
Abstract
Patient, 19-year-old male, presented with fever, abdominal pain, headache, and vomiting presented after vaccination with ChAdOx1 CoV-19 (AstraZeneca, University of Oxford, and Serum Institute of India, and adenoviral-based vaccine) with alteration in sensorium and thrombocytopenia. He was diagnosed to have extensive venous sinus thrombosis with mass effect, midline shift, and underwent decompressive hemicraniotomy. He had a good outcome.
Introduction
Vaccine-induced immune thrombotic thrombocytopenia (VITT) is a very rare syndrome (1 case per 26,500 to 1 case per 1,27,300 first doses of AstraZeneca/COVISHIELD administered) 1 associated with COVID-19 vaccines.
Case History
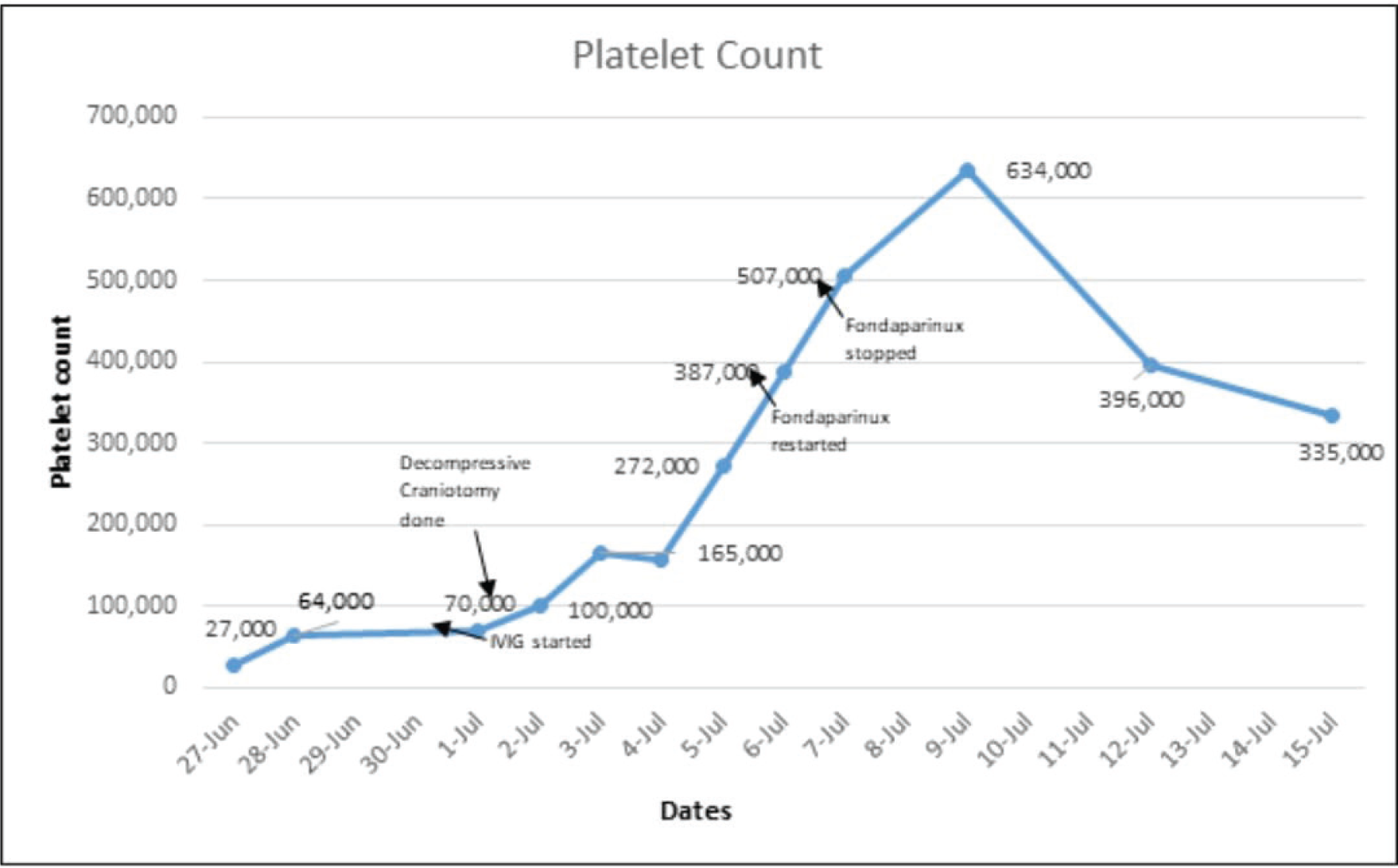
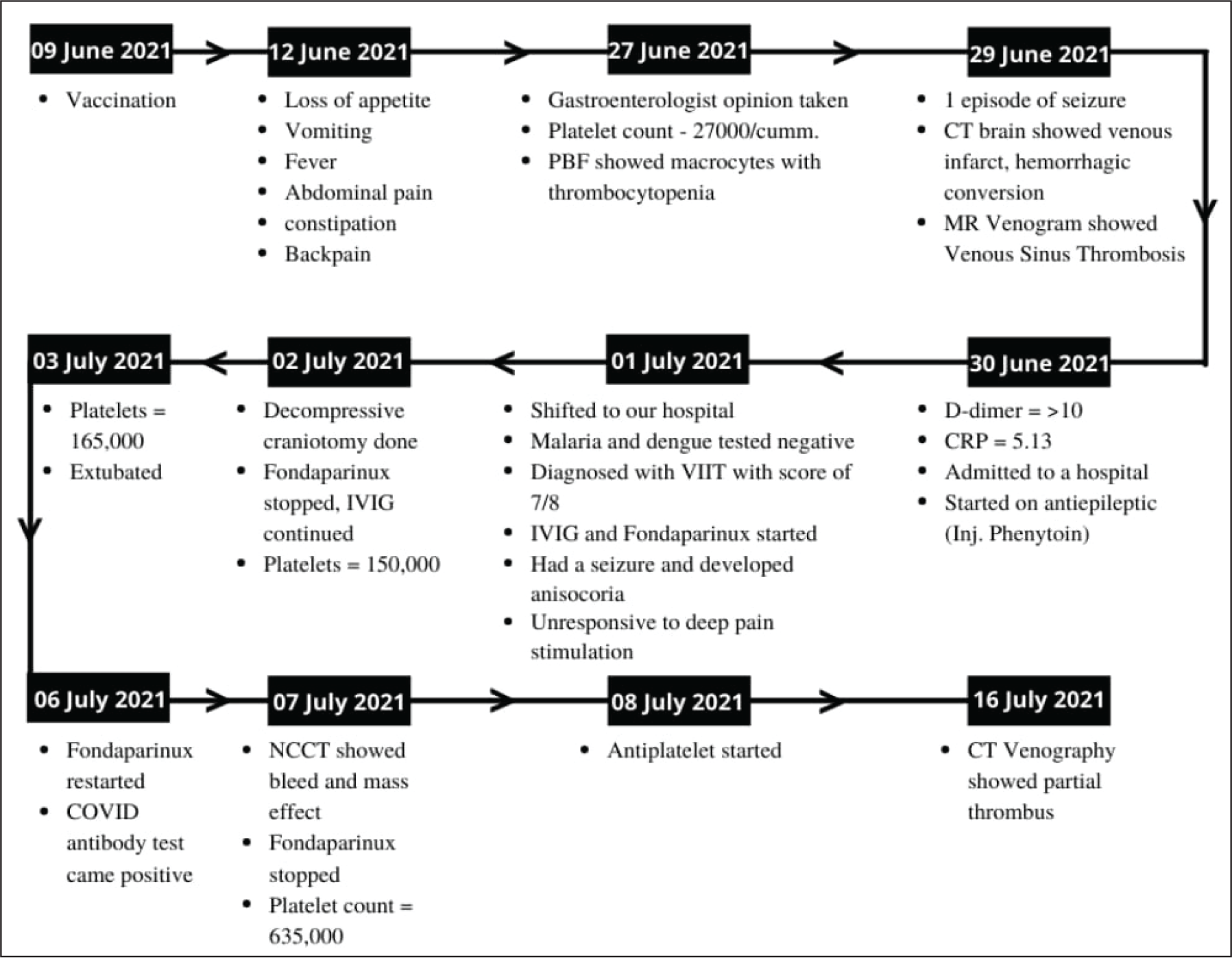
A 19-year-old young male was admitted to our hospital with a history of seizures and alteration in sensorium preceded by fever, abdominal pain, and thrombocytopenia. The patient with no prior morbidity has a history of vaccination on June 9, 2021 with ChAdOx1 CoV-19 vaccine (AstraZeneca, University of Oxford, and Serum Institute of India, an adenoviral vector-based vaccine). Post-vaccination, he initially developed a persistent fever from day 2 onward accompanied by body aches, vomiting, and abdominal pain which was not investigated initially and treated on lines of gastritis at a local dispensary. In view of lack of relief, he consulted a gastroenterologist; when ultrasonography abdomen was found to be unremarkable, liver function test did not show any major abnormality. The platelet count was recorded to be 27,000 (Figure 1). Treatment was continued with antibiotics (levofloxacin, cefixime, ornidazole, and rabeprazole). He continued to worsen and suffered from seizure-related headaches when neurology opinion was taken and noncontrast computed tomography (NCCT) and magnetic resonance venography revealed venous sinus thrombosis of right internal jugular vein, sagittal and transverse sinus.
