
Abstract
Background
Near-miss recognition is important in home-visit nursing because it enables patient-safety risks to be identified before they reach older clients in less regulated home environments. This study investigated factors related to near-miss recognition among home-visit nurses caring for older adults and visualized these factors using quantitative content analysis.
Methods
A cross-sectional anonymous online questionnaire was conducted among home-visit nurses in Japan with at least 3 years of experience. Of 237 collected responses, 177 were valid and included in the analysis. Participants reported the patient-safety risk category and provided free-text descriptions of factors related to near-miss recognition. Japanese text was analyzed using KH Coder in two steps: automatic word-frequency extraction followed by manual vocabulary refinement. A co-occurrence network was generated using the Jaccard index.
Results
Near-miss recognition was frequently reported in medication management, visit scheduling, and physical assistance. The co-occurrence network highlighted four factors: client participation in medication management, team-based sharing of visit schedules, physical assistance via comprehensive observation, and experience-based sensitivity to subtle incongruity. Recognition involved procedural actions and experience-based judgments. Participants monitored clients’ residual capacities and residential environments to ensure patient safety.
Conclusions
Near-miss recognition in home-visit nursing for older adults was supported by client participation, team-based sharing, comprehensive observation, and experience-based sensitivity. These results suggest the need to compare near-miss recognition across various care settings and translate experience-based judgment into explicit knowledge to support patient safety for novice home-visit nurses.
Background
Globally, many older adults prefer to age in place and receive home-based care when long-term care is needed, 1 a trend evident in Japan, too. 2
Thus, the need for home-visit nursing among older adults is growing, but home environments are less regulated than hospitals and pose unique safety risks, 3 including limited space, environmental clutter, insufficient professional communication, and increasing task complexity.4–7 Within this risk-laden context, home-visit nurses are constantly mindful of predicting and avoiding patient safety risks. 8
In international terminology, patient safety incidents include near misses, no-harm incidents, and harmful incidents. Near misses are incidents that could have harmed a patient but do not reach the patient, whereas no-harm and harmful incidents do. 9 Because near misses occur more frequently than harmful incidents and often share similar root causes, 10 they provide valuable opportunities to identify vulnerabilities in care processes and strengthen preventive safety practices before risks reach the patient. However, near-miss reporting is limited by organizational culture, lack of reporting systems, and fear of blame. 11
Near-miss recognition is important in home-visit nursing because it involves identifying patient safety risks before they reach older clients. Existing research has primarily focused on incidents that reach patients, with less attention to how home-visit nurses recognize and respond to earlier-stage risks. Therefore, this study investigated factors related to near-miss recognition among home-visit nurses caring for older adults and visualized these factors using quantitative content analysis.
Methods
Study design
This study employed quantitative content analysis to uncover qualitative aspects within overlooked textual data. 12
Participants and recruitment
Participants were practicing home-visit nurses in Japan with at least 3 years of experience in home-visit nursing for older adults. Nurses working exclusively in psychiatric or pediatric home-visit nursing were excluded.
Participants were recruited by the first author through multiple voluntary routes. The primary route involved using publicly available lists of certified nurse specialists and certified nurses to identify home-visit nursing services employing these nurses. Administrators at 51 of the 76 contacted services (67.1%) permitted dissemination of the study information to their nurses; these services received a written study information sheet with the online form URL. To protect anonymity and voluntariness, administrators were asked only to distribute the study information and were not asked to report how many nurses received it. Interested nurses reviewed the written study information and independently accessed the online form. Informed consent was obtained when participants clicked the consent button. Limited supplementary recruitment was also conducted through local home-visit nursing service associations and existing research team networks to reach administrators of home-visit nursing services. Because these supplementary routes included indirect access to administrators, the exact number of services that ultimately disseminated the study information to nurses could not be determined.
Data collection
Data were collected between August 2024 and March 2025 using a cross-sectional anonymous online questionnaire in Japanese on patient safety in home-visit nursing for older adults. The questionnaire first collected participants’ overall nursing and home-visit nursing experience and the patient-safety risk category associated with near-miss recognition. The primary data consisted of free-text descriptions of factors related to near-miss recognition, while descriptions of the recognized situations were collected as supplementary contextual information. Each participant completed the questionnaire only once and was asked to provide one free-text response describing the most recent near-miss recognition that they could clearly recall.
