
Abstract
Background
Methotrexate (MTX) is a dangerous drug that can cause serious adverse effects. It is teratogenic and contraindicated during pregnancy. Community pharmacists play a key role in MTX risk management and in ensuring its safe and effective use. This research aims to explore the levels of implementing the required measures to provide MTX safely by community pharmacists in Jordan.
Methods
This was a cross-sectional questionnaire-based study. The study population comprised all pharmacists and pharmacy technicians working at community pharmacies in Amman, Jordan. A questionnaire designed to capture the intended outcomes was developed by the researchers based on a review of the essential measures needed to dispense MTX safely.
Results
A low level of adherence to implementing risk management measures was generally observed among research participants. Notably, 95.1% reported that they rarely request a negative pregnancy test from young female patients before dispensing MTX. Counselling the patients about the impact of taking MTX during pregnancy and the need to avoid breastfeeding while taking MTX were the most widely implemented risk management measures (although still sub-optimal). Counselling about avoiding infections and regarding sun exposure was provided by almost 50% of research participants for each measure.
Conclusion
Findings of this study are alarming, and they call for certain revisions of the current pharmacy practice in Jordan when it comes to dispensing high-risk medications. Based on the findings of the current study, several practice-related recommendations can be proposed to enhance the safe dispensing of MTX in community pharmacy settings.
Introduction
Methotrexate (MTX) is a folic acid analogue that is widely used to treat several types of cancers and resistant forms of autoimmune diseases, such as rheumatoid arthritis and psoriasis.1,2
MTX has a narrow therapeutic index and can cause serious adverse effects, such as bone marrow suppression and liver toxicity. 3 It is teratogenic and contraindicated during pregnancy because it carries a high risk of major birth defects, miscarriage, and foetal death. 4
Before starting MTX therapy, a comprehensive patient assessment is required. Laboratory testing including a complete blood count, renal function tests (serum creatinine, blood urea nitrogen, and urinalysis), and liver function tests (serum bilirubin, AST, ALT, serum albumin) should be conducted. Furthermore, when prescribing MTX to any female of reproductive age, the use of effective contraceptive methods is mandatory and the patient must be counselled about its teratogenic risks. 4
Community pharmacists play a key role in MTX risk management and in ensuring its safe and effective use because of their high accessibility and their frequent, close interactions with patients.4,5 Their roles include verifying prescriptions, confirming correct weekly dosing, detecting potential drug interactions and contraindications, providing patient education on proper medication use, and promoting adherence to treatment regimens (emphasizing adherence to the once-weekly regimen and the importance of regular monitoring), follow-up on laboratory testing, and reporting of adverse drug reactions.4,6,7 Despite available national guidelines and safety recommendations for dispensing MTX, studies have shown that these recommendations are applied inconsistently and poorly implemented in community pharmacy settings.8–12
In Jordan, the concept of risk management specific to MTX dispensing has not been widely addressed in Jordanian pharmacy literature. This article aims to explore the levels of implementing the required measures to provide MTX safely by community pharmacists in Jordan.
Methods
This was a cross-sectional questionnaire-based study. Data were collected between September 2024 and June 2025. The study population comprised all pharmacists and pharmacy technicians working at community pharmacies in Amman, Jordan. No restrictions for inclusion were applied to research participants from the mentioned population. Convenient sampling was used to achieve the required sample. A questionnaire designed to capture the intended outcomes was developed by the researchers based on reviewing the essential measures needed to dispense MTX safely. The questionnaire in its online form was used by two research assistants who conducted the interviews anonymously with research participants face-to-face at their workplaces after gaining their verbal consent. The questionnaire consisted of five main parts: participant characteristics (four questions), pregnancy and breastfeeding (nine questions with three options for the answers; rarely, sometimes, and always), adverse reactions to MTX (one multiple responses question and three yes or no questions), periodic lab tests (three questions with three options for the answers; rarely, sometimes, and always), and finally one yes or no question regarding counselling about the correct method to take MTX. Data analysis and cleaning were carried out using the Statistical Package for the Social Sciences Version 25. The research was granted ethical approval from the Institutional Review Board (IRB) at Middle East University (MEU) with approval number of (825-2025/2026).