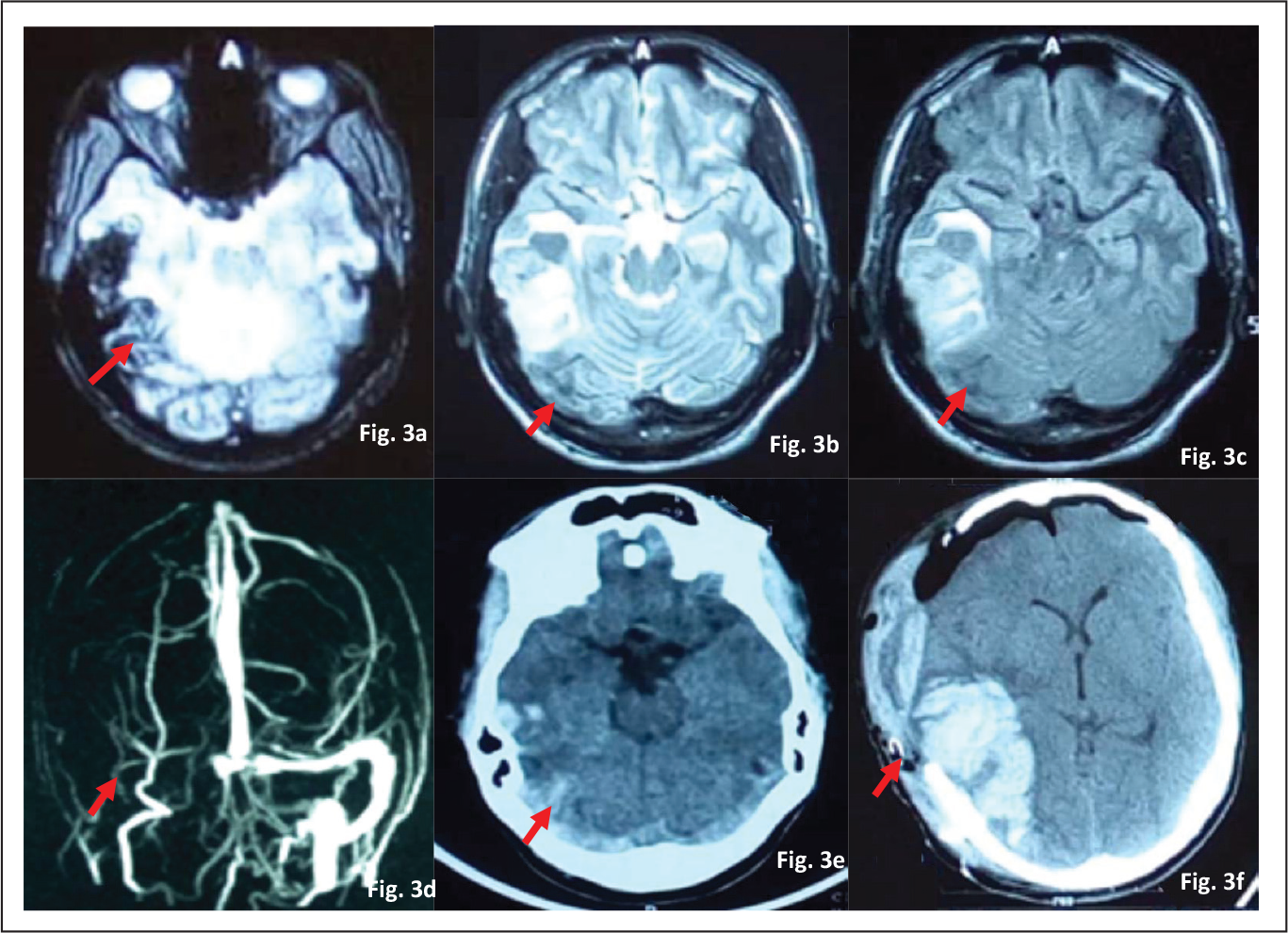
At the time of admission, the patient was dull, drowsy, complaining of persistent abdominal pain without any neck stiffness, or focal neurological deficit. Platelet count was low (70,000), hence considering other differential diagnoses, a workup for dengue and malaria was done and found to be negative. To evaluate further causes of thrombocytopenia, antinuclear antibody test was sent which was negative. There was no underlying malignancies or drug on board causing thrombocytopenia. The 4T score which is a modified score for heparin-induced thrombosis (HIT) for diagnosis of VITT was 7 out of 8 indicating a very high possibility of VITT. Keeping the possibility of VITT, intravenous immunoglobulin (IVIG) was started (Figure 2). On the night of admission to our hospital, patient had an episode of seizure and developed anisocoria. The patient became unresponsive to deep pain stimulation. Urgent magnetic resonance imaging was done which showed worsening of mass effect with midline shift (Figure 3). Neurosurgical consultation was taken and the patient underwent urgent decompressive craniotomy. Patient was started on IVIG and temporary discontinuation of fondaparinux was done. His platelet counts significantly improved on the second day (1,50,000) and third day (1,65,000).
The patient was extubated and restarted on fondaparinux and later switched to dabigatran. NCCT was repeated 32 days’ post-vaccination which did not indicate any significant worsening and midline shift. The patient was switched from intravenous antibiotics to oral antibiotics. The patient was stable, tolerating feed, and able to walk independently. He was finally discharged with optimized medication.
Showing Serial Platelet Count With Timeline
Timeline of Important Clinical Events and Investigations in Our Patient
(a) Axial GRE Image Shows Abnormal Blooming in Right Transverse Sinus and Adjacent Right Temporo Parietal Lobe With Widening of Sinus Consistent With Sinus Thrombosis With Hematoma. (b and c) Axial T2W and Flair Images Shows Absence of Flow Void in Right Transverse and Sigmoid Sinus. (d) Frontal MIP Image From Coronal TOF MRV Shows Lack of Flow in Right Transverse and Sigmoid Sinus. (e) Axial Unenhanced CT Image Shows Area of Abnormal Hyper Attenuation in Right Transverse and Sigmoid Sinus Consistent With CVT. Also Noted Right Temporal Shift With Mild Edema. (f) Axial Unenhanced CT Image Shows Right Front Parietal Craniotomy Defect With Large Intraparenchymal Hematoma and Subgaleal Hemorrhage With Pneumocephalus
