
Abstract
The New Brunswick Colon Cancer Screening Program (NBCCSP) rejects individuals deemed above average risk for colorectal cancer (CRC) on the presumption that screening will occur via primary care providers. We examined the CRC screening outcomes among a retrospective cohort of patients deemed not average risk (NAR) and rejected from the NBCCSP. Within a randomly selected subset of 191 NAR patients with accessible data and no prior CRC screening, 120 (62.8%) remained unscreened at the end of the study period. In a matched case-control study, NAR patients who received colonoscopies waited nearly a year longer than average-risk individuals. Furthermore, NAR patients also waited significantly longer for a diagnosis of cancer compared to average-risk patients. Above-average-risk patients would benefit from expanded programmatic screening of the NBCCSP.
Colorectal cancer (CRC) is the third most diagnosed cancer in Canada. 1 CRCs account for ∼12% of cancer deaths among Canadians. 2 Organized population-based screening programs can help prevent CRC by allowing identification and removal of polyps before malignant degeneration occurs, and identifying early asymptomatic cancers that are still curable. 3 However, population-based screening programs are not accessible to everyone who may benefit from an organized screening approach.4,5 We contend that some individuals who are rejected from CRC screening programs given their risk level for CRC (i.e. above-average risk) would benefit from expanded programmatic CRC screening.
In Canada, organized CRC screening programs are offered by all 10 provinces and two of the three territories. Like other Canadian screening programs, the New Brunswick Colon Cancer Screening Program (NBCCSP) targets residents aged 50–74 via invitations through the postal service. 6 The biannual invitation includes a screening questionnaire that determines program eligibility based on CRC risk.
According to current NBCCSP clinical practice guidelines, an average risk (AR) individual has no symptoms and no personal history of colorectal adenomatous polyps, CRC, inflammatory bowel disease, or family history of CRC that meets program exclusion criteria (i.e. first-degree relative with CRC at age ≤ 60 or two or more first-degree relatives with CRC 7 ). Individuals who do not fall into the AR category are considered not average risk (NAR) and are rejected from the program. It is expected that NAR individuals are being actively followed by their primary care provider and/or specialists. However, the presumption that NAR patients have access to the care and follow-up they require may be faulty, especially given that ∼15% of New Brunswickers do not have access to a primary care provider. 8
Increased demand for colonoscopies has further exacerbated the situation and challenged the timely provision of the procedure.9–11 Long colonoscopy wait times may result in some NAR individuals receiving no screening as they wait for a colonoscopy instead of the more intensive screening intended for them by the NBCCSP. Consequently, NAR residents may receive delayed cancer diagnosis and/or missed opportunities for diagnosis. We sought to determine if some individuals designated as NAR by the NBCCSP have been overlooked and have not been receiving expected care and follow-up. We hypothesized that NAR individuals would be less likely to receive screening and experience longer wait times from program invitation to colonoscopy compared to AR individuals.
Methods
To conduct this retrospective cohort design with a descriptive and matched case-control study, a waiver of informed consent for secondary use of data was requested and granted from the Horizon Health Network's (HHN) Human Research Protection Program, inclusive of the Research Ethics Board (File # RS 2020-2923) for individuals who were invited to participate in the NBCCSP from 1 January 2016 to 31 December 2017. Provincial-level data were collected from the NBCCSP, the New Brunswick Department of Health, and regional data from HHN, one of two health authorities within New Brunswick, and electronic medical records (EMRs). Provincial colonoscopy and advanced adenoma data were unavailable for the NAR group; as such, a random cohort with data available through HHN's EMR was used for colonoscopy-related analyses, as described below. Though over 5 years old, these data are still relevant as only minor changes were made to the NBCCSP in January 2025, which do not impact the relevance of our results (see the Supplemental Appendix for the patient screening questionnaire relevant at the time the study was conducted, as well as the updated version implemented in 2025). Specifically, key changes involved: (1) the AR categorization where “no personal history of a 1st degree family history of CRC” was changed to “no personal history of 1st degree relative diagnosed with CRC at age ≤60 or two or more 1st degree relatives diagnosed with CRC at any age”; and (2) The criteria for exclusion from the program of “two or more 2nd degree relatives with polyps or CRC” had been removed from the new guidelines.
