
Abstract
The older people in Bangladesh’s tea gardens live in impoverished conditions, lacking access to public services and isolated from the mainstream population, which makes them vulnerable to poor physical and mental health. The present study aimed to explore the health risks of elderly individuals residing in tea plantations during the COVID-19 pandemic. Based on in-depth interviews and focus group discussions (FGDs), the study highlighted that the imposition of lockdown and social distancing measures reduces family income and purchasing capacity, disrupts the food supply chain, reduces their food intake, increases the habit of alcohol consumption, limits their access to healthcare professionals and thereby exacerbating the health vulnerability of older people in the tea gardens of Bangladesh. The study called for joint efforts by the government, civil society, social service agencies and non-governmental organisations (NGOs) to expand the social safety net in the tea gardens and initiate pragmatic measures to ensure healthcare for the tea gardeners.
Introduction
British rulers established the tea industry in Bangladesh during the colonial period in 1854. 1 They brought unskilled labourers from various regions of India, primarily from Bihar, Orissa, Madras, Andhra Pradesh, Madhya Pradesh, West Bengal and Uttar Pradesh, where hunger, unemployment and extreme poverty were common (Banglapedia, 2014; Jalil & Gauala, 2024). In Bangladesh, 87,534 registered and 20,065 non-registered tea workers are employed in 163 tea estates. The elderly individuals in the tea plantations of Bangladesh differ from the local population in terms of race, culture, language, religion and lifestyle. These distinct features create vulnerability and deprivation in their current living pattern, including isolation, exploitation and disadvantage (Al-Amin et al., 2017).
Tea garden workers are categorised into permanent and temporary based on their employment status. Permanent workers, referred to as registered workers, receive a range of benefits, including educational facilities for their children, housing, healthcare, weekly rations, leased land and festival bonuses. In contrast, temporary workers, who are known as casual or unregistered workers, earn lower wages and do not have access to the benefits provided to permanent workers (Al-Amin & Islam, 2020; Biswas et al., 2020; Islam & Al-Amin, 2019). A temporary worker can attain permanent status when a permanent worker from the same family retires or leaves the job (Biswas et al., 2020). However, garden owners prefer to hire more casual or temporary workers to minimise costs and increase profits. Many workers had to wait years to gain permanent status, and this process often takes anywhere from 6 months to 40 years. Temporary workers are allowed to reside in the garden only if a family member has permanent employment status (Al-Amin & Islam, 2020).
Workers on plantations depend on their employers for housing, food, medical care and education for their children. They often find themselves in substantial debt to the company. The daily wage for a registered worker is only BDT170 (approximately $1.70), while a casual worker can earn as little as BDT120 (approximately $1.20) for 8 h of work (Islam & Al-Amin, 2024). The government leases land to tea garden owners with the condition that several amenities and facilities must be provided to workers in addition to their regular wages. According to the Bangladesh Labour Law 2006 and the Bangladesh Labour Rules 2015, the tea garden management must provide accommodation, healthcare, education and water and sanitation facilities for workers and their families. While these non-wage benefits are available to permanent workers, temporary workers do not have access to them (Razzaque et al., 2022).
The Bangladesh Tea Workers Welfare Fund Act of 2016 established various welfare provisions for tea garden workers. This includes financial grants from the welfare fund for workers who are permanently incapacitated during work and subsequently suspended. Additionally, workers’ families may receive monetary grants from the fund if a worker dies while employed or within 5 years after retirement. The act also offers financial support for the marriage of a worker’s daughter, covers medical expenses, purchases assistive equipment and funeral expenses and buys textbooks.
Previous research (Bora et al., 2018; Chowdhury et al., 2011; Das & Islam, 2006; Jalil & Gauala, 2024) revealed that people living and working in tea gardens experience multiple vulnerabilities, including wage discrimination, lack of healthcare, inadequate food and nutrition, poor housing, insufficient access to water and sanitation, indecent work conditions and instances of sexual harassment. Earlier studies (Ahmad et al., 2015; Chowdhury et al., 2011; Das & Islam, 2006) indicated that many basic needs of tea garden workers remain unmet due to low wage structures and a lack of resources. These studies highlight a vicious cycle of poverty in tea garden areas, where workers are often deprived of access to education, healthcare and other fundamental rights. In a relatively recent study, Al-Amin et al. (2017) categorically explored the poverty situation and social exclusion among tea garden workers in Bangladesh. The results showed that these workers could not seek employment outside the gardens due to their remote locations and various socio-economic factors, including ethnicity, culture and language.
