
Abstract
This study aims to explore how non-governmental organisations (NGOs) generate certain components of social capital through the provision of healthcare. Two NGOs, the Development Association for Self-reliance Communities and Health (DASCOH) and the renowned American charity, Cooperative for Assistance and Relief Everywhere (CARE), were selected to examine their healthcare services in two villages in the Sunamganj District of Bangladesh. This research employed a multi-method qualitative data collection procedure, including in-depth interviews, focus group discussions and key informant interviews. Results showed that, despite structural limitations, NGOs’ health services have made important strides towards the improvement in haor residents’ well-being, particularly during the endemic floods that hit the area every year. The activities of NGOs contributed to three essential elements of social capital: (a) the organisation of community participation, (b) the establishment of networks between service providers and patients and (c) the building of trust between NGOs and communities. The findings of this research can be useful to policymakers, development practitioners, health workers and NGO managers for designing and developing haor community development activities.
Introduction
Health is a basic human need that transcends gender, race, religion and nationality. Although health is a worldwide public benefit, most developing countries such as Bangladesh still struggle to avail it for its populations owing to a lack of resources. The country’s deprived people, notably the haor people, have little or no means to satisfy their healthcare requirements. Bangladesh is a developing country in the South Asian region, covering about 1.99 million hectares (19,998 sq. km). About 19.37 million of its people live in the haor area which is highly vulnerable to the impacts of climate change (GoB, 2012). Flash floods are common in the haor basin, posing a serious health risks to its residents. Despite the availability of huge resources, the haor basin is identified as a high food insecure locality and hotspots of poverty in Bangladesh. Poverty creates other problems like malnutrition (Mia, 2021). The haor is overwhelmed with huge problems such as flash floods, poverty, extreme dependency on natural resources, lack of alternative sources of income, inadequate health facilities and sanitary latrines, scarcity of potable water, poor road connectivity, the insufficient and flimsy infrastructure of educational institutions (Alam & Hasan, 2010). The haor people are isolated in a rural area, as their transportation to the cities is hampered by poor roads, which are easily rendered inaccessible due to floods. Bangladesh’s health service is managed by district hospitals located in district capitals. However, for haor people, even a trip to their district capital is difficult and often impossible, thus restricting their accessibility to the state’s health services, especially when they are most needed, such as after floods. Consequently, non-governmental organisations (NGOs) have tried to fill this gap by prioritising healthcare services for the haor people. A significant number of studies (EI Arifeen et al, 2013; Mercer et al., 2004; DGHS, 2012; Save the Children, 2011) have focused on NGOs’ health services in Bangladesh, yet none of these studies has investigated their roles in the creation of social capital for their clients. Hence, the objective of this study is to explore how NGOs generate certain components of social capital through the provision of healthcare, thereby improving the health condition of the haor people in Bangladesh. To this end, we evaluated the healthcare initiatives of two NGOs in two villages in the Tahirpur Upazila, in the Sunamganj District of Bangladesh. This study focused on the three elements of social capital: norms, networks and trust, and then explained how they work in the healthcare service delivery of NGOs. Our discussion and conclusions are backed by the theory of social capital discussed later in this article.
Haor People’s Access to Healthcare
A haor is a kind of wetland ecosystem, with a vast, bowl-shaped floodplain depression located in Bangladesh’s north-eastern area (Haque et al., 2022). It is comparable to swampland in that it has a low-lying river basin region. After the monsoon, the haor is submerged for about six months of the year. Haors cover a total area of about 8,59,000 hectares, which is around 43% of the total area of the haor districts and approximately 17% of the country’s land area (GoB, 2012). The extreme seasonality of the haor economy forces the local people to remain unwaged for a considerable period; thus, they often suffer poverty and hardships. The haor economy depends on mono-crop cultivation of Boro rice during the winter period. Yet, unseasonably early flash floods often sweep away the standing crops, resulting in the loss of people’s harvest and potential income. During the wet season, the haor region goes underwater, eliminating all alternative means of survival and eliciting an acute shortage of food. The extreme level of poverty results in poor health and a desperate need for healthcare, which is scarce in the region.
