shown that healthcare professionals often lack the training and confidence necessary to properly communicate bad news.26,28 Delivering “bad news” or “stressful news” to patients can be an extremely difficult and daunting task. Factors such as the healthcare professional's fears and anxieties, lack of proper communication skills or defined protocols, and the potential patient reaction—where they blame the bearer of the news—can further complicate this process. 11 The phenomenon where patients associate the bad news with its deliverer is common: the easier it is to identify the source of the news, the easier it is to direct anger and blame toward that person. 11 This anxiety is compounded by the lack of training many healthcare professionals receive in communication skills, particularly in delivering bad news or discussing sensitive topics with patients. 26 Without the appropriate tools and techniques, professionals may struggle to manage these conversations in ways that minimize patient distress while maintaining a positive relationship. The result can be suboptimal information sharing, patient dissatisfaction, loss of trust in the healthcare provider, and potentially even conflict situations that may escalate into violent episodes against healthcare personnel. 28 However, when done well, breaking bad news can help patients understand, accept, and adapt to their situation.26,29–31 Patients who comprehend their condition are better prepared to make informed decisions, have a greater sense of control, and avoid inappropriate or ineffective treatments.29,31
Although violence against healthcare professionals is a recognized issue, its resolution remains controversial due to the lack of universally adopted standards, 32 Instead, models tailored to specific healthcare areas, such as oncology, have been implemented.33,34 To overcome the challenges of effective communication, healthcare organizations should prioritize communication training as an essential part of professional development, equipping healthcare workers with the skills necessary to deliver bad news empathetically and effectively.14,28,35
For training to yield the desired results, it is crucial to identify best practices to address this delicate aspect of clinical work. These include proper emotional preparation of professionals to manage patient reactions such as shock and anger in a calm and controlled manner,36,37 as well as de-escalation techniques to communicate bad news while minimizing negative patient reactions through effective communication.38,39
This study aims to analyze the relationship between the communication of bad news and aggressive behaviors in healthcare settings. Specifically, the research investigates: (1) the prevalence and types of aggression towards healthcare professionals in relation to communication breakdowns, (2) the main triggers of violent incidents, and (3) the impact of workplace settings on the likelihood of aggression. The study also examines the effectiveness of current institutional measures in mitigating such risks and explores potential areas for improvement.
Italian legislative context and the role of clinical risk in aggressive behavior
In recent years, the issue of safety in healthcare has gained increasing attention, not only concerning patient protection from clinical errors but also in ensuring the security of healthcare professionals. Aggressive behaviors toward healthcare personnel are influenced by multiple factors, including working conditions, patient expectations, and relational dynamics. 40 In Italy, workplace safety legislation is governed by Legislative Decree 81/2008, which requires employers to assess all health and safety risks for workers, including those related to violence and aggression. In the healthcare sector, these provisions are further reinforced by Law No. 113 of August 14, 2020, which establishes specific measures to prevent violence against healthcare professionals, such as the creation of the National Observatory on Healthcare and Social-Healthcare Professionals’ Safety, the introduction of stricter penalties for those who commit assaults against healthcare workers, and awareness campaigns to prevent violence, 41 including the possibility of arresting perpetrators within 48 h. 42
In Italian healthcare institutions, Clinical Risk Units play a crucial role within the broader concept of healthcare safety management, particularly in monitoring adverse and sentinel events. Among these, aggressive behaviors from patients and their families toward healthcare personnel are included. 43 Firstly, this phenomenon can be associated with a malfunctioning healthcare and assistance system, which acts as a trigger for episodes of violence. Secondly, assaults on healthcare personnel lead to general service disruptions, ranging from temporary service interruptions to a loss of trust among healthcare professionals in their work, potentially resulting in burnout.
To effectively address the issue of aggressive behaviors in healthcare, an integrated approach combining legislative, organizational, and educational measures is necessary. Strategies include training healthcare professionals in conflict management, designing safe work environments, providing psychological support to professionals involved in violent incidents, and implementing monitoring systems to identify risk signals early and intervene proactively.44,45 Clinical risk management and the prevention of aggressive behaviors are closely linked and represent a priority in ensuring high safety and quality standards in healthcare. Promoting a climate of trust and mutual respect, with collaboration between institutions, healthcare organizations, and professionals, is essential. 46
Materials and methods
This study is an observational retrospective analysis. The data analyzed were collected from reports submitted by healthcare professionals according to institutional protocols for reporting assaults on staff. Specifically, data were obtained through the Clinical Risk incident reporting system from two large and important Local Healthcare Authorities in Southern Italy, covering the period from 2019 to 2023. One Local Healthcare Authority includes three hospitals as well as community-based healthcare services, which encompass outpatient clinics, general practitioners, rehabilitation centers, and home care. The other institution, a University Hospital, comprises two hospital facilities. Collectively, these institutions serve a population of approximately 1.5 million inhabitants.
Since these reports are voluntary, each aggression event was detailed by the involved healthcare professionals. All reports of aggression in which at least one healthcare professional was clearly identified as a victim and at least one patient or family member as the aggressor were included. Cases were excluded when the dynamics were not clearly described, involved conflicts exclusively between healthcare professionals, or were not clearly attributable to a communication defect (e.g., cases of intoxication or psychosis). The data are presented in Table 1.
Healthcare professionals assault data 2019–2023.