Near-miss recognition was operationally defined as a home-visit nurse recognizing an incorrect action, unsafe situation, or hazardous home environment in advance. This definition was intended to distinguish latent patient-safety risk recognition from recognition of no-harm or harmful incidents that had already reached the client. The questionnaire instrument was pretested with two experienced home-visit nurses.
For the analysis, the first author screened all responses and retained only those related to near-miss recognition. Classification was based on whether the nurse had proactively implemented patient-safety measures and whether the risk had reached the client. Final inclusion was determined through consensus among the research team.
Data analysis
Quantitative content analysis was conducted on Japanese text describing factors related to near-miss recognition using KH Coder (version 3.03a, official package) in two steps. 13 Morphological analysis used ChaSen with the IPA Part-of-Speech System Japanese Dictionary (IPADIC).
First, word frequencies were automatically extracted to minimize researcher bias. Function words, including particles and auxiliary verbs, and hiragana-only nouns, verbs, and adjectives, were excluded as stop words. Words segmented into semantically incomplete units by IPADIC were individually specified for forced extraction. Negated word forms were extracted as independent terms using an official KH Coder plugin. Second, vocabulary was refined by integrating synonymous words and excluding words with limited relevance to near-miss recognition factors, guided by contextual similarity. For example, the integrated term “Set” comprised “Set” and “Prepare” and also included “Arrange” only when it appeared adjacent to “Medication.” A co-occurrence network was then generated to visualize relationships among frequently co-occurring terms. Co-occurrence strength was measured using the Jaccard index, with a threshold of 0.2 to improve readability and interpretability. The analysis was led by the first author and iteratively discussed with coauthors experienced in quantitative content analysis and KH Coder.
Only report-relevant results were translated into English by the first author; the coauthors checked them against the original Japanese and reviewed them. Lexical distinctions in Japanese were preserved where possible; terms difficult to translate literally were translated contextually. Machine translation was used only as a supplementary aid. This study was reported in accordance with the STROBE statement. 14
Results
Of the 237 responses collected, 177 were valid; 60 were excluded because they described recognition related to no-harm or harmful incidents. Representative excluded responses included a no-harm incident in which a nurse realized that the scheduled visit time had already passed only after being contacted by the client, and a harmful incident involving bleeding during nail clipping. Regarding overall nursing experience, 3 participants had 3–4 years, 17 had 5–9 years, 46 had 10–19 years, and 111 had ≥20 years (Table 1). Regarding home-visit nursing experience, 45 participants had 3–4 years, 56 had 5–9 years, 40 had 10–19 years, and 36 had ≥20 years (Table 1). As shown in Table 1, medication-related near-miss recognition was most frequent (n = 71), followed by visit scheduling (n = 51) and physical assistance (n = 25), with fewer cases involving medical devices, information sharing, residential environment, and nursing records. From the free-text responses, 1277 unique words were extracted; 1043 remained after preprocessing, including stop-word removal. The mean frequency was 3.48 (SD = 13.38), reflecting a skewed distribution, with some highly frequent words. The common automatically extracted words related to near-miss recognition were “confirm” (Kakunin, 121 occurrences), “check” (Chekku, 23), and “information” (Jōhō, 20) (Table 2).
Participant characteristics and near-miss categories (N = 177).
