
Abstract
Adolescent males comprise a significant number of youth in out-of-home care, yet our understanding of their past adverse experiences and current functioning remains relatively limited. The current study relied on data from the Assessment and Action Record—second Canadian version for a representative sample of 508 12- to 17-year-olds in out-of-home care across the province of Ontario (Canada). Findings indicated high rates of maltreatment (especially emotional abuse) as the primary reason for child welfare entry, with an elevated occurrence of multiple exposure to different types of maltreatment (71.6% of youth). Once in care, male youth appeared vulnerable to continuing adverse experiences, with 23.8% experiencing maltreatment (emotional abuse and neglect) and non-maltreatment adversity primarily in the form of school changes and suspensions. Results on current functioning suggested some relative strengths (e.g., developmental assets) but also challenges in the areas of substance use, mental health, caregiver relationship, and academic performance. Past emotional abuse and neglect, as well as greater maltreatment exposure, significantly predicted greater substance use, while greater past-year individual adversities (e.g., school changes and suspensions) predicted poorer academic performance. Findings point to the importance of child welfare’s continued monitoring of adolescent males’ safety and well-being across home and school settings, as well as the reliance on trauma-informed practices to address the multiple needs of male youth in out-of-home care. Our findings also highlight the importance of using data in child welfare practice to regularly assess the well-being of youth in out-of-home care for purposes of service planning and delivery.
Prevalence data for the province of Ontario (Canada) indicate that there were 7,730 children and adolescents living in out-of-home care in 2016 (Statistics Canada, 2016). Of Ontario child maltreatment investigations in 2013, about 3% resulted in out-of-home placements, with 2% to foster care, 1% to informal kinship care, and <1% to group homes or residential treatment (Fallon et al., 2015). The present study made use of a sample of 12- to 17-year-old males in out-of-home care in Ontario to better understand adverse childhood experiences and links with current functioning (e.g., socio-emotional, educational). It is critical to understand the level of need among adolescents in out-of-home care so that Ontario child welfare may provide services “in a manner that respects a child’s or young person’s need for continuity of care and for stable relationships within a family and cultural environment” (Child, Youth and Family Services Act, 2017, S.O. 2017, c. Sched.1). This population is relatively understudied (Simmel, 2012), which is concerning given the number of child welfare-involved youth who are male as well as their greater vulnerability to experiencing adversity and impairments in mental well-being and functioning (Euser, Alink, Tharner, van Ijzendoorn, & Bakermans-Kranenburg, 2013; Fernandez, 2008; Indias, Arruabarrena, & De Paúl, 2019). In Ontario, incidence data suggest that rates of substantiated childhood maltreatment are the same for adolescent (12–15 years) males and females (Fallon et al., 2015) yet male youth are overrepresented in out-of-home placements (i.e., foster, kinship, and group home care), with approximate rates of 54.5% for 10- to 16+-year-olds and 46% for same-aged females (Miller, 2017). On a related note, adolescent males appear to remain involved with child welfare for longer periods of time, to experience greater placement instability, and to achieve less permanency in comparison with female youth (Farmer, Mustillo, Burns, & Holden, 2008; Kemp & Bodonyi, 2002; Webster, Barth, & Needell, 2000). It should be noted, however, that some research suggests that sex does not play a significant role in placement instability and permanency outcomes (Becker, Jordan, & Larsen, 2007).
By virtue of their placement in out-of-home care, children and adolescents would have experienced adversity severe enough to warrant removal from their primary caregivers. Among substantiated investigations, Ontario data show that the primary reasons for child welfare contact across males and females (newborn–15 years) were as follows: exposure to intimate partner violence (48%), neglect (24%), emotional abuse (13%), physical abuse (13%), and sexual abuse (2%; Fallon et al., 2015). Similarly, an Ontario sample of 15- to 20-year-olds living in out-of-home care (Goldstein et al., 2011) indicated that moderate to severe neglect was reported by 39.4% (emotional neglect) and 36.6% (physical neglect) of youth, followed by physical abuse (36.6%), emotional abuse (34.3%), and sexual abuse (19.0%). Note, however, that this study did not present data on exposure to family violence, and the findings were not presented separately by adolescent sex. As such, specific information on the types of maltreatment experiences among adolescent males within Ontario child welfare remains unknown.
While it is important to understand maltreatment experiences of youth in out-of-home care, it is also important to note that exposure to multiple victimization is common. Cyr et al. (2012) examined the prevalence of multiple victimization among 139 child welfare-involved 12- to 17-year-olds in the province of Quebec (Canada). Based on telephone interviews, 9 in 10 reported some type of direct (e.g., physical or sexual assault) or indirect (e.g., witness to violence) victimization in the past year alone and, among these victimized youth, 92% reported at least one other type of victimization in a separate event. In general, research has found that the majority of youth involved with the child welfare system have experienced multiple types of maltreatment (Collin-Vézina, Coleman, Milne, Sell, & Daigneault, 2011; Lau et al., 2005). In addition, exposure to greater adversity (which is common among maltreated youth within child welfare) is linked with greater psychological distress and mental health impairments, as well as fewer resilient outcomes (Afifi et al., 2014; Collin-Vézina et al., 2011; Segura, Pereda, Guilera, & Hamby, 2017). For example, in a Spanish sample of 127 12- to 17-year-olds in out-of-home care, greater victimization experiences significantly predicted more mental health difficulties in the form of internalizing and externalizing behaviors (Segura, Pereda, Guilera, & Abad, 2016; Segura et al., 2017). In addition, research suggests that non-maltreatment adverse childhood experiences can be found among maltreated children and adolescents. For example, Dong, Anda, Dube, Giles, and Felitti’s (2003) retrospective study indicated that childhood maltreatment types tended to occur not only alongside one another but also with other types of childhood adversity, such as parental substance use, parental mental illness, and parental criminal activity. To the best of our knowledge, however, such an examination has not been undertaken with a representative Canadian national or provincial sample of child welfare-involved male youth.
