
Abstract
Abstract
Children living in sub-Saharan African (SSA) countries face a plethora of challenges that require adaptation and resilience for them to develop typically. The experiences of epidemics, armed conflicts, and many other man-made and natural disasters create abject poverty and psychological issues: the vulnerable children become orphans and/or refugees in addition to premature deaths because they lack safety nets. This article explores the role of faith (i.e., religion or spirituality) as a source of resilience with regard to chronic stressful life events experienced by children. There is need to establish the role of faith in children's lives because of the different types of adverse events that impact child development. African countries are inundated by many hazards that impact children more than any other age group and this trend requires urgent intervention by all stakeholders. At research level, there is need to conduct studies that explore, over prolonged periods of time, the processes and role of spirituality/religion (S/R) in facilitating or inhibiting children's adjustment to traumatic experiences. Additionally, at policy level, there is need for governments in SSA to implement policies, intervene and protect children; in addition to encouraging collaboration among the religious fraternity, traditional leaders, and other stakeholders to make the world a better place for children.
Introduction
Childhood is a critical period for child development, yet children from low to middle income countries (LMIC) face a confounding array of biopsychosocial risks that may put pressure on their adaptive capacities and affect their developing brain and mental health (Evans & Cassells, 2013). Nonetheless, children all over the world are exposed to immense stress such as divorce and illnesses, while others encounter catastrophes such as war, poverty, drought and floods. All these catastrophes increase poverty because, more often than not, children lack protection and assistance programmes, thereby increasing exposure to stressful environments. How parents or caregivers respond to these stressful situations, and how they assist their children to respond, plays a significant role in showing a distinction between adults who promote or inhibit resilience in the children.
Sub-Saharan Africa (SSA) experiences many epidemics (e.g., HIV and AIDS, cholera and malaria), armed conflicts and many other disasters, creating susceptibility to significant health problems. Civil and religious wars create refugees and asylum-seeking groups, in addition to deaths (Ögtem-Young, 2018). Different communities are prone to different types of stressors, suggesting the use of different defence mechanisms to enable children to adapt to stressful environments to mitigate negative consequences. If children do not deal with stressors efficaciously, they may fail to negotiate adolescence. This failure may lead to risky behaviour, for instance, living on the streets, substance use and promiscuity (Evans & Cassells, 2013; Mosavel, Ahmed, Ports, & Simon, 2015) and dropping out of school. However, it may not be prudent to claim that the children have failed; rather society and the system are to be blamed for failing to intervene and help the children, who are trying to eke a living.
In addition to the foregoing risks, SSA communities have to adapt to orphanhood due to AIDS deaths and civil wars. Orphanhood gives rise to child-headed households (CHH) and most of the times ‘crisis fostering’, whereby family breakdown necessitates the child’s movement (Alber, Martin, & Notermans, 2013). CHH and unplanned movement may lead to a plethora of disorders and chronic stress if there are no resources and appropriate intervention.
Despite all the confounding factors, the death of a household member was found to be associated with higher stress levels (Hjelm, Handa, de Hoop, & Palermo, 2017; UNICEF, 2017c; Wild, Flisher, & Robertson, 2011). Whether such experiences defeat or strengthen a child depends, in part, on his/her resilience since resilience manifests itself in diverse contexts. Additionally, protective factors or resources available may assist children in building resilience. Intervention may also help children become resilient and enable coping with childhood adversities. Previous research has shown the role of protective factors (personal, social and environmental assets) in resilience (Anastasova, 2014; Centres for Disease Control and Prevention, 2017). Spirituality/religiosity (S/R) as a social asset was found to influence resilience in youths in previous studies in Zimbabwe, South Africa, Mexico and elsewhere (Bruce et al., 2012; Mosavel et al., 2015; Vinueza, 2016). The associations were also found among older caregivers (Reis & Menezes, 2017; Shaibu, 2016). Seeking spiritual support, forgiveness, religious purification and positive perceptions were associated with less psychological distress and post-traumatic growth (PTG; Anastasova, 2014; Brewer-Smyth & Koenig, 2014; Wild et al., 2011). Psychologists may also include the spiritual needs of their patients in therapy. Including S/R needs assists in identification of patients’ ‘spiritual values and history, belief systems, unhappiness, and needs’ (Rego & Nunes, 2016). While some children may require S/R guidance and work with spiritual care workers, others may possess completely different needs. The most important factor is that each child should be treated as a unique individual by addressing his/her biopsychosocial, physical and spiritual needs, if warranted.
Despite the above, children do not have access to counsellors most of the time nor do they have access to any other protective factors to transcend adversity in SSA communities because they have no control over resources. Nonetheless, resilience is the concept that despite many negative factors within their lived contexts, they can still withstand destructive environments, develop resistance, and therefore thrive (Craig, 2012; Masten, 2018; Southwick, Bonanno, Masten, Panter-Brick, & Yehuda, 2014). They can achieve this mammoth task mostly with the help of parents or caregivers, particularly when still very young. When children move from one developmental stage to the next, they shift their reliance from outside support to their own skills, while continually building and strengthening their personal attitudes and feelings, thereby building resilience (Drutchas & Anandarajah, 2014). Caregivers, if training children to be resilient, should take cognisance of the developmental stages.
Developmental milestones assist in validating and reassuring caregivers that they are providing requisite knowledge and skills needed to raise a healthy and well-adjusted child. Children’s early experiences, for instance, the type of attachments they form with their caregivers and their first learning experiences, have a huge influence on their future physical, cognitive, emotional and social development (Drutchas & Anandarajah, 2014; Sigelman & Rider, 2015). A well-adjusted child, therefore, has a high probability of dealing with challenges encountered and overcoming adversity because risk factors increase the likelihood of negative cognitive, behavioural and health outcomes. Previous research in Eritrea, Nigeria and Rwanda attested to the foregoing, young children between the ages of 0 to 3 years old are exposed to malnutrition, disease, stress and violence during episodes of forced displacement and deprivation that will have negative long-term effects (Akresh, Lucchetti, & Thirumurthy, 2012) during different developmental milestones. Nurturing children to have a positive perception and relationship with God at a very early stage (neonatal) in their lives through interaction with their guardians and precinct or environment will help in building resilience. Children who have a positive or optimistic image of a higher being (e.g., God) are better equipped to deal with vulnerabilities than their counterparts and are more likely to cope with adverse events before adversity occurs (Vinueza, 2016).