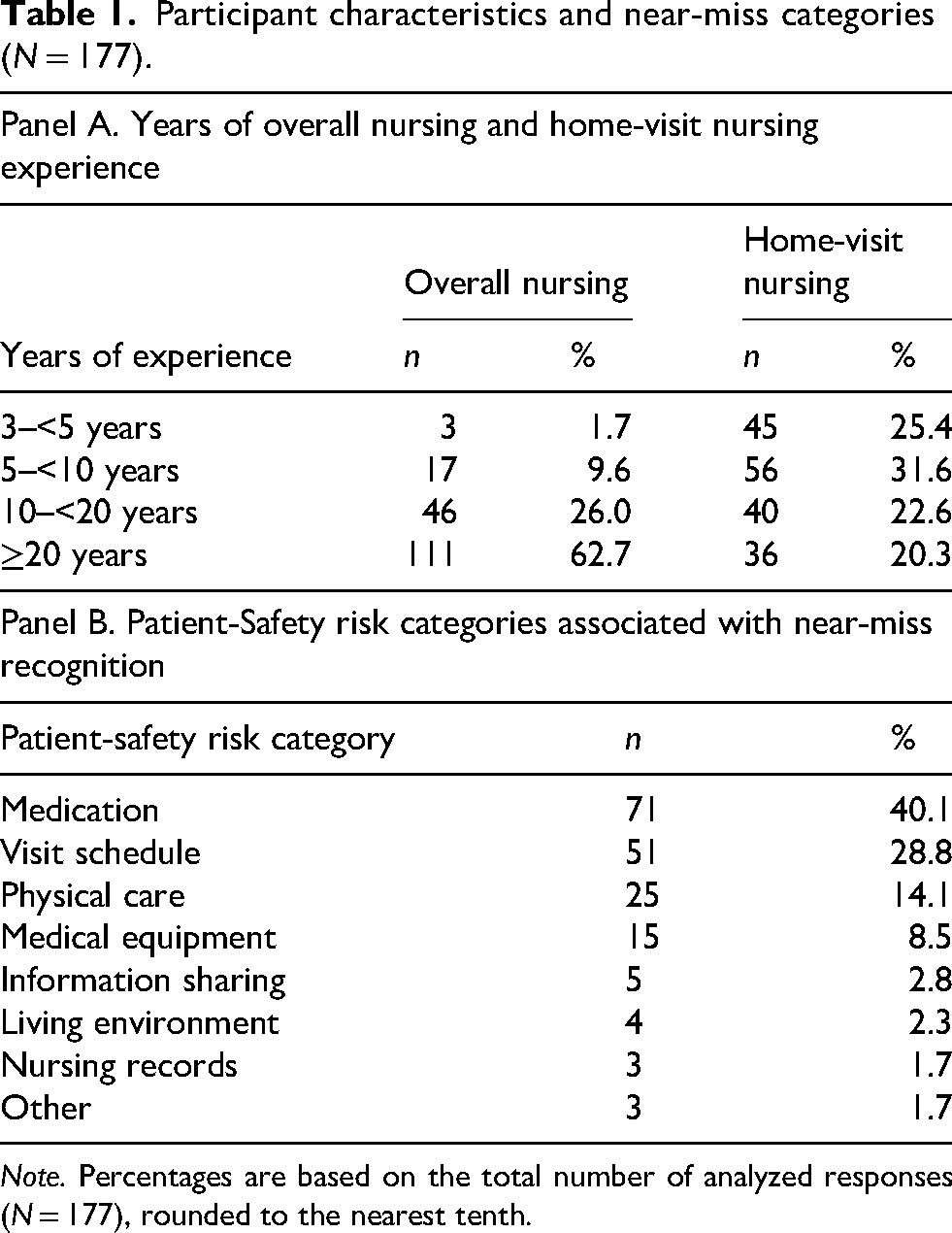
Note. Percentages are based on the total number of analyzed responses (N = 177), rounded to the nearest tenth.
Frequently occurring automatically extracted words.