Haor regions experience excessive hydrological conditions, such as extreme rainfall and resultant flash floods (Nowreen et al., 2015). Sudden flash floods not only wash away their crops and properties but also destroy their houses, sources of drinking water and sanitary systems. These hardcore poor lack resources to rebuild their homes and sanitary systems or set up tube wells for safe drinking water within a short time. Due to the lack of materials, appropriate technology and space for the construction of toilets, they often remain without sanitary latrines. According to Sharma (2010), only 11% of the households in this region have hygienic latrines, 69% have unhygienic latrines and 20% defecate in the open. Haque et al. (2016) showed that 61% of the mothers are ignorant of the availability of maternal healthcare, 36% received antenatal care (ANC), 47% sought ANC from government institutions and 95% delivered at home with the assistance of untrained birth attendants. Adequate maternal healthcare practices are crucial to both maternal and infant nutrition outcomes. The haor region of Bangladesh is vulnerable and performs poorly, as maternal and child health indicators are falling behind compared to other areas (Haque et al., 2022). In haor areas, lack of resources, extreme weather conditions and parents’ social norms underlie the high mortality rates both for mothers and their children (Chakraborty et al., 2020). Bangladesh is one of ten countries that accounts for nearly 60% of the global burden of maternal mortality. Although the maternal mortality ratio (MMR) in Bangladesh declined by 40% from 322 per 1,00,000 live births in 2001 to 176 per 1,00,00 live births in 2015 almost achieving the target for MDG-5: Millennium Development Goal (MDG) (Improve maternal health), the burden of direct obstetric care deaths in the country remains high, comprising almost two-thirds of maternal deaths in Bangladesh (Moinuddin et al., 2017). Uddin et al. (2009) argued that immunisation coverage is very low in haor areas due to irregular/cancelled/extended programmes of immunisation (EPI). Immunisation staff are often absent in the villages, and the government has no alternative strategies for remote areas. Geographical barriers, poor road conditions and the lack of transportation make it difficult to reach the health facility and contribute to low levels of utilisation of skilled care during and after childbirth. Compounding these challenges is also a shortage of health service providers in these regions (Moinuddin et al., 2017). During floods, haor people are afflicted with many waterborne diseases, causing health complications, such as fever, pneumonia, malaria, stomach pain, cough, diarrhoea, dysentery, gastrointestinal illness and night-blindness (IUCN, 2010). All these occur at a time when floods have disrupted transportation, and people are unable to access medical services.
NGOs’ Healthcare Initiatives in Haor Communities
The term ‘non-governmental organizations’ (NGOs) denotes an entity that is formed by a group of people working independently of the state, with the aim of serving the common people (Islam, 2019; Islam & Morgan, 2012; Piotrowicz & Cianciara, 2013). They are neither a part of the government nor run to make profits (Islam & Morgan, 2015). The target populations of NGOs are poor and disadvantaged people. NGOs offer a wide range of services that are fundamental to people’s survival, including credit, education, health, agricultural extension and sanitation (Rabby, 2012; Uddin, 2011). In Bangladesh, NGOs concentrate on addressing poverty, unemployment, malnutrition, health, education and natural disasters (Hossain et al., 2023; Islam, 2019; Islam & Morgan, 2012). They started with relief activities after the independence of Bangladesh and subsequently undertook development activities (Hossain et al., 2023) and thus making them active agents in the economic development of Bangladesh.
