
Abstract
Abstract
Introduction: Anatomical localization of brain infarcts based on clinical symptoms and signs is a key step in stroke diagnosis, but evidence linking specific clinical features with infarct locations is limited. We aimed to identify symptoms and signs of ischemic events that statistically favor precise posterior circulation locations.
Patients and Methods: We analyzed data from the New England Medical Center Posterior Circulation Registry for 407 adults with previous posterior circulation ischemia (confirmed by brain/vascular imaging). Using multivariate logistic regression and the binary sorting table method, we determined the negative and positive predictive values of 24 signs and symptoms for infarct localization within the proximal, middle, or distal posterior circulation territories.
Results: Visual field defect (hemianopia) was a positive or negative sign for all 3 brain stem regions. The presence of visual field defect positively correlated only with the distal region (P < .001), and its absence indicated infarction in the proximal (P = .007) or middle (P < .001) territories. Visual field defect showed the greatest localizing sensitivity and specificity with other signs: visual field defect absence with presence of nausea−vomiting for the proximal region, or hemiparesis and other motor signs in the middle region; presence of visual field defect alone or with absence of generalized weakness in the distal region.
Discussion and Conclusion: Presence of visual field defect alone statistically confirms the occurrence of a distal region infarct and excludes proximal or middle territory involvement. Moreover, presence or absence of this sign in the presence of other signs or symptoms localizes the event to proximal or middle regions.
Introduction
The symptoms and signs of the presenting patient are a fundamental component of clinical assessment following brain infarcts and hemorrhages, and remain the primary focus of physicians in determining the anatomical location of the event.1,2 Clinical localization is important for optimizing the use of brain and vascular imaging, 2 and for determining the cause of the ischemic event. Further localization within the territories supplied by the vertebral and basilar arteries and their branches (the posterior circulation) provides key information about stroke mechanisms and the subsequent risk of particular vascular lesions. 1 Prompt recognition of the event location helps to guide the treatment of posterior circulation ischemic events and may help to reduce morbidity and mortality. 3
The posterior circulation supplies very diverse regions of the brain (eg the brainstem, cerebellum, thalamus, and posterior portions of the cerebral hemispheres), in contrast to the anterior circulation, which feeds the anterior and lateral portions of the cerebral hemispheres. 4 Ischemic injury in the posterior circulation is therefore associated with many different brain signs and symptoms, making identification of the precise location of the event challenging and increasing the risk of misdiagnosis. 5 Indeed, localization is crucial for ensuring diagnosis is accurate and the most appropriate management strategies are implemented. 2 There are some data linking specific clinical features with infarct locations,6-11 but robust evidence is limited, and improved strategies for reducing stroke diagnostic errors are needed. 5 Searls et al 2 were the first to publish a correlation analysis of the most frequent symptoms and signs by territory, confirmed by brain imaging, in patients with posterior circulation ischemia included in the New England Medical Center Posterior Circulation Registry (NEMC-PCR). Here, we aimed to expand on these findings by conducting an in-depth analysis using multivariate logistic regression to identify symptoms and signs that statistically favor an infarct location in a particular anatomical territory within the posterior circulation, also using data from the NEMC-PCR.
Materials and Methods
Study Design and Participants
The NEMC-PCR is a large database prospectively collected between 1988 and 1996 at the New England Medical Center, Boston, Massachusetts, USA. 12 The NEMC-PCR is the largest published registry of posterior circulation transient ischemic attacks and/or strokes confirmed by brain and vascular imaging (N = 407); methodological details have been described previously.2,12,13 As this was an observational study using data collected retrospectively and with no involvement of treatment, patients were not required to provide written or oral consent.