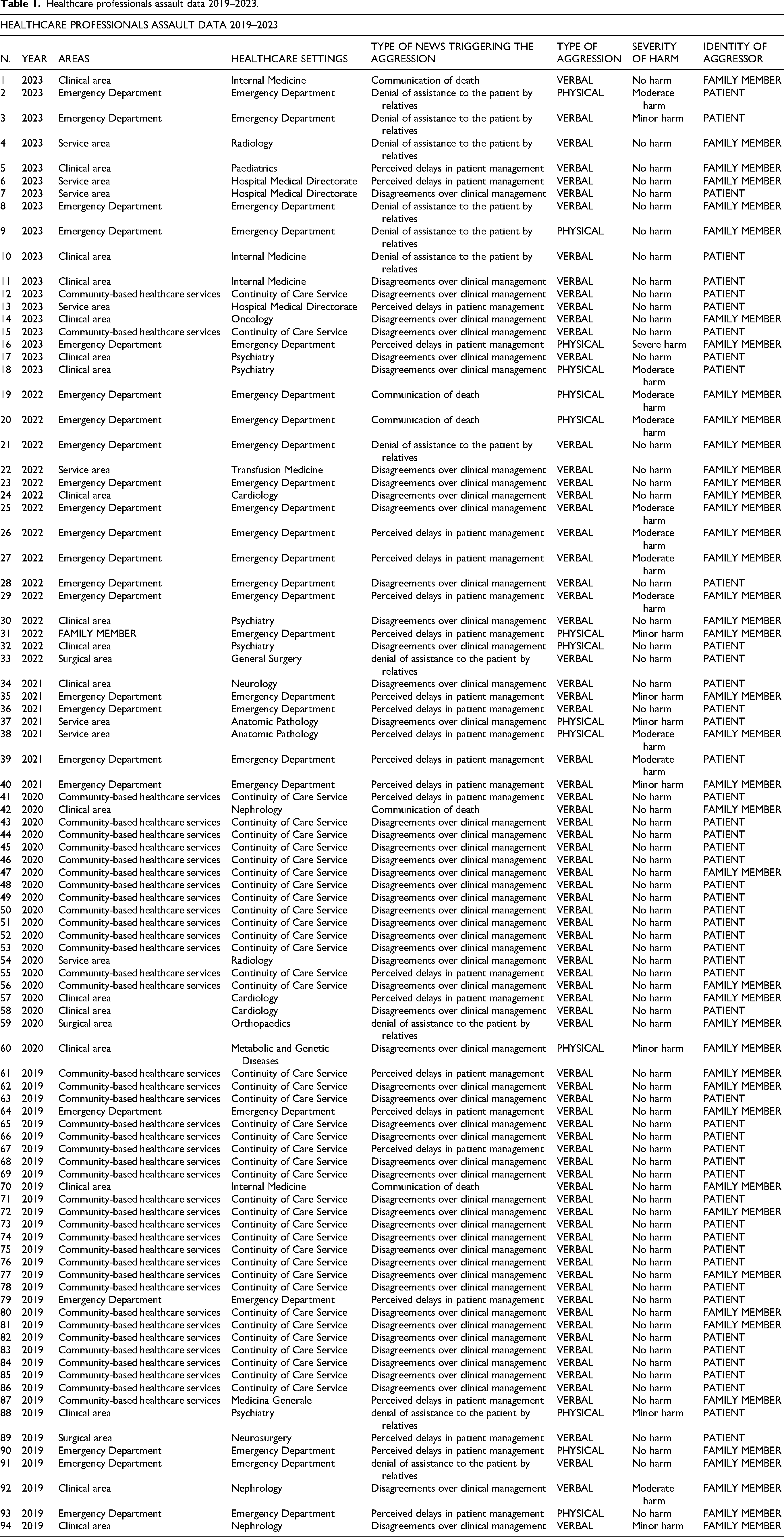
The analysis examined the total number of assaults in each institution, selecting incidents originating from possible communication failures between healthcare personnel and patients or their families. Event descriptions recorded in incident reporting forms were categorized according to the following criteria:
Type of aggression (2 subcategories: “verbal” or “physical”) Type of news triggering the aggression (4 subcategories: “denial of assistance to the patient by relatives”, “perceived delays in patient management”, “communication of death”, “disagreements over clinical management”) Areas where the aggression occurred (5 subcategories: “community-based healthcare services,” “surgical area,” “clinical area,” “service area,” “Emergency Department”) Severity of harm (4 subcategories: “no harm,” “minor harm,” “moderate harm,” “severe harm”) Identity of the aggressor (2 subcategories: “patient” or “family member”)
The data were analyzed using descriptive statistics to summarize absolute and relative frequencies of variables. To assess significant differences between categories, the following statistical tests were used:
Chi-square test of independence (χ²) to compare frequency distributions between categorical variables Linear regression test to evaluate temporal trends in aggression over the considered period
The statistical significance level was set at p < 0.05. All analyses were conducted using the statistical software JAMOVI-Electron.
Ethical considerations
This study is a retrospective observational analysis based on pre-existing data collected through the institutional incident reporting systems of two Local Healthcare Authorities in Southern Italy. The data were collected for institutional purposes of monitoring and managing clinical risk and are fully anonymized. Therefore, no ethics committee approval was required as the study did not involve direct interventions on patients or the collection of new personal data.
Results
The overall analyzed data are reported in Tables 1 and 2.
Total reported assaults.