Although we recognise the multidimensional nature of resilience, this article focuses on the role of faith as a source of resilience with regard to traumatic life events and chronic stress (e.g., children infected or affected by HIV). The article reviews the literature on the role of faith on resilience of children including adolescents, with a focus on sub-Saharan Africa. The article begins with conceptual clarifications followed by distribution of religions and the age structure and hazards in SSA that need resilience. The next section analyses previous studies on S/R and resilience. Further
Conceptual Clarifications
Most people confuse the use of the words spirituality and religion. We tend to agree with Drutchas & Anandarajah’s perspective that the boundaries of the two terms cannot always be separated (Cornah, 2006; Drutchas & Anandarajah, 2014). Popcak posits that there is nothing wrong with using the terms ‘faith’, ‘spirituality’, ‘belief’ and ‘religion’ interchangeably even though he did not use them interchangeably (Drutchas & Anandarajah, 2014; Popcak, 2014). Both spiritual and religious usage include ‘a search of the sacred’ as part of the definitions (Meichenbaum, 2007). Nonetheless, spirituality is defined as an attempt to seek purpose and meaning in life, and a direction of life in relation to a universal spirit or God (Cotton et al., 2012; Meichenbaum, 2007; Popcak, 2014), inclusive of empowerment, service to others, empathy and compassion. According to Miller (2015, p. 1),
Spirituality is an inner sense of relationship to a higher power that is loving and guiding. The word we give to this higher power might be God, nature, spirit, the universe, the creator, or other words that represent a divine presence. But the important point is that spirituality encompasses our relationship and dialogue with this higher presence.
Religion is defined as a form of social institution with its accompanying beliefs, practices, symbols and rituals (Meichenbaum, 2007; Ögtem-Young, 2018). Religion also encompasses sense of belonging, code of ethics, frequency of religious attendance and prayer as part of its definition. Nevertheless, faith is a strong belief in the doctrines of a religion, based on spiritual conviction rather than proof and assurance that God’s promises will never fail (Popcak, 2014). This definition of faith encompasses spirituality and religion. This article will use spirituality/religion (S/R) to denote faith. From a psychological perspective, faith is an innate drive to search for meaning, purpose and significance (Popcak, 2014; Ungar, 2014). Ögtem-Young posited that faith is used as a tool of resilience (Ögtem-Young, 2018; Ungar, 2014). S/R serves important roles in coping, survival, and maintaining overall well-being within sub-Saharan African cultures and communities, especially after diagnosis of HIV/AIDS, thus helping to maintain good mental health, especially for orphans.
Resilience is the concept that regardless of many negative experiences, people still bounce back and adapt in response to stress, challenges, threats and adverse life events (Craig, 2012). Previous research findings have revealed that resilience protects against and may reverse; traumatic experiences (e.g., tragedy, adversity and threats), psychopathology (e.g., depression, anxiety, fear, helplessness and other negative emotions), and thus is a resource for health and well-being (Ungar, 2008, 2013). Ungar’s definition was more comprehensive—he added ‘context and culture’ (p. 221), and ‘navigation and negotiation’ (p. 225) to the foregoing definition of resilience (Ungar, 2008). Resilience also deals with the capacity to flourish in the face of adversity.
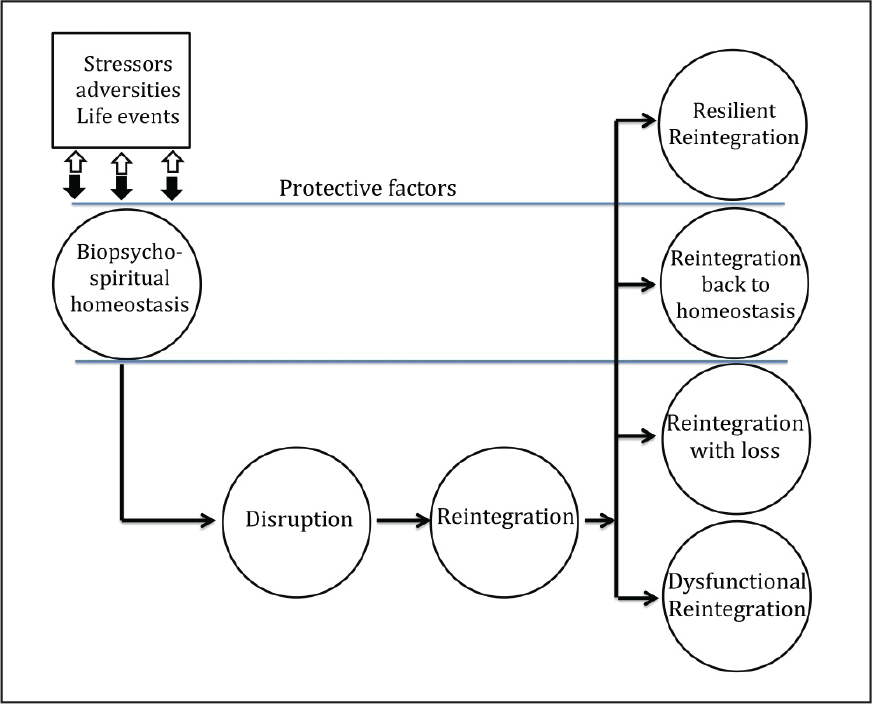
There are many definitions of resilience, but for this article we will surmise that resilience usually becomes an important factor after a crisis, devastating or adverse event (e.g., a disaster like Cyclone Idai). Other examples, for instance, the kidnapping of the school girls by Boko Haram in Nigeria and homophobia in South Africa have left survivors devastated and more often than not, struggling with post-traumatic stress disorders (PTSD). These potential threats at a grand scale require individuals and communities to be resilient as risk and danger are difficult to diminish through protective and preventive measures of governments and policymakers (Ögtem-Young, 2018). The events keep occurring at intermittent intervals. A definition of resilience that includes a spiritual source of strength is also ideal (Richardson, 2002) for this article (see Figure 1).