The poverty rate among tea garden workers in Bangladesh is alarmingly high, with 61.9% living below the poverty line. This figure is three times higher than the national average and four times higher than the rate in Sylhet Division, where most tea gardens are located. Additionally, the level of multidimensional poverty among tea gardeners is twice the national rate (Razzaque et al., 2022). Most tea garden workers face multidimensional deprivations, including low wages, limited access to health care, education and social protection services, and restricted livelihood opportunities (Razzaque et al., 2022). The isolation from mainstream Bangladeshi society, distance from local communities, a sedentary lifestyle and strict plantation rules contribute to their impoverished condition and vulnerability (Al-Amin & Islam, 2020; Islam & Al-Amin, 2024).
Past research from Bangladesh (Ahmad et al., 2015; Ahmmed & Hossain, 2016; Chowdhury et al., 2018; Hassan, 2014; Hossain et al., 2017; Jalil & Gauala, 2024) has drawn attention to inadequate housing facilities, a lack of proper washrooms and the absence of clean drinking water in tea gardens. The studies also highlighted that many older people have become accustomed to practising open defecation due to the unavailability of washroom facilities in the gardens. For instance, Chowdhury et al. (2011) indicated that social vulnerability manifests in tea gardens, where many people are illiterate and do not adhere to hygiene practices. Approximately 20% of tea workers defecate near natural drains, while 45% use unhygienic latrines. Similar unsanitary practices and poor sanitation systems have been observed in tea gardens in other countries as well. For instance, about 65% of the tea garden population in India had adopted open defecation practices due to a lack of sanitary latrines and the distance of these facilities from their workplace (Bora et al., 2018).
The outbreak of COVID-19 deepened the vulnerability of older people in tea gardens since they are at high risk of COVID-19 and vulnerable to the indirect consequences of the pandemic. World Health Organization (WHO) prepared a technical guideline emphasising the provision of home care and community-based health care for them. Older people and their caregivers are recommended to understand preventive measures and promote physical and mental health during the outbreak of the pandemic (World Health Organization, 2020). So far, no studies have explored the health vulnerability of older people living in tea gardens in Bangladesh following the outbreak of COVID-19. Therefore, this article addresses the knowledge gap and explores the health vulnerability and challenges of older people living in tea gardens in Sylhet district, Bangladesh.
Conceptual Framework
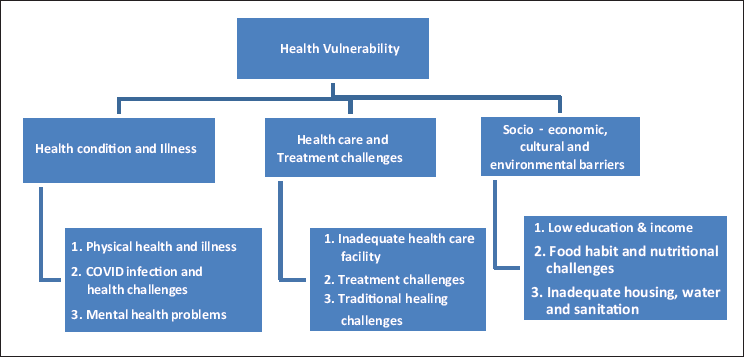
The present study conceptualised health vulnerability from three dimensions: health and illness, healthcare and treatment and socio-economic and cultural challenges (Figure 1). The health vulnerability of older people in tea gardens results from multifarious conditions emanating from biological, social and environmental factors. People feel a sense of vulnerability due to a decline in physical and mental health conditions. The nature of work in tea gardens often leads to specific diseases such as back pain. The outbreak of COVID-19 increased the physical and mental health risks, which further deteriorated the health conditions of older people. Health vulnerability can arise from various factors, such as lack of healthcare facilities, unwillingness to seek treatment, reliance on traditional healing methods, and inaccessible and unaffordable healthcare facilities. Another aspect of health vulnerability is embedded within sociocultural and environmental contexts, which can hinder or promote health and wellness. The consumption of nutritious food, leading a healthy lifestyle, financial ability to purchase nutritious food, knowledge about balanced diets, access to pure drinking water, personal hygiene and adequate housing and sanitation system play a significant role in determining the overall health and wellness of individuals.
Conceptual Framework for Understanding Health Vulnerability.