Among the major NGOs working in the haor areas are International Union for Conservation of Nature (IUCN), Center for Natural Resource Studies (CNRS), DASCOH, CARE, NGO Forum, Water Aid, etc. Environmental protection, maternal and child health, water, sanitation and hygiene, education and biodiversity are the primary foci of these NGOs’ interventions. The main tasks of NGOs in the healthcare system are providing health services and community health advocacy. Mothers’ assembly is held in the community to raise awareness about maternal and child health and nutrition. With support from NGOs, women meet in the courtyard and learned about pregnancy, safe delivery, and danger signs, maternity and neonatal health services provided in a variety of health facilities (Hossain et al., 2023; Matin et al., 2023). In addition, household visits by community health workers (CHWs) to provide antenatal counselling, delivery advice and referral help for difficulties, including sick children, to reach rural target people in the haor (Matin et al., 2023). Services provided range from medical, social and psychological intervention to integration activities, care and nursing, material and financial support, educational and information services and training and skills development. Many studies demonstrated that NGOs could play an important role in delivery of healthcare services to mothers (Haque et al., 2022). Moreover, a study showed that visits by NGO health professionals, the Household Food Insecurity Access Scale (HFIAS) and women’s empowerment have significant effect on domestic violence (Haque et al., 2016). Based on the data reported by 27 partner NGOs from 1996 to 2002, Mercer et al. (2004) found that child and maternal mortality is relatively low in areas where the NGOs are working. In support of this argument, Ahmed et al. (2006) identified four major barriers to access to NGO healthcare services, namely low income, lack of awareness about the kind of services, deficiencies and inconsistencies in the quality of services and lack of proximity to the healthcare facility.
Social Capital: A Model for Healthcare Interventions of NGOs in Bangladesh
The term ‘social capital’ refers to an entity comprised of various aspects of social structures and facilitating specific actions within the structure. Social capital is a kind of resource that promotes community development through coordinated action. Bourdieu is commonly recognised as an early proponent of social capital who said:
social capital is the sum of resources, actual or virtual, that accrue to an individual or a group by virtue of possessing a durable network of more or less institutionalized relationships of mutual acquaintance and recognition. (Bourdieu & Wacquant, 1992, p. 8).
Coleman (1988) identified social capital as a type of resource, as it involves the reciprocity of individual and wider networks of relationships that are bound by a high degree of trust and shared values. Social capital could be an asset for the disadvantaged communities and not just an instrument of privilege. Social capital is a significant apparatus that has huge social implications in the community (Islam, 2017). Community members can benefit in a variety of ways from utilising social capital elements. As an instance, the adoption of social capital elements fosters the norms of reciprocity, accelerates the flow of information and develops mutual trust among the participants, which act as a foundation for future cooperation. Putnam (1993) argued that people who have a dense network of social interaction can lobby more effectively for medical services. If people wish to change their behaviour and adopt a healthy lifestyle, they tend to emulate people in their trusted network (Buckland, 1998). People in well-connected communities are well positioned to influence local health services due to their better awareness of the services, resulting in their improved access to the services (Hendryx et al., 2002). The shared objective among individuals is essential for communities and individuals because it stretches a universal sense of tackling social disasters like the impacts of flooding on health and health systems. Further, solidarity creates a bond between individuals, both in intimate relationships (primary groups) and voluntary associations (secondary groups), making it possible to achieve a variety of other social goals (Putnam, 1993). Family, friends and neighbours are part of primary groups, whereas fraternal lodges and civic organisations are part of secondary groups. Interaction among the primary groups supported by secondary groups creates communication pathways, predictable positive outcomes and the potential for trust (Litwak et al., 1989).
Several studies have shown that social capital has significant implications for people’s community healthcare. Stephens (2008) found that a positive relationship exists between social capital and health. Ogden et al. (2013) revealed that social capital strengthens health policy and programmes through advocacy, participatory policy analysis and governance. They argued that this happens by creating bonds within communities, connecting communities and linking communities to health and other social system decision-makers. By drawing on a case study from Gujarat state in India, Mekonnen et al. (2015) explored the significance of social capital for the integration of Health Information Systems (HISs) and health outcomes. Individuals with higher social participation may be more engaged in community-based efforts to improve government health services and, therefore, may be more inclined to use them. Based on the linking social capital framework, Musinguzi et al. (2017) examined the claim that village health teams (VHTs), as an example of CHWs, link and connect communities with formal healthcare services. Grootaert (1998) found that social capital was initiated to increase health, education, agricultural extension and water supply facilities in the community. Jamil and Muriisa (2004) explored the process by which social capital is created and sustained to cope with HIV/AIDS challenges in Uganda. A good number of studies (e.g., Abom, 2004; Dowla, 2006; Islam, 2015, 2017; Islam & Morgan, 2012; Jianxiu, 2006; Mondal, 2000) have highlighted the social capital initiatives of NGOs towards community development. Involvement in civic organisations boosts the capacity of community residents to identify the health needs of the community through their initiatives. These initiatives increase the sense of perceived self-efficacy and confidence of the community members to tackle their problems collectively (Uddin et al., 2009; Ulleberg, 2009).
