
Abstract
Background and objective
Amongst the varied neurological manifestations of COVID-19 infection, stroke is one of the common complications. A large portion of patients had large vessel occlusion (LVO) which increases the risk of malignant cerebral infarction requiring decompressive craniectomy. The impact of COVID-19, however, on decompressive craniectomy is not well described. Through this study, we aim to study the impact of decompressive craniectomy in COVID-19 patients presented to our tertiary care hospital.
Material and methods
Data of all acute ischemic stroke patients who tested COVID positive during the study period was collected. From among them, patients requiring decompressive craniectomy were included. The demographic, clinico-radiological parameters related to stroke, treatment received, outcome and complications were noted. In addition, data from all case reports and case series published on patients with COVID-19, who had developed ischemic stroke and underwent decompression craniectomy was collected and systematically reviewed.
Results
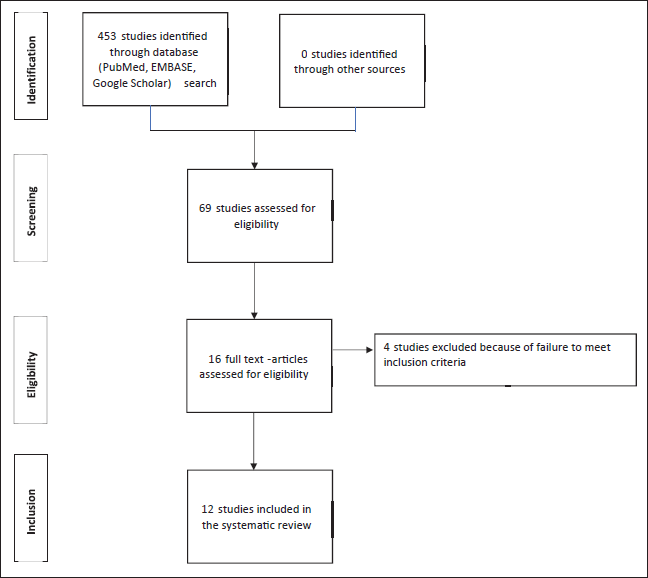
Twenty-seven stroke patients tested positive for COVID-19 infection, out of whom five patients underwent decompression hemicraniectomy in view of neurologic deterioration. The review of literature yielded 453 abstracts. After reading the full text of 69 articles, 12 studies on 15 patients finally met our inclusion criteria and were included in the systematic review. The mortality rate was 40% among stroke patients requiring decompressive craniectomy in COVID-19 patients. The mortality rate and functional outcomes of this cohort are comparable to the pre-pandemic period.
Conclusion
Decompressive craniectomy is a life-saving procedure in COVID-19 patients with malignant infarctions similar to patients in the pre-COVID-19 era.
Keywords
Introduction
The coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a global health emergency. Many papers have been published across different specialities citing the coronavirus as the cause of various systemic manifestations. Similarly, various neurological manifestations have been described by several authors as a manifestation of COVID-19. Amongst the varied manifestations, stroke is one of the common complications that has been described. All forms of stroke including ischemic stroke, intracerebral haemorrhage (ICH) and cortical venous thrombosis (CVT) have been described in association with COVID-19. There has been an increase in number of strokes reported in younger population with no risk factors. A large proportion of these patients had large vessel occlusion (LVO), which increases the risk of malignant cerebral infarction requiring decompressive craniectomy. Decompressive craniectomy is a life-saving procedure and increases the chance of improved functional outcome in malignant infarctions. It is known that COVID-19 worsens the prognosis of stroke; however, the impact of COVID-19 on decompressive craniectomy is not well described. Through this study, we aim to present the impact of decompressive craniectomy in COVID-19 patients presented to our tertiary care hospital.