Individuals who responded to the invitation to participate in the NBCCSP were divided into AR responders (ARRs), consisting of individuals who responded and were accepted into the NBCCSP, and NAR responders (NARRs), consisting of individuals who responded and were rejected from the NBCCSP. Patients who received a diagnosis of CRC prior to the invitation were excluded. The NARR group would also include individuals who previously had a colonoscopy within the past 5 years, as they would also be rejected from the NBCCSP; however, to exclude this group of patients in the below conducted analyses, the cohort sample exclusions included those who, according to available EMR data, had a colonoscopy pre-invitation to the NBCCSP (see Figure 1).
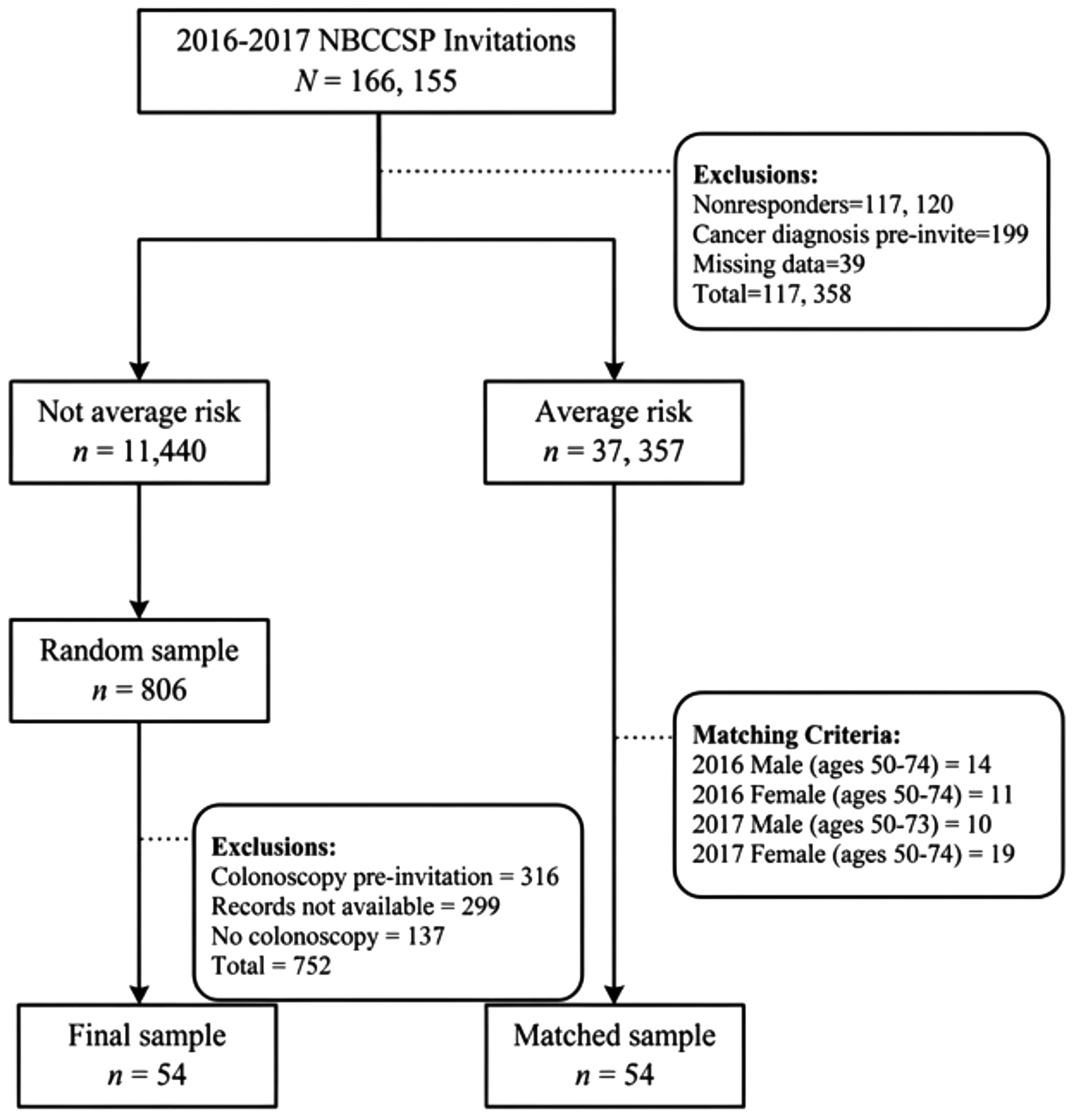
Flow diagram of study participants.