Evaluation of Symptoms and Signs
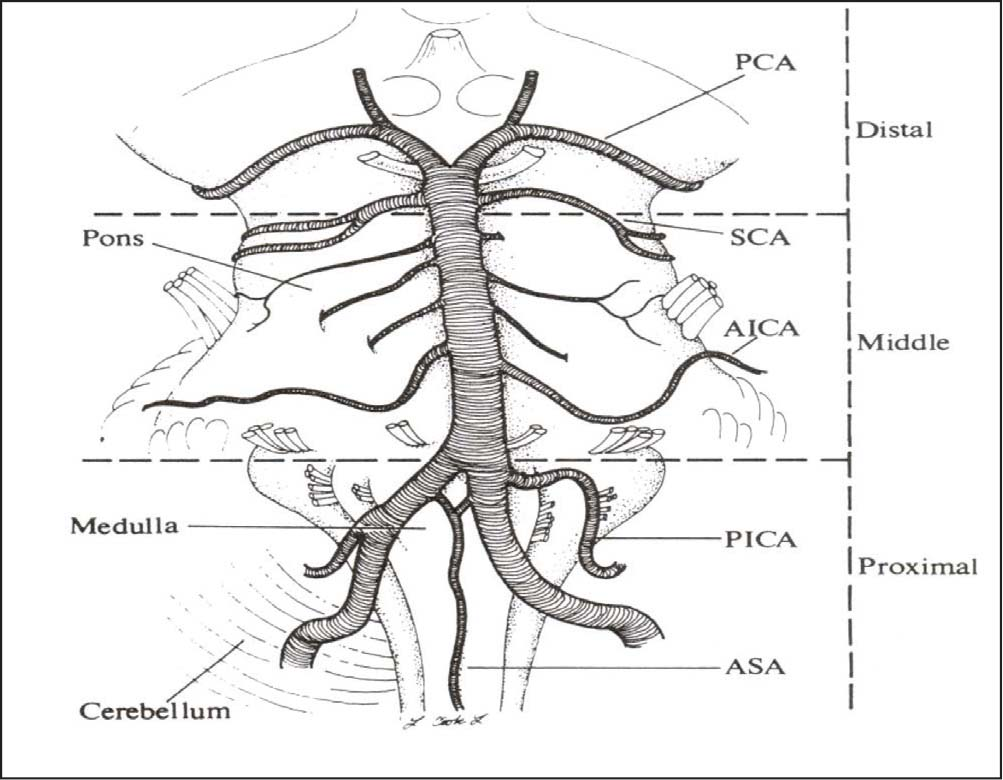
We analyzed the negative and positive predictive values for each symptom and sign among patients whose brain ischemia was limited to the proximal, middle, or distal posterior circulation territories. The intracranial posterior circulation territories were defined as: (a) proximal territory, which consists of the medulla and posterior inferior cerebellum, territory supplied directly by the intracranial vertebral artery and its posterior inferior cerebellar artery (PICA) branch; (b) middle territory, which includes the pons and the anterior inferior cerebellum, territory supplied directly by the basilar artery and its anterior inferior cerebellar artery (AICA) and penetrating artery (PA) branches; and (c) distal territory, which includes the superior cerebellum, thalamus, midbrain, and occipital and temporal lobes, territory fed by the rostral basilar artery and its superior cerebellar artery (SCA), posterior cerebral artery (PCA), and their penetrating artery branches (Figure 1).
Statistical Analysis
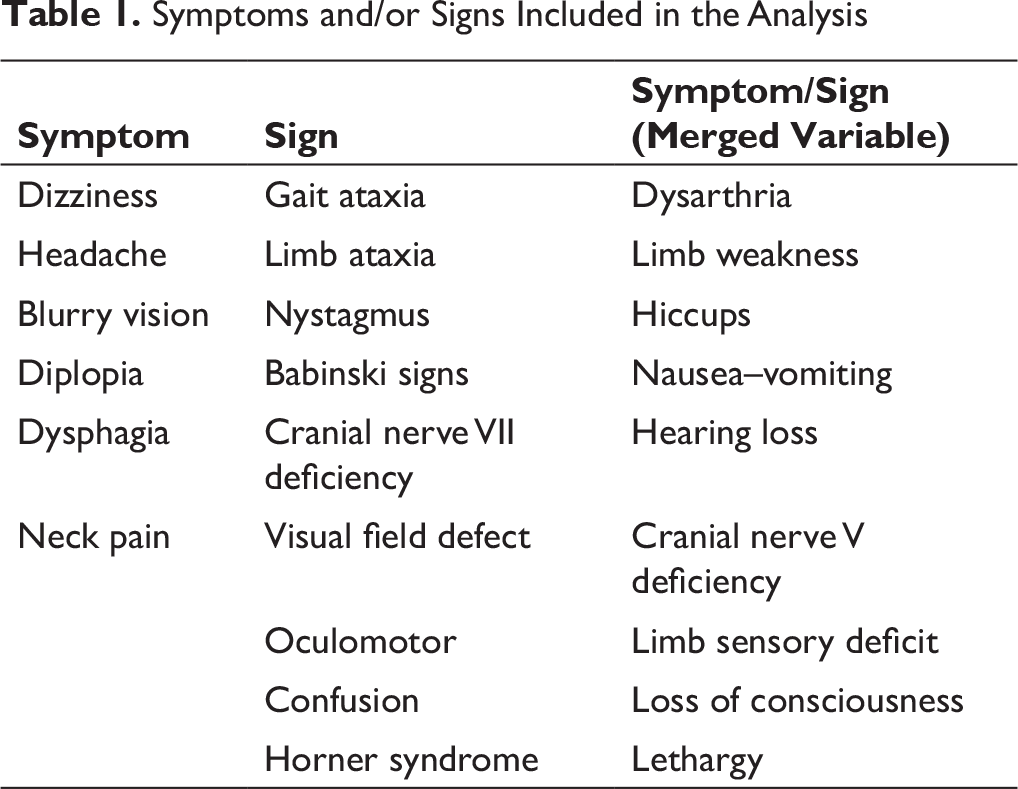
In total, 24 brainstem symptoms and/or signs were studied (Table 1). These symptoms and/or signs were the most frequently reported within the entire posterior circulation in the NEMC-PCR. 2 These data were analyzed further to define the utility of these symptoms and signs in favoring or excluding a particular location of the infarct within the posterior circulation.
Symptoms and/or Signs Included in the Analysis
To obtain the best results, multivariate logistic regression and the binary sorting table method were used. Input data consisting of 407 patient records (48 explanatory variables and 3 output binary variables) were analyzed using multivariate statistical analysis. Multivariate logistic regression was independently applied to the output variables of proximal, middle, and distal at a significance level of 0.05 using the general model:

Here, “xk” and “ck” are “kth” explanatory variables and their coefficient, “H”, is model order, “s” is its activation, and “y” is the output variable as probability of being in a particular territory. The main aim was to find the best submodel for every output variable. A submodel is defined as a model that uses only a subset of explanatory variables, with a valid submodel