There is no doubt that childhood maltreatment can have a devastating impact on the well-being and functioning of adolescents across multiple domains, including mental health (internalizing and externalizing behaviors), relationships, cognitive outcomes, and education (Fernandez, 2008; Gallitto, Lyons, Weegar, Romano, & The MAP Research Team, 2017; Kolko et al., 2010; O’Higgins, Sebba, & Gardner, 2017; Petrenko, Friend, Garridoa, Taussiga, & Culhanea, 2012; Romano, Babchishin, Marquis, & Fréchette, 2015). For example, Romano, Babchishin, Marquis, and Fréchette’s (2015) literature review found that children and youth with maltreatment histories often experienced impairments in both their academic performance and mental health (e.g., anxiety, low mood, aggression, social skills deficits, poor interpersonal relationships), and these impairments appeared to be particularly pronounced among maltreated children and youth in out-of-home care. Moreover, educational difficulties appeared to be greater for males (than females), for adolescents (than younger children), and for neglect (than primarily other types of maltreatment, in particular physical abuse).
With regard to additional outcomes and predictors, the Ontario Incidence Study (Fallon et al., 2015) asked child welfare practitioners to complete a checklist of child difficulties that they became aware of during the course of their investigation. At least one difficulty was identified in 41% of substantiated investigations, with academic problems and mental health (i.e., internalizing behaviors) being the most common (each at 19%), followed by attention-hyperactivity problems (13%), aggression (12%), attachment issues (e.g., relationship with the caregiver; 12%), and intellectual or developmental impairments (10%). In an Australian child welfare study with a small (N = 59) convenience sample of 4- to 15-year-olds, Fernandez (2008) found clinically elevated scores for 35.8% of the sample on internalizing behaviors (e.g., depression, anxiety) and 34% for externalizing behaviors (e.g., aggression), based on caregiver reports. The percentage of children and youth in the clinical range was significantly higher compared to a community-based sample (12.8% for internalizing, 12.9% for externalizing). Sex-based analyses were not conducted for caregiver reports. Teachers also reported on the sample’s functioning, with findings indicating that aggressive behavior was the primary concern for males although no age-based analyses were conducted. Finally, academic difficulties were found among children and adolescents in out-of-home care, compared with those within the community. However, the study’s small sample did not make it possible to conduct age- and sex-based analyses.
Turning more specifically to adolescents in out-of-home care, a study (Guibord, Bell, Romano, & Rouillard, 2011) involving 122 12- to 15-year-olds in the province of Ontario that focused on depressive symptoms and substance use found that 35% endorsed elevated mental health concerns (i.e., depressive symptoms), and 22% indicated having used alcohol and/or substances in the past year. While depressive levels were high across adolescents, females had significantly higher depression scores than males. There were no sex differences for substance use, but findings indicated greater risk with increasing age. Finally, the greater the perceived quality of the youth–caregiver relationship, the lower the risk for both depression and substance use. In another Canadian sample of 53 14- to 17-year-olds in residential (group home) care in the province of Quebec, there were no statistically significant sex differences across four types of maltreatment that were assessed (i.e., emotional abuse, physical abuse, emotional neglect, and physical neglect), but one exception was sexual abuse where reports were higher for female youth than males. Findings also indicated each form of abuse and neglect was significantly associated with clinical levels of mental health difficulties in the form of anxiety, depression, anger, post-traumatic stress, and dissociation (Collin-Vézina et al., 2011). Goldstein et al. (2011) reported similar relationships between abuse/neglect types and mental health outcomes for adolescents in out-of-home care.
In a U.S. sample of 343 15- to 19-year-olds in out-of-home care, findings from a self-report questionnaire indicated that 25% reported borderline or clinical levels of internalizing behavior problems, while 28.3% reported externalizing behavior problems that were in the borderline or clinical range. It should be noted that analyses were not conducted separately by sex (Auslander et al., 2002). Finally, Kolko et al. (2010) conducted a large (N = 1,848) U.S. nationally representative study of one mental health outcome—post-traumatic stress symptoms—among child welfare-involved 8- to 14-year-olds who were either still living with their biological families or in out-of-home care. Findings for young adolescents (12–14 years) indicated 15.7% in out-of-home care were above the clinical cutoff for post-traumatic stress, and this rate was significantly higher than youth who remained in their biological home (6.7%). In terms of predictors, younger age (8–10 years), abuse by a nonbiological caregiver, violence in the home, and child depressive symptoms all predicted greater post-traumatic stress symptoms. Sex was not a significant predictor, although analyses were not conducted separately by age and placement status.
Study objectives
Adolescent males appear to be overrepresented in Ontario out-of-home care and, in general, they seem to have longer child welfare involvement. As such, the objective of the current study was to better understand maltreatment and adversity experiences among this particular population of child welfare-involved youth, as well as their functioning across important domains that span well-being, relationships, education, and resilience. Past research has provided some information on the topic but has been limited in several ways, such as through the reliance on convenience sampling, the presentation of results for male and female youth together (e.g., Auslander et al., 2002; Goldstein et al., 2011), and the lack of differentiation between maltreated adolescents who remain within their biological homes versus those placed in out-of-home care (e.g., Cyr et al., 2012). To address these potential confounds, we decided to focus specifically on a representative sample of adolescent males, all of whom were living in out-of-home placements. We undertook to (1) examine the prevalence of past maltreatment and other adverse experiences and (2) understand the links between these adverse experiences and current functioning. We assessed functioning in academic performance, caregiver relationship, mental health, substance use, and developmental assets. We expected to find high rates of past maltreatment and other adverse experiences among adolescent males, as well as high rates of co-occurring adversity. We also expected these adverse experiences to predict difficulties across functioning domains.
Methods
Participants and procedures
We relied on previously collected data from the Ontario Looking After Children (OnLAC) project from the province of Ontario (Canada). The goal of the OnLAC project, which began in 2000, is to improve developmental outcomes for youth in out-of-home care by way of annual assessments intended to monitor a number of domains (e.g., behavior, academic performance, family/social relationships) and subsequently inform child welfare plans of care (Miller, Vincent, & Flynn, 2017). The primary way in which youth are monitored is through the second Canadian adaptation of the Assessment and Action Record (AAR-C2), which is completed for youth who have been in out-of-home care for at least 1 year. The AAR-C2 is completed by child welfare practitioners as a “conversational interview” alongside consenting youth (if 10 years or older) and foster caregivers (Miller et al., 2017). In 2006, the Ontario Ministry of Children and Youth made it mandatory for all child welfare agencies to use the AAR-C2 on a yearly basis (Flynn, Vincent, & Legault, 2009). The current study used the most recent available OnLAC data from 2017. Access to the data was made available through an agreement with the OnLAC project developer (Dr. Robert Flynn at the University of Ottawa) following approval from our University’s Office of Research Ethics and Integrity (H08-18-01).