With regards to adolescents, they are considered as children the world over. Children will thus include everyone under the age of 19 years. However, recently, the age range for adolescents has been increased from 10–19 years to 10–24 years (Sawyer, Azzopardi, Wickremarathne, & Patton, 2018). The authors concurred that the shift was a result of delayed timing of role transitions, for instance, completion of education, marriage and parenthood, which continue to shift popular perceptions of when adulthood begins. The Adolescent Health Committee (2003) would concur with this change since they believe that society favours a more functional definition based on the biopsychosocial readiness of young people to enter adulthood. The committee unequivocally stated that adolescence began with the onset of physiological normal puberty and ended when an adult identity and behaviour become accepted. Thus, we will use the new age range for adolescents and they are also considered as children in this article.
The next section addresses the distribution of religions and the age structure in some parts of SSA.
Distribution of Religions and the Age Structure in Some Parts of SSA
The most widely practiced religions in Africa are Christianity (45%) and Islam (40.6%; Pew Reasearch Center, 2015). The Botswana Council of Churches posited that Pentecostal churches (Christians) comprise 73 per cent of faith-based organisations (FBOs) in the country and are the majority faith community (Ögtem-Young, 2018). Christianity is common in the whole of sub-Saharan Africa, whereas Islam is found mostly in North Africa and the Horn of Africa. In addition to Christianity and Islam, there are other smaller religious groups, for instance, folk religions and a few Africans are religiously unaffiliated. The practiced religions are often adapted to African cultural contexts and belief systems and are usually combined with the practice of traditional beliefs. By 2060, the number of Christians living in SSA are expected to increase from approximately 26 per cent to more than 40 per cent (Pew Research Center, 2015). Mcclendon also posited that people who are religious in SSA are relatively young and have more children than their counterparts elsewhere (European Christians), thereby contributing to the projected rapid population growth in the ensuing decades (Pew Reasearch Center, 2015). However, according to the Pew Research Centre, Muslims are increasing more rapidly than Christians.
Approximately 46 per cent of the region’s Muslims were under 15 years, 41 per cent of the 44 per cent of followers of folk religions were Christians and 40 per cent were unaffiliated (Pew Reasearch Center, 2015). The centre also reported that the median ages of these groups ranged from 17 (for Muslims) to 20 (for the unaffiliated). The median age for SSA as a whole was found to be 18 (Pew Reasearch Center, 2015), confirming how young this group is. This young generation needs resilience to cope with the many adversities encountered in their communities. The adversities include hazards (e.g., man-made and natural disasters), chronic illnesses, and high rates of poverty, unemployment, substance use, overcrowding and many others. The hazards that are common in SSA will be discussed.
Hazards in Sub-Saharan Africa that Need Resilience
With a population of 761,390,000 from its 53 countries, Africa’s population is highly susceptible to disasters (Centre for Research on the Epidemiology of Disasters, 2017). Africa’s natural hazards are mainly endemic diseases, drought and floods. The natural disasters interact with man-made ones, such as civil wars; air, road and railway incidents and industrial hazards (e.g., mining accidents). Although Africa is less prone to natural disasters than other continents, 20 out of 100 occur in Africa and the continent suffers 60 per cent of all disaster-related deaths (Centre for Research on the Epidemiology of Disasters, 2017; Loretti & Tegegn, 1996). This is probably due to the type of hazards that affect the African continent, under-reporting and the circumstances prevailing in Africa (e.g., poverty and fragile economies) make it easy for any disaster to escalate and multiply its impact, for instance, the recent Cyclone Idai.
In the immediate aftermath of Cyclone Idai, one of the worst weather-related disasters in the Southern Hemisphere that landed on 14 March 2019, 1.5 million children were affected in Zimbabwe, Mozambique and Malawi. The World Vision’s Response Director for Cyclone Idai was worried about its impact on children because the cyclone showed how vulnerable children were from these kinds of disasters that displaced people, destroyed homes, crops and forced large numbers of children out of school due to damage and schools being used as evacuation centres (World Vision, 2019). Most children interviewed reported coping through talking to members of the clergy and Sunday school teachers, counselling, being listened to and singing gospel songs (personal communication). The foregoing view alludes to the fact that ‘faith based communities can provide psychosocial healing by exercising their pastoral vocation through counselling’ (Vinueza, 2016, p. 11), particularly after exposure to an adverse event. For disaster settings like cyclones, rituals may be reflected in the building of shrines or the provision of religious relics that encourage religious practice (Vinueza, 2016).
Although endemic diseases (e.g., HIV and AIDS, malaria), armed conflicts, road traffic injuries, floods, storms and earthquakes occur more in certain countries than others (Centre for Research on the Epidemiology of Disasters, 2017), children in these countries all require adaptive capacities and resilience. The Global Burden of Disease Project by WHO and the Demographic and Health Survey (DHS) programme by the United States Agency for International Development (USAID) have documented health conditions and diseases, both endemic and epidemic that inhibit resilience. For instance, SSA is home to only 12 per cent of the global population, but accounts for 71 per cent of the global burden of HIV infection, which is estimated to be 25.6 million (UNAIDS, 2017a). Nonetheless, the scaling up and widespread coverage of antiretroviral therapy (ART) has led to a substantial decline in new HIV infections, although the incidence rate is still unacceptably very high, especially in South Africa (23%; UNAIDS, 2017b). About 15 per cent of those infected were women aged 15–24 years (UNAIDS, 2017b). Nonetheless, most religions discourage premarital sex. If the children are brought up in these religious institutions, the incidence rate among children would be greatly reduced. Resilience would also be requisite for children to survive this pandemic as they face a plethora of challenges due to the epidemic.