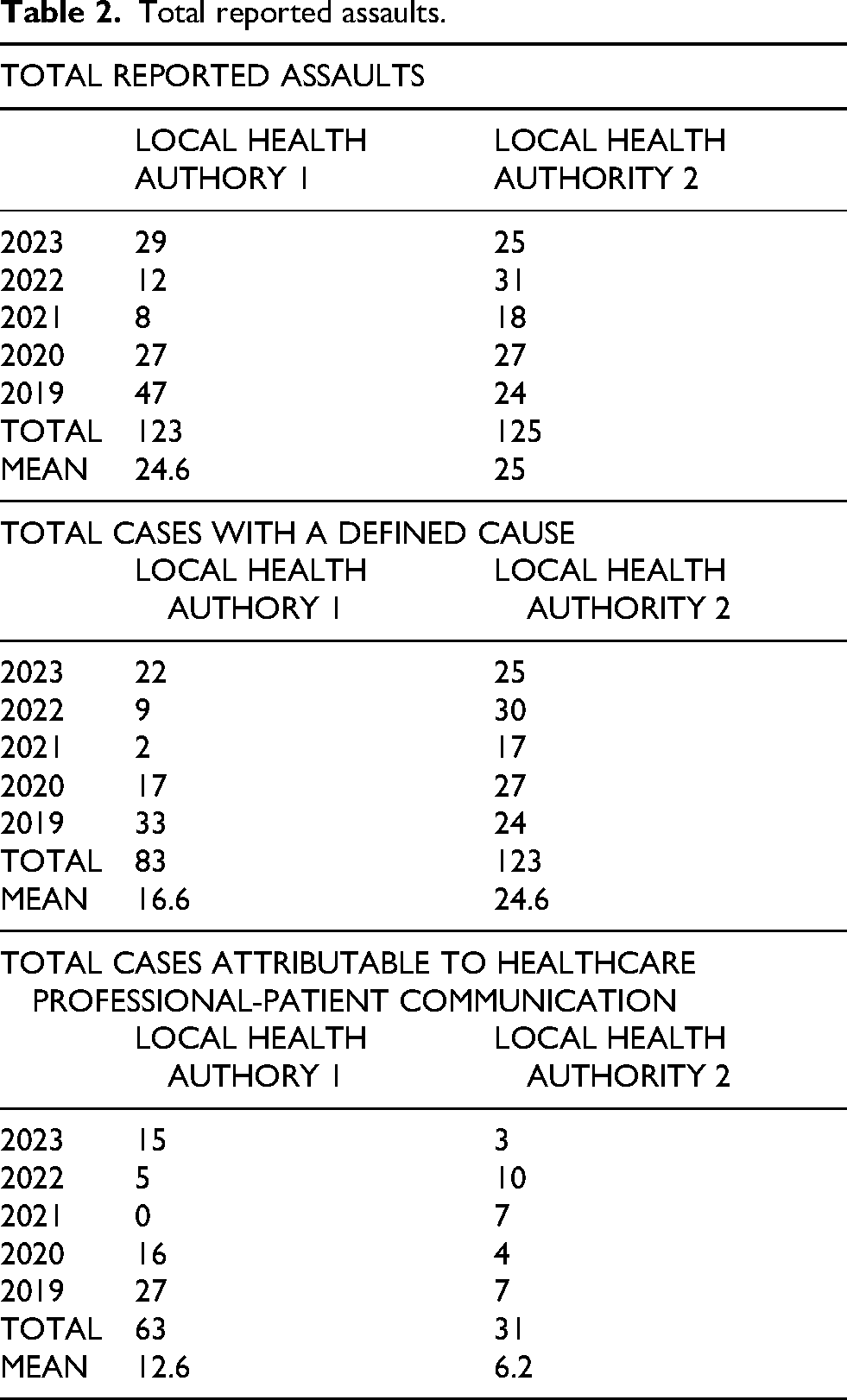
During the period 2019–2023, a total of 248 assaults were recorded across the two healthcare institutions (123 and 125, respectively), with a homogeneous annual average of assaults between the two Local Healthcare Authorities (24.6 assaults/year and 25 assaults/year, respectively). Among the submitted incident reports, 206 cases included a description that allowed for the identification of a cause (83 for one facility, 123 for the other). Finally, upon analyzing the case descriptions, a total of 94 assault cases were identified as being attributable to communication failures between healthcare professionals and patients or their families (63 for one institution, 31 for the University Hospital).
The overall trend of assaults on healthcare personnel attributed to possible communication errors showed a peak in 2019 (34 cases), followed by a significant decline in 2020 (20 cases) and reaching a minimum in 2021 (7 cases). From 2022 onwards, the numbers began to rise again, with 15 cases in 2022 and 18 in 2023.
Type of aggression
Between 2019 and 2023, 85.1% of reported assaults were verbal, whereas 14.9% were physical. To assess the difference between these two categories, a chi-square test of independence was conducted, revealing a highly significant difference in the frequency distribution between the two types (χ² = 47.52, p < 0.001), confirming that verbal aggression was significantly more frequent than physical aggression.
The temporal trend showed a decrease in verbal assaults between 2019 and 2021, followed by an increase in the subsequent years, while physical assaults remained relatively constant with a slight increase. However, a linear regression analysis did not identify a significant variation over time for either type (p > 0.05).
The data are presented in Table 3.
Type of assault.

Triggers of aggression
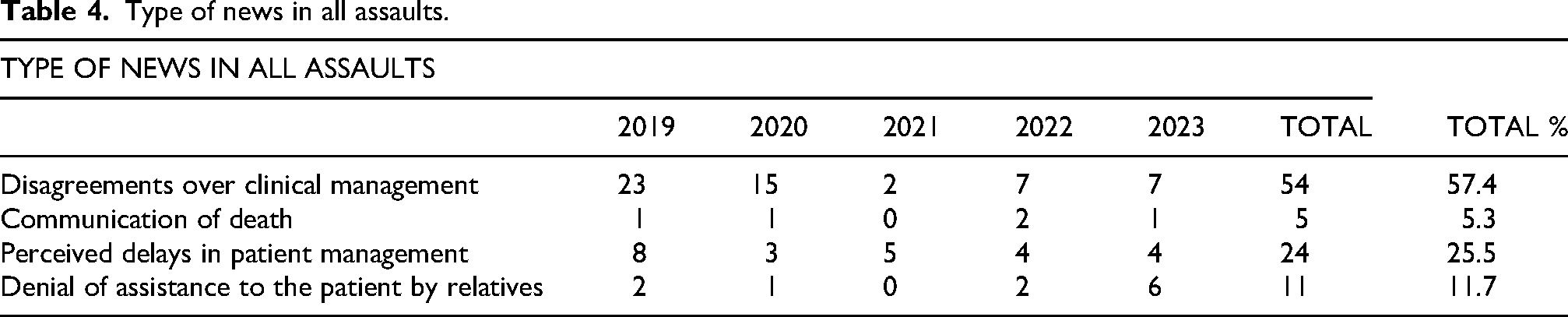
The analysis of aggression triggers indicated that the primary cause was disagreements over clinical management (57.4%), followed by perceived delays in patient care (25.5%). Denial of assistance by family members accounted for 11.7% of incidents, while the communication of a patient's death represented only 5.3%.