Objectives
The objectives of this study were to:
Understand the health risks of elderly individuals living in tea plantations in the Sylhet district of Bangladesh during the COVID-19 pandemic. Analyse the barriers to accessing healthcare services encountered by older adults living in tea gardens.
Methodology
The study used a qualitative research methodology to explore the health vulnerability of elderly individuals in tea gardens in Bangladesh. Primary data was gathered through focus group discussions (FGDs) and in-depth interviews. First, focus groups were held with older people in the tea gardens to understand the common problems related to COVID-19-induced health vulnerability. The FGDs helped create guidelines for the in-depth interviews and find potential interview subjects. Secondary sources such as policy documents, journal articles, academic books and official documents were used to contextualise the study.
Location and Research Participants
The Lakkatura tea garden area of the Sylhet district was purposively selected for the study as it is the most extensive tea garden in Bangladesh, covering around 3,200 acres of land with an annual production of 500,000 kg of tea (Ahmad et al., 2015). Data were collected from the in-depth interviews and FGDs with older people living in the Lakkatura tea gardens of Sylhet, Bangladesh. The following inclusion criteria were used to recruit the respondents:
To be included in the study, respondents should be individuals over 60 who live permanently in the tea garden area. The study included literate and illiterate elderly individuals who voluntarily wanted to participate, regardless of gender or employment status.
Twenty-one older adults in the Lakkatura tea garden were selected for the study. Initially, the participants were selected based on the information collected from the FGDs. The subsequent participants were recruited purposively using the snowball sampling technique.
Data Collection
Two data collectors were recruited for data collection, considering their prior practice research experience. The investigators were trained in research ethics, methods and data collection techniques. The interviews were conducted in the garden premises at a convenient time for the respondents. The interviews were recorded with the participants’ permission. On average, in-depth interviews were 45 min–1 h, and the FGDs were 2 to 2 h and 30 min long. The fieldwork was conducted from January to June 2022. The interviews were continued until a saturation point was reached, at which point no new information was produced, and similar data were frequently repeated across the interviews. The three FGDs were conducted with six to eight participants in each group to collect primary data.
Ethical Guidelines
The study adhered to the ethical guidelines established by Miles and Huberman (1994). Participation in the study was voluntary and based on the principle of informed consent. At the beginning of the interviews and focus groups, the data collectors explained the study’s purpose and nature, answered any questions, and addressed participants’ concerns. We sought the cooperation of all participants and obtained written consent from those who could write. For those who were not literate, consent was assumed once the information was provided and questions could be asked. Participants were assured that their responses would remain confidential using a code instead of their names (Neuman, 2014).
Data Analysis
The transcripts from the interviews and focus groups were analysed in three stages using thematic analysis (Denzin & Lincoln, 2011). In the first stage, the transcripts were coded according to the study’s objectives. In the second stage, they were revisited to identify recurring and emerging themes. Finally, the transcripts were re-read and re-coded using the constant comparative method to highlight categories derived inductively from the participants’ narratives. The trustworthiness of the analytic process was strengthened through method triangulation, which involved comparing findings from focus groups and interviews to identify consistencies and contradictions, thereby enhancing the credibility of the interpretations.