consisting of only significant explanatory variables on given level of 0.05. The best submodel is both valid and has the minimum possible P value from logistic regression analysis. Using binary optimization heuristics, we found the best submodels of 7 output variables in the first step. Following on from the applicability of previous statistically significant results, we applied the individual threshold value θ to the logistic regression model output thereby obtaining a binary output b = y > θ. After this procedure, a 2 × 2 contingency table was used to determine the sensitivity and specificity of the best submodels. Using a compromise threshold value of 50% yielded an unbalanced result of very low values of sensitivity together with high specificities. Therefore, threshold values were optimized to maximize classification quality, which is a minimum of sensitivity and specificity indicators, resulting in the properties for the best 7 submodels.
A binary sorting table as a novel principle was used as the referential method. The aim was to find the best submodel again using only pure sorting principles. All explanatory and output variables were binary ones. Using H explanatory variables for a given output and experimental data, we could observe a maximum of 2H input binary patterns. We formed a data cluster (input class) for every input binary pattern and then used the majority principle for the decision, whether the class was positive (y = 1) or negative (y = 0). Such a submodel is a naïve but natural one and suitable for sensitivity and specificity calculations via a 2 × 2 contingency table. Properties of the best third-order submodels were collected. Binary sorting tables were better than threshold logistic models in the case of proximal, middle, and distal modeling. Threshold logistic models were better in the remaining cases.
Every model was reported as a subset of explanatory variables, their coefficients and P values. Negative coefficients indicated a negative predictive value and positive coefficients indicated positive predictive value. Logistic regression gave probabilities of < 0.000001 for the proximal, middle, and distal territories, indicating that the best submodels were significantly better than the other valid logistic submodels for a given output. The optimum model order did not exceed 3 explanatory variables.