A chi-square test confirmed a non-random distribution of causes across the categories (χ² = 61.83, p < 0.001), with disagreements over clinical management being significantly more frequent than other causes.
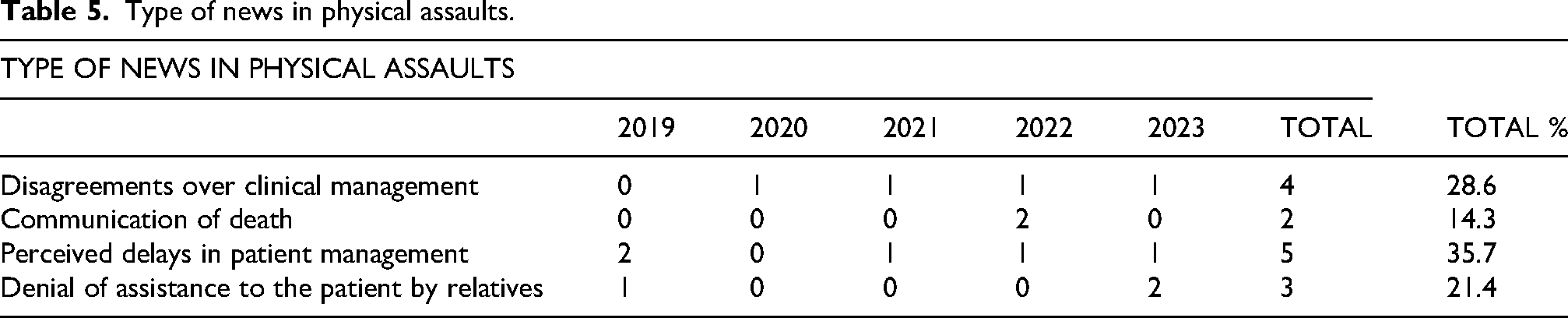
For physical assaults alone, the distribution of causes appeared more balanced: perceived delays in patient care were the primary trigger (35.7%), followed by disagreements over clinical management (28.6%), denial of assistance (21.4%), and communication of death (14.3%). However, the chi-square analysis of differences in trigger frequencies for physical aggression did not yield statistical significance (χ² = 5.92, p = 0.11).
The data are reported in Tables 4 and 5.
Type of news in all assaults.
Type of news in physical assaults.
Context of aggression
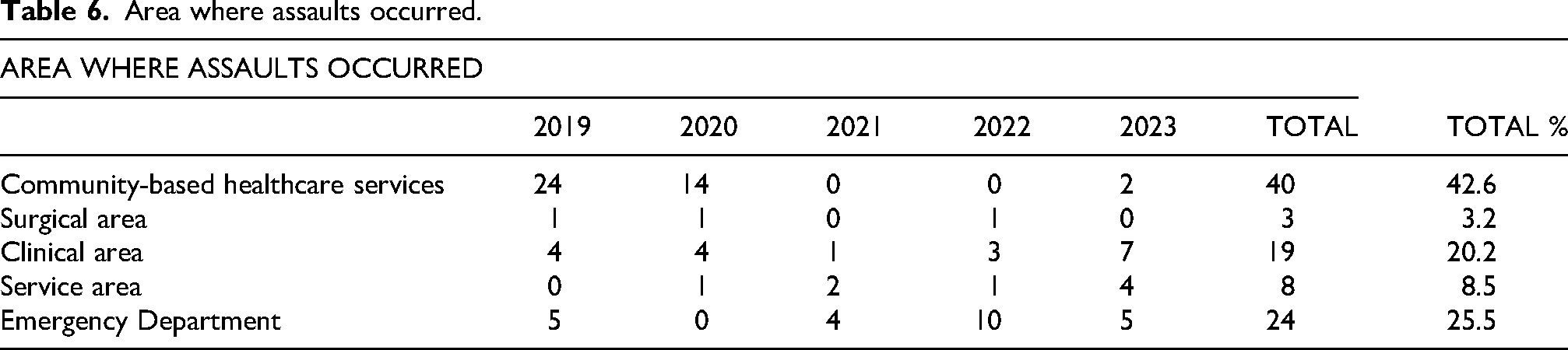
Assaults predominantly occurred in community-based healthcare services settings (42.6%) and the Emergency Department (25.5%), followed by clinical wards (20.2%). Specifically, within clinical areas, one in four assaults occurred in Psychiatry (5 assaults, 26.3%). Other high-risk wards included Internal Medicine (4 assaults, 21%), Cardiology (3 assaults, 15.8%), and Nephrology (3 assaults, 15.8%). Surgical and service areas exhibited lower frequencies (3.2% and 8.5%, respectively). A chi-square test revealed a significant difference in the distribution of aggression occurrences across different areas (χ² = 82.74, p < 0.001), with community-based healthcare services settings being significantly more affected than other areas.