In addition to HIV, the second most prominent disaster affecting Africans is floods. In 2016, more than 41 million people were affected by floods (Centre for Research on the Epidemiology of Disasters, 2017). Cyclone Idai impacted 3 million people and caused damages worth 2 billion USD (Bearak, 2019). These disasters affect children more as they have no means of dealing with the aftermath or trauma. Victims require support to bounce back from these traumatic events. Children lack protective factors and are thus more vulnerable. According to Meichenbaum (2007), most people in North America cope with trauma by turning to prayer and religion. This finding is not peculiar to North Americans, the same applies to sub-Saharan Africans. Trauma exists the world over and coping is dependent on protective factors available, and S/R are examples of protective factors.
With regards to displacement due to armed conflicts, SSA accounts for 13 of the 20 countries hosting the larger number of refugees in the world (UNAIDS, 2017a). By the end of 2016, a record 65.6 million people were displaced as a result of persecution, conflict, violence or human rights violations (UNAIDS, 2017a). Contrary to popular media claims, LMIC host 10.1 million refugees or 86 per cent of the world’s refugees (UNCHR, 2015). Most of these are from Iraq, Syria and Yemen. The highest number of refugees in SSA are in Uganda and are mostly from South Sudan (UNCHR, 2015). However, Somalia, Sudan, South Sudan, Eritrea and the Democratic Republic of Congo (DRC) accounted for about one-third of the total number of refugees from SSA, although UNHCR claims it is difficult to have accurate figures. Refugees are mainly hosted in camps in peripheral and poor areas; therefore, it is inconceivable to imagine the implications to children who also become refugees. The strong presence of children in Africa’s refugee population implies that we should also look at the potential long-term effects of forced displacement on survivors. The share of children and women among refugees is higher in Africa than elsewhere, in particular East and West Africa. Thus, any action to benefit refugee children needs to start from a recognition of their innate value, worth and their positive capacities as creatures made in the image of God (Dillen, 2012, p. 71). The children need to adapt (resilience); they also need schooling and health services.
S/R provide key elements to cope for people dealing with post-traumatic effects (Brewer-Smyth & Koenig, 2014; Goldhill, 2018; Ögtem-Young, 2018; Shaw, Joseph, & Linley, 2007; Ungar, 2014). For instance, in African communities, church congregations visit those undergoing severe trauma or the bereaved in their homes, pray together and offer their support, which are invaluable for recovery. In other instances, traumatic experiences deepen people’s faith, as they may turn to S/R for relief and emotional release (Brewer-Smyth & Koenig, 2014; Shaw et al., 2007; Ungar, 2014). Previous researchers in Iran (Jenaabadi & Mir, 2019) and the USA (Brewer-Smyth & Koenig, 2014; Ungar, 2014) found a high correlation between S/R and resilience in the hope for a better future. Religion and spirituality constitute ‘a source of emotional and cognitive support, a form of social and political expression and mobilization, and a vehicle for community building and group identity’ (Gozdziak & Shandy, 2002, p. 129).
Positive S/R coping, religious openness and participation, and intrinsic religiousness were found to be associated with post-traumatic stress (Brewer-Smyth & Koenig, 2014; Shaw et al., 2007). In addition, positive S/R coping lessened the chances for developing depression and maladaptive coping strategies in adolescents (Reynolds, Mrug, Hensler, Guion, & Madan-Swain, 2014). The next section addresses associations between S/R and resilience in previous studies.
Previous Studies on Influences of S/R in Resilience
Although there has been a dearth of information on research with regards the role of faith on children’s resilience in sub-Saharan Africa, a pilot study by Mpofu et al. (2011) in Zimbabwe revealed that youths’ resilience practices are supported by church affinity and a broad collectivistic cultural model embedded in extended family obligations. The finding most likely applies to other Southern African countries. S/R played a pivotal role in resilience building in the face of stressors, particularly health issues, therefore enhancing adaptability and coping (Cotton et al., 2012; Dillen, 2012; Hunter-Hernández, Costas-Muñíz, & Gany, 2015; Ögtem-Young, 2018; Ungar, 2014), although other protective factors also played a significant role (Ögtem-Young, 2018). In addition, childhood spirituality was found to be related to chronic disease coping (Drutchas & Anandarajah, 2014), therefore, resilience. Further, multivariable models of an African/American study revealed that having a religious preference was associated with higher levels of S/R (R2 = 0.07–0.25, P < .05; Cotton et al., 2012). The other factors that were found to be associated with resilience in previous studies were personal assets (e.g., high self-esteem) and different types of supports (Brewer-Smyth & Koenig, 2014; Mosavel et al., 2015). S/R also provided survivors with a sense of self-control, sense of identity and an understanding of their stressful situations (Manning, Carr, & Kail, 2016). Parents or caregivers of children living with disabilities fall into this group. They are strengthened by their faith so as to cope and build resilience against disability (Manning et al., 2016; Pandya, 2018).
Meichenbaum (2007) reported that about 43 to 60 per cent of people who had emotional problems were found to turn to their priests first for help, leading to resilience. Survivors’ resilience was also found to be influenced by spiritual meaning-making and perceptions of events determined how the survivors dealt with their negative life experiences (Glenn, 2014). The health belief model (HBM) comes into play here. The HBM postulates that messages will achieve optimal behaviour change if they successfully target perceived barriers, benefits, self-efficacy and threats or consequences (Jones et al., 2015).
Glenn (2014) explained how resilience could be interpreted in a theological manner using three themes, namely spirituality, grace and resurrection/hope, while Manning named the components of resilience as ‘having divine support, maintaining purpose, and expressing gratitude’ (Manning, 2012, p. 352), which were said to promote and maintain well-being (Ögtem-Young, 2018). In addition, positive patterns of religious coping such as seeking help in letting go of anger facilitate resilience (Roehlkepartain, King, Wagener, & Benson, 2006). The interpretation and components of resilience named herein show a relationship to S/R (i.e., resurrection, divine, etc.).