Results
The demographic and disease characteristics of patients included in the NEMC-PCR database have been described previously. 13
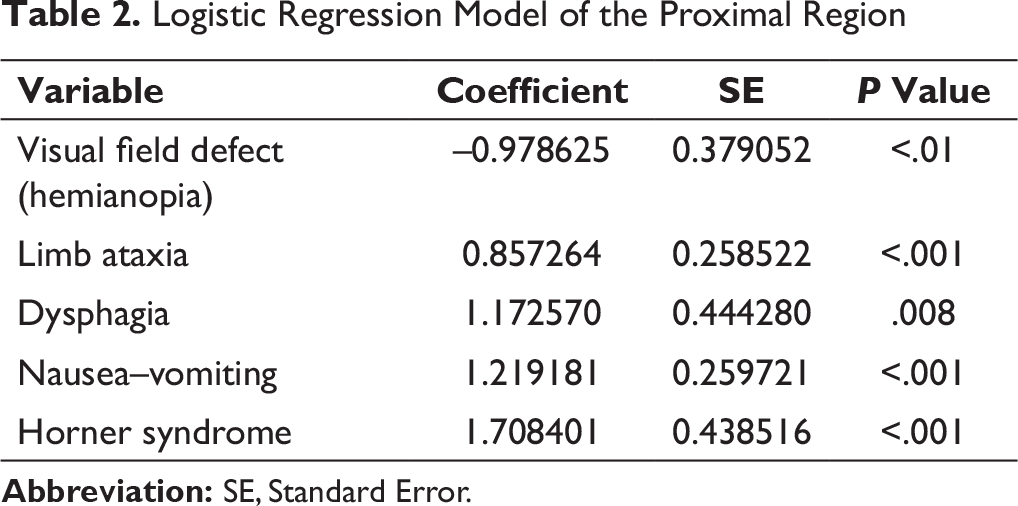
Logistic Regression Model of the Proximal Region
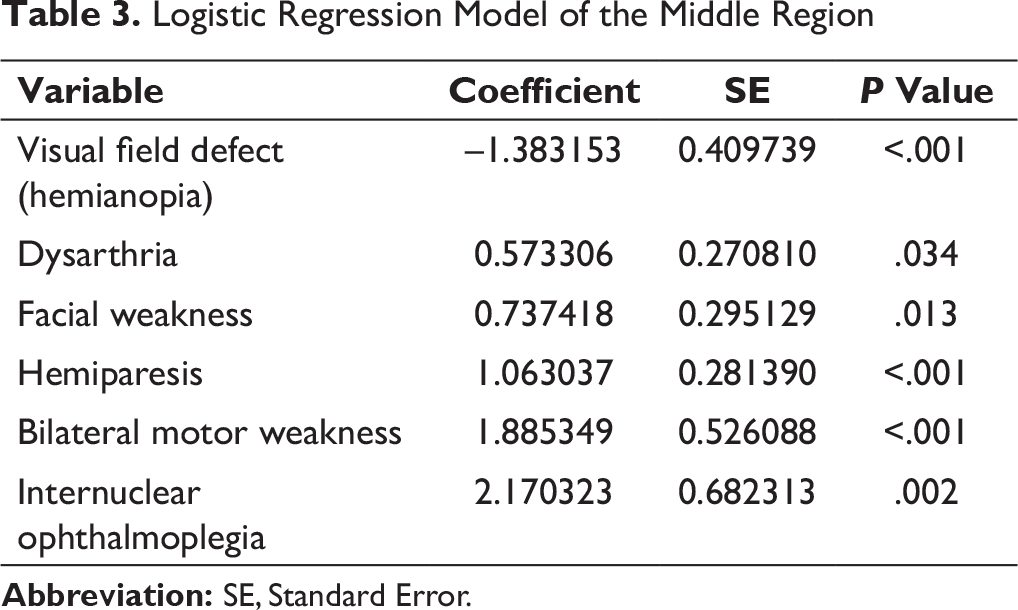
Logistic Regression Model of the Middle Region
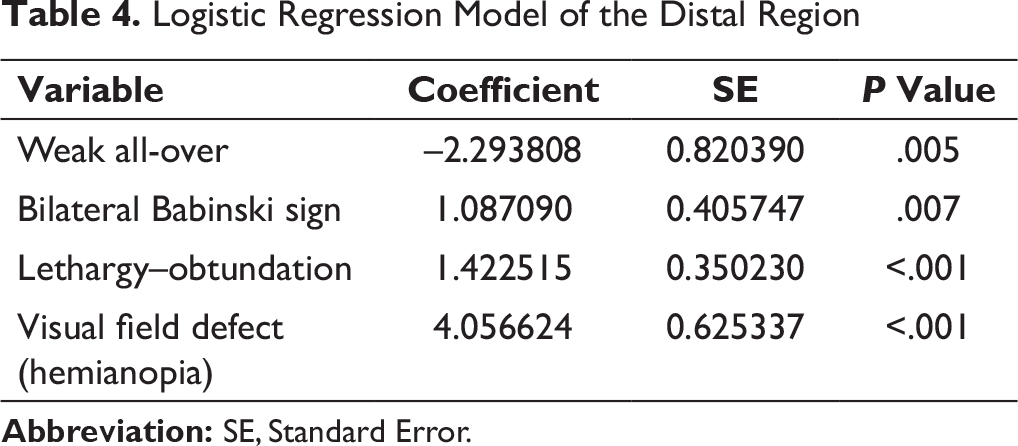
Logistic Regression Model of the Distal Region