Findings and Discussion
Socio-demographic Profile of Participants
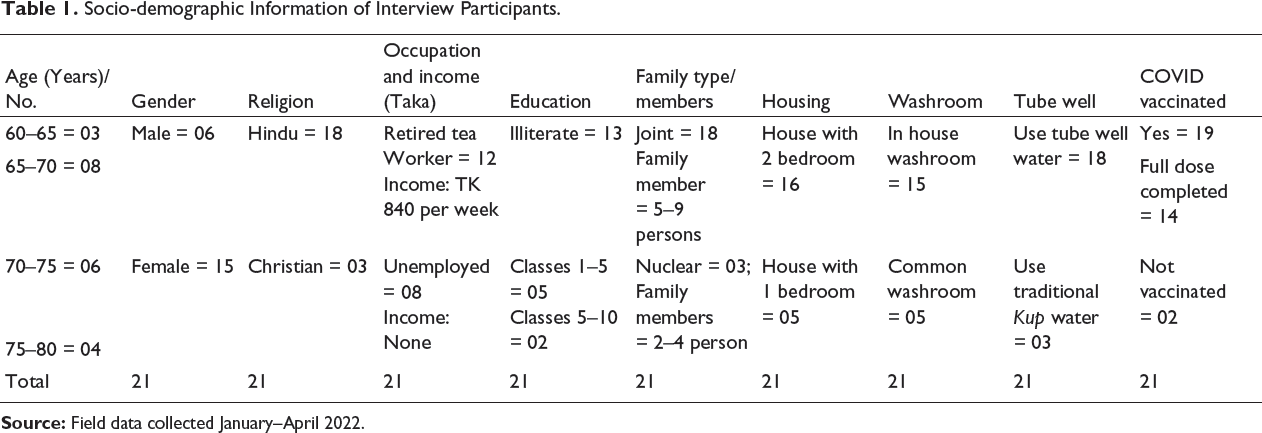
Table 1 presents the socio-demographic profile of the participants. The findings indicate that the majority of participants (n = 15) were female. In terms of age, 3 participants were below 65 (≤65) years old, 8 were below 70 (≤70) years old, and the remaining participants were above 70 (≥70) but below 80 (≤80) years old. Regarding religious affiliation, most participants (n = 18) identified as Hindu, while three participants followed Christianity. In terms of education, the majority of participants were illiterate (n = 13). Five participants had completed only primary education, and two had enrolled in secondary education. Most participants (n = 18) belonged to joint families, typically consisting of five to nine members. The findings also revealed that many participants resided in two-room houses provided by the tea garden authority and had access to single washrooms. However, many families lacked personal washroom facilities in their current housing arrangements.
Socio-demographic Information of Interview Participants.
Health Vulnerability: Physical Health Condition and Illness
Tea plantation workers endure physically demanding labour, receive low wages, lack adequate food and reside in unhygienic conditions, leading to numerous health issues in their later years. The present study revealed that older people in tea gardens suffer from multiple diseases, including headache, skin diseases, fever, cough and cold, gastric ulcer, toothache, heart disease, hypertension, cancer and asthma. The types of health problems vary from long-term illnesses such as hypertension and heart diseases to seasonal issues such as fever, cough and cold, and asthma. All the diseases cause deterioration of their physical health and increase health vulnerability. The following extracts point out their vulnerable health condition:
I have been suffering from hypertension and heart disease for the last two years. Apart from these two diseases, I suffer from seasonal illnesses such as fever, cough and cold.
The previous research (Rahman et al., 2021) highlighted the prevalence of malnutrition, fever, headache, tuberculosis, diarrhoea, hypertension, stroke, musculoskeletal pain and prostate and lung cancer among older people in tea gardens in Bangladesh. This study also noted a lack of drinking water, latrines and sanitation facilities in the garden areas. As a result, many poor elderly residents are forced to practice open defecation in the gardens, which increases their vulnerability to health problems.
I have been suffering from multiple health problems, such as diarrhoea, dysentery, and skin diseases. My family do not have a toilet facility. It is difficult to go to nearby bushes or jungles for defecation.
Tea garden workers have suffered from back pain and other physical complications due to the long hours spent collecting tea leaves.
I had severe back pain, pain in the hands and feet, and a burning sensation in the chest. I also have problems with appetite and indigestion.
The high prevalence of back pain among tea garden workers is largely attributed to the nature of their work, which requires them to stand for long periods. As Ahmmed and Hossain (2016) noted, long work hours, the risk of snake bites, exposure to wind and rain and lack of toilet facilities significantly increase the health vulnerabilities of tea garden workers in Bangladesh. Furthermore, the COVID-19 pandemic has amplified the vulnerabilities of older tea garden workers. Rahman et al. (2021) further explored that tea workers are particularly susceptible to diarrhoea and other health issues due to the lack of access to clean drinking water. Malnutrition is also a concern, as many workers struggle to afford nutritious food, and alcohol consumption further impacts their health and financial stability.
Al-Amin and Islam (2020) pointed out that alcohol plays a significant role in the lives of tea workers, serving as a ‘tranquiliser’ for those who endure long hours with low wages and minimal civic amenities, which often leads to social isolation. The present study indicates that alcohol consumption among older tea gardeners increased during the COVID-19 pandemic, as many turned to drinking to cope with the extended hours of isolation, further heightening their health vulnerabilities.
We drink locally-made alcohol. However, we took more during the COVID-19 time.
I had more time during the COVID-19 period. I can only interact with a few people. I cannot go outside. So what should I do all the time? I took more alcohol.