The current study focused on adolescent males aged 12–17 years (N = 508). The original data set included 3,126 youth aged 10–19 years. We eliminated youth who did not meet the age criteria (i.e., 12–17 years of age) at the time of AAR-C2 completion, resulting in a remaining sample of 2,368 youth. We then eliminated female youth, leaving a total of 1,017 12- to 17-year-old male youth. From this male sample, we excluded 441 whose primary reasons for entry into child welfare were not related to maltreatment (e.g., requesting community support, parental respite). The remaining 576 adolescent males were identified as having experienced childhood abuse or neglect as a primary reason for child welfare involvement, but we were required to eliminate 68 of these youth because they were missing more than 20% of data on either the maltreatment or other adversity variables. These various steps resulted in our final sample of 508 12- to 17-year-old male youth. It should be noted that imputation is not recommended when participants are missing more than 5% of their overall data (Tabachnick & Fidell, 2007) or more than 20% of responses to a single scale (Mazza, Enders, & Ruehlman, 2015; Peng, Harwell, Liou, & Ehman, 2006).
Measures
Demographics
Child welfare practitioners respond to AAR-C2 items to provide demographic information for the adolescent in their care. In the current study, we used the following data: current age, ethnicity, type of placement, years living with the current caregiver, number of changes in primary caregiver, contact with birth family, age when first placed in out-of-home care, and past-year maltreatment experiences.
Maltreatment and adversity variables
Child welfare practitioners responded to AAR-C2 items on the maltreatment experienced by the adolescent. They were asked to indicate the young person’s primary reasons for entry to child welfare services. There were three maltreatment options, namely physical/sexual abuse by commission, emotional abuse, and neglect. They were summed for a total score that could range from 0 to 3, with higher scores indicating a greater number of maltreatment experiences. Child welfare practitioners also reported on individual-related adversities and adverse family experiences that the adolescent may have experienced over the previous year by selecting from a list that also included various forms of maltreatment. There were 12 individual-related non-maltreatment adversities (e.g., change in caregiver, school suspension), 14 non-maltreatment adversities related to the youth’s birth family (e.g., parental substance abuse, parental serious mental health impairments), and 5 maltreatment types (i.e., exposure to intimate partner violence, neglect, physical abuse, sexual abuse, emotional abuse). Total adverse childhood experiences were calculated by summing the number of endorsed items, with a potential range of 0–12 for individual and 0–14 for birth family adversities. Higher scores indicated greater past-year adversities. Maltreatment could range from 0 to 5, with higher scores indicating greater past-year experiences.
Domains of functioning
Relationship to caregiver
Adolescents completed the 4-item Quality of Relationship with Caregiver Scale that assesses the quality of the relationship with the caregiver as perceived by the youth (Statistics Canada & Human Resources Canada, 1999). Items are answered along a 3-point scale from 0 = very little or not very close to 2 = a great deal or very close. Items (e.g., How well do you feel he/she understands you?) were summed for a total score that could range from 0 to 8, with higher scores indicating higher perceived relationship quality. This scale demonstrated very good internal consistency for our sample (α = .84).
Substance use
We used 2 items developed by the AAR-C2 to assess past-year alcohol and cannabis use. Adolescents responded along a 4-point scale from 0 = daily to 3 = not at all. Items were reverse-scored so that higher scores indicate greater frequency of use. Total scores could range from 0 to 6, and the scale showed good internal consistency for our sample (α = .77).
Mental health
Adolescents completed the Positive Mental Health Scale (Keyes, 2006). This 14-item scale includes items related to various aspects of past-month mental well-being, such as you belonged to a community and confident to think or express your own ideas. Responses are along a 6-point scale from 0 = never to 5 = every day. Total scores could range from 0 to 70, with higher scores indicating greater perceived mental health. This scale showed excellent internal consistency for our sample (α = .92).
Academic performance
Caregivers completed the Academic Performance Scale (Statistics Canada & Human Resources Canada, 1999). This 4-item measure assesses performance in specific school subjects (e.g., math) as well as overall. Responses are on a 3-point scale from 0 = poorly or very poorly to 2 = very well or well. Total scores could range from 0 to 8, with higher scores indicating better academic performance. The scale showed very good internal consistency for our sample (α = .88).
Developmental assets
Internal and external assets were measured using a briefer version of Scales’ (1999) measure. Child welfare practitioners responded to 20 items on external assets that assessed four domains, namely support, empowerment, boundaries and expectations, and constructive use of time. Responses to each item (e.g., Young person feels safe at home, school, and in neighborhood) were on a dichotomous scale. Total scores could range from 0 to 20, with higher scores indicating a greater number of external developmental assets. This measure showed good internal consistency for our sample (α = .77). There were also 20 items on internal assets that measured commitment to learning, positive values, social competencies, and positive identity. Responses to each item (e.g., Young person places high value on helping other people) were dichotomous so higher scores indicated a greater number of internal developmental assets. This scale demonstrated very good internal consistency for our sample (α = .88).
Data analyses
We conducted descriptive analyses to understand the prevalence and types of past maltreatment and non-maltreatment adversities, as well as child welfare involvement. To examine the relationship between adverse experiences and current functioning, we conducted separate linear regressions for each of the six domains (academic performance, relationship to caregiver, mental health, substance use, internal assets, external assets). Predictor variables included the presence of various maltreatment types, total maltreatment score, and the number of adverse individual- and family-level experiences. We considered controls among sociodemographics (e.g., current age, services received in the last year) and placement variables (e.g., age when first placed in out-of-home care, number of caregiver changes, current placement type, length of time living with current caregiver) that have been linked with some of the outcomes examined (Chow, Mettrick, Stephan, & Von Waldner, 2014; Farmer et al., 2010; O’Higgins et al., 2017; Perry & Price, 2017; Rock, Michelson, Thomson, & Day, 2015) and/or that would seem reasonable to include because of their potential impact on youth well-being and functioning (e.g., number of placement changes and youth–caregiver relationship). In the end, we included current age, age at child welfare entry, and number of caregiver changes in analyses because they were significantly correlated with predictor and outcome variables. Analyses were conducted using SPSS version 24.