Methods
This is a retrospective cohort study of patients admitted to the COVID care centre of our hospital during the second wave of the COVID-19 pandemic in India (April 1– June 30, 2021). Data of all the acute ischemic stroke patients presenting to the emergency department during the study period and tested COVID positive through Rapid Antigen Test/ CBNAAT/ RT-PCR test was collected. From among them, patients requiring decompressive craniectomy were included in this study. Demographic details and data regarding the hospital course were retrieved from the institutional records section. Laboratory and radiological data were retrieved from the electronic portals using the patients’ hospital registration number and the following information was collected: demographic characteristics, COVID symptoms, risk factors for stroke, clinical and radiological parameters related to stroke, treatment received, outcome and complications. The study was carried out in accordance with the ICJME guidelines and was approved by our institutional ethics committee (IECPG-07/2021).
Review of literature
A comprehensive literature search was performed using multiple electronic databases – PubMed, Embase and Google Scholar till 26 July 2021 using the following search criteria: (((stroke) AND (COVID)) OR ((stroke) AND (coronavirus))) AND ((((((surgery) OR (decompression)) OR (craniectomy)) OR (decompression craniectomy)) OR (hemicraniectomy)) OR (decompression surgery)).
Inclusion criteria
Studies were included in the systematic review if they met all of the following inclusion criteria: (a) all case reports or case series published on patients with COVID-19, who had developed ischemic stroke and underwent decompression craniectomy; (b) published studies in all languages were included and for those available in other languages, English translated version and/or English version results were sought by contacting the corresponding author twice via email.
Exclusion criteria
Studies were excluded from the systematic review if they met any of the following exclusion criteria: (a) studies conducted on animal subjects; (b) unpublished or preprint studies; (c) case studies with full text not available or not translated to English language.
Data synthesis