The physical health of older individuals in tea gardens is poor due to the nature of their work, lack of access to nutritious food and insufficient healthcare facilities. Studies demonstrated that the health vulnerability of older people significantly increased during the COVID-19 pandemic in many countries, including Bangladesh (Islam et al., 2021) and Italy (Sanfelici, 2020). Since older adults were considered at high risk for coronavirus transmission, their physical movement, social interactions and visits to healthcare facilities were restricted compared to younger populations.
COVID-19 Infection, Misconceptions and Vaccination
The findings indicate that the rate of COVID-19 infection was low in tea gardens, and most people practised physical and social distancing during that time.
Neither my family nor I got infected by COVID-19. We, the tea garden people, do not go outside the garden or visit any COVID-infected people. I took two doses of the COVID-19 vaccine.
Many older people in tea gardens mistakenly believe COVID-19 will not affect poor individuals engaged in manual labour.
I believe that hard-working people like me will not be affected by Coronavirus. We work hard … Coronavirus will not attack us.
The majority of older people get vaccinated during the pandemic. The following narratives point out the issue:
I got two doses of the COVID-19 vaccine and learned about coronaviruses from TV. Our young people also informed us of this and encouraged us to vaccinate.
However, a few older people reported not taking the COVID-19 vaccines because of inadequate knowledge, fear of its potential consequences, irregularity and mismanagement of the tea garden health centre.
I was scared about the vaccine’s consequences for our physical health, so I did not take the COVID-19 vaccine.
I did not take the COVID-19 vaccine. When I went to our health centre to get it, they told me there was a shortage of vaccines.
COVID-19 Pandemic and Social Distancing: The Role of Panchayet
The study found that the Panchayet
2
system prevalent in tea gardens played an important role in sensitising tea gardeners during the COVID-19 outbreak. Although the Panchayet is responsible for maintaining administration in the gardens, it distributed masks and sanitisers, prevented outsiders from entering, and taught the gardeners to maintain personal hygiene and social distancing measures, given the severity of the humanitarian crisis during the pandemic.
Our Panchayet recruited a security guard in the garden for our protection. You know many people come into our area to roam, but we fear that if anyone gets sick, we all will die.
Panchayet and the garden manager gave us hand sanitiser, masks, soap, face cream, toothpaste, and detergent powder.
Tea garden workers are entitled to subsidised food, accessible general health facilities and subsidised accommodation from the tea garden administration. However, various studies (Islam & Al-Amin, 2019; Jalil & Gauala, 2024) report that the facilities they received are insufficient even for subsistence living. They cannot manage a balanced diet independently with the wages and subsidised facilities. Therefore, tea garden workers, including older people, depended on support from various social welfare institutions, including Panchayet, for survival during the pandemic.
Mental Health Conditions During COVID-19 and Challenges
The present study explored the deplorable mental health condition of older people during the COVID-19 pandemic. The global pandemic impacted every aspect of human life by promoting social distancing, limiting social interactions, reducing income, disrupting the supply of daily necessities and creating a world of uncertainty (Jalil & Oakkas, 2024; Lingam & Suresh Sapkal, 2020; Magnusson & Jha, 2024; Pawar, 2024). Therefore, people, irrespective of their ethnicity, language, nationality, race and caste, experienced increased tension, anxiety, sleep disturbances and emotional issues affecting their mental health (Pawar, 2020a, 2020b; Zrihan-Weitzman, et al., 2024). The effects of the COVID-19 pandemic on the mental health of elderly tea garden workers are described below.
Anxiety for the Future of Children and Grandchildren
The mental health of elderly tea workers is being affected because they are worried about the future lives of their children and grandchildren. The COVID-19 pandemic has disrupted various aspects of human life, such as social interaction, employment, food supply chain, health facilities and education, leading to a decline in the mental health of older people worried about the uncertain future. The following excerpts illustrate the deplorable mental health conditions of the elderly people living in the tea gardens of Bangladesh.
I saw the COVID-19 situation on TV and worried about my children’s future during the pandemic.
My two sons work outside the garden. I was afraid of thinking about the health risks of my sons. I was anxious about any possible casualties due to the pandemic.
Older people in tea gardens also expressed heightened anxiety regarding their children’s future due to their impoverished state.
I was worried about my children’s future. I struggled with economic hardship while trying to cover our family expenses with my modest income. I felt frightened, thinking our children would also have to endure a challenging life like ours.
