
Abstract
Objective:
To report a case of young male with stroke and bilateral internal carotid artery (ICA) dissection.
Background:
Cervical Artery Dissection in Stroke Study trial has provided some insight on management of patients with ICA dissection. However, there is a need to modify the management strategies as per specific clinical scenario.
Design/Methods:
Case report and literature review.
Results:
A 45-year-old male presented with 1 month old history of acute onset numbness of right half of the body with slurring of speech. Computed tomography angiography showed complete occlusion of left cervical ICA just beyond origin with presence of fusiform dilatation and spiral flap in right extracranial cervical ICA. The patient was started on antiplatelets and taken for endovascular procedure using 2-mesh-based carotid stents. Patient was discharged after 3 days on antiplatelet therapy. At 1-year follow-up, there were no fresh symptoms.
Conclusion:
This case emphasizes the role of successful endovascular management of carotid dissection in a young male. These clinical situations may not be fully represented in trials, and a case-based approach is required.
Keywords
Introduction
Carotid dissections (CADs) are a significant cause of stroke in young patients. Previous trials have shown some insight into the optimal management strategies for this subgroup of patients. 1 However, with the advancement in the field of neurointervention, a new domain is opening up for the management of such patients in typical case scenarios. We describe the successful management of a young male with complex internal carotid artery (ICA) dissection.
Case Report
A 45-year-old male presented with 1 month old history of acute onset numbness of right half of body with slurring of speech which lasted for few minutes. He underwent magnetic resonance imaging (MRI) at that time which showed patchy lacunar infarct in left cerebral hemisphere with nonvisualization of left ICA and supply of bilateral cerebral hemispheres from right ICA (Figure 1). There was no history of headache, retroorbital pain, or photopsia. No past history of trauma, hypertension, or diabetes mellitus was present. Patient had history of smoking for last 15 years. In present examination, there was no evidence of limb weakness, cranial nerve palsy, sensory loss, or gait imbalance. His complete hemogram, lipid profile, and coagulation profile were within normal limits. A computed tomography (CT) angiography showed complete occlusion of left cervical ICA just beyond origin with presence of fusiform dilatation and spiral flap in right extracranial cervical ICA (Figure 2). Distal to the dissecting aneurysm, the right ICA was normal and supplying the contralateral hemisphere. He underwent vessel wall MRI as well as clinical work up for vasculitis which was inconclusive. Rest of the workup for connective tissue disorders and fibromuscular dysplasia was inconclusive. The patient was started on Aspirin 300 mg and clopidogrel 75 mg for 1 week and then taken for endovascular procedure using 2-mesh-based carotid stents (CGuardTM EPS stents; InspireMD, Boston, MA) of size 6 × 40 mm and 7 × 40 mm. Immediate postprocedure, there was complete reconstruction of the ICA with nonvisualization of flap and return to normal caliber (Figure 3). No intra- or postprocedure complications were seen. The patient was closely monitored for risk of hyperperfusion syndrome and blood pressure was maintained below 110/70 mm of Hg. Patient was discharged after 3 days on antiplatelet therapy. At 1-year follow-up, there were no fresh symptoms.
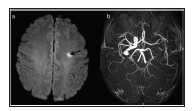
(A) Axial DW image shows presence of small lacunar acute infarct in left frontal lobe (black arrow). (B) MR angiography image shows nonvisualized left ICA and bilateral cerebral hemispheres are supplied by right ICA (white arrow). DW, diffusion-weighted; ICA, internal carotid artery; MR, magnetic resonance.
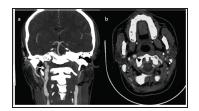
(A) Coronal CT angiography image shows left side abrupt tapering of left ICA (black arrow) with nonvisualized distal ICA suggestive of dissection. Right ICA shows fusiform dissecting aneurysm (white arrow). (A) Axial CT angiography image shows presence of dissecting flap without intramural hematoma. CT, computerized tomography; ICA, internal carotid artery.
(A) Lateral selective ICA preprocedure run shows presence of dissecting fusiform aneurysm with true (white arrow) and false (black arrow) lumens depicted by high frame rate. (B) Lateral selective CCA run postprocedure shows two partially overlapping stents placed resulting in immediate resolution of the flap and return of normal ICA caliber. CCA, common carotid artery; ICA, internal carotid artery.

Discussion
The most significant insight into the treatment for CAD came from the Cervical Artery Dissection in Stroke Study (CADISS) trial, which mentioned that there is very low risk of recurrent stroke after CAD on medical management and there was no significant difference with antiplatelet or anticoagulant therapy. 1 Another important subgroup analysis published from the CADISS trial involving the dissecting carotid aneurysms also reinforced that these may follow a benign course and medical management should be followed. 2
However, our case presented with unique clinical challenges which may not be explained by the study population in CADISS. First thing was that there was bilateral CAD, with symptomatic side already having complete occlusion and asymptomatic side had dissecting fusiform aneurysm with spiral flap.
To evaluate the most appropriate strategy in such scenario, we will have to see the results of CADISS trial and previously published literature in detail. In the CADISS trial, the proportion of patients with bilateral dissection was very few. Also, there was no mention of any clinical scenario with bilateral dissection with complete occlusion on one side. The extent of dissection, aneurysm type, for example, fusiform or saccular and flap morphology was also not mentioned in detail. 1
In their results, it was seen that resolution rate was higher in patients imaged shortly after presentation and was also found lower in asymptomatic dissecting aneurysm. 2 Other subgroup multivariate analysis showed that only age and presence of intramural hematoma were associated with recanalization on follow-up. There was no association of use of any type of medical therapy with recanalization. 1
In another study involving dissecting aneurysms, it was found that none of the aneurysms located on the asymptomatic side had disappeared on a 3-year follow-up. 3 Another study found that reduction in size of dissecting aneurysms was seen mainly in small saccular dissecting aneurysms. 4
It has been stated that the CADISS trial was underpowered and also several meta-analyses have reported much higher stroke rates in CAD than stated in CADISS, thus making it important to look for an alternative intervention strategies. 5
A published meta-analysis has already established the feasibility of stenting in extracranial dissections and shown 99% technical success, very low complication rate, and no new neurological deficit over a 2-year follow-up. 6
Our case was a young male who had bilateral dissection, with complete occlusion on symptomatic side and large dissecting aneurysm on asymptomatic site. There was no intramural hematoma, the dissection was extensive and showed aggressive spiral configuration and reaching from near bifurcation to petrous segment of ICA. In light of the knowledge from published literature and our own experience, endovascular stenting was performed with good clinical outcome.
Conservative management with anticoagulants or antiplatelet can be considered in dissecting aneurysms as shown by CADISS trial. However, a situation like this with bilateral dissection, symptomatic side complete occlusion, and asymptomatic side large fusiform aneurysm with spiral aggressive looking dissection will require endovascular management to prevent devastating outcome. A recent study has shown importance of perfusion in deciding endovascular management for CAD. 7
Embolism, thrombus formation, hypoperfusion due to occlusion or flap extension are all important considerations guiding the treatment of CAD for stroke prevention. 7 We would also want to stress on considering the rest of imaging such as disease extent before deciding best clinical course.
Till the time, direct head on comparison trials between medical therapy and endovascular therapy are not available for dissecting aneurysms, the choice has to be made on case-to-case basis in complicated scenarios.
Footnotes
Declaration of Conflicting Interests
Funding
The author received no financial support for the research, authorship, and/or publication of this article.