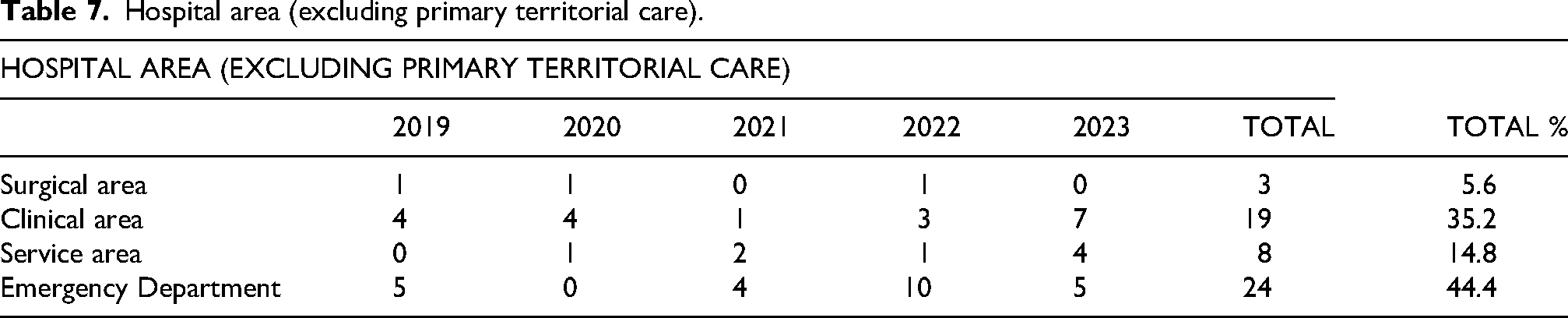
Excluding community-based healthcare services and considering only hospital settings, the Emergency Department emerged as the most frequent context for aggression (44.4%), followed by clinical areas (35.2%) and service areas (14.8%). The surgical area was the least affected (5.6%). Again, a chi-square test confirmed a significant difference between hospital areas (χ² = 33.68, p < 0.001).
The data are reported in Tables 6 and 7.
Area where assaults occurred.
Hospital area (excluding primary territorial care).
Severity of harm
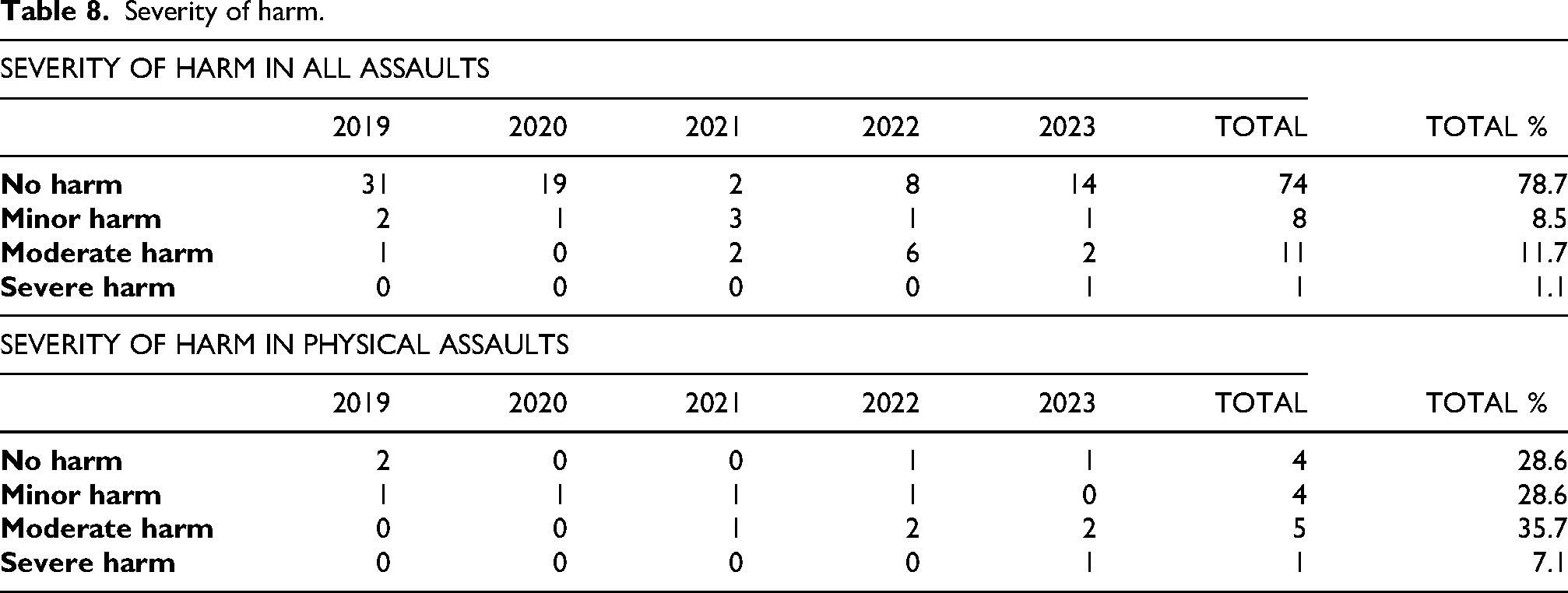
In 78.7% of cases, assaults did not result in significant physical harm to the healthcare professional. However, 8.5% of incidents resulted in minor injuries, 11.7% in moderate injuries, and only one case (1.1%) led to severe harm.
Analyzing physical assaults specifically, 35.7% caused moderate injuries, while 28.6% resulted in no physical consequences. Minor injuries were reported in 28.6% of cases, and severe harm occurred in 7.1%. A chi-square test analyzing the differences in harm levels across all assaults was statistically significant (χ² = 49.32, p < 0.001), confirming that in most cases, no physical harm was sustained. However, within physical assaults, the harm distribution showed a weaker association (χ² = 7.83, p = 0.05), suggesting greater variability in the physical impact of assaults.
The data are presented in Table 8.
Severity of harm.