Results
The study included a total of 265 responses from community pharmacists who fit the inclusion criteria. The general characteristics of research participants are shown in Table 1.
General characteristics of study sample.
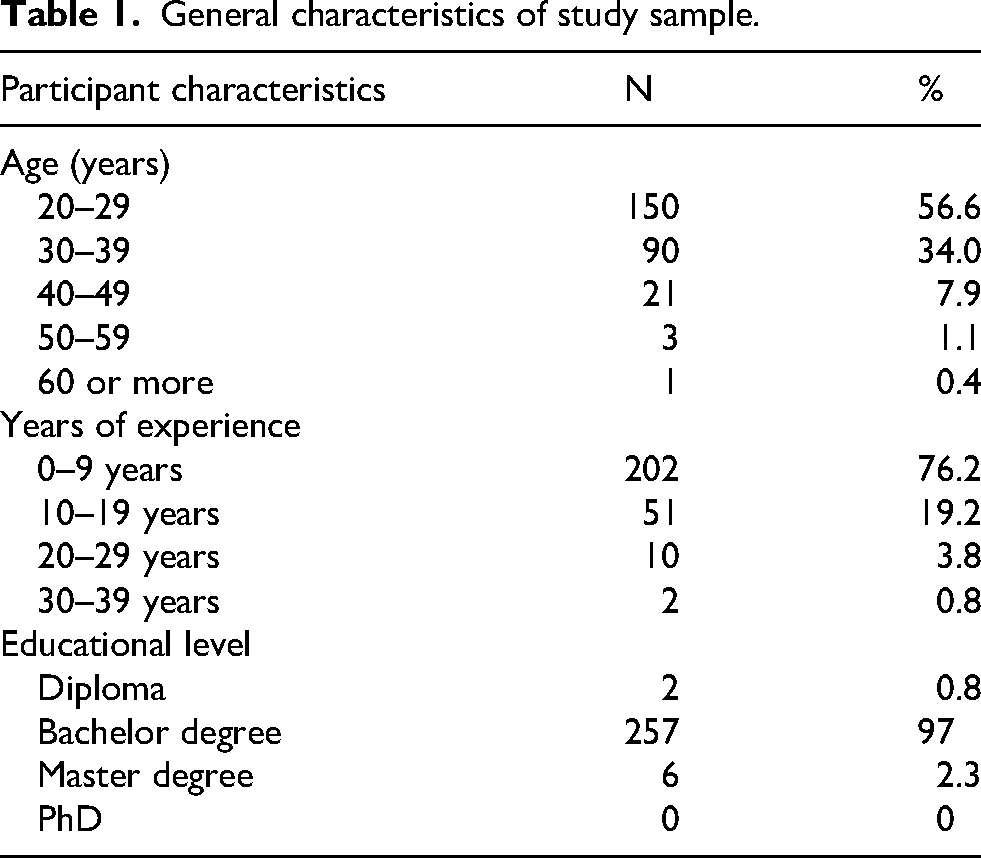
The youngest age group (20 to 29 years) comprised more than half of the study sample, and the age group from 30 to 39 years comprised almost one third. This was also reflected in the years of experience of research participants as 76.2% had up to 9 years of experience and 19.2% had from 10 to 19 experience years. Moreover, the vast majority of respondents (97%) were bachelor’s degree holders.
The frequency of providing pharmaceutical counselling regarding risk management measures to prevent foetal and neonatal exposure to MTX is shown in Table 2.
Risk management measures to prevent foetal and neonatal exposure to methotrexate.
