
Abstract
This study aimed to investigate the demographic, clinical, and placement factors associated with psychotropic medication prescribed to youth in foster care presenting with a request for a psychotropic medication. Additionally, this study explored placement instability after the initial prescription of psychotropic medication since entering foster care. Insight into specific factors that may influence the number of placement changes of youth in care prescribed psychotropic medication within a medication oversight program can help provide proactive support and timely mental health interventions. Psychotropic medication data were obtained for youth in the oversight program ages 0 to 18 who entered foster care from 2015 to 2021 (N = 480) and merged with placement data from an integrated administrative database. Regression analyses examined demographics, clinical factors, and placement instability predicting antipsychotic or polypharmacy prescription following an initial psychotropic medication review. The number of placements and hospitalizations in the following two years was analyzed by medication types. After controlling for covariates, entering care on no medication predicted the prescription of an antipsychotic, and polypharmacy of youth in care prescribed at least one psychotropic medication. Additionally, among youth with a psychotropic referral, being initially prescribed an antidepressant or an antipsychotic and a disruptive behavior diagnosis predicted the number of subsequent placements and hospitalizations. These factors can help identify youth at high risk for placement instability and psychiatric hospitalization at the point of referral for psychotropic medication, allowing for targeted intensive mental health treatment and casework.
Introduction
Youth in foster care are a highly vulnerable population with increased rates of mental health and behavioral concerns. It is estimated that 40-60% of youth in child welfare have a mental health diagnosis (Lehmann et al., 2013; Scozzaro & Janikowski, 2015). This level of mental health need is likely to be related to the high levels of trauma experienced by youth who enter foster care. One study found that about 80% of older youth in foster care had experienced a traumatic event (Salazar et al., 2012), and another indicated that youth who had experienced trauma had more behavioral and mental health challenges (Kisiel et al., 2009). The high prevalence of behavioral issues is concerning as it increases the probability of foster care-specific vulnerabilities, including placement instability (Aarons et al., 2010) (defined as having more than two placements in a single episode) (Child Welfare Outcomes 2016: Report to Congress, 2024) and higher rates of psychotropic medication prescription (Fontanella et al., 2014; Palmer et al., 2023; Patten et al., 2012). Prior research suggests that trauma symptoms are also associated with placement instability (Clark et al., 2020) and that frequent placement changes predict increased prescription of psychotropic medications (Tan et al., 2022). While many systems, including caregivers, clinicians, and larger institutional factors, can influence youth development and mental health (Bronfenbrenner, 1979), youth in foster care may be especially susceptible to adverse outcomes due to the complexity of their needs and the compounding of risks in foster care.
Understanding the susceptibility for multiple moves among youth in care prescribed psychotropic medications is critical because placement disruptions pose unique risks for youth with mental health needs. Continuity of care is threatened when a youth is moved to a new home, as placement changes can lead to gaps in medical history and care (Fontanella et al., 2015; Mekonnen et al., 2009). Additionally, not having an established provider increases the risk of unnecessary polypharmacy (the use of more than one medication from either the same or different medication classes (Kukreja et al., 2013) and inappropriate treatment termination (Fontanella et al., 2015; Mekonnen et al., 2009).
Nationally, psychotropic medication review programs have been established in most states to provide oversight of psychotropic prescriptions for youth in foster care. These programs help ensure that psychotropics are not over-prescribed and align with a child’s clinical needs (Fernandes-Alcantara et al., 2017). Review programs have the potential to address concerns regarding unnecessary prescribing of multiple medications or medications with adverse side effects, like antipsychotics (Correll, 2008). Antipsychotics are approved for schizophrenia, bipolar mania, and irritability in autism (Christian et al., 2012) and are often used off-label for disruptive behavior (Penfold et al., 2013). Additionally, review programs may help identify youth with clinical characteristics associated with a high risk for multiple placement moves and hospitalizations. Despite this potential, most research has focused on the description of psychotropic use and demographic variation. For example, among youth who came into care on psychotropic medication, one study found that 56% took multiple medications (Palmer et al., 2023); other studies have indicated that 23% of youth in foster care take antipsychotic medications (Tan et al., 2022) and 12% take multiple medications (Fernandes-Alcantara et al., 2017). Existing research also suggests that white youth in foster care are prescribed psychotropic medication more often than racial minority youth (Medhekar et al., 2019; Zito et al., 2008), and males are prescribed multiple medications more often than females (Medhekar et al., 2019; Zito et al., 2008). As expected, youth in residential settings and those with psychiatric hospitalizations have the highest rates of psychotropic medication use (Saldaña et al., 2014; Stambaugh et al., 2012). Additional research is needed to understand both the predictors of psychotropic medication use in the context of a medication review program and the characteristics of youth who continue to be at risk for placement moves and hospitalizations after initiation of a psychotropic medication.
In this study, we sought to explore factors associated with placement instability and the prescription of psychotropic medications for youth in foster care in the context of a statewide psychotropic medication review program. Using retrospective longitudinal methods, we investigated the relationship between demographic factors, prescriber type, diagnosis, placement type, and initial psychotropic medication prescriptions for youth first entering foster care and prescribed at least one psychotropic medication in a midwestern state between 2015 and 2021. Placement instability and hospitalizations were also investigated up to two years later. Specifically, we undertook this study to determine the distribution of diagnosis, age, sex, and race by medication type; the demographic, clinical, and prior placement variables that predict the initial prescription of psychotropic or polypharmacy; and predictors of placement moves and number of hospitalizations for youth in the two years after their initial psychotropic medication prescription. This study’s focus complements previous research that provides insights about the needs of youth who are prescribed psychotropic medications, but does not address the relative contribution of a broader range of factors in the prescribing of antipsychotic and multiple medications. Understanding factors and predicting patterns in the context of a medication review program and whether specific medications or clinical factors predict placement instability can inform the youth’s needs assessment, continuity of care, and care coordination strategies (Huefner et al., 2017; Medhekar et al., 2019; Scozzaro & Janikowski, 2015; Tan et al., 2022).