A descriptive analysis of the provincial level data from NBCCSP and New Brunswick Department of Health was conducted on demographics, fecal immunochemical test/guaiac-based fecal occult blood test (FIT/gFOBT) screening, cancer diagnosis, and death that occurred up to 30 June 2020, except for the cancer data, which, at the time of analysis, was only available up to 31 December 2019.
The provincial level data from the NBCCSP and New Brunswick Department of Health were used to investigate the difference between the time (days) from program invitation to diagnosis of cancer for ARR and NARR groups, using an independent samples t-test. Variables were screened for normality and outliers using the procedures outlined by Tabachnik and Fidell. 12 A sample size analysis was conducted using G*Power 3.1.9.4, and a minimum sample size of 260 was needed for testing for group differences in time from colon cancer screening invitation to cancer diagnosis (α = .017, 1 − β = .8, d = 0.35, one-tailed).
A matched case-control study was conducted using NBCCSP invitees assessed as NARR, who were randomly selected, employing a simple random sampling and a random number generator. For this sample, HHN EMR data regarding colonoscopies were retrieved when available. Those NARRs found, in the HHN EMR data, to have received colonoscopies within the follow-up period were exactly matched by year of invite, sex, and age to program invitees assessed as ARRs and who had also received colonoscopies within the follow-up period (see Figure 1). A sample size analysis was conducted using G*Power 3.1.9.4, and a minimum sample size of 99 was needed for testing the matched case-control study (α = .017, 1 − β = 0.8, f2 = 0.15).
Results
Out of a total of 166,155 NBCCSP invitations sent, 117,120 individuals did not respond; thus, corresponding to an overall response rate of ∼29.5%. One hundred and ninety-nine NBCCSP responders (0.004%) received a CRC diagnosis prior to their invite and were excluded. Table 1 outlines the demographic information of 2016 and 2017 invitees, which, after exclusions, included 37,357 ARR and 11,440 NARR group individuals, and indicates frequencies of FIT/gFOBT screening, cancer diagnoses, and death during the follow-up period. 10,325 individuals in the NARR group received neither a gFObt nor an FIT during the follow-up period; however, as noted in the Methods section, provincial colonoscopy data were unavailable for this group. It is conceivable that a significant portion of these individuals may have been screened with colonoscopy. To address this limitation, as described above for the matched case-control study sampling, 806 NARRs were randomly selected, and their hospital-level EMR data across HHN institutions were reviewed. There was no EMR data available for 299 patients, leaving 507 NARRs to review (Figure 1). Of these NARRs, 316 had received one or more colonoscopies prior to the invitation, leaving 191 patients who responded to the invitation and had not previously been screened. Among these 191 patients, 54 received a colonoscopy, and 17 underwent gFOBT within the follow-up time frame. However, 120 (62.8%) of the 191 NARRs who had not previously been screened remained unscreened at the end of the study period.
Demographics, screening, and cancer frequencies for a cohort of NBCCSP invitees from 2016 to 2017.