The literature on NGO social capital initiatives towards the rural poor and disadvantaged people is scarce. To the author’s knowledge, no single study has focused on NGOs’ social capital initiatives towards the healthcare of the haor people in Bangladesh. Therefore, this study attempts to expound on the healthcare initiatives of NGOs in rural areas through the lens of social capital.
Objectives
The general objective of the study was to know the healthcare services of the NGOs in the haor communities through the lens of social capital. However, the specific objectives of the study were:
To explore the role of NGOs in fostering cooperation and facilitating collective action among haor communities in Bangladesh. To understand the effectiveness of NGO interventions in improving healthcare access and strengthening information networks in haor regions. To discover the strategies utilised by NGOs to build trust and maintain engagement with haor communities in Bangladesh.
Materials and Methods
Haors with their unique hydro-ecological features are large bowl-shaped floodplain depressions located in the North-Eastern region of Bangladesh. There are almost 373 haors located in the districts of Sunamganj, Habiganj, Netrokona, Kishoreganj, Sylhet, Moulvibazar and Brahmanbaria. Among the haor area of these seven districts, Sunamganj has the largest haor area of 2,68,531 ha which is about 73% of the total area of the district (CEGIS, 2012). The study was conducted in the Sunamgonj District of Bangladesh to evaluate the healthcare initiatives of NGOs in the haor areas. Tanguar haor, one of the largest haor in the area which spans about 100 square kilometres (39 sq mi) of which 2,802.36 ha, is wetland. It is the source of livelihood for more than 40,000 people (Haque et al., 2022).
A qualitative case study approach was undertaken to get a better understanding of the healthcare role of NGOs through the lens of social capital. We purposively selected two NGOs, namely CARE Bangladesh and the DASCOH, as they have been providing healthcare services to the rural poor in haor areas. We purposively selected two villages—Joypur (Uttar Sreepur Union) and Lamagaon (Dakshin Sreepur Union) of Thahirpur Upazila, District of Sunamganj—given their remoteness and the prominent role of these two NGOs in providing community-based healthcare services in that area. These villages (Lamagaon and Joypur) are also the success cases of the NGOs, CARE and DASCOH respectively. We recruited two research assistants, male and female, considering the social and cultural background of rural Bangladesh, and imparted the necessary training before going to the field for data collection.
Table 1 shows the details of research participants and data collection techniques.
Research Participants and Data Collection Techniques.
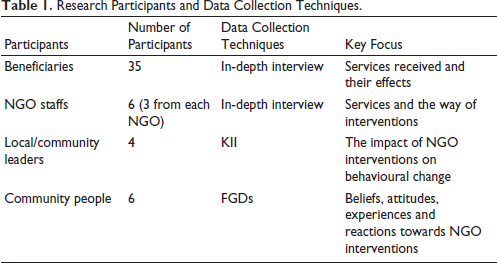
We gleaned data from a range of participants, including beneficiaries, NGO staffs and volunteers involved in delivering healthcare, officials from the health department of the central government and local representatives of the haor community. For the collection of data, we conducted in-depth interviews with the beneficiaries of the two NGOs operating in the two villages; focus group discussions (FGDs) with male and female members of different ages from the selected villages; and key informant interviews (KIIs) with the chairman and members of the Union Parishad, school teachers, NGO staff and volunteers. We formulated separate sets of interview guidelines for the collection of data from participants of different strata. We also took observation notes to substantiate the data gleaned from research participants by employing different techniques of data collection.