Two independent review authors (PS and SG) performed the literature search using the above-mentioned search terms. Full text articles were selected if the abstract suggested the presence of relevant data. The reference lists of the assessed articles were also searched for relevant studies. Inclusion or exclusion of studies was based on uniform decision. Any divergence was resolved through discussion among all authors. The following information was extracted from each eligible study: journal name, first author, year of publication, demographic characteristics of the patients including age, sex, clinical and imaging features, laboratory parameters, outcomes and complications.
Statistical analysis
We used descriptive statistics to summarize and visualize the patient data. For categorical variables, we used frequency and calculated proportions using the number of patients with data available as the denominator. Continuous variables were reported as mean ±SD or as median with range respectively for normal and non-normal distributions, whereas categorical variables were presented as counts and percentages. Statistical analyses were performed using Excel.
Results
Current study
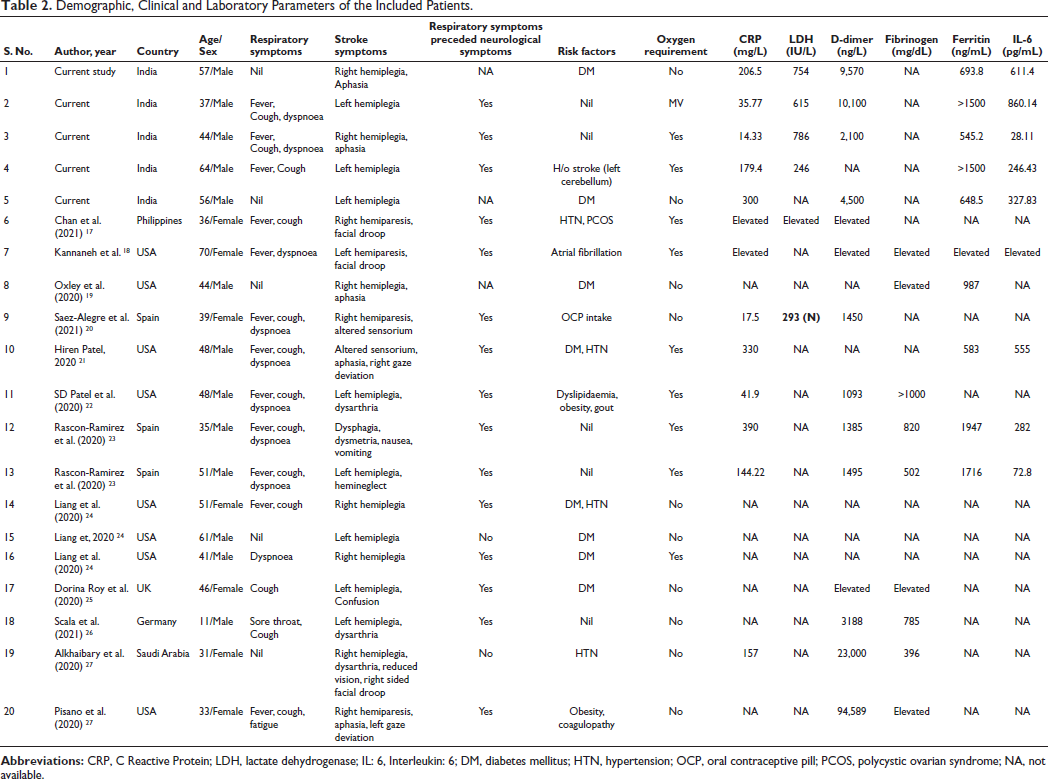
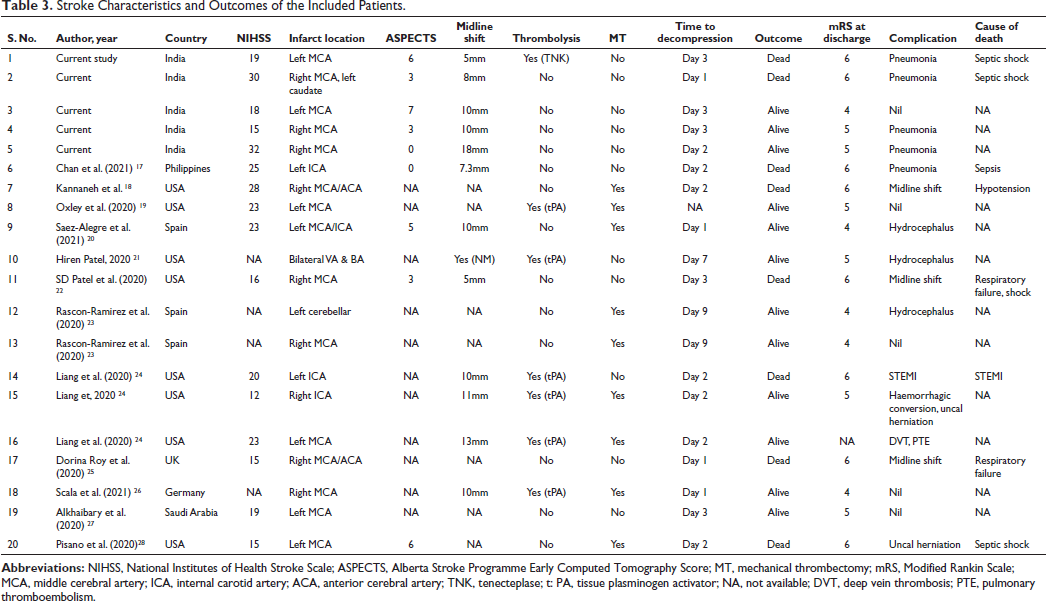
A total of 84 stroke patients (ischemic – 63, haemorrhagic – 20, CVT – 1) presented to the emergency during the study period. Of them, 27 patients (ischemic – 19, haemorrhagic – 8) were tested COVID positive. Among them, 10 patients had large territorial infarcts, out of which five patients underwent decompressive craniectomy. The baseline characteristics of the included patients are summarized in Tables 1 and 2. The median age of the patients was 56 (37-64) years and all patients were male. Out of the five, two patients were asymptomatic for the COVID-19 infection and in the other three patients, respiratory symptoms preceded the stroke. There were no risk factors for stroke in two out of the five patients. One patient required mechanical ventilation at the time of presentation while two patients did not require any oxygen support at the time of admission. Inflammatory markers were significantly elevated in all patients. The MCA was the most common artery involved and the median NIHSS was 19 (15-32). Imaging and outcomes of the included patients are summarized in Table 2. Acute stroke management involved thrombolysis in one patient while none of the patients underwent mechanical thrombectomy. All patients underwent decompression craniectomy within 72 hours from the onset of stroke and the indication of the surgery was neurological deterioration in all five cases. Two out of the five patients died during the hospital course and the cause of death was refractory septic shock with multiple organ dysfunction syndrome.