Missing data analyses showed a rate of 7.9% across all study variables. The MCAR significance test showed that the data were not missing completely at random so adolescent males with more than 20% missing items on either predictor or outcome variables were removed from analyses. We carried out an analysis for outliers and found no univariate or multivariate outliers, according to the Mahalanobis distance (p < .001). Regression assumptions of multivariate multicollinearity, linearity, and homoscedasticity were met, with the exception of adverse family-related experiences which required a square root transformation. We calculated effect sizes for each regression using Cohen’s (1988) f 2 statistic, where f 2 ≥ .02, f 2 ≥ .15, and f 2 ≥ .35 represent small, medium, and large effect sizes, respectively.
Results
Demographic and child welfare involvement characteristics
The average age of adolescent males was 15.0 years (SD = 1.5, range 12–17). The most common ethnic background was European (42.5%), followed by Indigenous (19.1%), Caribbean (9.6%), African (4.3%), and South/South-East Asian (1.2%). The majority of adolescent males were English speaking (93.6%). For child welfare involvement, Table 1 indicates that most youth (52.8%) were living in foster care, followed by group homes (24.5%), kinship care (9.4%), and independent living (5.6%). Note that 7.6% of youth were in other unspecified placement types. On average, adolescent males had been in their current placement for 2.5 years (SD = 3.5) and had experienced 5.2 primary caregiver changes (SD = 3.7) since child welfare entry. Despite their out-of-home placements, the majority of youth (83%) had regular contact with their birth families, be it on a weekly or monthly basis. Turning to child welfare entry, practitioners indicated that the mean age at the time of the first out-of-home placement was 8.0 years (SD = 4.7), and the primary reason was emotional abuse (42.2%), followed by physical/sexual abuse (29.5%) and neglect (28.2%). Because more than one primary reason could be indicated, we calculated the average score and found it to be 1.1 (SD = 0.85, range 0–3). One form of maltreatment was reported for 28.3% of male youth, whereas 41.5% experienced two types and 30.1% experienced all three types.
Child welfare involvement (N = 508).
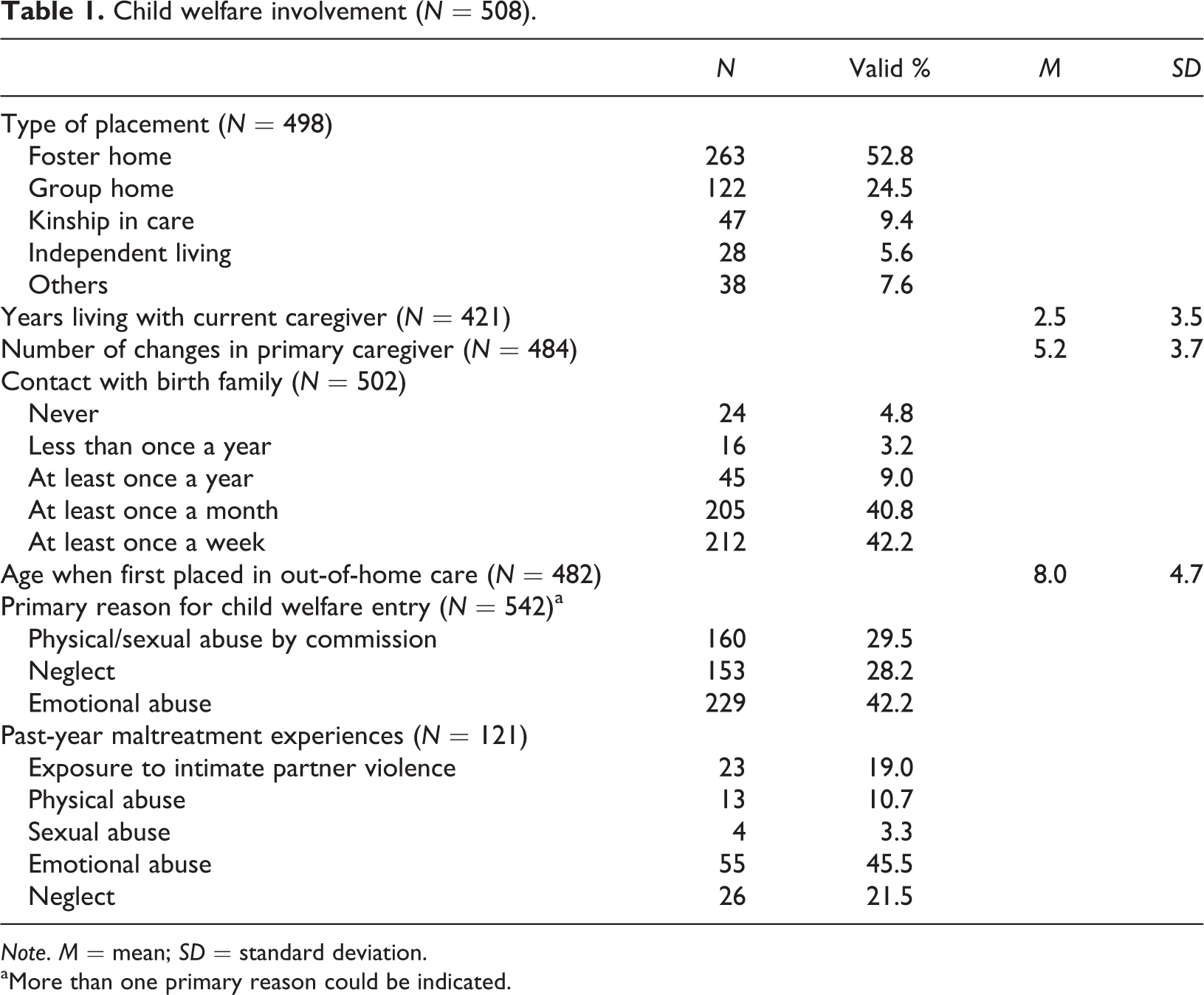
Note. M = mean; SD = standard deviation.
aMore than one primary reason could be indicated.
Practitioners indicated whether male youth experienced any form of maltreatment in the year prior to the AAR-C2 completion. Results showed that 121 male youth (23.8% of the sample) experienced maltreatment despite being in out-of-home care. Of these youth, 45.5% experienced emotional abuse, followed by neglect (21.5%), exposure to intimate partner violence (19.0%), physical abuse (10.7%), and sexual abuse (3.3%). Practitioners provided information on adverse family and individual experiences in the year prior to the AAR-C2 completion. The mean number of adverse family experiences was 1.7 (SD = 1.0), with the most frequently reported being parental substance use (23.6%), followed by parental serious mental health impairments (8.9%) and death of a relative or friend (7.1%). For individual adversities, the mean number was 2.0 (SD = 1.8), and the most frequently reported was changing schools (40%), followed by school suspensions (37.4%), change in caregiver due to youth behavioral problems (35.4%), and school truancy (30.9%).