Furthermore, 20 previous studies were reviewed in Australia and 12 (60%) reported positive associations between S/R and quality of life (QOL), hence resilience (Counted, Possamai, & Meade, 2018). Other previous studies showed a high correlation between QOL and resilience (Mhaka-Mutepfa, 2018; Mhaka-Mutepfa, Mpofu, & Cumming, 2015). From time immemorial, S/R has always been said to provide a sense of togetherness, belonging, cohesion and comfort from the feeling that you are not alone regardless of your age. In many SSA communities, poverty, HIV/AIDS and other hazards have resulted in children facing many challenges in most aspects of their lives (Mhaka-Mutepfa et al., 2008), which calls for S/R.
In a previous study in Sri Lanka, orphans were found to have inner peace and resilience after exposure to war (Fernando & Ferrari, 2011). The authors revealed that the orphans received divine intervention from their Buddhist and Christian practices, which were used to promote faith, personal well-being and a sense of belonging, helping them to be resilient. The children living in orphanages were also taught Buddhist and Christian values which recognised peace and compassion, despite having been exposed to war. However, the children studying in Sri Lanka were still exposed to risk because they had no access to parental love and guidance. Given the importance of the formation of a secure attachment relationship in early childhood, disturbances to the parent/caregiver–child relationship in these early years are particularly traumatic for young children. Young children depend on their caregivers for protection from external stressors and for helping them to understand how to respond to stressful/traumatic events (Brewer-Smyth & Koenig, 2014; Goldhill, 2018; Shaw et al., 2007). When parents cannot provide this protection, young children’s development and well-being becomes increasingly vulnerable to poor outcomes.
Resilience from S/R was found to prevent, minimise and overcome the damaging effects of orphanhood and war. The same intervention strategies that were used in Sri Lanka can be used with SSA children of similar faith. The 15 war torn countries in Africa (e.g., Nigeria, Sudan, Somalia, etc.) that are experiencing post-war conflict and tension can make use of these evidence-based practices. The finding that S/R plays a key role in facilitating children’s resilience to war-related trauma should be taken seriously by stakeholders who work with children who have been exposed to such trauma. Particularly taking into account the fact that such children are deeply affected precisely because the cultural systems (e.g., family, neighbourhoods and schools) that normally function to support and protect their development have been severely damaged or destroyed (Wright & Masten, 2005). Thus, S/R can assist children in coping with illnesses and trauma, separation from family, experience of loss and identifying ways of dealing with debilitating negative feelings.
In another study, South African youths reported that the community and individual resilience they had were a result of community connectedness, hope and altruism (Mosavel et al., 2015). The finding is similar to other research findings (Glenn, 2014; Ögtem-Young, 2018), which is an important implication for positive youth development efforts. In South Africa, because of an influx of refugees from other African nations and a high incidence of crime, community connectedness, hope and altruism are required attributes to prevent xenophobia. The three qualities are also preached and recognised highly among Christian values; no wonder there is a positive influence on resilience. While, hopelessness, especially in the youths, encourages them to get involved in risky behaviours (e.g., substance use, promiscuity, etc.), community hope, which may result from S/R, establishes the ability for them to remain positive regardless of all the adverse events encountered (Manning, 2014; Mosavel et al., 2015).
In addition, community connectedness was said to provide an opportunity for residents to have a sense of belongingness and associated negative experiences (Ahmed, Albalawi, Alshehri, AlBlaihed, & Alsalamah, 2017; Mosavel et al., 2015). This finding was more prevalent among adolescents as they are at a stage where they seek self-identity. Nonetheless, coping and hope were found to be evident among many African youths who, regardless of poverty, illnesses and violence, are still hopeful that divine intervention will reduce crime and risky behaviours (Ahmed et al., 2017). For instance, Ahmed et al. (2017) quoted one female participant, ‘I was thinking if I could be Cinderella or God I would change all the minds of the people so that they could be saved instead, and I know that they wouldn’t rob people if they are saved’. The excerpt confirms the perception that faith plays a crucial role in people’s lives to enable overcoming the odds. Ethnic minority communities and migrant groups, in most African countries, require resilience and coping strategies inclusive of faith to manage the challenges encountered. The foregoing studies show how faith is used as a tool of resilience by youths from diverse communities. The findings suggest that youths can discern concerns explicitly about the many risk factors in their communities.
Acknowledging these difficulties is a good way of encouragement in building resilience, thereby confronting the risk factors. Thus, extant literature shows that S/R promotes resilience through processes such as attachment relationships, provision of social support, provision of guidelines for conduct and moral values as well as provision of opportunities for personal growth and development. However, S/R does not always have a positive role in building resilience, for it can be two-pronged. Meichenbaum reiterated that religious activities, including faith-based interventions, interfere with healing by affecting coping and the healing processes, either negatively or positively (Drutchas & Anandarajah, 2014; Meichenbaum, 2007). The next section addresses the negative impact of S/R on resilience.
The Negative Impact of S/R on Resilience
Previous scholars have found that S/R can also have a negative impact on resilience (Brewer-Smyth & Koenig, 2014; Drutchas & Anandarajah, 2014; Mpofu et al., 2011; Ögtem-Young, 2018). Investigations by Drutchas and Anandarajah revealed that spiritual beliefs either support or hinder children’s ability to cope with chronic illnesses (Drutchas & Anandarajah, 2014). Faith was also found to be associated with mental health, that is, neuroticism (e.g., anxiety, fear, stress, depression, etc.) and psychotic disorders (i.e., schizophrenia and schizoaffective disorders) when perceptions and understandings of S/R rest upon negative feelings and beliefs (Brewer-Smyth & Koenig, 2014; Ögtem-Young, 2018; Reynolds et al., 2014). In addition, some caregivers may destroy resilience in children by sending S/R messages that inhibit resilience. The reason children experience negative effects is that under certain conditions S/R and other forms of faith-based interventions can interfere with adaptive coping and healing processes for children in crisis (Drutchas & Anandarajah, 2014; Meichenbaum, 2007). This finding was supported by Counted et al.’s review of studies in Australia; 3 out of 20 (15%) of the studies reported inverse associations between S/R and QOL, therefore, resilience (Counted et al., 2018). The finding confirms that the interference could go either way and S/R could also be a source of susceptibility.