Systematic search
The search yielded 453 abstracts. After reading the full text of 69 articles, 12 studies containing 15 patients finally met our inclusion criteria and were included in the systematic review (Figure 1 and Tables 1–4). The age of the patients ranged from 11 to 70 (median 44) years and majority were male (n = 8). Stroke was preceded by respiratory illness in all except three patients. There was evidence of systemic inflammation in all patients for whom data was available. There was at least one traditional risk factor for stroke in 12/15 (80%) patients. Stroke involved anterior circulation in all except two patients. The median NIHSS score was 20 (12-28). Acute stroke management included thrombolysis in five patients and mechanical thrombectomy in nine patients. Six patients succumbed during the hospital stay due to various causes. Patients who were alive were functionally dependent at the time of discharge, similar to the patients in our cohort.
The PRISMA Study Flow Diagram.
Characteristics of the Study Population.
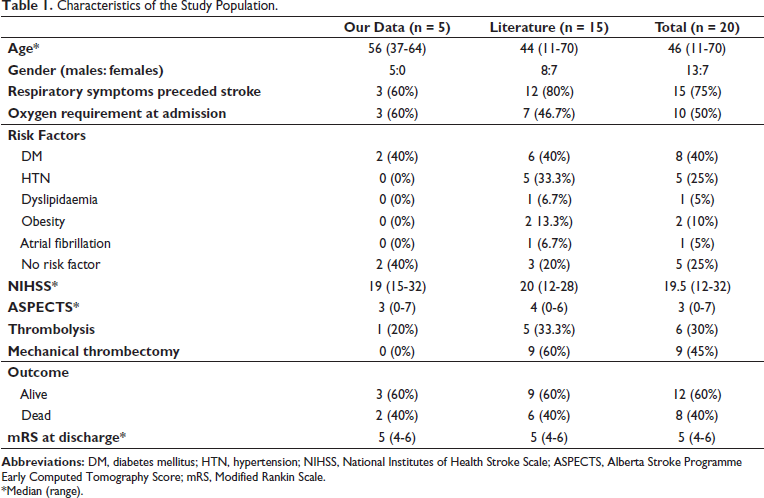
*Median (range).
Demographic, Clinical and Laboratory Parameters of the Included Patients.
Stroke Characteristics and Outcomes of the Included Patients.
Comparison of Data Between Alive and Dead Patients.
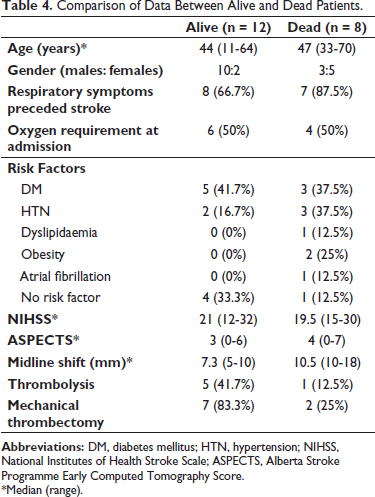
*Median (range).
Discussion
Human coronavirus can penetrate the central nervous system and cause various symptoms. Neurological manifestations were seen in up to 30% of the patients during the COVID-19 pandemic. 1 Stroke is one of the common neurological manifestations described during this pandemic. The incidence of acute ischemic stroke among COVID-19 patients ranged from 0.9% to 2.7% in a meta-analysis. 2 There has been an increase in the number of strokes in COVID-19 patients younger than 50 years and a large proportion of these patients have large vessel occlusion, which predisposes them for malignant cerebral infarction. The median age of strokes in our systematic review was 46 years.