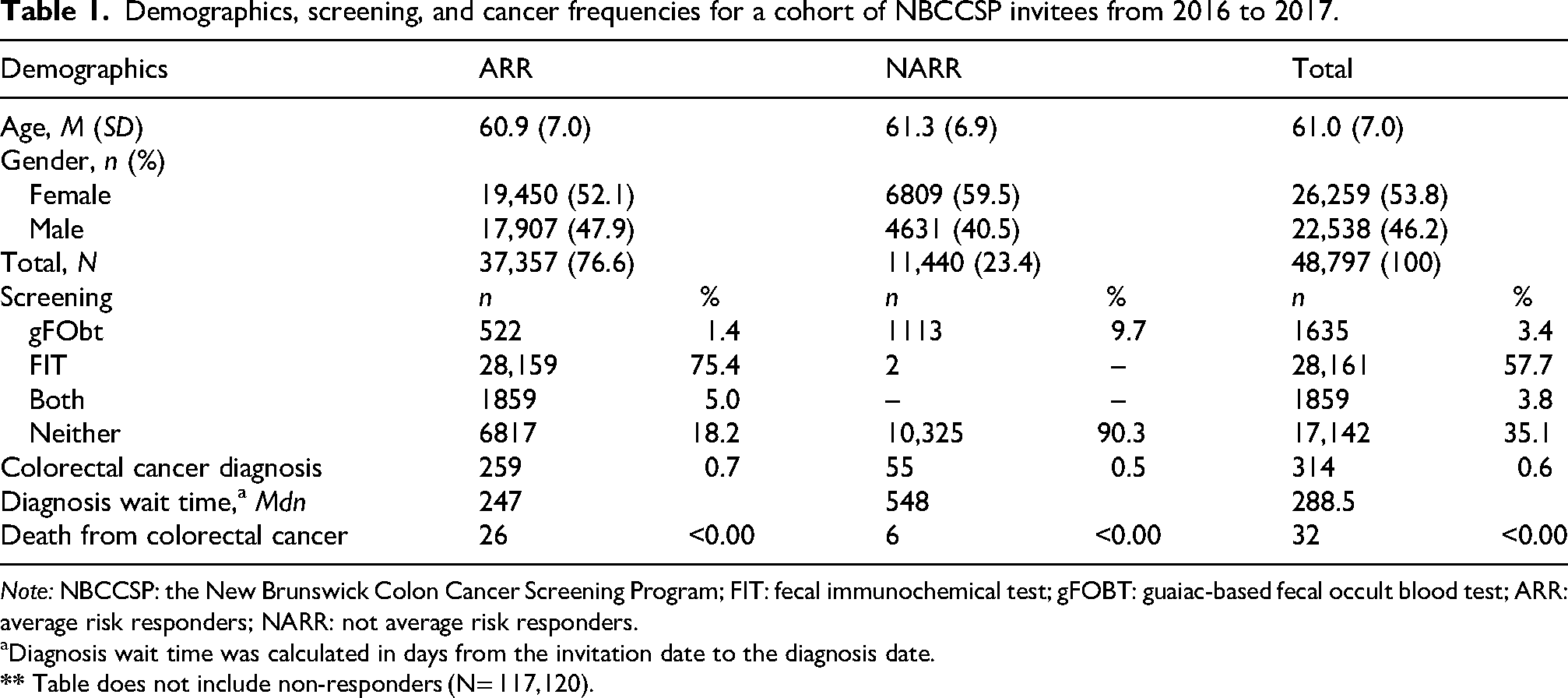
Note: NBCCSP: the New Brunswick Colon Cancer Screening Program; FIT: fecal immunochemical test; gFOBT: guaiac-based fecal occult blood test; ARR: average risk responders; NARR: not average risk responders.
Diagnosis wait time was calculated in days from the invitation date to the diagnosis date.
The comparison, using the available provincial data, between the NARR and ARR groups regarding the time to colon cancer diagnosis (time from program invitation date to diagnosis date) was performed. The time variable was normally distributed for the NARR group (n = 54) but not for the ARR group (n = 259), which was positively skewed. Therefore, the nonparametric Mann–Whitney U test was conducted to compare the distribution of time to colon cancer diagnosis between the ARR group (Mdn = 247, IQR = 469, n = 259) and the NARR group (Mdn = 548, IQR = 451, n = 54). Results of the Mann–Whitney U test indicated the NARR group experienced significantly more days to cancer diagnosis than the ARR group, U = 4631.5, z = −4.07, p < .001.