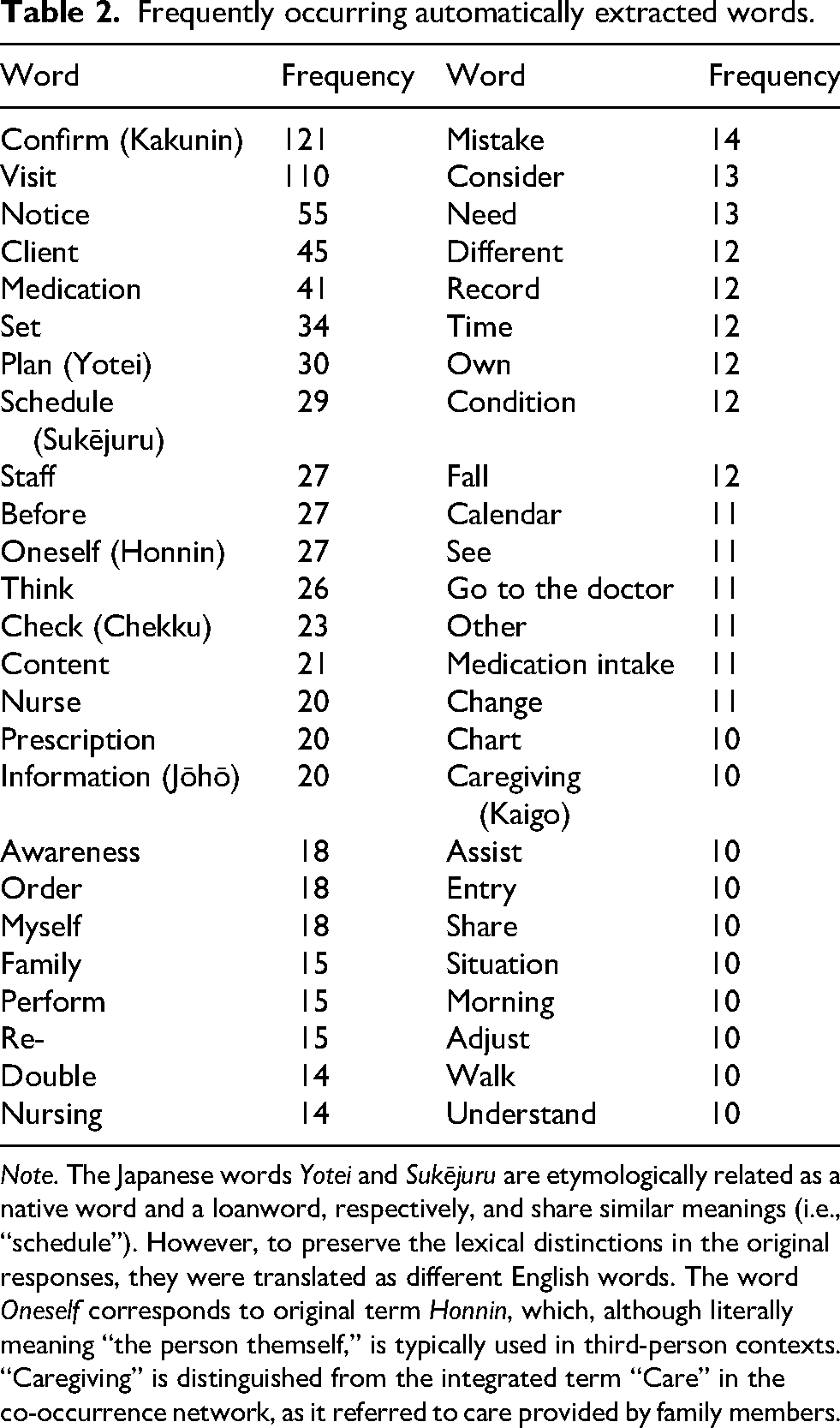
Note. The Japanese words Yotei and Sukējuru are etymologically related as a native word and a loanword, respectively, and share similar meanings (i.e., “schedule”). However, to preserve the lexical distinctions in the original responses, they were translated as different English words. The word Oneself corresponds to original term Honnin, which, although literally meaning “the person themself,” is typically used in third-person contexts. “Caregiving” is distinguished from the integrated term “Care” in the co-occurrence network, as it referred to care provided by family members.
Interpretation of the co-occurrence network
The co-occurrence network visualized semantic relationships among terms related to near-miss recognition in home-visit nursing (Figure 1).