Methods
Study Design and Data Sources
A retrospective research design was used to investigate the relationship between placement instability and psychotropic medication prescription for youth in the Illinois Department of Children and Family Services (DCFS) foster care. Data were extracted from the University of Illinois at Chicago’s Clinical Services in Psychopharmacology (CSP) database and an integrated database, compiled from Illinois DCFS administrative data and maintained by Chapin Hall, an affiliated research center of the University of Chicago.
The Clinical Services in Psychopharmacology was established in response to a state law mandating that DCFS provide consent for any psychotropic medication prescribed to youth in care. The law further specifies that an independent medication review is conducted for all psychotropic medication consent requests to ensure the safety and appropriateness of the proposed treatment. While parental rights are not typically terminated when youth enter care in Illinois, the state grants DCFS guardianship over youth in care, including the power to grant medical consent. Prescribers wishing to prescribe a psychotropic medication complete and submit a medication consent form, CFS Form 431a. This form includes patient name, the DCFS ID, date of birth, sex, height, weight, race and ethnicity, placement name and type, prescribing clinician and specialty, psychiatric and medical diagnoses, all current medications and dosages, discontinued medications, type of request (new, renew, or increase), requested medication, dose and frequency of administration, and target symptoms supporting the use of the medication. Since July 2008, all data has been maintained in an SQL database. The consent form is reviewed by the Clinical Services in Psychopharmacology team, where research specialists and registered nurses ensure it includes all necessary and accurate information, including a check that symptoms and diagnosis are consistent. The form is then forwarded to a child and adolescent psychiatrist, who makes recommendations to DCFS based on the diagnosis, symptoms, and other relevant clinical information. The integrated database is a longitudinal administrative data set that includes data on demographic characteristics, placement type and frequency, and hospitalization frequency for children who have received services from DCFS. Chapin Hall processes and distributes the data to other university partners working with DCFS. Both datasets contained a unique DCFS ID for each child, which was used to link the data. The Institutional Review Board of the University of Illinois at Chicago and DCFS received and approved all study procedures.
Sample
The study sample included youth who first entered DCFS custody between 2015 and 2021 and were prescribed at least one psychotropic medication after entering care. All study participants were between 0 and 18 years old. Participants’ data were tracked until they left DCFS care, turned 18, or until the end of the study period (two years after a youth’s first medication request). Any medication requested only once and never renewed, or marked as discontinued, was removed. Since this data only shows a prescription request, not use, it was not possible to determine whether the medication was taken without follow-up data. Youths who left and reentered DCFS care during the study period were still included to ensure sample inclusivity.
Measures
Placement instability was measured before a youth’s first medication request and up to two years after (or until they left DCFS care, whichever came first). Placement instability was measured by the type and total number of placements a youth resided in. Type of placement as defined by DCFS include residential care, subsidized guardianship, group home, specialized foster home, regular foster home, and home of a relative. Total number of placements excluded unplanned events (e.g., runaway episodes, inpatient hospitalizations, and detention) as well as permanency outcomes (e.g., adoption, subsidized guardianship, and reunification). Any placement disrupted by an unplanned event was treated as continuous, as these events are temporary absences from a youth’s ongoing foster care placement, not a move (Social Security Act (479). n.d.). Notably, an inpatient stay included any hospitalization (psychiatric or medical); an estimated 20% were likely medical inpatient stays, but could not be identified because prior coding did not specify the type of hospitalization.
Psychotropic medication use was measured by the type of medications and the number of unique and concurrent medications prescribed. Psychotropic medications were categorized into six groups: attention deficit hyperactivity disorder (ADHD) medications (stimulants, alpha agonists, and atomoxetine), antidepressants (selective serotonin reuptake inhibitor, selective serotonin-norepinephrine inhibitors, tricyclics, monoamine oxidase inhibitors, bupropion), anxiolytics/anti-anxiety (benzodiazepines, hydroxyzine, buspirone), antipsychotics (first generation and atypical), mood stabilizers (lithium carbonate and anticonvulsant mood stabilizers), and other e.g., desmopressin, benztropine) (Fontanella et al., 2014; Zito et al., 2008). Any requested medication counted towards the total number of medications and rates of polypharmacy; however, only ADHD, antidepressant, and antipsychotic medications were analyzed individually. Diphenhydramine and melatonin were not included in the analysis because they may be taken over the counter without DCFS’s knowledge. Polypharmacy was defined as the use of more than one medication from either the same or different medication classes (Kukreja et al., 2013), estimated by the receipt of the prescriptions at two or more time points for at least 60 days (Schubart et al., 2014) to avoid miscategorizing a medication due to cross-titration or tapering (Chen et al., 2011; Medhekar et al., 2019).
Diagnoses, as assigned clinically by the requesting clinician, were categorized into eighteen non-mutually exclusive categories and diagnostic categories derived from the Diagnostic Statistical Manual (DSM-5); like medication classes, these categories were used to count total diagnoses. In the analyses, five broader categories of diagnoses were used, including: disruptive behavior disorders (disruptive mood dysregulation disorder, conduct disorder, oppositional defiant disorder); anxiety, depression, eating disorders, and post-traumatic stress disorder (identified with the acronym ADP); bipolar disorder; neurodevelopmental (developmental disorder and intellectual disabilities, autism spectrum disorder), and ADHD. ADHD and bipolar disorder diagnoses were considered their own categories to remain consistent with the symptoms and corresponding medications typically prescribed (Edelsohn et al., 2021; dosReis et al., 2014). Prescriber specialty was recorded using the National Provider Identifier in the Clinical Services in Psychopharmacology database and included child psychiatrists, general psychiatrists, and other (dosReis et al., 2014) prescribers (including advanced practice nurses). Child demographics included age, race, and sex. Race included White, Black, Latinx, and Other. Sex included male and female. The age of youth in care was calculated at the time their first medication was requested after entering care.