Current functioning
Table 2 indicates that adolescents’ perceived relationship quality with their primary caregiver was similar to the mean from the 2016 AAR-C2 data for 10- to 17-year-old males (M = 6.6; SD = 1.6) and between the 25th and 50th percentile (Miller et al., 2017). The mean score for alcohol and cannabis use was close to the 75th percentile using AAR-C2 data for 10- to 18+-year-old males (Miller et al., 2017). For overall mental health, the mean score for our sample was lower than that of the AAR-C2 data for 10- to 17-year-old males (M = 55; SD = 12.4) and slightly above the 25th percentile (Miller et al., 2017). Based on caregiver reports, the mean score for academic performance was similar to that from the 2016 AAR-C2 data for 10- to 17-year-old males (M = 3.6; SD = 2.3) and between the 25th and 50th percentile (Miller et al., 2017). For external developmental assets, the mean score based on practitioner reports was slightly higher than that from the AAR-C2 data for 10- to 17-year-old males (M = 13.4; SD = 3.8) and at the 50th percentile (Miller et al., 2017). For internal assets, the mean score was slightly higher than that from the AAR-C2 data for 10- to 17-year-old males (M = 12.4; SD = 5.5) and slightly above the 50th percentile (Miller et al., 2017).
Descriptive information for domains of functioning.
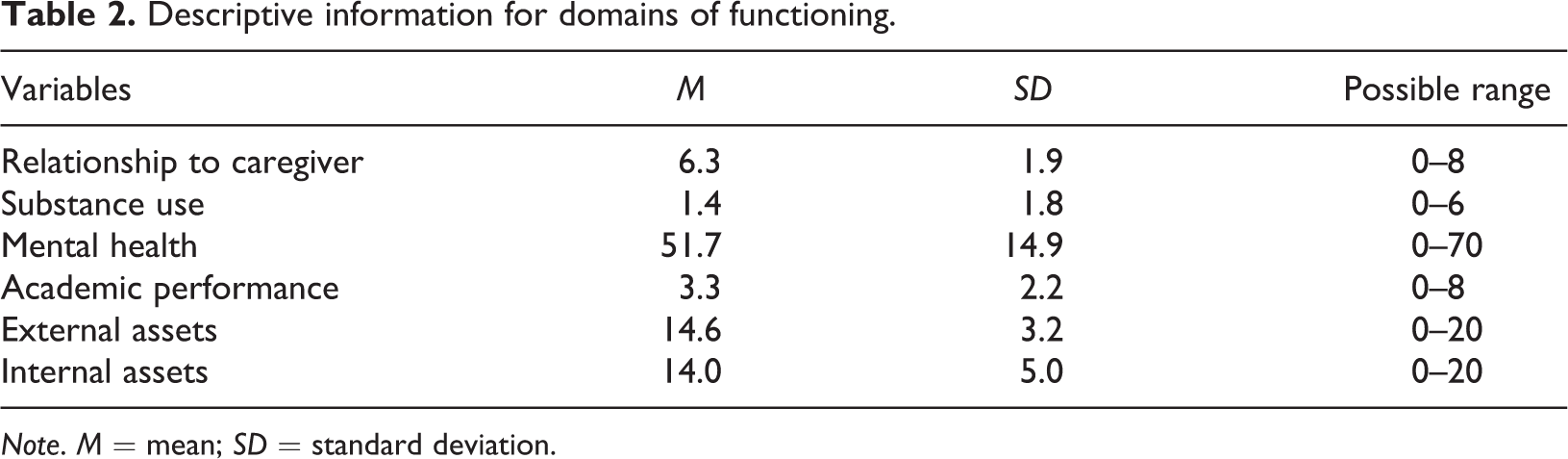
Note. M = mean; SD = standard deviation.
The link between past adversity and current functioning
Prior to the regression analyses, we conducted simple bivariate correlations among all predictor and outcome variables. For the correlations among proposed predictor (adversity) variables and outcomes, Table 3 shows that neglect and emotional harm as the primary reason for entry into the child welfare system were significantly associated with greater substance use (r = .19 and r = .14, respectively), and neglect was also associated with greater practitioner-reported external assets (r = .12). The greater the number of maltreatment types experienced by adolescent males as a reason for child welfare involvement, the greater the use of substances (r = .25) and the better the relationship with the primary caregiver (r = .10). Surprisingly, a greater number of past-year adverse family experiences was significantly correlated with better adolescent-reported mental health (r = .12), as well as a better caregiver relationship (r = .11). Finally, a greater number of past-year individual adversities was negatively associated with five of the six outcome variables. Past-year individual adversity was positively associated with greater substance use (r = .53), suggesting that the greater the number of individual adversities, the greater the substance use among adolescents in our sample.
Correlations among study variables.