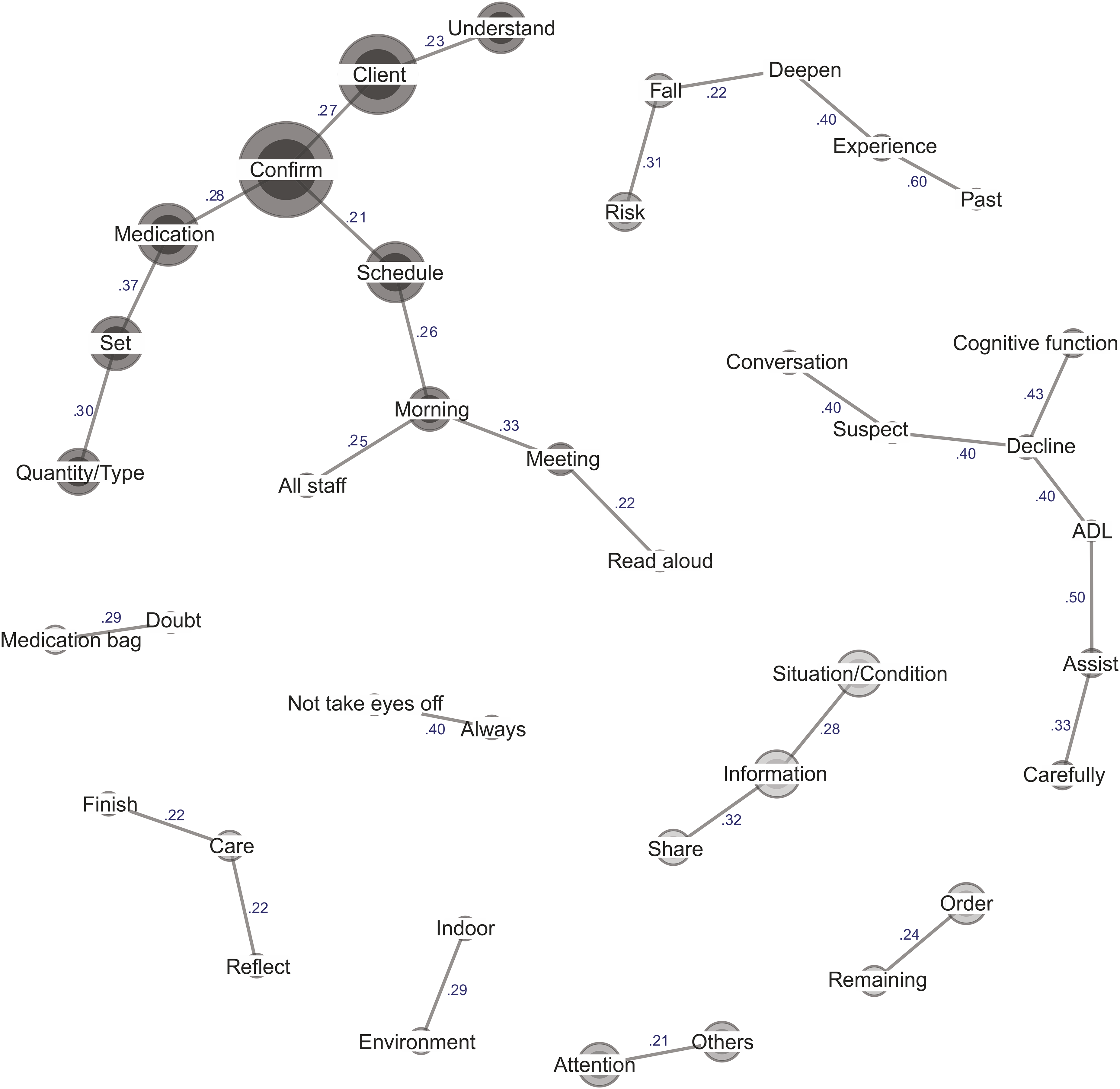
Co-occurrence network of near-miss recognition in home-visit nursing.