Statistical Analyses
Descriptive statistics were used to describe the placement or unplanned event a youth resided in when prescribed their first psychotropic medication since entering DCFS care, and demographic variables by medication type. Descriptive statistics were used to obtain means, standard deviations, and correlations for all study variables. A multiple logistic regression analysis examined whether clinical factors (diagnosis, other medication, prescriber type), placement factors (years in care, number of prior placements, number of hospitalizations), or demographic characteristics (age, race, sex) predict the prescription of antipsychotics or polypharmacy among youth prescribed at least one psychotropic medication since entering DCFS care. Two linear regressions analyzed clinical and demographic variables in relation to the number of placements in the following two years post-initial psychotropic prescription. The first one included the type of medication and the total number of diagnoses. To clarify associations between medication types and subsequent moves in the first analysis, a second regression analysis included individual diagnostic categories. Medications and diagnostic categories could not be analyzed together due to the multicollinearity between the two sets of variables. To examine predictors of subsequent hospitalizations, a multiple logistic regression analysis investigated the association between medication, placement, and demographic factors and the number of hospitalizations in the two-year follow-up post initial psychotropic prescription. A post hoc power analysis conducted using G*Power 3.1 (Faul et al., 2009) indicated that the total sample (N = 480) provided adequate power for the planned models. Using a two-tailed α = .05, event rates between 0.28 and 0.33, and 13–15 predictors per model, the sample achieved ≥.80 power to detect medium effects (OR ≈ 1.60-1.65), and power exceeded .95 for larger effects (OR ≥2.00). These results support the adequacy of the sample for identifying medium-to-large associations, although small effects (OR <1.30) would be underpowered. Missing data were minimal (<5%) across all analytic variables. Little’s MCAR test indicated no systematic pattern of missingness, and missingness was not associated with primary predictors or outcomes. Accordingly, analyses were conducted using complete-case procedures. Sensitivity analyses that included missingness indicators yielded comparable results, and multiple imputation was not considered necessary. The results were reported as standardized beta (β) with 95% confidence intervals (CI). All analyses were run in SPSS Statistics. P values <.05 were considered significant. All statistics were two-sided.
Results
Descriptive Data of the Distribution of Sex, Race, and Diagnosis by Medication Type and Overall
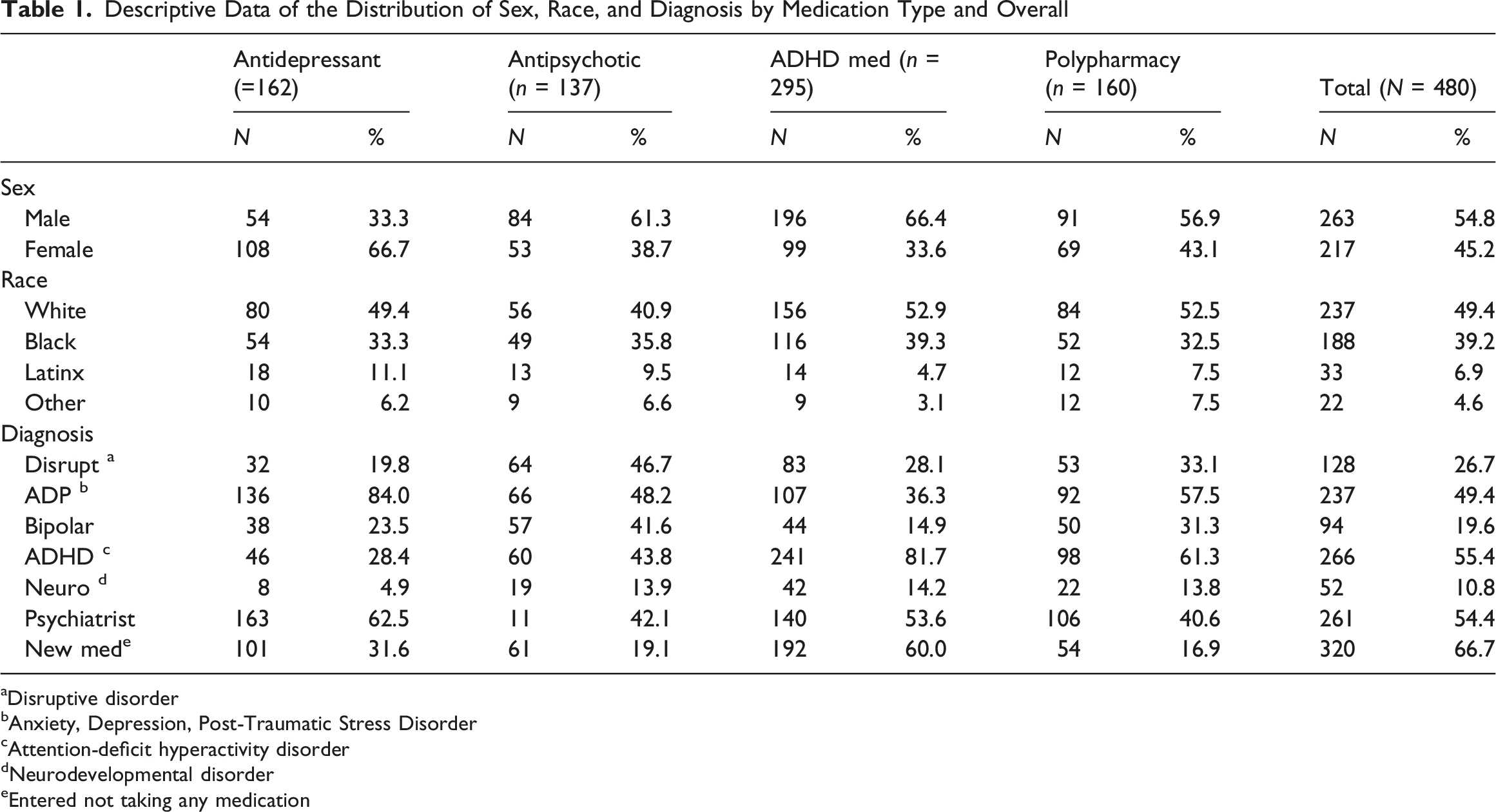
aDisruptive disorder
bAnxiety, Depression, Post-Traumatic Stress Disorder
cAttention-deficit hyperactivity disorder
dNeurodevelopmental disorder
eEntered not taking any medication
Descriptive Data of the Distribution of Age, Medication Prescribed, Prior Placements, and Years in Care by Medication Type and Overall

As compared to the entire population in foster care in Illinois during this period (Children's Bureau, Child Welfare Outcomes Report Data) children in this sample were older and slightly more likely to be male, although racial distribution was similar (51% male in overall Illinois foster care population) (U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau, 2022).