In the case of vulnerability, for example, certain spiritual beliefs, values and myths can interfere with the children’s health-seeking behaviours. Apostolic Faith church goers in SSA may not seek medical services for their children (Mpofu et al., 2011), for instance, immunisations for communicable diseases, because of their S/R beliefs. Studies on Apostolic faith organisations done in Zimbabwe (Ha, Salama, Gwavuya, & Kanjala, 2014; Mpofu et al., 2011) and Botswana (Mpofu et al., 2011) revealed that children were exposed to health risks from obligatory roles and teachings that prevent health-seeking behaviours. Members of the Apostolic Church of God do not use traditional or modern medicine or allow authorities to immunise their children, claiming that illness can only be healed through prayer (Mpofu et al., 2011). In Botswana, the permanent secretary of that era in the Ministry of Health sought the intervention of the high court with regards to immunising children. The high court subsequently ruled that parents or guardians refusing immunisation of their children would be charged with child abuse. Nonetheless, implementation may be difficult because identifying culprits is problematic.
In another study in Zimbabwe (Kriss et al., 2016), children were more likely to have received no basic vaccinations (aOR = 1.83, 95% CI: 1.22–2.77) than children of non-Apostolic organisations, and they were less likely to have a vaccination card (aOR = 0.68, 95% CI: 0.52–0.89), despite advocacy and awareness campaigns to educate the sect on the importance of vaccinations. Thus being affiliated with the apostolic faith is a significant risk factor in reducing the utilisation of health services, thereby exacerbating chronic illness and death. Nonetheless, LMIC were less subjected to a full series of vaccines than their counterparts (Oyo-Ita et al., 2016; UNICEF, 2017b), for several other reasons.
A previous study found four factors that hindered mothers taking up immunisation for their children in Senegal: (a) geographic area; (b) mother’s characteristics (e.g., level of education); (c) not attending ante-natal clinic; and (d) not giving birth at a health facility (Mbengue et al., 2017), with factors (c) and (d) also non-existent among most Apostolic faith organisations . Mbengue’s results justify why most of the Apostolic Faith organisation congregates fail to seek health services in SSA as they lack three of the factors (b to d). Other factors inhibiting immunisation uptake in SSA were suggested by previous researchers (Adeloye et al., 2017). They did a systematic review in Nigeria and found that busy schedules of mothers, shortage of vaccines, vaccine safety concerns and lack of information, in addition to mothers’ low education, led to low coverage of immunisation. Nevertheless, Africans should be made aware that immunisation is a powerful public health strategy for improving child survival, not only by directly combating key diseases that kill children but by also providing a platform for other health services (Oyo-Ita et al., 2016).
In collectivistic African cultures, decision-making often happen within a family, and younger members look up to and respect the advice of elders (Ögtem-Young, 2018), particularly men. Primarily, husbands make decisions concerning their sick children. The culture is also practised by religious groups, for instance, the Apostolic Faith. Words, actions and the environment play major roles in inhibiting resilience in their children. Children, therefore, lack life skills and are even forced to marry older men who have many other wives. These forced marriages increase the spread of HIV/AIDS and trauma and exacerbates poverty, leading to helplessness. In the context of Botswana and elsewhere, previous researchers posited that African independent churches (one of the three groups of churches that exist in Botswana) were founded by Africans to enable them to worship in African ways (Mpofu et al., 2011). These churches, like the Apostolic Faith of God, do not believe in the use of modern medicine, and they practice rituals such as birth and death rites and also polygamy.
In addition to the rites, S/R beliefs can reinforce prejudice, discrimination and stigma (Ögtem-Young, 2018), which contribute to intolerance and severe violence. For instance, 8 out of 10 conflicts in Africa have a religious dimension (e.g., in Mali, Nigeria and Somalia; Basedau, 2017). In the Central African Republic (CAR), Muslim and Christian groups are intolerant of each other and commit human rights violations (Cadman, 2015). The violence started as political and later became religious. The Muslims and Christians murder members of each other’s religious sect as retaliatory killings. Homes have been burnt and about 500,000 people have been displaced. Children have been used in combat and women have been raped. The consequences of having children participate in wars, rape and murder is inconceivable. This is evidence that faith has a negative impact on children’s resilience when they kill each other for S/R beliefs, which they may not fully comprehend as children. However, calls for religious tolerance and condemnation of fanaticism from the international community have been loud. These CAR communities and elsewhere need resilience and help from the international community to get through these atrocities. Previous experience from the devastating effects of these wars could be an opportunity for the international community to learn from past mistakes and enhance cosmopolitanism, international law and human protection (Cadman, 2015). Nevertheless, it is vital to note that a survey revealed that most Africans are tolerant of S/R, ethnicity, nationality and HIV, but not homosexuality (Afrobarometer, 2016).
However, this article will not have done any justice to the topic if the impact of HIV and AIDS on adolescents’ resilience is not addressed.
The Impact of HIV/AIDS on Vulnerable Children’s Resilience in Sub-Saharan Africa
UNICEF has reported that although progress has been made in curbing the spread of HIV, the current state of the AIDS response in SSA does not suffice to eradicate contracting HIV and AIDS in children and adolescents, thereby increasing incidence of chronic illnesses among the children (UNICEF, 2017a). Adolescents are at a higher risk of contracting HIV, especially if lacking religious values that promote abstinence. Three in four new HIV infections in adolescents (aged 15–19 years) occur in sub-Saharan Africa, and for every five adolescent boys living with HIV, there are seven girls (aged 10–19 years) (UNICEF, 2017a). These statistics also prove the reality of gender-based violence in SSA as girls are more prone to infections. About, 43 per cent of the 2.1 million children living with HIV around the world had received ART (UNICEF, 2017a), suggesting 57 per cent are most likely living with chronic illness as they are not on medication.