Client participation in medication management
Factors related to near-miss recognition were often reported in situations involving assistance with oral medication using pill calendars. Participants described methods for verifying whether the dispensed medications matched physicians’ orders, during which they detected errors. In the co-occurrence network, terms such as “medicine,” “confirmation,” “client,” “set,” and “quantity, type” were closely connected, reflecting the practice of double-checking medication content with clients. For example, one participant (10–19 years of nursing and home-visit nursing) described a case in which a discrepancy between the contents of dispensed medications and the prescription instructions was identified while setting oral medications, before the client took the medication, as follows: “Being aware that errors may remain after medications are dispensed, I was able to notice the discrepancy while setting the medications and confirming the quantity and type of each dose together with the client.”
Additionally, one participant noted that, although the client did not fully understand the medication's purpose, they could confirm dosage and schedule, enabling the nurse to identify an error. Although many older adults receiving home-visit nursing had physical and cognitive impairments, participants emphasized their residual capacities rather than deficits. When double-checking with clients was not feasible, participants verified remaining medications at each visit and confirmed adherence. In Japan, medications are typically dispensed in bags labeled with the client's name, drug, administration method, and quantity. Participants compared these bags with prescriptions and reflected on-site before leaving as an alternative approach to near-miss recognition.
Team-based sharing of visit schedules
For near-miss recognition related to visit scheduling, co-occurring terms included “schedule,” “morning,” “meeting,” “all staff,” and “read aloud.” These terms reflected morning meetings in which all staff read aloud and checked the day's visit schedule. One participant (≥20 years of nursing and home-visit nursing) reported, “While reading the visit schedule aloud during a morning meeting, I noticed that a visit was missing from the schedule and adjusted the schedule accordingly.” Unlike hospital nurses, home-visit nurses often work alone, outside the office. Thus, morning meetings may provide important opportunities for double-checking plans with others. Through group confirmation, participants reported receiving external attention, which contributed to the prior recognition of scheduling errors. This result suggests that ritualized routines, such as morning meetings, have a greater function than formal procedures; they elevate procedural behavior into meaningful practices for risk prevention.
Physical assistance via comprehensive observation
Near-miss recognition during physical assistance was expressed through co-occurrences such as “always–not take eyes off” and “carefully–assist,” commonly used in mobility and bathing support. One participant (≥20 years nursing; 10–19 years home-visit nursing) described taking extra caution during bathing because the client was undressed and the floor was slippery, stating, “I kept my hands on the client at all times and never took my eyes off the client.” This illustrates the vigilance required in home environments often unsuited for safety. The term “ADL” co-occurred with “assist” and “decline,” indicating greater caution when supporting clients with reduced function. Terms such as “indoor” and “environment” also appeared, describing actions such as increasing lighting intensity before nail care or clearing cluttered floors to reduce falls. Near-miss recognition during physical assistance involved monitoring both clients’ conditions and the physical environment.
Experience-based sensitivity to subtle incongruity
A co-occurrence—“conversation–suspect–decline–cognitive function”—showed how nurses adapted to older clients in home-visit nursing contexts where they could not remain constantly present. This pattern appeared in medication, equipment, and scheduling. For example, one participant (≥20 years of nursing; 10–19 years of home-visit nursing) described the following: “I suspected cognitive decline from the client's incoherent conversation. Because the client was also having difficulty, I proposed support with oxygen cylinder management, which enabled intervention without resistance and helped prevent unsafe behaviors, such as going out with an empty cylinder.”
Participants often assessed cognitive function intuitively during natural conversations without formal tools. Sensitivity to subtle incongruity appeared to be an important competency, represented by the co-occurrence “past–experience–deepen,” reflecting refinement of intuition over time. The co-occurrence “share–information–situation, condition” further emphasized the role of information exchange in client care.
Discussion
Implications for patient-safety practices in home-visit nursing
The importance of the four factors identified in this study—client participation, team-based sharing, comprehensive observation, and experience-based sensitivity to subtle incongruity—has also been noted in previous hospital nursing studies.15–18 However, home-visit nurses provide care alone during limited visits and within individualized private spaces. Therefore, the results may reflect distinctive characteristics of patient-safety practices in home-visit nursing.