We classified, organised and set the pattern of data according to research objectives. A thematic analysis was conducted to identify, analyse and interpret patterns of meaning in the data. The data was triangulated to increase the reliability and validity of the study. We presented the data to a small group of residents and NGO staff for review and recommendations. The major themes identified in this study include establishing social norms and promoting cooperation, strengthening information networks and improving access to healthcare, and enhancing trust between NGOs and local communities.
Ethical Issues
The ethical guidelines for qualitative research were followed throughout the study, and information taken from different sources of existing knowledge was properly acknowledged. Verbal consent was taken from the participants before conducting interviews. To maintain the confidentiality of the information and identity of the participants, all data were anonymised. It was made clear to the participants that they are flexible to refuse to answer or withdraw participation at any point if they felt uncomfortable. Besides, pseudonyms were used to maintain the confidentiality of the participants. A guarantee of confidentiality and anonymity of sources was provided to the authorities of DASCOH and CARE.
Results
Creating Norms and Fostering Cooperation
The rural people have an excellent sense of collaboration, which is often less utilised due to the lack of proper mobilisation capacities and motivation. Several NGOs are working in the haor areas, providing special programmes intended for the development of the community. DASCOH arranges Uthan Boithok (group meeting in the home yard) to create health awareness. They counsel pregnant women on nutrient-rich foods and maternal health issues. By organising meetings in the home yards of local people, the NGOs allow their voices to be heard, which instil a sense of cooperation among the target group. Courtyard meetings conducted by community-based health workers were used as the main platform for dialoguing with the community to discuss the rights and needs of women related to maternal and child health. During FGD, a female respondent explained DASCOH services as follows:
NGO-Apa (sister) (NGO field workers) arranges meetings in our Para (community). They teach us about maternal care, risk factors during pregnancy, hygiene, and so on. We now understand the importance of nutrient-rich foods for pregnant women, but we lack the funds to purchase nourishing foods, and there are no vegetables or nutritious foods available in local markets.
NGOs in the haor areas arrange meetings at regular intervals in the community where all the people gather in a yard, which is called a ‘home-yard meeting’. The main objective of this meeting is to create space for community voice and encourage a forum for sharing views, opinions, wishes and concerns about the development programmes run by the NGOs. These meetings explore different health-related issues to create awareness among the community people, thereby enabling them to take the appropriate measures to overcome the health risks and challenges. As explained by an NGO worker, the gathering of people in a regular meeting gives an impetus to collective actions and infuses the norms of cooperation.
By bringing all women to a meeting, NGOs have been able to develop a certain level of reciprocity and thereby foster the norms of cooperation among the participants. During the meeting, they share every information and use the acquired knowledge when necessary to solve their problems.
They also advise pregnant women to take nutritious foods to maintain their health. One of the participants has mentioned the benefits of yard meetings as follows:
NGOs call all community women to yard meetings to discuss health-related issues. Once, we felt shy about being in front of many people. Now, we learn a lot of health-related issues. We talk to each other and share our opinions. Everybody is cooperative in helping each other if the necessity arises. NGOs teach us to get our problems solved together. We are here for each other. […]
This is just one of the remarkable experiences of a woman who participated in a community meeting arranged by the NGOs to enlighten them about health-related issues. The programmes and activities of NGOs are different from each other. Although they generally deliver services to people, irrespective of their gender, some services are exclusively for women. Nevertheless, male members of the community impart training for future preparedness and development of crisis-coping capacity. As mentioned earlier, rural people already have social capital in the forms of cooperation, reciprocity and personal networks, all of which facilitate cooperation in problem-solving. However, NGOs play a catalytic role in fostering the existing base of social capital by integrating local people to solve their problems through their collective actions. The basis of cooperation was primarily at the individual level, but NGOs’ interventions have helped to move the wheels of relationships ahead in the spirit of achieving common objectives with the rural community living in the haor basin.