Predictors of Antipsychotic Prescriptions
Multiple Logistic Regression Analysis of Initial Medication Prescriptions: Antipsychotics and Polypharmacy
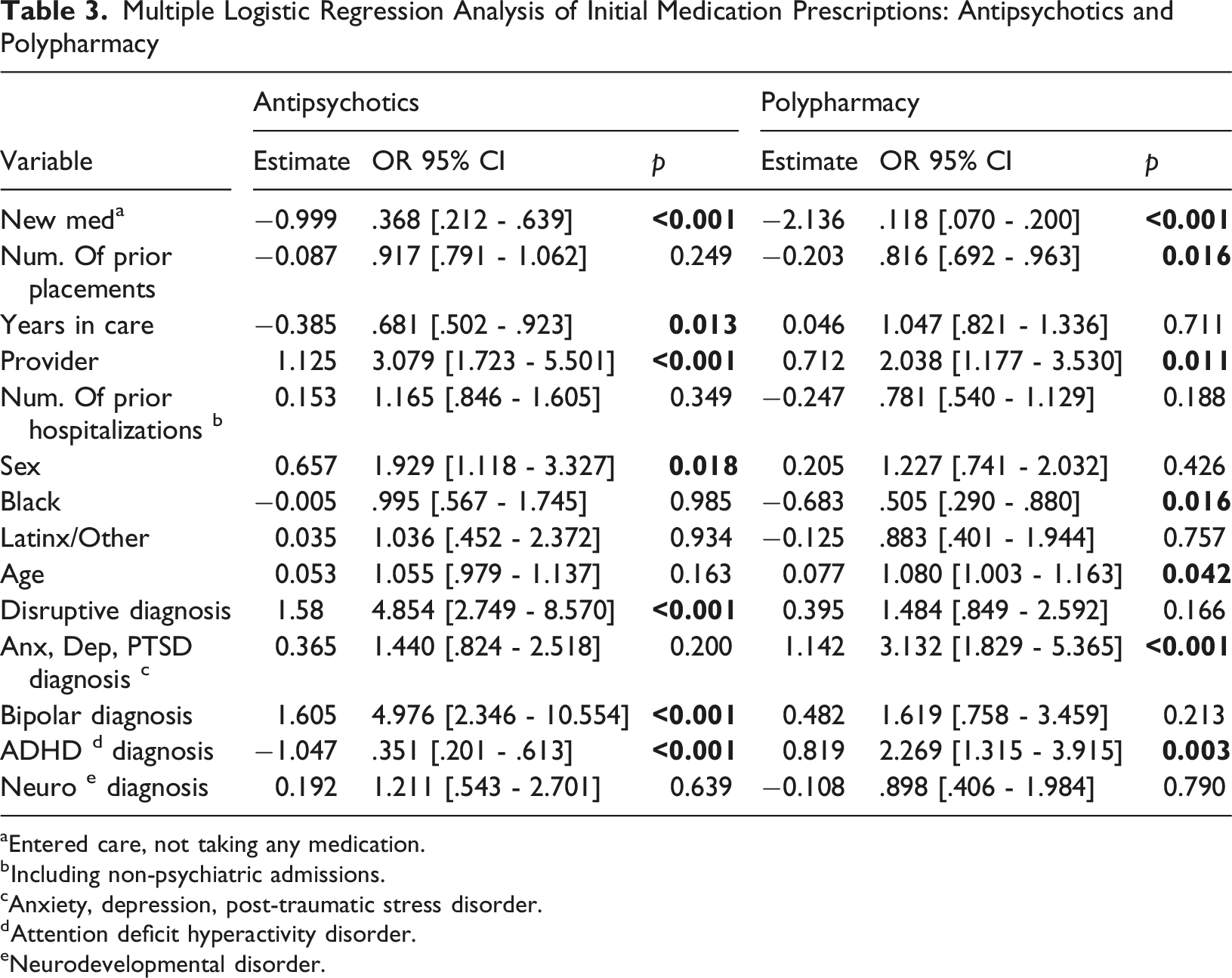
aEntered care, not taking any medication.
bIncluding non-psychiatric admissions.
cAnxiety, depression, post-traumatic stress disorder.
dAttention deficit hyperactivity disorder.
eNeurodevelopmental disorder.
Predictors of Polypharmacy
The logistic regression model predicting initial polypharmacy prescription was significant χ2 (14) = 178.358, p < .001. Clinically meaningful predictors included having an ADP diagnosis (OR = 3.132, p < .001) or ADHD diagnosis (OR = 2.269, p = .003), both increasing the likelihood of receiving multiple medications. Being treated by a psychiatrist (OR = 2.038, p=< .011) was also correlated with increased the odds of polypharmacy. Older age exerted a small but significant effect (OR = 1.080, p = .042). Several predictors were associated with decreased odds of polypharmacy, including Black youth (OR = 0.505, p = .016). A higher number of placements before the initial prescription(s) also decreased the likelihood of polypharmacy (OR = 0.816, p = .016). Youth who entered care on no medication were correlated with markedly reduced odds (OR = 0.118, p < .001), a large effect suggesting different treatment pathways (see Table 3).