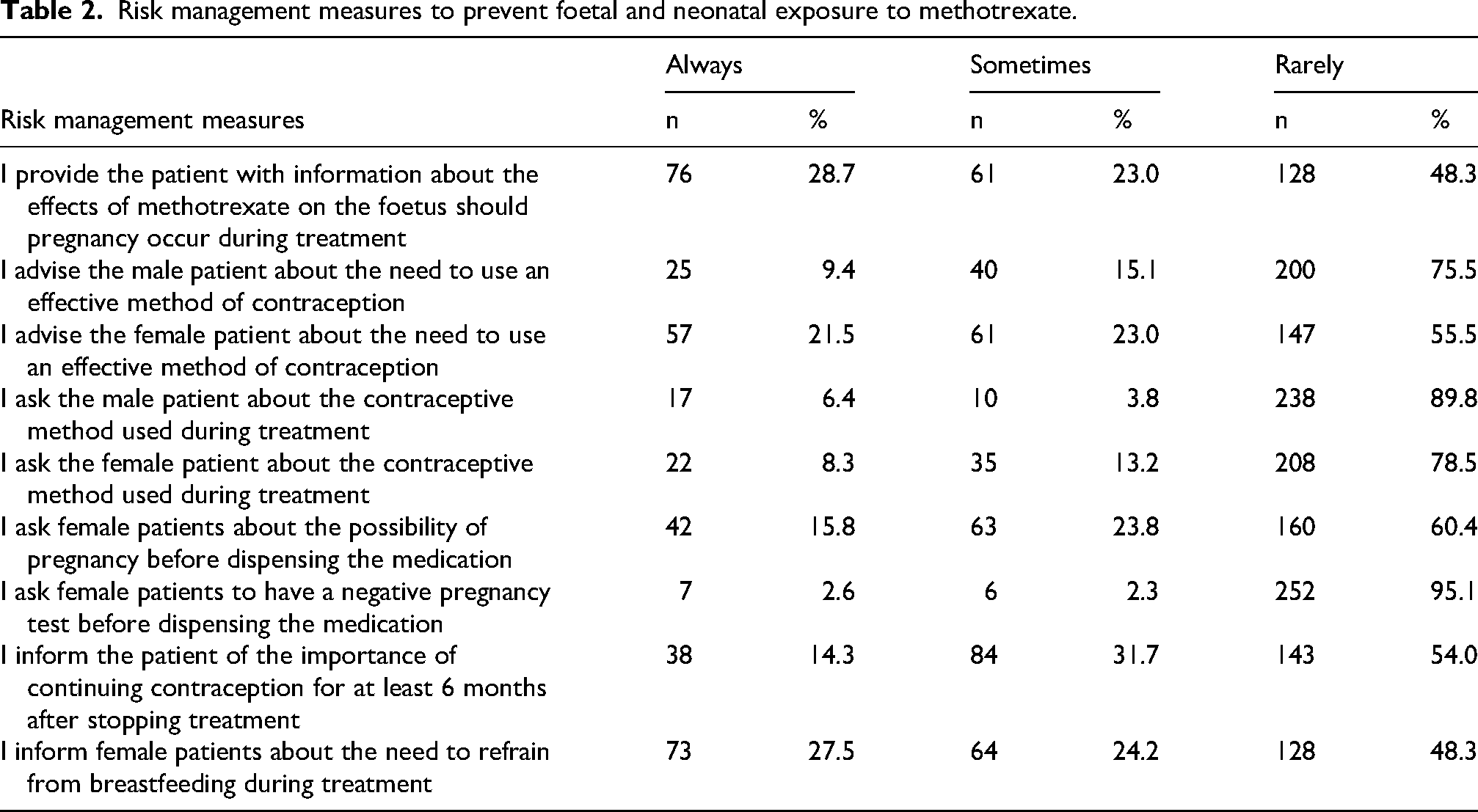
A low level of adherence to implementing risk management measures was generally observed among research participants. For each risk management measure, the majority of respondents reported that they rarely implemented the measure. Notably, the vast majority of participants (95.1%) reported that they rarely request a negative pregnancy test from young female patients before dispensing MTX. Counselling the patients about the impact of taking MTX during pregnancy and the need to avoid breastfeeding while taking MTX were the most widely implemented risk management measures (although still sub-optimal). Research participants reported that they always implemented the aforementioned measures in 28.7% and 27.5% of the cases, respectively.
The researchers used chi-square test to explore any associations between the characteristics of research participants and the frequency of implementing risk management measures to prevent foetal and neonatal exposure to MTX, and the results are shown in Table 3.