UNICEF also posits that HIV services for prevention of mother-to-child transmission (PMTCT) have made one of the greatest public health achievements in recent years. However, there is need to have accurate statistics on the prevalence and incidence of PMTCT so that stakeholders may intervene efficaciously. For instance, Eastern and Southern Africa were found to have 50 per cent of new HIV infections in children (0–14 years) even though the regions had the highest proportion of pregnant women (88%) receiving antiretroviral drugs for PMTCT; PMTCT coverage in West and Central Africa was found to be at 49 per cent, accounting for 38 per cent of new infections in children and 25 per cent of all children living with HIV (UNICEF, 2017a). These statistics confirm that more still has to be done to reduce these figures. These statistics portray the need for stakeholders interested in the welfare of children to inculcate resilience in these vulnerable children for them to leave a normal life. In addition, uptake of ART for children who are not on ART (1.2 million), should be expedited to reduce incidence of chronic illnesses. Medication will also act as a protective factor and may enhance their QOL, hence resilience.
Nonetheless, trends for new HIV infections among older adolescents (aged 15–19 years) in Eastern and Southern Africa (21% decrease) is looking better than trends in Eastern Europe and Central Asia (27% increase). Despite the decrease, UNICEF reports that there have been 5.7 million new adolescent HIV infections since 2000, which is still ridiculously high, in our opinion, considering the unavailability of data for adolescents regarding treatment access and AIDS-related deaths, suggesting the need to improve measures on data collection and creative or innovative programmes that work towards curbing the new infections. In 2016, 41 countries were said to have reported decentralisation of adolescent treatment data and among these countries, the median ART coverage was said to be around 36 per cent (UNAIDS, 2017b), which is far from adequate.
The statistics above confirm the need for stakeholders interested in the welfare of children to address their S/R needs so as to reduce new adolescent infections in the region as a whole. Most religious groups discourage premarital sex and belonging to such religious groups will reduce the incidence rate.
Churches and FBOs can promote S/R as a resilience factor among children by highlighting vulnerable children’s realities and needs (Vinueza, 2016, 2017), thereafter try to address each and every need efficaciously. For instance, religious rituals like prayer, scripture reading, worship and meditation provide psychosocial support and may promote resilience. These practices can assist children to connect with the self, God and others as a community of believers. The connections usually foster motivation, optimism and best practices in interpreting change. S/R directly impact the children’s well-being by mediating the relationship between S/R and mental health and/or recovery (Cornah, 2006; Vinueza, 2017). Factors mediating the relationship between S/R and mental health will be discussed next.
Factors Mediating the Relationship Between S/R and Mental Health that Lead to Resilience in Children
Previous research has found that there is a positive correlation between church attendance and lower levels of depression among adults, children and young people (Brewer-Smyth & Koenig, 2014; Cornah, 2006; Vinueza, 2017). Additionally, previous researchers (Swinton, 2001) found that believing in a higher being was also correlated with reduced depressive symptoms. Further, children who have positive active relationships to spirituality were 40 per cent less likely to use and abuse substances, and had 60 per cent less depression than other teenagers (Vinueza, 2016). Associations between spirituality and anxiety or stress have also been found (Brewer-Smyth & Koenig, 2014). Quantitative research demonstrated reduced levels of anxiety in children who had chronic illnesses or had experienced traumatic events. Spirituality was found to have similar effects as yoga and meditation among believers. These studies show the mediating relationships between S/R and mental health that lead to resilience.
In one previous review, according to Cornah (2006), 11 studies reported correlations between religion, spirituality and trauma-based mental health problems. The three findings were as follows:
S/R usually benefit some people in dealing with the aftermath of trauma. Traumatic experiences can lead to a deepening of S/R. Positive religious coping, religious openness, readiness to face existential questions, religious participation and intrinsic religiousness are typically associated with improved post-traumatic recovery (Cornah, 2006, p. 18).
However, readers should take cognisance of the fact that increased mental health problems are often found amongst those with a strict religious upbringing; this depends on how S/R is expressed. For instance, certain children may realise that their S/R beliefs are not understood or explored within mental health services. For many, their spiritual life or beliefs may be ignored by clinicians or their spiritual experiences may be treated as nothing more than an indication of psychopathology.
Certain kinds of religious coping (i.e., coping styles, locus of control, social support and social networks and environment-spiritual buildings, for example, churches, temples or mosques) may help children conspire with a higher being (God) in coping with stress or trauma in order to deal with adversity. The following are excerpts from (Cornah, 2006) to express this point:
While I’ve been ill? … sometimes I find just going into a church … some churches have an aura … you can go and pray. I can always find that with [name of church] it has an atmosphere. (p. 30) God became a friend … everything, I discussed with God … [He] put up with loads … it’s how I survived. (p. 32)
The foregoing excerpts help to explain how certain research justify how religious communities can provide ‘protection by space and protection by presence’ (Vinueza, 2016, p. 9). ‘Protection by space’ was said to be the different ways places of worship can provide physical protection while ‘protection by presence’ relates to the way in which believing in a higher being (e.g., God) can provide therapy and recovery (Refugee Studies Centre, 2013). Additionally, religious beliefs contribute to building resilience because they help victims in adapting to new circumstances, cause optimism and motivation, see difficulties as challenges or gifts from God, regain control of their lives and recover from negative events (Refugee Studies Centre, 2013; Vinueza, 2017).
Consider another excerpt from Vinueza (2017, p. 92):
When migrants see such difficulties facing them and do not see any solution, spirituality allows them to ‘see’ more than what they have in front of them. The impossible becomes possible. This gives them the strength they need to continue fighting.
Thus, any action to benefit refugee children needs to start from a recognition of their innate value, worth and their positive capacities as creatures made in the image of God (Dillen, 2012, p. 71). The next section identifies implications for research, practice and policy.