Discussion
VITT is a rare clinical syndrome observed in a small number of individuals who have received ChAdox1 CoV-19 and Ad26-Cov2S Vaccine (Johnson & Johnson). Both the vaccines contain an adenoviral vector. Although rare in view of mass vaccination, clinicians need to be aware of this clinical syndrome so that appropriate management can be unveiled. It is caused by immunoglobulin G and antibodies that recognize platelet factors. 2 They cause platelet activation and are not heparin-dependent.3, 4 Thrombus can occur at any site including pulmonary embolism that is adrenal, cerebral, and ophthalmic thrombosis. They are believed to be similar to HIT. Risk factors are unknown but younger age and female gender are found to be affected more. The syndrome begins within 5 to 10 days’ post-vaccination and the syndrome may take a longer time in 1 case (21 days). Although male gender CVT can sometimes be seen, the presence of simultaneous thrombocytopenia and thrombosis at an appropriate time window following vaccination leads to this diagnosis. The typical platelet counts between 10,000 and 1,00,000 with median count 20,000 to 2,50,000/µL. D-dimer was significantly elevated in 1 patient with proven venous sinuous thrombosis and venous infarct.
VITT is caused by antibodies that recognize platelet factor 4 (PF4) bound to platelets. PF4 antibody testing was not done due to the nonavailability of the ELISA PF4 assay. His 4Ts score was 7 out of 8. 5
Due to rapid recognition, IVIG was immediately started, and doing craniotomy in presence of thrombocytopenia was challenging. Heparin was avoided because early reports in which patients were treated with heparins described clinical worsening, including death, and early recommendations were to avoid heparin because of the resemblance of VITT to HIT. Only fondaparinux (x-a inhibitor) and dabigatran were used. The patient had a good outcome complete recovery on follow-up.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.