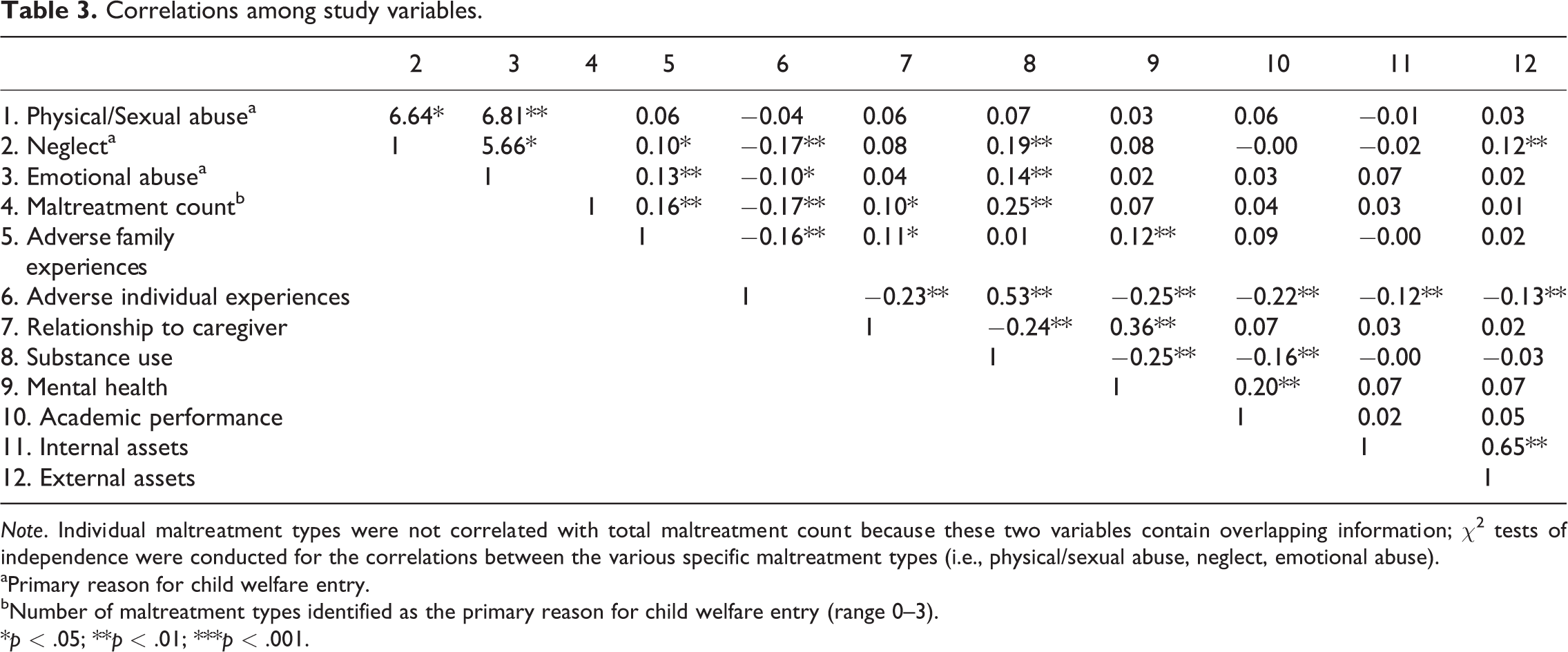
Note. Individual maltreatment types were not correlated with total maltreatment count because these two variables contain overlapping information; χ2 tests of independence were conducted for the correlations between the various specific maltreatment types (i.e., physical/sexual abuse, neglect, emotional abuse).
aPrimary reason for child welfare entry.
bNumber of maltreatment types identified as the primary reason for child welfare entry (range 0–3).
*p < .05; **p < .01; ***p < .001.
Turning to correlations among the proposed adversity predictors, Table 3 indicates that the relationship between physical/sexual abuse and neglect was significant, χ2 (1, N = 508) = 6.64, p < .05, as was the relationship between physical/sexual abuse and emotional abuse χ2 (1, N = 508) = 6.81, p < .01. Neglect and emotional abuse also were significantly related, χ2 (1, N = 508) = 5.66, p < .05, and they were both significantly associated with greater adverse family experiences (r = .10 and r = .13, respectively) but fewer individual adversities (r = −.17 and r = −.10, respectively).
There were a number of significant correlations among the outcome variables. Specifically, male youth who reported better mental health reported lower substance use (r = −.25), better academic performance (r = .20), and a better caregiver relationship (r = .36). Practitioners who indicated a greater number of internal assets in adolescent males also indicated greater external assets (r = .65). Finally, greater substance use was associated with poorer academic performance (r = −.16) and a poorer caregiver relationship (r = −.24).
Table 4 presents the regression analyses for potential maltreatment and adversity predictors on adolescent males’ current functioning. Of the various maltreatment types that were the primary reason for child welfare entry, emotional abuse significantly predicted greater substance use (B = .36, p < .05) and better academic performance (B = .47, p < .05). Emotional abuse accounted for 17.2% of the variance in substance use and 4% of the variance in academic performance, both of which represented small effects (f 2 = 0.03 and f 2 = 0.02, respectively). Neglect significantly predicted greater substance use (B = .74, p < .001) and accounted for 20.6% of the variance, which is a small effect (f 2 = 0.04). Neglect also significantly predicted greater external assets (B = 1.35, p < .05) and accounted for 4.3% of the variance, which is a small effect (f 2 = 0.02). In terms of maltreatment count, a greater number of maltreatment types experienced at the time of child welfare entry significantly predicted greater substance use (B = .39, p < .001). This variable accounted for 20.6% of the variance in substance use and reflected a small effect (f 2 = 0.04).
Maltreatment and adversity predictors of current functioning.