Three of my children are studying at different schools. I struggle to bear my family’s expenses and education and am anxious about their uncertain future.
Anxiety About Their Future Life
The older individuals in tea gardens are worried about their futures because of the COVID-19 pandemic. Their concerns mainly revolve around financial arrangements both during and after the pandemic. In the tea gardens, elderly residents have expressed concern about meeting their current needs and making ends meet, mainly because they are retired and rely on their children’s earnings.
Since I have no income after retirement, I feel helpless. I am dependent on my son for all my expenses. How long can my son support me during the pandemic?
One participant reported that his mental health condition is affected by thinking about future uncertainties.
I crossed the pension age range many years ago, but I cannot apply for retirement as I am the only earning member of my family. My body does not support working more, and there is also a restriction on working in COVID-19.
The usual practice within the tea garden community is to be cared for by family members after retirement. However, one elderly tea worker expressed concern because he lacks family support for his care in old age.
I face a relationship breakdown with my children. They do not contact me. I feel sad and sometimes feel depressed.
The participants highlighted a range of issues related to their declining mental health. Their concern ranged from financial insecurity to care deficiency in their later life. However, all participants attributed these issues to the COVID-19 pandemic, which had a devastating impact on their mental well-being.
Treatment Methods and Challenges: Where Do They Receive Treatment?
The findings revealed that elderly individuals often visit a healthcare centre in the tea garden area to treat common health issues such as fever, cough and cold, stomach-ache and pain.
I used to get medication for fever, cough, and pain from the clinic in the garden. Sometimes, I purchase medicine from the nearest pharmacy. For significant health issues, I seek treatment at Osmani Medical College Hospital.
The finding reveals that qualified doctors are unavailable in the tea garden clinic. The physician at the garden only provides free paracetamol, antihistamines and other inexpensive medicines to tea garden workers. Retired older workers do not receive regular access to medicine. Their ability to access government hospitals is also restricted due to the countrywide lockdown.
There is no specialist doctor in the garden hospital. The one who is available does not behave well with us. There is even a complaint against him that he sells medicine.
The garden hospital only prescribes paracetamol. However, I cannot go to public hospitals due to the lockdown.
Some older people visit nearby pharmacies outside the tea garden area. Since they cannot afford the doctor’s consultancy fee, they ask the pharmacist to provide whatever medicine is appropriate to heal their sickness.
I visit the nearest pharmacy and garden clinic. They provide medicine using common sense; they are not specialist doctors.
What Problems and Challenges Do They Face?
The findings of this study indicate that the impoverished condition of elderly individuals in tea gardens contributes to their health vulnerability. Due to financial constraints, they are reluctant to seek medical care at public hospitals outside the garden. Many cannot afford the transportation costs associated with visiting these hospitals. Furthermore, financial constraints prevent them from seeing specialist doctors outside the garden. Additionally, restrictions on transportation during the countrywide lockdown forced them to depend on the health centre within the garden.
I cannot afford to see the doctor. I can only get medication from the garden clinic. Sometimes, I have to buy medicine from the pharmacy because the garden clinic does not provide medication for hypertension and eyesight issues.
This study explored the fear of being accepted by the hospital staff and the anxiety about communication with educated health professionals, which prevents many older people from visiting public hospitals. Some older people are confused about whether they will receive proper treatment in public hospitals due to their ethnic identity and miserable economic conditions.
I cannot get service in the large public hospital because I cannot talk like them. Without service, sometimes we are back home, and our suffering increases.
We do not feel comfortable to seek treatment outside the community. Because we are tea workers, we do not get proper treatment in the hospital. We do not even know the procedure of getting services.
Some participants expressed dissatisfaction with the health facilities available on the garden premises, pointing to the malpractices that the responsible health workers committed.
There is a shortage of medicines in the garden hospital. They provide napa, histamine and antacids for all diseases. We often found them closed.
The findings also indicate they face challenges accessing healthcare facilities in the tea garden. No health services are provided during an emergency.
We usually visit tea garden hospital, but it opens only in the morning. We often need emergency medical help in the evening or night, and there is nothing like that.
The garden hospital remains closed most of the time. Therefore, I visited the nearby pharmacy and bought medicine from there.
The participants’ narrative highlighted the challenges older people in the tea garden encountered in accessing healthcare at government hospitals during the outbreak of the COVID-19 pandemic.