Information Network and Access to Healthcare
Haor areas are characterised by inadequate infrastructure, poor communication networks and slow economic progress because of their physical and geographical features. These, coupled with lack of healthcare centres, health specialists and medicine, have put people at a health risk. In this situation, the arrival of NGOs was a godsend to the rural people. Access to necessary healthcare and related services was impossible for haor residents before the appearance of NGOs in the community. Nowadays, NGOs are working with a large section of the haor population to create health awareness and impart training to local village doctors and midwives. It was observed that haor people, especially the women, regularly visit the local health centres for medical care and necessary information, particularly about maternal and child care, food and nutrition and common diseases and their symptoms. NGOs have brought a wider community under the coverage of their programmes and established a connection between them and the community, towards the visionary objective of ensuring health for all. The vast majority of haor people are illiterate and poor, and are thus unable to afford even the lowest cost of modern healthcare facilities. Also, they cannot get proper treatment and healthcare advice due to inadequate public transport between their villages and the Upazila Health Complex (UHC), where all central government health services are provided. NGOs have turned the tide for the haor folks by bringing healthcare services to their doorsteps. In this regard, one of the participants said:
Earlier, only the rich people could visit doctors, as the poor could not afford medical treatment. Now, we have the opportunity to see doctors and receive treatment here in our village.
Building Trust Between NGOs and the Communities
The haor community is an underprivileged community, especially in terms of access to modern healthcare facilities. As a remote community, they are deprived of most of the public health services. NGOs have succeeded in bridging this gap by delivering services that promote healthcare. During a KII, a participant said:
At the very outset of the program, community members were unwilling to welcome NGOs into their community and were also dubious about the intention of the NGO’s voluntary services. Rural people do not want to talk to outsiders, and thus, they have some degree of confusion about the motives of NGO services being free of cost. Subsequently, the programs gained wider acceptance and recognition due to the regular activities of NGOs that integrate the local people into different social, motivational and awareness-raising programs arranged in the home yards of community members.
NGOs’ roles are crucial in organising the community and making them understand their healthcare needs for improved well-being. Different sections of the population are invited to join the programmes aimed at providing them with knowledge and educative information that promote collective management of their problems. The experiences of NGO health workers indicate that they encountered a lot of challenges in reaching and offering services to the targeted groups. As an instance, women were found to exhibit negative attitudes when counselled by female health workers on family planning methods. However, the situation improved over time, with women beginning to adopt contraceptives and other family planning methods.
Additionally, the NGO initiative to mobilise local people by organising joint meetings involving different stakeholders has built a basis of trust between community people and NGO workers. A few years ago, the concept of nutrition was alien to many of the local people. However, following DASCOH’s awareness and health promotion efforts, nutrition has become one of the building blocks on which improved health in the haor area was built on. The NGOs also provide training to school teachers from the community on nutrition and arrange parent–guardian meetings. Subsequently, teachers also disseminate nutritional information to their students, which leads to reduced malnutrition. In these ways, the people of the haor communities have changed their diets over time.
When educated local people become involved in the healthcare programmes run by the NGOs, the rest of the community develops positive attitudes towards the programmes. NGOs also play a major role in building trust by providing group-based services like water and sanitary facilities, with every member of the group also contributing to the cost. One of the NGO facilitators said:
Through our programs, we have developed reciprocal relationships with the community. Whenever they face any health-related problems, they come to us for aid and advice instead of going to public healthcare providers. We make every effort to provide the best possible service to the people. We develop a sense of cooperation among the people for their collective development by engaging them in group-based work like constructing tube wells for safe drinking water.
Trust-building is a major building block in community development, and through it, NGOs have been able to involve community people in healthcare programmes. One of the participants stated:
At first, we did not accept NGOs as good actors. When they offered awareness-raising programs and provided us with information that we found beneficial for our lives, our perception changed. Over time, people have become much more dependent on NGO services. Our doubts about NGOs withered away as we got benefits from them. Now we have learned a lot from them.
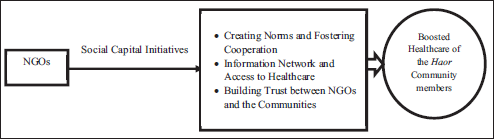
A graphical presentation regarding NGOs’ social capital initiatives towards healthcare has been illustrated below (Figure 1).