Association between characteristics of study sample and risk management measures to prevent foetal and neonatal exposure to methotrexate.
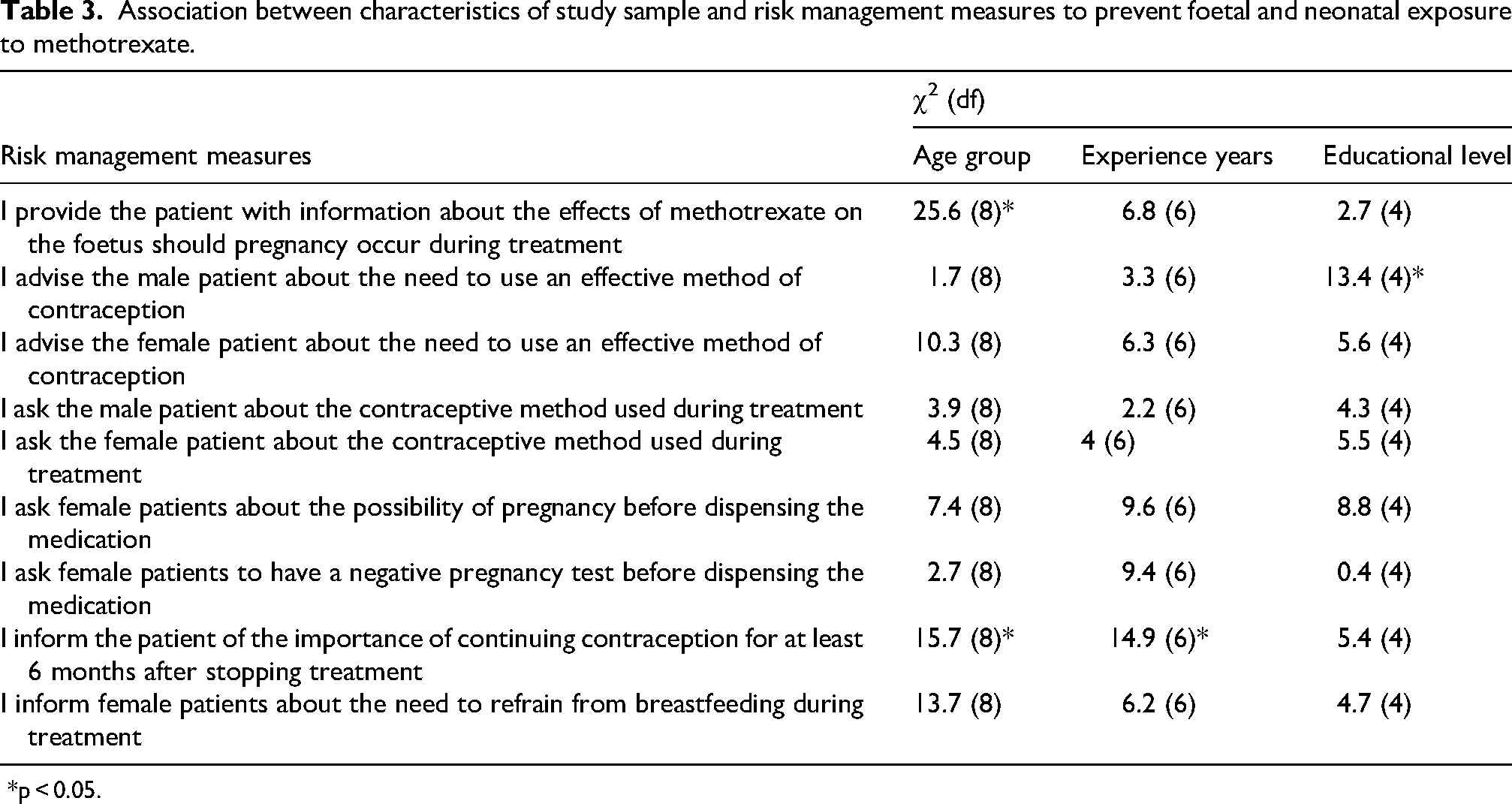
*p < 0.05.