My wife was sick during COVID-19. I suffered a lot to manage her treatment in the tea garden. Then, I took her to Sylhet Osmani Medical. Because of the lockdown, there was no transport on the road; at last, we were bound to go by rickshaw to travel long distances.
During COVID-19, I was sick two or three times but could not visit the hospital because of the lockdown. I did not get any transport to the hospital.
Traditional Healing: Alternative Attempt to Cost Minimisation
Tea garden workers adopt traditional healing procedures to get cures for most diseases. It is a common practice among tea gardeners to visit rural kabiraj, Purohits and Ojhas to heal their health condition (Rahman et al., 2021). The present study also revealed that all participants utilised traditional medicine and spiritual healing during their lives.
I never visited the tea garden clinic for treatment. I do not know whether they will provide medicine or not. We follow our traditional treatment. We often visit the Kobiraj for Jhar fhuk.
Bhesojo medicine is better. The man collects different herbal leaves and different parts of the tree. He adds many things and makes medicine. It works for many diseases. You do not need to spend much money on this.
Due to the lockdown and social distancing, older people in tea gardens have difficulty accessing modern medical services, increasing their reliance on traditional healing practices.
We prefer bhesojo (herbal) treatment from the healer of a tea garden. During the pandemic, we relied on bhesojo medicine and jhar-fuk from traditional healers. We often visited the Puruhit and kabiraj [traditional healers].
The narratives provided by the elderly individuals in tea gardens underscore a significant shift in healthcare strategies during the COVID-19 pandemic. Their increased reliance on traditional healing practices, which are non-scientific in nature, raises concerns about the potential health risks for older people during the pandemic.
Food Habits, Diet and Nutrition Challenges
The findings revealed that elderly individuals in tea gardens could not access sufficient food due to low wages, extreme poverty and lack of alternative sources of financial support. As a result, many tea garden workers suffer from malnutrition. Most participants reported that their diet mainly consisted of homemade wheat bread with fried potatoes, tea, biscuits and bread for breakfast. They often have rice with mashed or fried potatoes and pulses for lunch. During winter, they consume vegetables, while fish and meat are considered luxury items they can only afford when they receive their wages. Meat is only prepared for special occasions or when guests visit.
We eat pulses, rice, and vegetables and occasionally fish and meat. We eat rice twice a day, have tea for breakfast with puffed rice or biscuits, and sometimes eat vegetables and roti [homemade bread].
Rice and vegetables are our staple food. Sometimes we get fish and meat. In the morning, I have tea, biscuits, and puffed rice.
Low Income and Insufficient Dietary Intake
Participants shared that older individuals in tea gardens are at a higher risk of poor health due to inadequate dietary intake. The lower income experienced during COVID-19 diminished their ability to purchase food, and disruptions in food supply mechanisms further exacerbated the situation. As a result, their vulnerability to health issues increased.
In the morning, we eat roti or ‘pantha vaat’ with green piper and sometimes potato vorta. We have hot tea with salt. Depending on our income, we eat rice with dry fish during the daytime and rice or roti with lentil soup at night.
With the low income from tea plucking, we can hardly afford nutritious food like meat, fish and eggs.
Lockdown and Food Shortage During the Pandemic
The COVID-19 pandemic significantly affected the food habits of older people in tea gardens. The existing research (Akter et al., 2022) also reported that the COVID-19 pandemic negatively affected the consumption of fish and meat among low-income people in the urban areas of Bangladesh. Since the countrywide lockdown and social distancing measures restricted the supply of essential foods, the prices increased. Similar findings were reported in some other studies (Banna et al., 2022; Das et al., 2020; Sohel et al., 2021) that low-income people in urban and rural areas of Bangladesh had to compromise a balanced diet during the COVID-19 pandemic. Henrickson (2020) highlighted COVID-19’s effects, showing that the pandemic caused extensive food insecurity, financial difficulties and homelessness. Many low-income families had to depend on a limited diet of potatoes, vegetables and rice, demonstrating their fight for essential nourishment during these difficult times. The present study found a similar situation in the tea gardens. The participants’ accounts revealed that older people face severe food shortages for themselves and their family members due to lockdown and social distancing measures.
We suffered during the COVID-19 pandemic. No vendors came to tea gardens, and the shopkeepers could not sell products without money, so the price of all necessary products increased. My son worked outside the tea garden, but his work was off. We cannot even manage sufficient food for our family members.