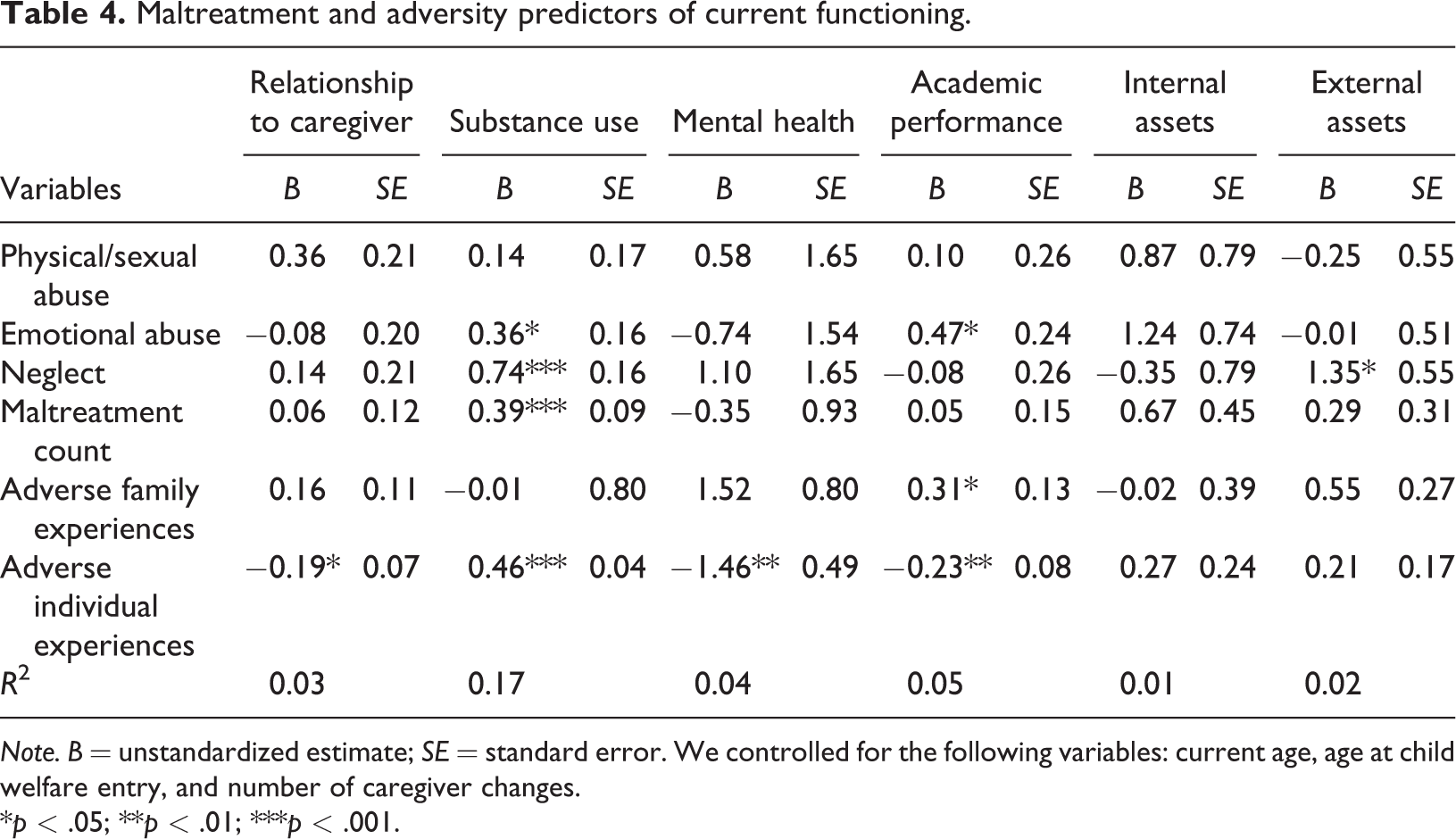
Note. B = unstandardized estimate; SE = standard error. We controlled for the following variables: current age, age at child welfare entry, and number of caregiver changes.
*p < .05; **p < .01; ***p < .001.
Findings indicated that a greater number of past-year individual adversities predicted greater substance use (B = .46, p < .001) and accounted for 36.3% of the variance (medium effect of f 2 = 0.15). Greater adverse family and individual experiences predicted better (B = .31, p < .05) and poorer (B = −.23, p < .01) academic performance, respectively. Adverse family experiences accounted for 8% of the variance in academic performance, which is a small effect (f 2 = 0.02), and individual-related adversities accounted for 6% of the variance, which is a small effect (f 2 = 0.02). Last, greater individual adversities significantly predicted poorer mental health (B = −1.46, p < .01), accounting for 8.1% of the variance and resulting in a small effect (f 2 = 0.02).
Discussion
The goal of the current study was to broaden our understanding of male youth (12–17 years) in out-of-home care, specifically their adversity experiences, current functioning, and links between adversity and functioning. One strength of the study was its reliance on a large sample that was representative of adolescent males in out-of-home care in the province of Ontario (Canada). An additional strength was the inclusion of multiple informants, namely the youth themselves along with their primary caregiver and child welfare practitioner.
At a descriptive level, practitioners indicated that the primary reason for adolescent males’ entry into the child welfare system was emotional abuse (4 in 10 youth), followed closely by physical/sexual abuse (3 in 10) and neglect (3 in 10). Unfortunately, no data were collected on exposure to intimate partner violence, even though Ontario incidence data suggest that this is the most common reason for substantiated child welfare investigations (Fallon et al., 2015). Moreover, it would seem important to inquire specifically about sexual abuse given that this form of maltreatment is often overlooked in males and/or not disclosed because of societal messages around masculinity and vulnerability (Romano, Moorman, Ressel, & Lyons, 2019).
Our results were similar to past research in highlighting the presence of child physical abuse among males (Afifi et al., 2014; Dong, Anda, Dube, Giles, & Felitti, 2003), although it should be noted that the AAR-C2 instrument in our study grouped physical and sexual abuse together so rates for physical abuse alone may have been slightly inflated. Emotional abuse among adolescent males in our sample was higher in comparison with past studies (Dong et al., 2003; Finkelhor, Turner, Shattuck, & Hamby, 2013) but similar to a study which made use of the same database, albeit a number of years prior to our study and with male and female youth grouped together (Goldstein et al., 2011). With regard to the differences, they are likely a function of informant differences (self- vs. practitioner-reported) and the nature of the research question, namely, whether an individual experienced various childhood maltreatment types compared to the primary reason for coming into contact with the child welfare system. Moreover, it can be argued that emotional abuse underlies all other forms of maltreatment in that messages about a child’s worth and right to love and protection are conveyed (verbally and nonverbally) through abusive acts of commission and/or omission (Vachon, Krueger, Rogosch, & Cicchetti, 2015). For child neglect, findings indicate that it was a concern for our sample of adolescent males, which mirrors most past research (Fallon et al., 2015; Goldstein et al., 2011), although Finkelhor, Turner, Shattuck, and Hamby’s (2013) prevalence rate was about half (15.2%). This latter finding (Finkelhor et al., 2013) may be partly attributable to the study’s reliance on a community-based sample of youth where maltreatment experiences are less extensive than for youth who come to the attention of child welfare (Fernandez, 2008; Kolko et al., 2010).
Although there were similarities and differences in rates of maltreatment exposure between our sample and past research findings, it would seem reasonable and unsurprising to conclude that adolescent males in out-of-home care have histories of severe abuse and neglect. Moreover, most male youth experienced multiple forms of maltreatment, as child welfare practitioners indicated that the majority (71.6%) had been exposed to more than one of the three maltreatment types assessed. These findings are consistent with past research that underscores the reality of multiple victimization, especially among child welfare-involved youth (Collin-Vézina et al., 2011; Cyr et al., 2012; Lau et al., 2005). While these particular results are in relation to primary reasons for child welfare entry, we also found that adolescent males continued to experience adversity even once placed in out-of-home care albeit one can argue to a lesser extent. Specifically, one in four (23.8%) had a past-year experience of maltreatment, with the most frequent being emotional abuse (45.5%) followed by neglect (21.5%). Also, adolescent males had experienced an average of two individual adversities over a 1-year period, most commonly in the form of change in school (40%) and school suspension (37.4%). These findings highlight the continued vulnerability of male youth even once removed from the more immediate safety concerns of abusive and neglectful biological homes.