NGOs’ Social Capital Initiatives Towards Healthcare.
Discussion
This study examines the healthcare services provided by NGOs in Bangladesh’s haor communities through the lens of social capital. The findings highlight that NGOs play a crucial role in fostering cooperation through targeted interventions in haor communities, which facilitate dialogue and decision-making, particularly in maternal and child health awareness. Regular meetings of NGO officials with community people reinforce community norms, strengthening community empowerment. While NGO programmes primarily target women, male involvement in crisis preparedness fosters broader community resilience. Consistent with these findings, existing literature suggests that NGOs can foster social capital, improving community well-being by increasing community engagement (Ali et al., 2014, 2016). Nevertheless, gaps in health literacy persist, particularly regarding prenatal care, nutrition, and maternal medication, limiting community members’ ability to make informed health decisions (Nawabi et al., 2021). NGOs in haor regions are addressing these knowledge deficits and mitigating health risks for mothers and infants through increasing information network. Studies emphasise NGOs’ indispensable role in providing healthcare services, particularly for impoverished populations in these areas (Chakraborty et al., 2020; Islam, 2014a, 2014). However, scholars have raised concerns regarding the extent of NGOs’ effectiveness in developing social capital through creating norms and enhancing cooperation among community people. Islam and Morgan (2012) argue that NGOs’ capacity for enhancing norms and cooperation as component of social capital development varies based on the contextual variations. In developed contexts, norms and cooperation development often relies on formal institutions, general moral obligations and trust in legal systems (Greif & Tabellini, 2010). In contrast, developing societies depend on informal networks, family ties and community-based cooperation (Elsner & Schwardt, 2015). This study finds that gathering of people during NGO interventions gives an impetus to people to collective actions and develop a certain level of reciprocity and thereby foster the norms and cooperation among the participants. furthermore, Rodríguez-Carmona (2004) warns that traditional NGO interventions may not adequately strengthen local institutions or ensure long-term sustainability. Furthermore, Jung and Moon (2007) emphasise that irregular flow of development aid may create unfavourable conditions, potentially diminishing community engagement. Addressing these concerns requires NGOs to adopt context-sensitive, participatory and locally-driven approaches to effectively contribute to social capital development through community engagement and empowerment (Hossain et al., 2012).
Information networks play a crucial role in developing social capital in rural areas. Stern and Adams (2010) explained Internet usage as a strategy for creating social networks, contributing to community attachment and social capital building. Townsend et al. (2016) also argued that online networking is particularly useful for developing social capital in rural areas, increasing face-to-face interactions. In addition, NGOs can play an important role in developing support network and enhancing access to healthcare services particularly in developing countries (Ibrahim, 2017; Rahman et al., 2019). For example, NGO-led information and education programmes like Uthan Boithok have developed networks among people while enhancing healthcare-seeking behaviours during illness in haor areas. Local NGO health centres foster community participation in health management (Ui et al., 2010) and strengthen social connectedness (DeMello et al., 2020). However, in the absence of government support, NGOs’ networking, outreach and relationship-building efforts may be disrupted (Contreras & Niles, 2022). Castillo (2023) reveals that rural communities face challenges in maintaining effective networks due to urbanisation, globalisation and technological changes. This study further explores that geographical remoteness and inadequate transportation infrastructure significantly hinder their activities. Seasonal flooding isolates haor communities for nearly half the year, exacerbating their vulnerabilities. In response, health NGOs have not only tackled these challenges but also addressed informational asymmetry by leveraging intra- and extra-community networks to disseminate health knowledge (Hakim et al., 2022; Islam, 2014a). While NGO initiatives have contributed to improved health outcomes, substantial investment in region-specific infrastructure and logistical challenges remains necessary for sustainable impact (Hossain et al., 2023).