The matched case-control study found the NARR group waited on average 299.1 days longer for colonoscopy than the ARR group. Figure 1 outlines the selection and matching process for the 54 matched pairs. The mean age of the 60 females and 48 males was 60.1 years (SD = 7.1). Two participants were excluded due to multivariate outliers. A weighted least squares regression was conducted to mitigate the effects of unequal variances and heteroscedasticity. The inverse of the variance for each group was used as the weight. Control variables (i.e. year, age, and sex) significantly predicted colonoscopy wait time (CWT) (F = 34.57, p < .0001). After controlling for matched variables, group membership significantly predicted CWT (F = 27.85, p < .0001), uniquely explaining 11.0% of the variance. Of the control variables, age (b = −.62, t = −8.16, p < .0001) and year (b = −.17, t = −2.28, p = .03) significantly predicted CWT (see Table 2). Notably, the NARR group waited significantly longer for their colonoscopy (x̅ = 489.5 days) compared to the ARR group (x̅ = 190.4 days; b = .34, t = 5.28, p < .0001). Cohen's f2 for group after controlling for matched variables was .28, representing a medium effect size. The median CWTs for the NARR and ARR groups were 460 and 146 days, respectively.
Summary of hierarchical regression analysis for control and group variables predicting colonoscopy wait time.
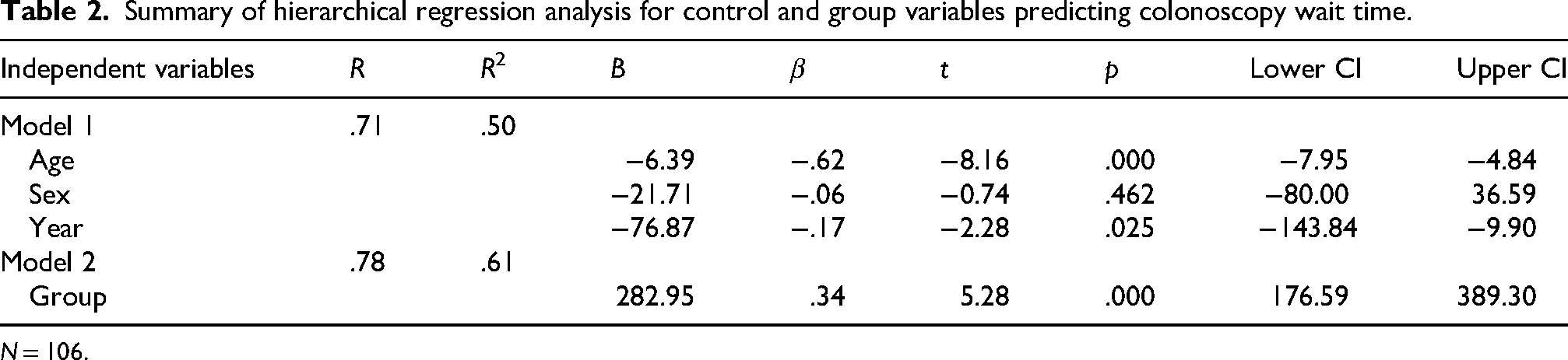
N = 106.
Discussion
The NBCCSP screens many ARRs, whereas NARRs are rejected from the program. As a result of the 2016 and 2017 NBCCSP invitations, over 30,000 ARR submitted an FIT. Many residents rejected from the NBCCSP may be followed by their primary care provider; however, some residents do not have access to primary healthcare providers. 13 We found that some NARRs may be falling through the cracks, as over half of the NARRs in the randomly selected sample, with available EMR data, who did not receive a colonoscopy prior to the invitation response, also did not have any CRC screening (FIT, gFObt, or colonoscopy) documented in their health records during the follow-up period. For NARRs, who were not previously receiving colonoscopies, wait times for colonoscopies were almost a year longer compared to ARRs. The NARR group also experienced significantly more days to cancer diagnosis than the ARR group.
Based on our data, it is clear that NARRs who did not have a colonoscopy within the specified time frame would benefit from programmatic screening. There is considerable heterogeneity in how CRC screening programs are implemented and organized across Canada and internationally. 14 For instance, some Canadian provinces adopt more inclusive screening pathways for individuals at elevated risk, such as British Columbia's program's facilitation of colonoscopy as a primary screening strategy for patients at higher risk,15,16 and Nova Scotia's practice of automatically mailing FIT kits to all Nova Scotians with a valid health card aged 50 years and older. 17 Evaluating alternate strategies utilized in other jurisdictions may provide insights on how to improve care and screening pathways for NARR individuals. Further research is needed to evaluate the effectiveness, feasibility, and equity of integrating alternative approaches to meet the needs of the population.