Table 3 shows that the age group of respondents was significantly associated with providing the patient with information about the effects of MTX on the foetus during pregnancy χ2(8) = 25.6, p < .05, and informing the patient of the importance of continuing contraception for at least 6 months after stopping treatment χ2(8) = 15.7, p < .05. Additionally, the years of experience gained by research participants was significantly associated with informing the patient of the importance of continuing contraception for at least 6 months after stopping treatment χ2(6) = 14.9, p < .05. And educational level was significantly associated with advising the male patient about the need to use an effective method of contraception χ2(4) = 13.4, p < .05.
As for attempts to minimize MTX adverse drug reactions, responses of research participants are shown in Table 4.
Measures to minimize adverse drug reactions to methotrexate.

The most commonly implemented measure to prevent MTX adverse drug reactions was counselling about avoiding contact with any infected patients (implemented by 55.5% of research participants). This was followed by advising patients about the need to avoid sun exposure while on MTX treatment (50.9%), and counselling the patients to wash their hands or to avoid direct skin contact with the drug (8.7%).
The researchers also explored the most common adverse drug reactions mentioned by the pharmacists taking part in the research while dispensing MTX. These are found in Table 5.
Adverse drug reactions mentioned by pharmacists during counselling.

The most commonly mentioned adverse drug reaction was having a high fever, chills, general fatigue, muscle pain, or sore throat may indicate an infection (mentioned by 72.5% of participating pharmacist). On the other hand, the least mentioned adverse drug reaction was bleeding in its different forms (Bleeding gums, blood in the urine, vomiting blood, or unexplained bruising may indicate blood problems), as it was mentioned only by 9.8% of respondents.
Finally, pharmacists taking part in the study were asked whether they recommend periodic lab tests for patients being treated with MTX. The responses are presented in Table 6.
Periodic lab tests recommended by pharmacists.

Responses of research participants showed that the most commonly recommended tests were liver function tests, followed by kidney function tests and comprehensive blood tests; these were always recommended by 6.4%, 5.3%, and 3.4% of respondents, respectively.
Discussion
To the best of our knowledge, this is the first study that explores pharmacists’ knowledge and dispensing practices related to MTX in the Middle East. Only a limited number of studies have addressed this topic, which limits our ability to compare our findings with those reported in the literature.
Since community pharmacists are often the final point of contact with patients before administration of medications, they help bridge the gap between prescribing and use. However, the findings of this study revealed a significant deficiency and inconsistency in the implementation of risk management practice in routine practice in Amman. Pharmacists play an important role in managing reproductive risks associated with teratogenic medications such as MTX.13,14 However, this study demonstrated a significant gap in community pharmacists’ practice regarding patient counselling and pregnancy risk management. This study revealed a notable deficiency in counselling related to the importance of effective contraception during MTX therapy and for an appropriate period after its discontinuation.
Only 28.7% of pharmacists consistently counsel patients about foetal harm if pregnancy occurs, and only 15.8% regularly ask about the possibility of pregnancy before dispensing MTX. The practice of requiring a negative pregnancy test before dispensing is also uncommon, as only 2.6% always request a negative pregnancy test before dispensing, while as many as 95.1% rarely do it. Previous studies indicated that a considerable gap may exist between safety guidelines and practice in relation to drug dispensing, especially concerning hazardous drug use and pregnancy, such as MTX. Only a minority of community pharmacist provide pharmaceutical care in this area and consistently counsel on foetal harm or actively inquire about pregnancy status, with even fewer requesting negative pregnancy tests.15–17
A recent cross-sectional study found that about 57% of community pharmacists in Saudia Arabia were not prepared to safely dispense medications during pregnancy. 17 Research conducted in the Canadian setting found that although many pharmacists are knowledgeable about the reproductive risks associated with MTX and its derivatives, the implementation and adoption of structured risk assessment strategies in practice remain limited. 16 Additionally, recent research from Addis Ababa highlighted gaps and variations in community pharmacists’ knowledge and practice regarding medication safety during pregnancy, highlighted the need for targeted training and continuous education programs. 18