Research, Practice and Policy Implications
Issues discussed in this article have far reaching implications for research, practice and policy. At research level, there is a need to conduct longitudinal studies that will explore over prolonged periods of time the processes and role of S/R in facilitating or inhibiting children’s adjustment to traumatic experiences. Such research should use the children themselves as active participants to understand how they feel. The research should also solicit the views of various stakeholders (e.g., pastors) in order to get a comprehensive picture of how effective the intervention is in building or inhibiting resilience. In addition, the research should utilise a wide range of data collection methods and also target children who have experienced multiple and diverse traumatic situations. Further, more research to better understand reluctance of immunisation uptake by some of these religious groups should also be done. Research that includes the strategies above would produce findings that would go a long way in informing the development of S/R models that take into account the unique needs of African children.
At a practice level, the findings on failure by children to access immunisation highlight the need for an ingenious multidisciplinary approach to defeat and overcome the barriers to childhood immunisation (Kriss et al., 2016; Mbengue et al., 2017) in sub-Saharan Africa. In addition, involving Apostolic and political leaders may improve interventions. Involving leaders at grassroots levels should help in eradicating top-down applications and practices (Ögtem-Young, 2018). Advocacy, particularly outreach programmes should be done in these communities with and without incentives to improve coverage. Immunisation can also be integrated with other services in LMIC, for instance, PMTCT programmes.
With regard to crime and man-made disasters, governments should work towards transforming community-level risks. The youths that were interviewed in South African studies mentioned legislation, the provision of services, addressing poverty, altruism and building community cohesion, which can be done through S/R. SSA countries can adopt events like those hosted by the Sardovaya organisation in Sri Lanka to build resilience at village, district and national levels; the organisation starts with non-denominational meditation followed by prayers that represent the available religions in their communities, inclusive of Christians, Buddhists, Muslims and Hindus (Refugee Studies Centre, 2013).
Communities may also come up with different ways to optimise use of protective factors available in their communities as a starting point inclusive of S/R. International mechanisms (e.g., financial support to courts) can help to collectively address situations of fanaticism and religious violence. The development of new rules and exemplars to fight against impunity and protect citizens from future massacres (Cadman, 2015) may also assist in building resilience in victims and their families.
In addition, stakeholders working with children should provide prevention and intervention efforts designed to promote children’s resilience. The health fraternity could benefit from the knowledge that a spiritual coping model could help patients heal particularly from chronic stress (Counted et al., 2018). However, a spiritual coping model alone is not sufficient to eradicate HIV even though it reduces new infections. To enhance resilience among the children, programmes should focus on a combination of prevention efforts, inclusive of the biomedical treatment for the infected, behavioural changes to maintain abstinence and prevent new infections or reinfections, HIV self-testing, pre-exposure prophylaxis, male circumcision, use of condoms and eradicating gender-based violence (UNICEF, 2017a).
At a policy level, there is a need for countries in SSA to emphasise policies that encourage collaboration between the religious fraternity, traditional leaders and other stakeholders. Involving traditional leaders is crucial because S/R in many African countries is closely linked to African traditional beliefs and practices. In addition, policymakers and governments should be well informed so as to incorporate multiple factors and manifestations of resilience when formulating policies for better outcomes. Results from previous studies also reinforced the need to develop trauma-informed practice protocols that incorporate S/R, which can be designed by Chaplains or spiritual care providers (Hipolito et al., 2014). The fact that children are at a higher risk for encountering challenges that may build or inhibit their resilience because of lack of protective factors requires explicit and specific attention to health policies and programmes. If implemented, low resilience and prevention of chronic problems among children may be immensely reduced.
Conclusion
To summarise the above, S/R plays a pivotal role in building resilience in children. Children’s faith (S/R) also functions as a powerful protective factor in some cultures. Previous research and literature has constantly shown a high positive correlation between S/R, mental and physical health and resilience (Mhaka-Mutepfa, 2018). When seeking mental health services, pastors are the first port of call, with more than 40 per cent seeking pastoral counselling rather than mental health providers (personal communication, pastor). S/R beliefs may allow a child to reframe or reinterpret events that are seen as uncontrollable, in such a way as to make them less stressful or more meaningful (Cornah, 2006; Ungar, 2014). Furthermore, emotions encouraged in most spiritual traditions, for example, hope, contentment, love and forgiveness, may improve children’s well-being and resilience. Thus, just like other forms of social support, spiritual or religious support is an invaluable source of self-esteem, knowledge, camaraderie and pragmatic assistance that enables children to cope with stress and trauma and achieve high resilience. However, despite the widely recognised positive aspects of S/R, there are still gaps in scientific knowledge of the progressive processes of S/R in resilience. More research is needed to explain these dynamic processes (Vinueza, 2016, p. 16).
S/R resources including prayer, meditation, church services and religious activities, and believing in the power of God help people, including children, cope with adversities. Adversities include death of parents, poverty, chronic stress, chronic illnesses, violence, disasters and others. Previous research highlighted the utility of S/R in physical and mental health and well-being among SSA people living with HIV/AIDS that should be taken into consideration in providing a caring and healthy environment. S/R groups were also found to reduce new infections from HIV among adolescents as they preached abstinence, thereby increasing resilience. S/R also influences the way children perceive health and disease and how they interact with other people. In SSA, many people still believe and belong to S/R institutions and religious plurality is common.
In previous studies, S/R were found to promote or inhibit resilience. Caregivers should empower children and use S/R to promote resilience. The role of S/R that have a negative impact on resilience should be fazed through education and informed consent. A multidisciplinary approach is, therefore, required to build resilience in children particularly in African societies since the region has more vulnerable and disadvantaged children than their counterparts because of poor economies and bad governance. All stakeholders interested in the welfare of children should play an active role in building resilience in children for them to experience a better QOL.
In addition to basic needs, children need safety, love and trust, hope and autonomy which all lead to resilience. These qualities are encouraged among religious communities since people tend to work together to create harmony and group cohesion is extremely valued. People are considered ‘good’ when they are generous and tend to the needs of others, thereby inculcating resilience.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.