Placement Instability During the Two-Year Follow-Up
Placement Instability Post Initial Medication Prescription Linear Regression Analysis (Diagnosis and Medication)
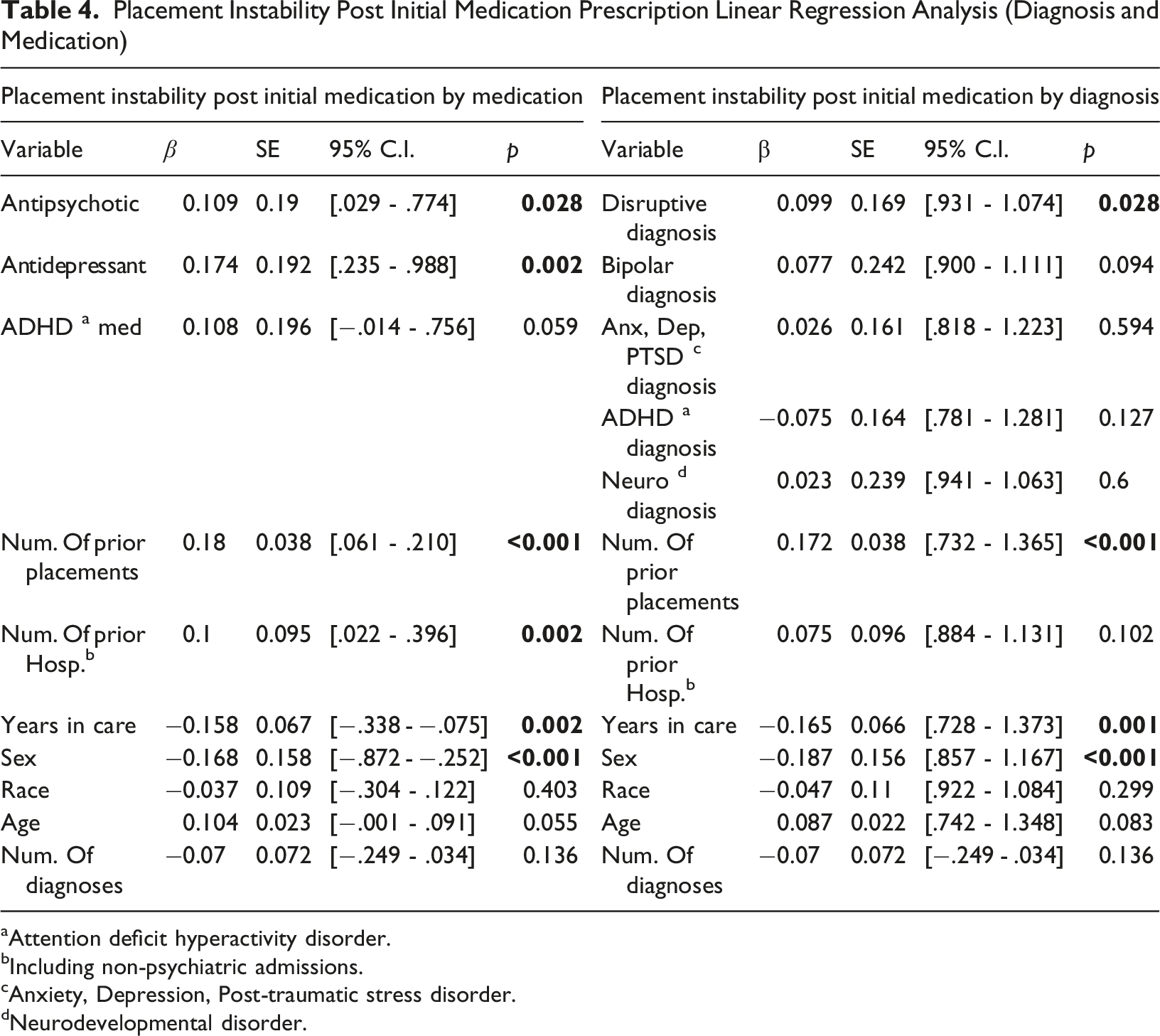
aAttention deficit hyperactivity disorder.
bIncluding non-psychiatric admissions.
cAnxiety, Depression, Post-traumatic stress disorder.
dNeurodevelopmental disorder.
The model including diagnostic categories was statistically significant (F (11,468) = 6.015, p < .001, R2 = 0.124). As shown in Table 4, youth with a disruptive behavior disorder experienced more placement moves (β = .10, p = .028). Fewer years in care before the first prescription predicted greater instability (β = −0.17, p = .001), as did having more prior placements (β = .17, p < .001). Being male predicted fewer placements in the two-year follow-up (β = −0.1987, p < .001).