A deficient level of contraception counselling was also observed. Only 21.5% of pharmacists always advised female patients to use effective contraceptive methods, and merely 9.4% consistently provided guidance to male patients regarding contraception. Furthermore, fewer than 10% regularly asked patients about the type of contraceptive method used. Although data on pharmacists’ practices in providing contraception guidance during MTX treatment is limited, it is well known that women and men should use contraception during treatment and for a period after discontinuation. 19 Both the EMA and FDA advise strict pregnancy avoidance and strongly recommend providing counselling to all patients.20,21
Beyond reproductive safety, pharmacists’ efforts to prevent MTX-related adverse drug reactions were inconsistent. Slightly more than half of respondents advised patients to take precautions to prevent infection (55.5%) or avoid sun exposure (50.9%). These figures are inconsistent with established practice guidelines, where structured infection risk counselling and education are essential components of patient management. 22 Current EULAR recommendations highlight the importance of infection risk management. The risk of infection should be discussed with every patient before initiating MTX, and this risk should be periodically reassessed. Patients taking MTX should be advised to report fever, sore throat, or any other signs of infection as soon as they notice them, so infection can be recognized and treated early. 23
Counselling on safe handling practices was also reported by only 8.7% of pharmacists. This is particularly concerning since MTX is classified as a hazardous drug. MTX may contact the skin during dispensing or when tablets are manipulated, which can create an occupational risk for caregivers and pharmacy staff. This concern is especially relevant for those who are pregnant or planning a pregnancy. 24 A similarly low level of counselling on occupational exposure risks has also been reported in healthcare settings in low- and middle-income countries. In these countries, worker safety measures are often not fully implemented, and counselling about hazards and different types of workplace risks is rare. 25
Inconsistent practice regarding the recognition of adverse drug reactions was also reported by community pharmacist. While 72.5% of participants referred to signs suggestive of infection, Jaundice was rarely recognized (13.23%) as a warning sign, and indicators of marrow toxicity were largely ignored (fewer than 10%). Hepatotoxicity and bone marrow suppression are commonly associated with MTX therapy, which may be dose-related or deteriorated by impaired drug clearance, and may appear with subtle or nonspecific symptoms that require close patient surveillance.26,27 Failure to inform patients of these warning signs may postpone diagnosis and result in avoidable harm.
MTX is associated with several serious side effects, including hepatotoxicity, nephrotoxicity, and myelosuppression.4,28,29 Therefore, regular laboratory monitoring is essential for the early detection of MTX toxicity. Pharmacy services can play a key role in improving adherence to recommended laboratory monitoring, including complete blood counts as well as liver and kidney function tests, through patient counselling and collaboration with prescribers. 30 However, this study highlighted a critical gap in community pharmacists’ practice regarding routine laboratory monitoring; only a small proportion consistently recommended appropriate laboratory monitoring, including liver function tests (6.4%), kidney function tests (5.3%), and complete blood counts (3.4%).
This research was limited by the number of pharmacists taking part in the interviews. Moreover, it was limited by the scarcity of the available evidence from Jordan and the surrounding countries which limited our ability to compare the status quo in Jordan with different experiences.
Conclusions
Findings of this study are alarming, and they call for certain revisions of the current pharmacy practice in Jordan when it comes to dispensing high-risk medications. Based on the findings of the current study, several practice-related recommendations can be proposed to enhance the safe dispensing of MTX in community pharmacy settings. National guidance focused on MTX dispensing should be developed or adapted for use in community pharmacies. Using a dispensing checklist for high-risk medicines such as MTX can help ensure that patients are well informed about the key information at the point of dispensing.
Additionally, community pharmacists should play a stronger role in supporting and ensuring appropriate laboratory monitoring. Promoting pharmacists’ role in the follow-up process and enhancing adherence to the recommended monitoring plan and laboratory assessment. The integration of dispensing software systems or electronic alerts within community pharmacy settings may also enhance follow-up processes and promote the safe use of MTX.
Footnotes
Ethical considerations
The research was granted ethical approval from the Institutional Review Board (IRB) at Middle East University (MEU) (grant number 825-2025/2026).
Consent to participate
A verbal consent was obtained from research participants prior to taking part in the research.
Consent for publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data can be supplied upon request.