Efficiency of Binary Sorting Table for Six Explanatory Variables
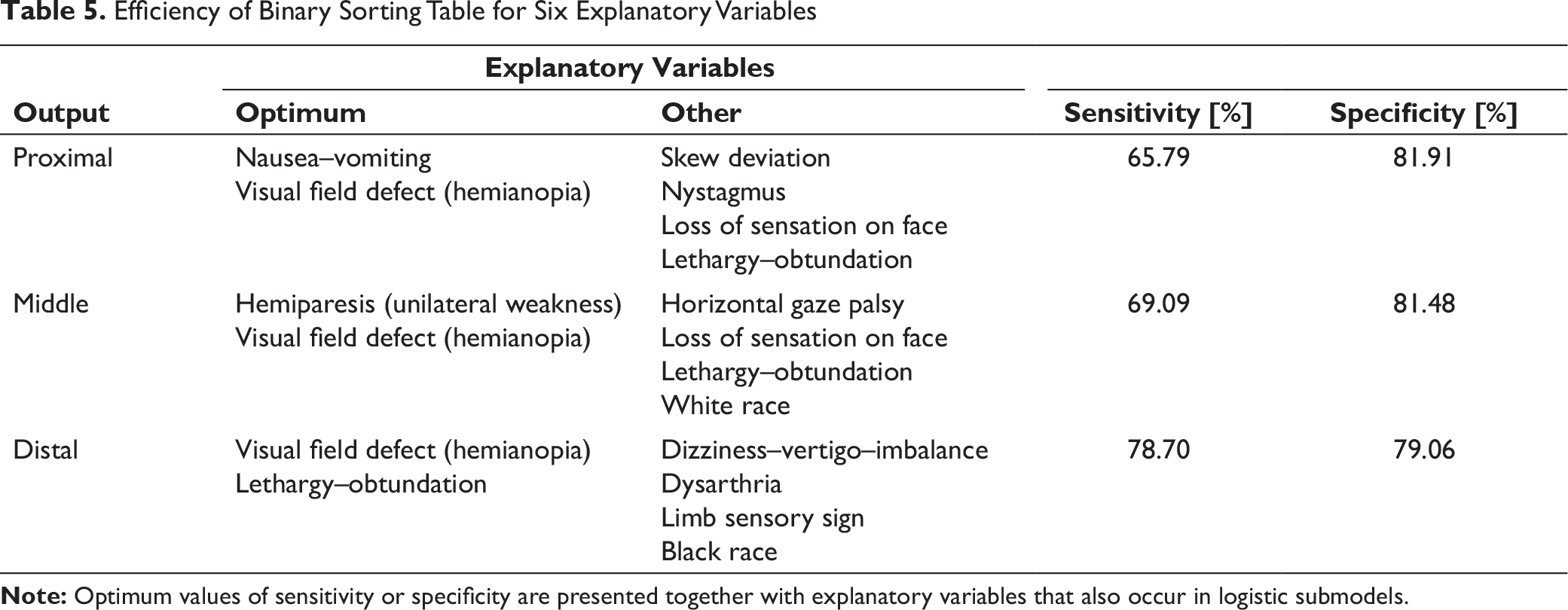
Binary sorting analysis confirmed these findings (Table 5). For each distinct region, further positive signs were identified to have sensitivity and specificity: nausea–vomiting for the proximal region, hemiparesis (unilateral weakness) for the middle region, and lethargy–obtundation for the distal region.