Hospitalizations Post Initial Medication Prescription Multiple Regression Analysis
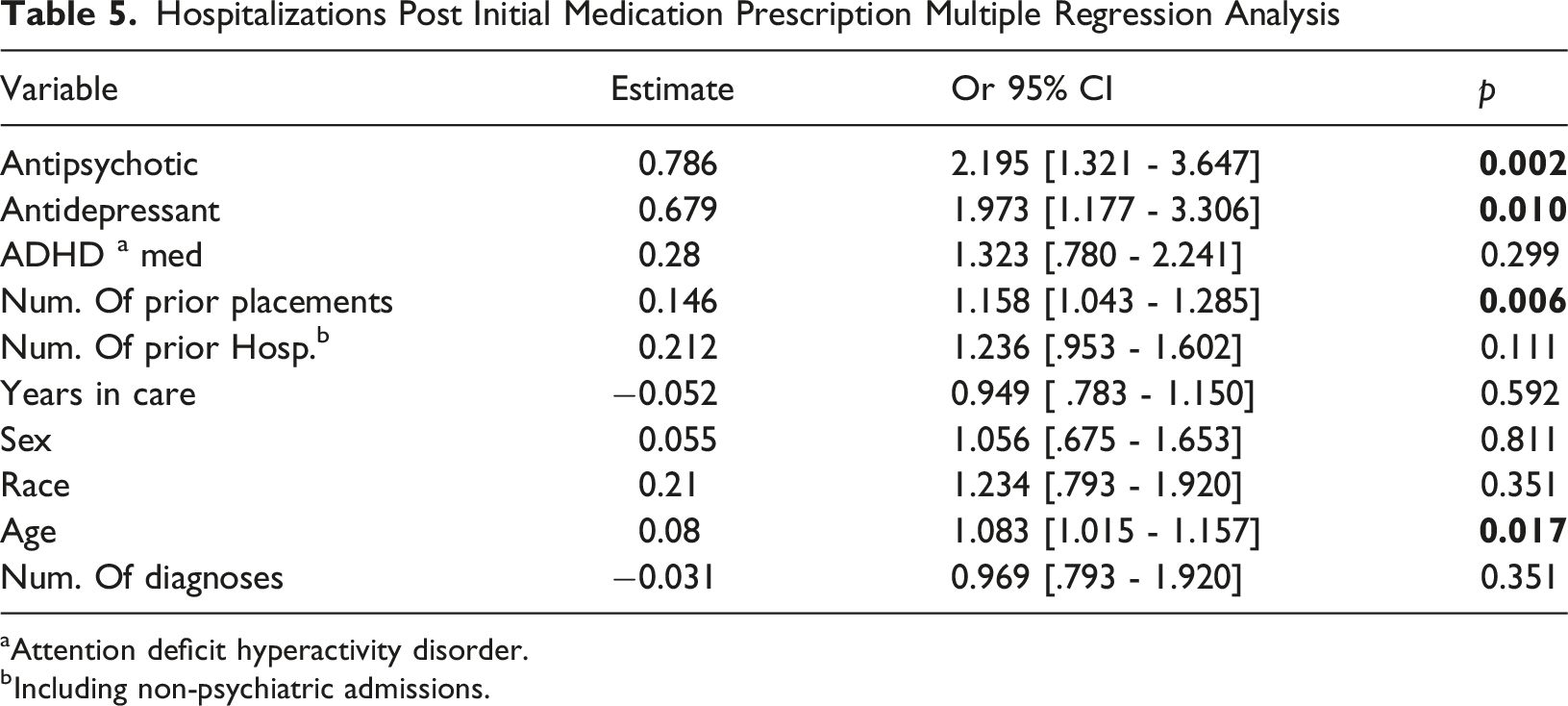
aAttention deficit hyperactivity disorder.
bIncluding non-psychiatric admissions.
Although each model evaluated multiple predictors, formal corrections for multiple comparisons (e.g., Bonferroni) were not applied. Such corrections can be overly conservative in exploratory observational analyses with correlated predictors and may obscure clinically meaningful associations by inflating Type II error. Instead, we emphasize effect sizes, confidence intervals, theoretical alignment, and consistency across models, and encourage cautious interpretation of small or marginal effects.
Discussion
Predictors of Initial Antipsychotic or Polypharmacy Prescription
Several demographic and clinical characteristics significantly predicted the initial prescription of antipsychotics or polypharmacy among youth in care prescribed at least one psychotropic medication. Consistent with prior research, males had higher odds of receiving an antipsychotic (Linares et al., 2013), a clinically meaningful finding given the magnitude of the effect. Black youth were less likely to be initially prescribed polypharmacy, although race was not associated with the prescription of antipsychotics. This pattern mirrors long-standing racial disparities in access to specialty psychiatry care and higher-intensity treatments (Medhekar et al., 2019; Zito et al., 2008). Age showed a nuanced effect: older youth were more likely to be prescribed polypharmacy but did not differ in likelihood of antipsychotic receipt. This may reflect greater diagnostic complexity over time, prior inadequate response to monotherapy, or provider comfort prescribing multiple medications to older adolescents.
Having a psychiatrist prescribe a youth’s initial medication was associated with higher odds of being prescribed an antipsychotic or polypharmacy. This is congruent with other studies (Zito et al., 2008) and may be a result of psychiatrists seeing individuals with more severe behaviors compared to other prescribers (Spencer et al., 2013). Similarly, hospitalized youth may be more likely to be treated by a psychiatrist. Youth not on medication upon entering foster care were more likely to be prescribed an antipsychotic or polypharmacy among youth with a referral for any psychotropic. While it would be expected that youth already on medication would have more behavioral issues, these results suggest that the lack of medication prescription upon entering care does not necessarily indicate less severe behavior. Before entering foster care, some youth may not have received psychiatric care due to caregivers not seeking or having access to such services. Alternatively, it could represent the development of severe emotional and behavioral disturbances after the youth enters care. As for diagnoses, having a disruptive behavior disorder or bipolar disorder predicted the prescription of antipsychotics. This finding aligns with what is considered the first line for bipolar disorder (Gautam et al., 2019), while use for disruptive disorders might indicate more severe symptoms involving aggression. Further, after controlling for other diagnoses, ADHD was associated with not being prescribed an antipsychotic for youth in this subpopulation. It is not uncommon for youth with ADHD to also have aggression or disruptive behavior (Saylor & Amann, 2016). Still, this finding suggests that within this subset of youth, ADHD diagnoses without this comorbidity are unlikely to be addressed with an antipsychotic. Having an ADP diagnosis or an ADHD diagnosis was correlated with being prescribed polypharmacy, even after controlling for other diagnoses. Among youth in foster care prescribed at least one psychotropic medication, these diagnoses might be less responsive to monotherapy than other diagnoses.