Trust-building is another fundamental component of social capital development and a crucial determinant of NGO success. The effectiveness of NGO interventions hinges on their ability to cultivate trust within communities, allowing for expanded programme reach and sustainable healthcare delivery (Haque et al., 2022; Islam, 2014). Despite their successes, NGO health initiatives face notable limitations (Choudhury et al., 2016). In haor areas, scepticism and mistrust have posed barriers to NGO acceptance. Initially, community members questioned the intentions behind NGO-led voluntary services, often perceiving these organisations as external entities disconnected from local realities. Over time, sustained engagement through awareness-raising and health initiatives has facilitated broader acceptance and recognition among community members. Bháird (2013) underscores that sociocultural differences between NGO staff and local communities can create communication barriers and resistance. Solomon et al. (2008) think that these barriers and resistance can be mitigated through participatory approaches and trust-building efforts.
Strengths and Limitations of This Research and the NGO Health Projects in the Haor Area
The existing evidence suggests that the NGOs’ social capital initiatives towards the healthcare of the haor (wetland) community are a pioneering, successful development intervention in Bangladesh. The study unveiled the NGOs’ role in enhancing the information network and community access to healthcare services, creating norms, fostering cooperation and building trust between NGOs and the communities. The greatest strength of this study was clarifying and highlighting the importance of community partnerships in development intervention, making it a pioneering research initiative in Bangladesh. Another strength of the study was the diversity of the participants, which ensured a richness of data. The results are generalisable to other parts of the country with similar levels of terrain and socioeconomic deprivation. This data will help policymakers and NGO authorities construct policies and programmes for the betterment of these beneficiaries and similarly poor and isolated people.
However, this study had some limitations. The first limitation was that the participants were limited and not nationally representative; due to financial constraint, the researchers selected only two NGOs for the study. Moreover, the data collection was limited due to the lack of transport infrastructure to go anywhere at any time. Thus, the findings cannot be implicated to the entire Bangladesh. It is crucial to research diverse perceptions in order to obtain authentic data to guide the framing of robust policies, legislation and approaches to cater to the real scenario in haor areas. Hence, we encourage others to investigate our findings to include more diverse and a larger sample size of haor areas in Bangladesh. In addition, it would have been better to gather data from all the NGOs in the area.
Conclusion and Policy Implications
NGOs in haor areas play a pivotal role in social capital development by fostering cooperation, enhancing networks and building trust among the haor communities. By introducing targeted interventions, NGOs address their healthcare challenges. Through home-yard meetings, nutritional counselling and awareness campaigns, NGOs have empowered women and other vulnerable groups to participate actively in healthcare initiatives. These activities have not only improved maternal and child health but have also instilled norms of reciprocity and cooperation. However, the lack of infrastructure and economic barriers in haor areas previously restricted access to modern healthcare services. NGOs are delivering health services directly to the community and training local health workers. Thus, they are playing the role as facilitators of information networks, enhancing health literacy needed for better health practices. Furthermore, the trust-building efforts of NGOs have been instrumental in overcoming initial disbelief within the community. By integrating local stakeholders into their regular activities, NGOs have earned the confidence of the haor people, strengthening collaboration and creating a favourable ambience for community-driven development.
The findings reveal the significant role of community-based programmes like Uthan Boithok in mobilising rural communities, fostering cooperation and addressing healthcare challenges in the Haor areas. The institutionalisation of these programmes would be more effective to foster collective problem-solving. These initiatives could be used as part of national health strategies to empower grassroots-level actions. Promoting public–private partnerships (PPPs) is essential to integrate NGO-led programmes into government healthcare systems. This collaboration would enhance the reach of health services, leveraging the trust and expertise NGOs have developed within communities. NGO-led engagement strategies are playing crucial role in improving the credibility and utilisation of public healthcare services. Expanding these strategies for community-based health workers, including midwives and doctors in community clinics, can ensure capacity building and effective knowledge dissemination within rural areas. However, removing barriers, especially infrastructural and economic barriers, is vital for better health access and complementing NGO efforts.
Footnotes
Acknowledgements
The authors are thankful to all participants and the local administration for their unconditional support while conducting this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research project was supported by the University Grants Commission (UGC) of Bangladesh.