Aggressor identity
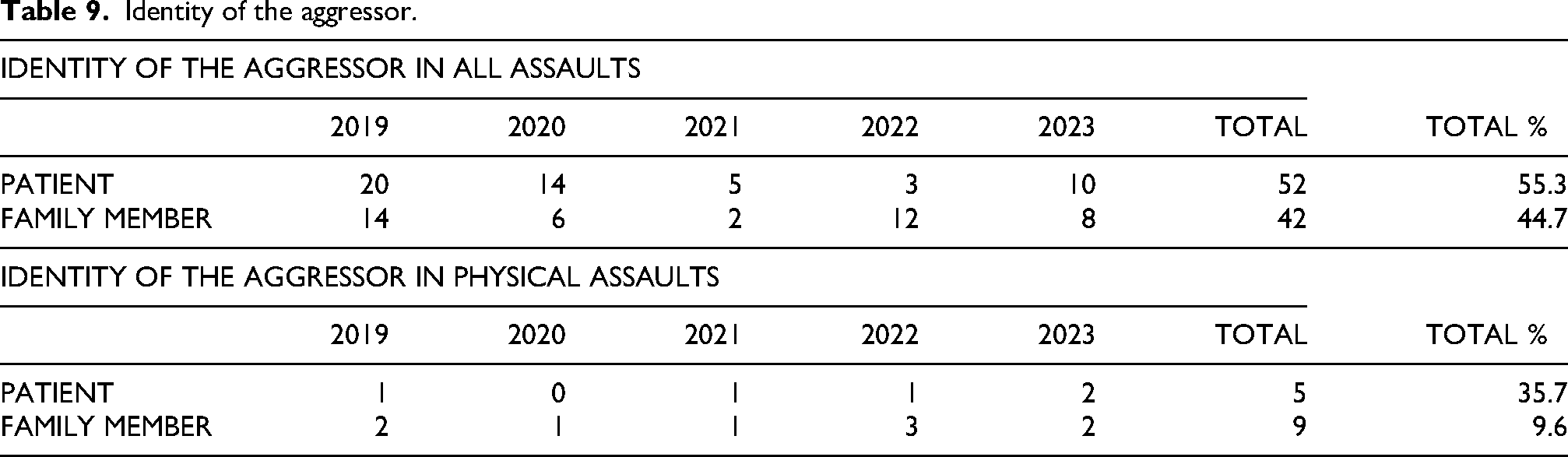
In 55.3% of cases, the aggressor was the patient, while in 44.7% of cases, the perpetrator was a family member. A chi-square test confirmed that this distribution was not random (χ² = 2.89, p = 0.089), indicating a trend (although not statistically significant) toward patients being more frequently responsible for assaults than family members.
When considering only physical assaults, the distribution shifted: 35.7% of incidents were perpetrated by patients, while 64.3% involved family members. In this case, a chi-square test indicated a statistically significant difference (χ² = 5.61, p = 0.018), suggesting that physical assaults were more often committed by family members than patients.
The data are reported in Table 9.
Identity of the aggressor.
Discussion
The data analysis highlighted that assaults on healthcare professionals represent a widespread phenomenon, with a predominance of verbal over physical episodes. This difference was highly significant (p < 0.001), confirming observations from previous national and international studies conducted in healthcare settings. 45
The overall trend of assaults on healthcare personnel between 2019 and 2023 showed a peak in 2019 (71 cases), followed by a significant decline in 2020 (54 cases) and a minimum in 2021 (26 cases). From 2022 onwards, the numbers began to rise again, with 43 cases in 2022 and 54 in 2023 (see Figure 1). Similarly, the trend of assaults attributable to communication failures between healthcare professionals and patients or their families exhibited a comparable pattern, peaking in 2019 (34 cases), followed by a significant decrease in 2020 (20 cases) and a minimum in 2021 (7 cases). Numbers then increased again from 2022 onwards, with 15 cases in 2022 and 18 in 2023 (see Figure 2).
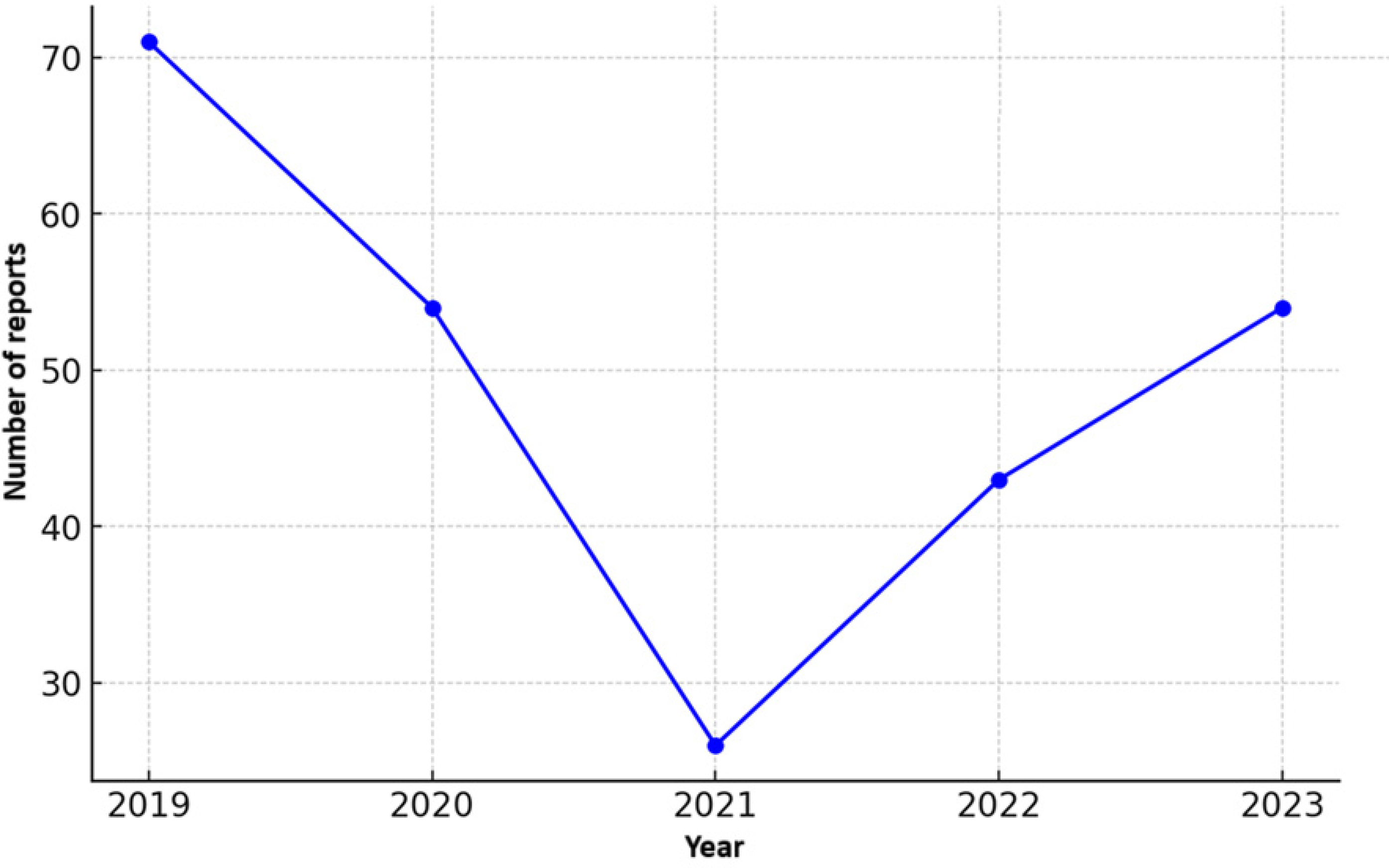
Trend of reported assaults 2019–2023.