There were no significant associations between the number of prior placements or hospitalizations and subsequent antipsychotic prescriptions. These findings indicate that in this subpopulation, after accounting for the other predictors in Table 3, youth with more placements or hospitalizations are no more likely to be initially prescribed antipsychotic medications. At the same time, fewer prior placements were associated with being prescribed polypharmacy after controlling for diagnoses. This subset of youth may have had severe behaviors at the point of entry into care, leading to immediate prescription of multiple medications and possibly placement in a more restrictive setting, resulting in fewer placements. Similarly, more years in care were correlated with lower odds of antipsychotic prescriptions. As with the finding regarding the number of prior placements and polypharmacy, this might be explained by a proportion of youth entering care with severe mental health issues that are quickly identified and treated. Additionally, some youth may have an acute emotional and behavioral reaction to entering foster care, leading to an early prescription for an antipsychotic medication.
Two-Year Follow-Up Placement and Outcome Predictors
After the initial medication prescription, being female predicted more placements in the two-year follow-up compared to males in both the medication and diagnosis models. In this subpopulation, sex was not significantly correlated with hospitalizations. Some research has found either no association (Stenason & Romano, 2023) or that boys are specifically at a higher risk of placement instability (Clark et al., 2020). However, with respect to placement moves, one study found girls were predicted to have more long-term behavior problems (Aarons et al., 2010), potentially accounting for these sex differences. Prior research in the general population of children in foster care has shown that older age is associated with greater instability (James et al., 2008). Yet in this study, which included children with a much higher average age than in the general population of children in care, an increase in age was associated with more hospitalizations after the initial prescription but not with placement moves. Race was not significantly associated with the number of placements experienced or having an inpatient stay post-initial prescription.
Antipsychotic prescriptions were found to be associated with an increased number of both placements post-initial prescription and having an inpatient stay. Antipsychotics are typically prescribed for bipolar and psychotic symptoms or externalizing behaviors such as aggression and impulsivity, which have been shown in previous research to increase risk for placement changes (Stenason & Romano, 2023). Consistent with these findings, in a separate analysis that did not include medication type (due to multicollinearity), disruptive behavior diagnoses were associated with a greater number of placements for youth in this subpopulation. These results may indicate a challenge faced by foster parents, case workers, and child welfare agencies in collaborating and addressing the underlying behavioral issues that contribute to both medication use and placement instability. Other research suggests that the primary evidence-based treatments for disruptive behavior, which involve teaching caregivers effective behavioral strategies to address these issues in the home, are often not provided to foster parents (Leathers et al., 2021). The correlation between disruptive behavior diagnoses and antipsychotic medications points to the need to implement these psychosocial interventions for youth prescribed psychotropic medication and to study their potential to support strong relationships with caregivers and positive placement outcomes.
Unexpectedly, among youth prescribed at least one psychotropic medication, a prescription of an antidepressant medication was also associated with subsequent placement moves and hospitalizations. Antidepressants are first-line medications for anxiety and depression and are frequently used for the treatment of post-traumatic stress disorder. While some correlation has been found between internalizing diagnoses and placement instability (Aarons et al., 2010), in this study, in which disruptive behavior diagnoses were controlled for, an association between ADP diagnoses and instability was not found within this subpopulation. Antidepressants are likely to be an indicator of more severe symptoms, which may include self-harm or suicidal ideation, leading to a higher risk of hospitalization. Additionally, antidepressants have been found to be effective in the treatment of irritability in youth with disruptive mood dysregulation disorders whose symptoms have not fully responded to stimulant pharmacotherapy (Towbin et al., 2020).
Placement moves before the youth’s initial medication request were associated with an ongoing risk of difficulties for youth after medications were prescribed. More prior placements were correlated to both more hospitalizations and greater placement instability, even after controlling for medications. In the second model predicting subsequent moves, youth prescribed a psychotropic medication with more prior placements were more likely to have disruptive behavior diagnoses. This indicates that prior placement instability is associated with factors that are not successfully addressed by medication. This could be due to a lack of psychosocial services, greater severity of behavior issues among youth with more prior moves, or relational difficulties not captured by diagnoses.
A higher number of hospitalizations before the initial prescription was also predictive of placement moves in the model that included medications. However, within this subpopulation, no significance was found in the model including diagnoses, indicating that this association is due to risks related to specific diagnoses rather than the number of hospitalizations. Youths who experienced an inpatient stay prior to receiving an initial psychotropic medication may have had more severe baseline behaviors compared to youths with fewer hospitalizations. Even with the addition of medication, youth in this subpopulation may be at a higher risk for instability compared to their counterparts due to the initial severity of their behaviors. Lastly, in contrast to previous research (Oosterman et al., 2007), this study found that among youth prescribed at least one psychotropic medication, the longer a youth resided in DCFS care, the less likely they were to experience additional placements in the follow-up period.
Findings from this study point to a trauma-informed approach, which could help in viewing psychotropic medication as a supportive tool within a more comprehensive care plan and not necessarily a stand-alone treatment (Blaustein & Kinniburgh, 2010). Repeated disruptions in caregiving environments can disrupt stable attachment formation and emotional regulation, increasing behavioral difficulties that may require addressing factors beyond psychiatric interventions (Blaustein & Kinniburgh, 2010).
Limitations
Several limitations need to be considered. First and foremost, diagnoses were established clinically, typically without the use of standardized diagnostic instruments. This may affect the validity of the findings, as a lack of standardized diagnostics may decrease the accuracy and consistency of the data. Additionally, clinicians may have reported inaccurate diagnoses and symptoms in the belief that such reports would be more likely to lead to approval of their requested medications. Furthermore, the clinical information was limited to diagnosis. This limits the scope of interpretation, as more specific or severe behaviors could be stronger predictors than diagnosis. Similarly, the lack of measurement of concurrent psychosocial intervention measures weakens the validity of the findings, as variation in these interventions may have explained the associations between different medication prescriptions and outcomes such as placement instability. The data on medication were generated from psychotropic medication consent requests, which might not have included all prescribed medications (e.g., if the medication was paid out of pocket). The lack of treatment fidelity data may also affect the validity of the interpretations, as the data included only medication prescriptions, not necessarily medication adherence or implementation.