In home-visit nursing, nurses’ face-to-face contact with clients is intermittent, making patient safety between visits a major concern. Previous research has suggested that supporting clients’ self-care abilities is important for patient safety in home-visit nursing. 19 Thus, client participation in medication management in this study may have supported not only error detection during visits but also patient safety between visits by increasing clients’ awareness.
In hospital settings, team-based sharing often focuses on patient information and care plans. 16 In contrast, home-visit nursing is embedded within clients’ individualized daily lives as one of multiple home-care services, making accurate visit scheduling important. Because visit scheduling requires coordination of clients’ needs and other services within unpredictable environments, 20 team-based sharing of visit schedules may represent a distinctive form of information sharing that supports patient safety in home-visit nursing.
In this study, comprehensive observation refers to observing both clients’ physical conditions and residential environments. Because home environments are not designed for care provision as hospitals are, 4 environmental adjustments may be needed for patient safety. However, as homes are also connected to residents’ identities, 21 home-visit nurses may need to balance safety-oriented environmental adjustments with respect for clients’ lifestyles.
Regarding experience-based sensitivity to subtle incongruity, hospital-based research has similarly reported that nurses’ subjective observations can help detect early changes in patients’ conditions. 18 However, home-visit nurses generally visit clients’ homes alone, limiting opportunities for immediate consultation and situational sharing. Previous research has also suggested that routinization of home-visit nursing care may reduce vigilance regarding patient safety. 8 Therefore, excessive reliance on an individual home-visit nurse's experience may pose patient-safety risks. Mechanisms may be needed to share experience-based cues among home-visit nurses and support timely communication and consultation during visits.
Limitations and future research
Several limitations should be noted. First, limiting each participant to a single response may have limited data volume and diversity. Second, self-reported responses may have introduced recall bias and subjective interpretation. Third, voluntary participation may have attracted nurses with greater patient-safety awareness. Fourth, detailed prior clinical backgrounds were not assessed, limiting interpretation of whether experience-based judgment stemmed from home-visit nursing-specific or broader clinical experience. Fifth, some original Japanese nuances may not have been fully conveyed. Finally, generalizability should be considered cautiously, as this study was conducted in Japan and the sample was biased toward experienced nurses. Future research is needed to compare near-miss recognition across home-visit nursing, hospital nursing, and long-term care facility nursing, and to examine how experience-based judgment can be translated into structured observation points and other explicit knowledge for novice home-visit nurses.
Conclusions
This study visualized factors related to near-miss recognition in home-visit nursing for older adults using quantitative content analysis. The frequently reported patient-safety risk categories were medication, visit scheduling, and physical assistance. The corresponding recognition factors highlighted the importance of client participation in care, team-based sharing, comprehensive observation that included indoor environments, and experience-based sensitivity to subtle incongruity. These results may provide a basis for comparing near-miss recognition across home-visit nursing, hospital nursing, and long-term care facility nursing. Future research should compare near-miss recognition across care settings and examine how tacit knowledge embedded in experience-based judgment can be translated into explicit knowledge for novice home-visit nurses.
Footnotes
Acknowledgements
The authors extend their gratitude to home-visit nurses who generously contributed their time and insight to this study.
Ethical considerations
This study was approved by the Ethics Review Board of the Graduate School of Medicine, Nagoya University (Approval No. 2024-0137) on July 24, 2024.
Consent to participate
Written explanations of the study objectives, procedures, and ethical considerations were provided to all participants. Participants provided informed consent by clicking a consent button on the online form.
Consent for publication
Not applicable. No identifiable personal data are included in this manuscript.
Authors’ contributions
Kazuma Haida contributed to the conceptualization and design of the study, acquisition and analysis of data, and interpretation of the findings. He also drafted the manuscript and was responsible for funding acquisition, project administration, and visualization. Takahiro Tanaka and Miyuki Ishibashi supervised the study, validated the findings, and critically reviewed the manuscript for important intellectual content. All authors have read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Yuumi Memorial Foundation for Home Health Care (grant number 2023B101-005).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the study's findings may be available from the corresponding author upon reasonable request. The data are not publicly available because of privacy and ethical restrictions.
Guarantor
Kazuma Haida