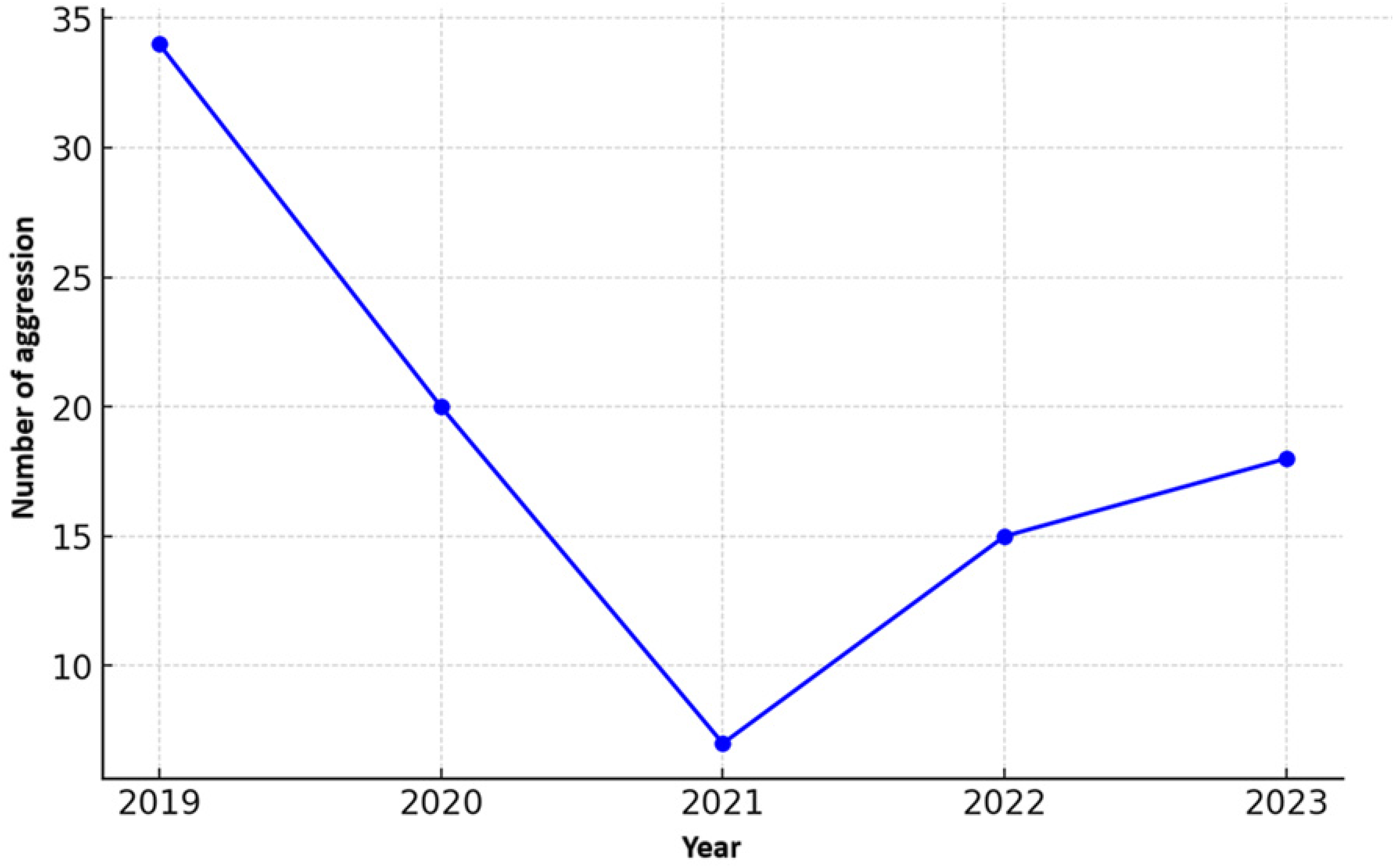
Trend of communication-related assaults 2019–2023.
This suggests a reduction in assaults during the pandemic period (2020–2021), followed by a resurgence in the subsequent years. This decline may have been influenced by health restrictions, reduced patient influx in healthcare facilities, or a combination of these factors. However, distinguishing causal factors in this temporal trend is beyond the scope of this research.