Additionally, in a small number of cases, information regarding placement history may be incorrect if a youth left care after an adoption and reentered care under a different DCFS ID and last name. While other identifying factors were used to identify these cases, it cannot be said confidently that all instances were accounted for. Although medication reviews followed standardized criteria, selection bias is possible because only youth who triggered a review (e.g., antipsychotic use, polypharmacy, higher-risk patterns) were included. Youth with lower clinical acuity or different prescribing trajectories may be underrepresented. Similarly, attrition related to non-follow-through with medication or early exit from care may reflect systematic differences between youth who remained in treatment and those who did not. Potential selection effects, such as symptom severity, placement stability, or engagement with services, could limit generalizability. Further, 20% of inpatient stays were not psychiatric, potentially weakening associations with this outcome. While statistically significant, some associations—particularly those with small effect sizes—should be interpreted cautiously. Although large and clinically meaningful effects were well-powered in this sample, smaller effects (OR <1.30) may be underpowered. Multiple predictors were examined across models; however, we did not apply formal corrections for multiple comparisons (e.g., Bonferroni), as such methods are highly conservative in exploratory observational research and can inflate Type II error when predictors are correlated. Instead, we emphasized effect sizes, confidence intervals, and theoretical alignment when interpreting findings and recommend caution when interpreting marginal associations. Results should be interpreted with caution, as this study only represents a sample of the Illinois population prescribed psychotropic medication within a statewide oversight program.
Implications
Findings from this study indicate that the subpopulation of youth in foster care who are prescribed psychotropic medications has a significant need for ongoing assessments and more effective services. More effective screening, comprehensive evaluations, and evidence-based services are needed for youth who are served by medication review programs. For youth with experiences that typically suggest less behavior severity (including not entering care on medication, fewer prior placements, and less time in care), those who were served by the review program were more likely than others to receive prescriptions for antipsychotics and polypharmacy, indicative of more severe psychiatric disorders. These youth might have higher levels of trauma prior to entering care or have entered care in part due to their significant mental health needs. Trauma symptom screening should be integrated into initial assessments. Despite the high level of trauma experienced by children in foster care, many states do not routinely administer trauma screening, which has been found to increase referrals to trauma-focused interventions (Connell et al., 2024). Systemwide trauma-informed child welfare initiatives have also been shown to strengthen child-caregiver relationships and improve outcomes (Bunting et al., 2019). Policy and training efforts should prioritize cross-system collaboration between child welfare and mental health providers and expand foster parent and provider training on trauma-responsive care and evidence-based interventions for foster children.
Services that combine medication management with evidence-based interventions to address disruptive behavior early in the youth’s child welfare tenure may lessen the risk for adverse placement outcomes (Bywater, 2011; Eisenberg et al., 2023). Requiring concurrent psychosocial interventions that focus on providing caregivers with effective strategies to parent and support children and adolescents with trauma histories (Kemmis-Riggs et al., 2018) when youth are prescribed psychotropic medication could improve outcomes and potentially reduce children’s reliance on medication. Utilizing a trauma-informed approach at all levels, with a focus on attachment, improving emotional regulation, and developmental competencies (Blaustein & Kinniburgh, 2010), may also be beneficial by ensuring that caregivers and caseworkers are supported in providing trauma-sensitive care.
While all youth served by a medication review program should receive additional screenings and more effective services, findings from this study point to subgroups within this high-risk population that should be flagged for intensive follow up. Youth who are prescribed antipsychotics, antidepressants, or polypharmacy, as well as those with disruptive behavior and prior placement instability, were at greater risk for subsequent placement instability and hospitalizations. Trauma-informed service models throughout the systems in which these youth are served are needed to support stability, and placements should incorporate evidence-based interventions to support both caregivers and youth (McPerson et al., 2018). Proactive services should focus on strengthening relationships, increasing caregiving support and positive parenting, and managing trauma reactions to reduce the risk of placement moves and increase the chances of permanency.
Conclusion
Youth who are served by statewide psychotropic medication management review programs continue to be at risk for hospitalizations and placement instability, with specific, identifiable clinical characteristics associated with higher risk. Further research would aid in the understanding of how to address these foster care-specific mental health challenges more comprehensively. While medication management programs have been successful in increasing oversight of children’s mental health needs and the types of medications that they receive, they have untapped potential to ensure that appropriate services are provided and reduce medication use when possible. Specifically, future research on integrated medication and psychosocial interventions and placement trajectories for youth in care is needed.
Footnotes
Author note
This study was presented, in part, at the 70th Annual Meeting of the American Academy of Child and Adolescent Psychiatry, New York, NY, October 23-28, 2023.
Roberto Lopez-Tamayo, PhD, served as the statistical expert for this research.
Acknowledgements
The authors would like to thank Prashant Patel, BS, of the University of Illinois at Chicago Clinical Services in Psychopharmacology for his help in managing the consent data and Catherine Francis, MPP, Associate Director of the Clinical Services in Psychopharmacology, for coordinating the efforts of the psychotropic medication consent program.
Ethical Considerations
The Institutional Review Board of the University of Illinois at Chicago and DCFS reviewed and approved all study procedures.
Consent for Publication
We confirm that this work is original and has not been published elsewhere, nor is it currently under consideration for publication elsewhere.
Child Welfare Outcomes (2016), Report to Congress, (2024), dosReis et al., (2014), Goldstein et al. (2024), Leathers (2006), SSA, n.d.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded in part by a contract between the Illinois Department of Children and Family Services and the University of Illinois at Chicago Board of Trustees.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Veronique Calmels and Dr. Naylor are employed through a contract between the Illinois Department of Children and family Services and the University of Illinois at Chicago. Dr. Naylor is the Psychiatric Consultant for the Illinois Department of Children and Family Services. Dr. Leathers and Dr. Lopez-Tamayo have no biomedical financial interests or potential conflicts of interest.