Programs within Canada and other settings should aim to fulfill all essential International Agency for Research on Cancer criteria for organized screening, as permitted by local resources. In our provincial jurisdiction, the NBCCSP is a Government of NB (GNB) run and funded initiative that is an active member of the National Colorectal Cancer Screening Network, under the Canadian Partnership Against Cancer. As such, the GNB's Department of Health working group for the NBCCSP would need to involve these stakeholders, the Regional Health Authorities, and healthcare provider stakeholders in revising and implementing changes to its program and associated policies. Patient partners could also be involved in these conversations so that program initiatives are effective, equitable, and patient-centered.
Implementing changes to the NBCCSP and associated policies to improve programmatic screening and help close the gap for NARRs who may be falling through the cracks may increase participation in the NBCCSP; thus, increasing costs. However, this cost should be acceptable to the GNB, given that the mandate of the NBCCSP is to reduce the incidence and mortality of colon cancer via “population-based” screening.
Notably, participation in the NBCCSP (29.5% response rate) was well below both the national Canadian target (≥60%) and average (49%), but comparable with some lower-performing Atlantic provinces such as Newfoundland and Labrador and Prince Edward Island.18,19 This underscores an opportunity for targeted and tailored approaches among population groups, including underscreened groups, to improve screening uptake. 18
Strengths and limitations
This study addresses an important and under-explored systems-level issue in CRC screening and raises important concerns regarding unintended consequences of program eligibility criteria. A major limitation of this study was the lack of retrospective data availability at the provincial level. Specifically, administrative billing data on the performance of colonoscopies could not be linked to the NBCCSP NARR group, nor was full cancer diagnostic data. Thus, regional-level data were used in these specific analyses. As such, information regarding procedures conducted outside of HHN facilities and the province were not captured. NBCCSP data also did not include identifiers of those in the NARR group who had a colonoscopy in the past 5 years; as such, they could not be excluded. However, all those in the NARR group with EMR data showing a colonoscopy during this pre-invitation period were excluded from our conducted analyses. Further research, including a longitudinal investigation of the cancer screening and cancer trajectories of the NARR group, as compared to the ARR group, would help to better clarify the clinical implications of the current screening practices.
Supplemental Material
sj-pdf-2-cri-10.1177_25160435261464428 - Supplemental material for The New Brunswick Colon Cancer Screening Program: Are above-average-risk New Brunswick residents falling through the cracks?
Supplemental material, sj-pdf-2-cri-10.1177_25160435261464428 for The New Brunswick Colon Cancer Screening Program: Are above-average-risk New Brunswick residents falling through the cracks? by Tracy A Freeze, Natasha Hanson, Leanne Skerry and Stephen A Smith in Journal of Patient Safety and Risk Management
Footnotes
Author contributions
Dr Tracy Freeze (PhD) is a research methodologist and contributed to the study design, data acquisition, data analysis, interpretation of data, drafting, and revision of the manuscript. Dr Natasha Hanson (PhD) is a research manager and contributed to the study design, drafting, and revision of the manuscript. Leanne Skerry (MA) is a research coordinator and contributed to the acquisition of data, as well as the drafting and revision of the manuscript. Dr Stephen Smith (MD) is a colorectal surgeon and contributed to the study conception, design, interpretation of data, and revision of the manuscript. All authors gave final approval for the manuscript to be published.
Ethical considerations
A waiver of informed consent for secondary use of data was requested and granted from the Horizon Health Network's Human Research Protection Program, inclusive of the Research Ethics Board (File # RS 2020-2923).
Consent to participate
A waiver of informed consent for secondary use of data was requested and granted from the Horizon Health Network's Human Research Protection Program, inclusive of the Research Ethics Board (File # RS 2020-2923), as the study involved retrospective/secondary use of previously collected data and met all relevant TCPS2 Article requirements for a waiver of consent.
Consent for publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Dr Natasha Hanson, PhD.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.