Discussion
Clustering of positive and negative signs greatly aids clinical localization within the posterior circulation territories. The previously published analysis from the NEMC-PCR reported correlations between separate vascular territories and the most frequent symptoms and signs of posterior circulation ischaemia. 2 Positive correlations were seen for dysphagia, nausea or vomiting, dizziness, and Horner syndrome in the proximal region; unilateral limb weakness and cranial nerve (CN) VII deficiency in the middle region, and limb sensory deficit, lethargy, and visual field defect in the distal region. These results support previous studies that have reported similar patterns of predominant symptoms and signs with infarcts in the different vascular territories.6-11 However, Searl et al noted that their findings highlighted important features of infarcts in specific territories rather than providing strong predictors of localization, and other studies have generally not aimed to differentiate between the range of clinical features as indicators of location but have focused on subtypes of ischemic disease within the territory, examined specific symptoms or signs, evaluated a particular patient group, or did not include imaging confirmation of the diagnosis. 2 To our knowledge, therefore, we present the first study to successfully use a statistical approach to show that absence or presence of a visual field defect sign aids with precise localization of infarcts in 3 brain stem regions of the posterior circulation.
We found that absence of the visual field defect sign together with the presence of limb ataxia, dysphagia, nausea−vomiting, and Horner syndrome is specific for a lesion within the proximal territory. Limb ataxia and nausea−vomiting indicate cerebellar-vestibular damage. Several small case series have reported the frequency of symptoms and signs of infarcts involving the PICA cerebellum, lateral medulla, and medial medulla. The most frequent symptoms and signs of full PICA cerebellar infarcts in a series of 66 patients were vertigo, gait ataxia, nystagmus, headache, vomiting, and limb ataxia. 14 The most frequent symptoms of lateral medullary infarcts in a case series of 33 patients were ataxia, vertigo, dysphagia, nausea−vomiting, and headache. 15 Vertigo, dysphagia, and nausea−vomiting were the most frequent symptoms in further case series of 33 patients with lateral medullary infarction. 8 In both of the latter two studies, the most frequent signs of lateral medullary infarcts were Horner syndrome, contralateral hypalgesia, ataxia, nystagmus, and facial hypalgesia.8,15 Given the above findings of full PICA cerebellar and lateral medullary infarcts, it was not unexpected that the symptoms of nausea−vomiting and the sign of Horner syndrome were significantly correlated with a lesion located in the proximal territory in our analysis.
Comprehensive evaluation of the signs and symptoms of middle territory infarcts has not been published previously. However, middle territory lesions appear to be predominantly indicated by motor symptoms and signs, including dysarthria, facial weakness, hemiparesis, bilateral motor weakness, and internuclear ophthalmoplegia. Our finding that visual field loss has a significant negative correlation with middle territory lesions is expected since the visual pathways do not cross any part of this territory. Since contralateral weakness and Babinski signs occur often in patients with pontine infarcts, it follows that these signs were negatively correlated with the proximal territory in the present study. Given the results of earlier studies, it is surprising that the signs facial nerve palsy, ataxia, and nystagmus did not have a significant positive correlation with the middle territory.16-20 The middle territory is supplied by penetrator arteries from the proximal and middle portions of the basilar artery, and by the AICA. Weakness was not a prominent sign of AICA territory infarcts in previous studies.16, 18,19 Symptoms such as vertigo, gait unsteadiness, nausea−vomiting, and facial palsy were frequent symptoms of AICA territory infarcts in prior studies16-19 but were not significantly correlated with middle territory infarcts in our analysis. These symptoms occurred with ischemia of other territories and were therefore not specific to the middle territory. However, among 111 NEMC-PCR patients with middle territory ischemia, only 8 (7%) had infarcts limited to the AICA territory, 13 which may explain the lack of specificity of vestibulo-cerebellar signs to the middle territory in our analysis.
In the distal region, we showed that visual field defect has the greatest positive localization value together with lethargy−obtundation and bilateral Babinski signs. Only lesions that involve the visual cortex and their afferent tracts and association areas cause visual field defects. The visual cortex is supplied by the PCA, the last major branch of the posterior circulation vessel tree. As motor and sensory signs have larger and more diffuse distribution within the posterior circulation territories, they are likely to be less precise as localizing tools than visual field defects. Our analysis shows that visual field defect is the only negative sign for the proximal and middle regions, and is the most sensitive and specific indicator for involvement of the distal region.