One of the most significant findings was the prevalence of disagreements over clinical management as the primary triggering factor (57.4% of total assaults), with high statistical significance (p < 0.001). This suggests that patients’ or family members’ subjective perception of the quality of care plays a key role in triggering aggressive behavior. Notably, in cases of physical assaults, delays in patient care emerged as the primary cause (35.7%), emphasizing the importance of timely care delivery as a preventive factor.
The healthcare setting emerged as a critical factor: most assaults occurred in community-based healthcare services (42.6%) and emergency departments (25.5%). Specifically, the Emergency Department was identified as the highest-risk hospital environment for assaults, confirming findings from previous literature.47,48 A chi-square test revealed highly significant differences across various care settings (p < 0.001), highlighting the need for targeted strategies to mitigate risk in these environments.
Regarding the consequences of assaults, in 78.7% of cases, no significant physical harm was reported. However, among physical assaults, the probability of moderate injuries was notably high (35.7%, p < 0.05). This indicates that, although most assaults do not result in immediate physical harm, physical violence can have significant clinical implications for the affected healthcare professionals.
The identity of the aggressor exhibited an interesting distribution: considering both verbal and physical assaults, patients were responsible in 55.3% of cases, while family members accounted for 44.7%. However, when focusing exclusively on physical assaults, family members were significantly more often the primary aggressors (64.3%, p = 0.018). This data is in agreement with other results present in the literature. 49 This suggests that the emotional stress experienced by patients’ relatives may represent a greater risk factor for episodes of physical violence.
he findings of this study suggest that preventing violence in healthcare should focus on improving physician-patient communication and implementing conflict management strategies to reduce disagreements over clinical management. 50 Additionally, optimizing waiting times and emergency care management in high-risk contexts such as Emergency Departments and community-based healthcare services is necessary.
Healthcare professionals should also receive training in de-escalation techniques to handle high-risk situations, and specific safety protocols should be implemented in areas most vulnerable to physical assaults. 51
This study has several limitations. First, the analysis is based on incident reporting data, which may underestimate the phenomenon due to underreporting of certain incidents. This issue is well-documented in the literature, 52 with reasons including fear, difficulties in properly reporting assaults, and skepticism about the effectiveness of reporting in preventing future incidents.53–55 Additionally, the lack of detailed information on the psychiatric conditions of aggressive patients limits the interpretation of violence dynamics. Future studies could integrate these data with interviews from healthcare professionals to gain a deeper understanding of perceptions and management strategies for assaults.
Conclusions
The analysis of data collected from the incident reporting systems of two major healthcare organizations in Southern Italy between 2019 and 2023 revealed that violence against healthcare professionals remains a critical issue, with a predominance of verbal assaults (85.1%) over physical ones (14.9%). Most episodes were triggered by disagreements over clinical management (57.4%), followed by perceived delays in patient care (25.5%) and denial of assistance by relatives (11.7%).
In terms of location, assaults predominantly occurred in community-based healthcare services (42.6%) and emergency departments (25.5%), while in hospitals, the distribution was more fragmented, with a predominance in clinical areas (35.2%) and emergency departments (44.4%). In clinical settings, one in four assaults occurred in Psychiatry. This finding suggests that emergency and high-interaction healthcare services are particularly exposed to the risk of assaults.
The analysis of severity revealed that in most cases, no harm occurred to healthcare professionals (78.7%), while 21.3% suffered injuries of varying severity, with only one severe case (1.1%). However, in physical assaults, the proportion of moderate or severe injuries was significantly higher (42.8%), underscoring the increased risk associated with physical violence.
Regarding the aggressor's profile, an almost equal distribution was observed between patients (55.3%) and relatives (44.7%). However, in physical assaults, family members were the predominant aggressors (64.3%), indicating that relational dynamics between healthcare professionals and patients’ families may be a critical factor in managing violence risk.
These findings align with trends in existing literature, confirming that violence against healthcare professionals is a multifactorial issue rooted in communication challenges, patient and family perceptions of care quality, and high-stress healthcare environments. 56 Identifying key triggers and high-risk areas is essential for developing effective prevention strategies, including improved staff training in patient and family communication, 51 the adoption of conflict management protocols, and enhanced security measures in high-risk settings. 50
Finally, the results highlight the need to improve incident reporting systems and encourage healthcare professionals to report violent incidents to obtain a more comprehensive mapping of the phenomenon and implement targeted interventions to protect staff. Promoting a culture of safety and support for healthcare workers affected by violence should be a priority for healthcare institutions and policymakers.
The quality of healthcare services today increasingly depends on effective communication and patient-caregiver engagement in the care process. As Italian law states, “Information is a form of care,” and the empathy associated with it integrates scientific competence with human skills. Identifying primary risk factors and high-risk areas is fundamental for developing effective prevention strategies that include better staff training in communication with patients and families, adopting conflict resolution protocols, and reinforcing safety measures in vulnerable contexts.
As the medical adage goes, “If you can heal, heal. If you cannot heal, soothe. If you cannot soothe, console” (Augusto Murri, 1841–1932).
Footnotes
ORCID iDs
Author contributions
Conceptualization, M.M. and I.G.; methodology, M.M. and I.G.; software, F.P., M.G.V., G.P. and R.R.; validation, M.M. and I.G.; formal analysis, F.P. and E.P.; investigation, F.P., E.P., S.C.B. and G.E.; data curation, F.P. and E.P.; writing—original draft preparation, ADL., R.R., M.G.V., F.P. and G.P.; writing—review and editing, M.M. and I.G.; supervision, I.G.; project administration, M.M. and I.G. All authors have read and agreed to the published version of the manuscript.
Ethical considerations
According to Italian legislation and EU Regulation 2016/679 (GDPR), no ethics committee approval or informed consent is required for studies based solely on anonymous data, as they do not involve identifiable personal information. The present study used anonymized data derived from incident reporting systems, and no individual-level identifiers were collected or processed.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.