We had a terrible situation during the pandemic. Vendors were not allowed to enter the garden. So how can we find vegetables and other food items? Lentil and potato were the only menus for us.
Older tea garden workers described how COVID-19 significantly affected their ability to buy food, decreasing the quantity and nutritional value of their meals. Like many countries such as Australia (O’Sullivan et al., 2020), Italy (Sanfelici, 2020) and India (Sengupta & Jha, 2020), many older individuals noted that family members lost their jobs due to government lockdowns and social distancing measures, emphasising the difficult situation they faced.
My elder son and the younger son were unemployed during the pandemic. I was the only earning member. I work part-time in a tea garden with little wage. That was the only income we survived with.
My two sons lost their jobs, which caused my family to suffer a lot. My elder son worked in the tea garden. During COVID-19, eleven members of my family depended on his meagre income. It was a horrible time, and we used to eat once a day; the other times, we had to starve.
Due to lockdowns and social distancing measures that limited the supply of essential foods, the prices of nearly all food items increased. Many participants reported that the cost of most food, especially fish and meat, was beyond their financial reach during the COVID-19 period. As a result, they had to compromise on maintaining a balanced diet, which negatively impacted their physical health.
The price of all foods increased during COVID-19. We could not buy fish, as the price was beyond our financial capacity.
How will I tell you what we eat? We earn very little money. We could not buy fish during COVID-19 because the price was so high.
Conclusion and Policy Implications
The findings of this study highlight the physical and mental health challenges faced by elderly individuals during the COVID-19 pandemic, mainly due to poverty, inadequate healthcare facilities and food insecurity. The global crisis has resulted in increased levels of tension, anxiety, sleep disturbances and emotional difficulties. Additionally, there are growing concerns about the future well-being of children and grandchildren due to significant disruptions in various aspects of life, including social interactions, employment, food supply chains, health services, education and overall mental health. The study also indicates that rising food prices during the pandemic present a major challenge to physical health and survival. Many families have experienced job losses, reduced incomes and food insecurity. Nationwide lockdowns and social distancing measures have limited the availability of essential food items, leading to price hikes. Consequently, many elderly individuals have had to depend on basic staples such as wheat, lentils, potatoes, vegetables and rice for their survival.
Despite the legal obligation to establish a welfare system for tea garden workers in Bangladesh, the tea company only provided limited services to meet their basic needs. Temporary workers, who make up a significant portion of the workforce, were not offered accommodations, food rations, healthcare or other benefits by the garden administration. Permanent workers also faced challenges, as the garden health centres lacked qualified medical staff and essential medicines. Additionally, during the COVID-19 pandemic, transportation to hospitals outside the garden was nearly non-existent, which increased health risks for elderly individuals.
Health service providers in tea gardens and hospitals need to be more responsive to the healthcare needs of marginalised older adults living in tea gardens and their family members. Due to resource constraints, it is essential to develop more flexible service provisions to meet their health requirements. Involving tea gardeners in the planning and delivery of health services is crucial for ensuring effective participation. The mental healthcare system in Bangladesh faces several challenges, including a lack of public mental health facilities, a scarcity of skilled professionals, inadequate financial resource allocation and social stigma.
It is essential to prioritise the mental health of older adults in tea gardens by providing guidance on health promotion, emotional control, stress reduction and anxiety management. Before implementing any programs for their well-being, inter-professional collaboration and community engagement should be emphasised. Therefore, it is crucial to involve the tea garden authorities, local administration, development workers, nutritionists, and community members in the planning and implementation of services. Health and social service providers should recognise the importance of service users’ beliefs, perceptions, and cultural factors and ensure their participation in all health services and development projects.
This study offered valuable insights into the health vulnerabilities faced by elderly individuals living in tea gardens in Bangladesh during the COVID-19 pandemic. It is important to explore their health vulnerabilities in the aftermath of the pandemic. Moreover, a significant number of tea garden workers are employed on a temporary or casual basis, which means they are not entitled to even the minimum welfare benefits available to permanent workers. Thus, further studies can be conducted to examine their conditions and provide support for elderly temporary workers in the tea gardens. Furthermore, to better prepare for future pandemics, healthcare access must be improved by ensuring the availability of qualified health professionals, essential medicines, and promoting health education. Social safety networks should be expanded so that both permanent and temporary workers can receive food, financial assistance, and welfare benefits.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the SUST Research Centre, Sylhet, Bangladesh (Project ID: SS/2021/1/37).