Signs and symptoms in patients who have distal territory infarcts have not been systematically analyzed. The distal territory comprises regions supplied by the rostral basilar artery, SCA, PCA, and their penetrating branches. This territory is the most heterogeneous within the posterior circulation as it includes midbrain, thalamus, superior cerebellum, and occipital and temporal lobes. Studies of infarcts in each of these regions can give an approximation of the most frequent signs and symptoms in patients who have distal territory infarcts. The “classic SCA syndrome” was originally thought to be characterized by the following symptoms and signs: ipsilateral limb ataxia, Horner syndrome, contralateral thermoanalgesia, and CN IV palsy. 21 Later studies of patients with SCA infarcts showed that contralateral thermoanalgesia and CN IV palsy were rare findings. Data from 36 patients with SCA infarcts showed that the most frequent symptoms were gait unsteadiness, dysarthria, nausea−vomiting, dizziness, and headache and the most frequent signs were limb ataxia, gait ataxia, nystagmus, dysarthria, lateropulsion, and Horner syndrome.22,23 SCA infarcts often occur in tandem with infarcts in the midbrain, thalamus, and PCA territory as a part of the “top of the basilar” syndrome. 24 The full syndrome is characterized by sudden coma, blindness or visual field deficits, amnesia, delirium, and vertical gaze paresis. PCA infarcts account for only 5-10% of the total infarcts in stroke registries.25,26 When infarcts are limited to the paramedian midbrain and/or thalamus the most common signs or symptoms are vertical gaze paresis, dysmemory, and hypersomnolence. 24
These distal territory infarcts and their related clinical findings can be ascribed to occlusions at different locations in relation to the supply of PCA branches.25,27-29 Occlusion of the P1 branch of the PCA can result in infarction of the midbrain cerebral peduncle, lateral thalamus, and the occipital and posterior temporal cortex. Occlusion of the P2 portion proximal to the thalamogeniculate arteries may cause infarction of the lateral thalamus, and occipital and posterior temporal cortex. Occlusion of the thalamogeniculate arteries can lead to infarction within the lateral thalamus. Cortical PCA branch occlusions lead to infarcts of the occipital and posterior temporal cortex. Findings from four large PCA stroke registries showed that the most frequent symptoms were visual field loss (90-97%), followed by headaches, sensory deficit, confusion, and dizziness, and the most frequent signs were visual field loss (57-94%), followed by neuropsychological deficits, sensory deficits, motor deficits, and oculomotor abnormalities. 30 In support of these findings, a positive correlation of the symptoms of blurry vision, limb sensory loss, and lethargy with an infarct in the distal territory was demonstrated in the previous NEMC-PCR analysis. 2 Indeed, blurry vision and limb sensory loss are highly specific for the distal territory because both symptoms often occur in patients who have lateral thalamic infarcts.
The positive correlation between the sign visual field defect and an infarct in the distal territory observed in our study was therefore anticipated. Finding that visual field loss is a sign specific to distal territory ischemia would be expected, because the visual cortex, part of the optic radiations, and the lateral geniculate nucleus are included within the PCA territory. Although the symptoms of weakness, dizziness, headache, and dysarthria, and the signs of weakness, ataxia, CN VII signs, and limb sensory deficits were commonly reported in patients with distal territory infarcts, they were also frequent manifestations of ischemia in patients with infarcts in other territories and were not specific to the distal territory.
Conclusions
The absence or presence of the single sign of visual field defect is a strong predictor for localizing infarcts within the posterior circulation territories. Absence of this sign indicates that involvement of the distal region is highly unlikely and statistically increases the probability of involvement of the middle or proximal regions. Presence of a visual field defect confirms involvement of the distal region and excludes involvement of middle and proximal regions. Presence or absence of this sign alone was highly sensitive and specific for all 3 regions, and together with the presence of motor or cerebellar signs was pathognomonic. Other positive signs and symptoms are more ubiquitous in patients who have posterior circulation ischemia. As localization is critical for ensuring accurate diagnosis following a brain infarct, further research is warranted to confirm that the predictive value of the presence or absence of individual and groups of signs and symptoms identified in our analysis can be applied to other populations with posterior circulation ischemia. The ability to confidently identify infarct location with signs and symptoms alone may help to guide clinicians in selecting the most appropriate management approach as early as possible after an event and before imaging confirmation is obtained.
Footnotes
Acknowledgments
We would like to thank Tamsin Williamson for medical writing support, Evžen Korbel for his contribution in sorting and clearing the data from the NEMC-PCR, and Eric Searls for his insights when planning the draft manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.