In terms of current functioning among our sample of male youth in out-of-home care, findings partially supported our expectations that there would be impairments across various domains. Based on percentile rankings, there was significant substance use compared with same-age, same-gender peers, as well as difficulties with mental health, caregiver relationship quality, and academic performance. Compromised academic outcomes have often been noted among youth with maltreatment histories, especially those in out-of-home care (Fallon et al., 2015; O’Higgins et al., 2017; Romano et al., 2015), as has substance use (Guibord et al., 2011) which may be considered a form of coping among these male youth. Impairments in mental well-being have also been highlighted in past research on youth with maltreatment histories, whether in their birth homes or in out-of-home placement (Fallon et al., 2015; Fernandez, 2008; Guibord et al., 2011; Kolko et al., 2010). Finally, there were some concerns among adolescents in our sample about the relationship with their primary caregiver, which is somewhat surprising given that the average length of placement was 2.5 years and given research suggesting the benefits associated with stable out-of-home placements (Newton, Litownik, & Landsverk, 2000; Rubin, O’Reilly, Luan, & Localio, 2007). This finding speaks to the importance of supporting caregivers in their work to provide trauma-informed parenting to address the multiple, complex needs of youth in out-of-home care.
Turning to the links between adolescent males’ past adversity and current functioning, results partially supported our expectation that adverse experiences would predict greater impairments in functioning. The presence of emotional abuse or neglect was associated with greater substance use among male youth, as was the greater number of maltreatment types experienced at the time of child welfare entry. While the effect sizes were small, these variables are nonetheless important given their continued impact on functioning despite their occurrence a number of years previously in the youth’s history. Similarly, greater past-year individual adversities predicted greater substance use, suggesting that adolescents might be turning to substances to cope with past maltreatment and/or individual-related stressful life events (e.g., academic difficulties; Henry & Thornberry, 2010).
A similar pattern of findings was noted for academic performance, with expected (greater individual adversities predicted poorer academic performance) and unexpected associations (emotional abuse and greater adverse family experiences predicted better academic performance) that were all small in terms of effect sizes. Although substance use and academic performance were the adolescent outcomes with the most statistically significant associations with past maltreatment and non-maltreatment adversities, we also noted several additional associations that again were expected in some cases (greater individual adversities predicted poorer mental health) and unexpected in others (neglect predicted greater external assets). The link between greater past-year family adversity and better academic performance seems counter-intuitive and was unexpected, given that these variables were not significantly correlated in our bivariate analyses. It should be noted, however, that the mean number of past-year adverse family experiences was low (M = 1.7) and may not have directly impacted adolescents’ functioning, given that they were not living with their biological caregivers, for which these data were gathered (i.e., parental substance abuse and mental health difficulties).
Limitations and directions for future research
Several study limitations are important to consider. First, we were limited in the variables we could examine because of our reliance on data that were already collected through a child welfare instrument in Ontario (i.e., AAR-C2). For example, in indicating the primary reason for child welfare entry, practitioners were limited to three maltreatment types that lumped together physical and sexual abuse and that excluded exposure to intimate partner violence. In addition, because of the comprehensive nature of the AAR-C2, it is not possible to collect in-depth information on all variables of interest (e.g., characteristics of maltreatment experiences in terms of onset age, duration, and perpetrator relationship). Moreover, the AAR-C2 may be vulnerable to social desirability responding biases and to inaccuracies when information about a youth is only collected from another individual (e.g., child welfare practitioner reports of the youth’s internal developmental assets). Future research may wish to consider supplementing the information gathered through large, representative databases with other assessment methods (e.g., child welfare files, youth standardized self-report questionnaires, semi-structured interviews) to gain a more comprehensive understanding of the maltreatment and adversity experienced by male youth in out-of-home care. Second, our focus was on the impact of past maltreatment and adverse experiences on current functioning because research on adolescent males in out-of-home care is still relatively new. As such, we did not explore more complex and comprehensive theoretical models that included potential mediating and moderating variables. Future research may wish to replicate and expand on findings from the current study to further our understanding of functioning among child welfare-involved male youth, as well as factors that promote better functioning and well-being. Third, there were a number of participants who were eliminated from analyses because of missing data on our primary variables of interest (i.e., maltreatment and adversity history). Finally, we did not conduct comparative analyses between child welfare-involved male youth with maltreatment histories and those who entered child welfare for reasons other than maltreatment. Future research may wish to incorporate this comparison group to further understand the possible unique impact of various forms of maltreatment on the functioning of child welfare-involved male youth.
Applied implications
Our findings highlight the continued vulnerability of male youth even once removed from abusive and neglectful biological homes and placed in out-of-home care and as such, the on-going responsibility of child welfare to actively ensure and advocate for adolescents’ safety and well-being in out-of-home placements. With regard to specific implications, we first suggest that it is imperative that child welfare practitioners regularly monitor all aspects of adolescent males’ functioning, well-being, and safety, with particular attention to substance use, academic achievement, mental health, and the caregiver relationship as well as the minimization of additional adversities (e.g., school changes, suspensions, maltreatment within out-of-home care). At the same time, it is important to build on those areas of functioning that represent strengths and competencies for adolescent males, be it within school, home, and/or the community. Second, male youth in out-of-home care undoubtedly continue to face challenges as a result of early, adverse experiences (especially in cases of multiple exposure). As such, child welfare practitioners need to interact with male youth in a trauma-informed manner and encourage those in regular contact with youth to do the same (e.g., educators, caregivers). Trauma-informed means adopting strategies that seek to understand and address the meaning of challenging emotions and behaviors through the lens of their past maltreatment and adverse experiences, rather than through the use of strategies aimed at behavioral control. In a similar vein, it would seem important to secure trauma-informed mental health services for adolescent males in out-of-home care to enhance their sense of well-being and functioning by way of addressing trauma impacts as they relate to adolescents’ experiences both within their biological families and within the child welfare system. Third, child welfare practitioners need to make regular use of research data (e.g., AAR-C2), alongside other sources of information (e.g., interactions with youth and caregivers), to inform their service planning for youth in their care as part of the growing emphasis on evidence-based practice within child welfare.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.