Several theories have been postulated regarding the putative mechanisms behind strokes in these patients. Firstly, COVID-19 patients have elevated serum levels of D-dimer, which is a marker of systemic hypercoagulability and render patients to systemic thrombosis. 3 Secondly, cytokine storm associated with COVID-19 infection results in exaggerated systemic inflammation, which causes disruption of the blood-brain barrier and CNS inflammation.4, 5 Lastly, SARS-Cov-2 virus attaches to ACE-2 receptor and causes its depletion through receptor-mediated endocytosis, which results in endothelial and smooth muscle dysfunction and also promotes vasoconstriction. 6 All these factors lead to a pro-inflammatory and prothrombotic state which can result in stroke in COVID-19 patients. 7 Four patients in our study had no risk factors for stroke and all patients had elevated inflammatory markers and D-dimer, indicating an underlying hypercoagulable and pro-inflammatory state.
The novel SARS-Cov-2 virus wreaked havoc on the global health care and India was at the epicentre of the pandemic from April to June 2021. There were several challenges faced by healthcare workers due to overcrowding of hospitals and collapse of health care system. The resources were diverted to the management of COVID-19 patients, which may have led to under management of non-COVID patients. Although there has been no decrease in stroke admissions during the pandemic period as compared to pre-pandemic period, there has been a decline in the mechanical thrombectomy procedures globally, increased in-hospital complications and mortality. 8 COVID-19 has also challenged the surgical services and training, largely due to deployment of doctors in other areas, adherence to the COVID-19 protocols and reduction in training opportunities due to decrease in number of elective surgeries. 9
Decompression craniectomy in stroke is a life-saving procedure in patients with malignant cerebral infarction. The mortality rate among the general population who underwent decompressive craniectomy for malignant middle cerebral artery infarction ranges from 20% to 55% in recent series, even after receiving the best medical care.10, 11 In contrast, patients who were managed medically had mortality rates as high as 76-80%, suggesting that decompressive craniectomy offers a survival benefit.12, 13 A recent meta-analysis showed that decompressive craniectomy was associated with reduced chance of mortality and increased chance of improved functional outcomes if performed within 48 hours of the onset of stroke. 14 However, there are several challenges in the management of these patients during the COVID-19 pandemic.
Firstly, due to lockdowns and limited number of hospitals managing the non-COVID and especially stroke patients, there is a delay in accessing the health-care services. Majority of these patients have severe COVID-19, requiring intubation and deep coma and/or paralysis which makes it very difficult to monitor for neurological status and hence the surgery may be delayed. Lastly, COVID-19 worsens the prognosis of stroke patients and has also been shown to increase the mortality rate associated with stroke. 15 GlobalSurg reported a 30-day perioperative mortality of 23.8% amongst COVID-19 patients undergoing emergency or elective surgery. 16 However, the data is scarce on such outcomes in COVID-19 patients requiring decompressive craniectomy.
In this study, we found a mortality rate of 40% among stroke patients requiring decompressive craniectomy in COVID-19 patients. Although the mortality rate was similar to pre-COVID era, the most common cause of death was pneumonia and 7/8 patients had died because of non-neurological causes. Although the data is limited and future studies with large sample size may be warranted, it is safe to assume from this study that decompressive craniectomy in COVID-19 patients is a life-saving procedure similar to pre-COVID era and efforts should be maximized in preventing nosocomial infections and pro-thrombotic complications associated with COVID-19.
Limitations
There are several limitations of this study. Firstly, patient numbers were limited due to the relatively short time period observed and scarcity of data in the literature. Secondly, we did not analyse the impact of COVID-19 on excess/neurosurgical mortality due to lack of presentation to hospitals. Lastly, our study did not include a long-term follow up of the patients, which helps in understanding other post-COVID sequelae.
Conclusion
Decompressive craniectomy is a life-saving procedure in COVID-19 patients with malignant infarctions similar to patients in the pre-COVID-19 era. The mortality rate remains the same and it is worthwhile to mention that the cause of mortality is largely due to nosocomial infections and COVID-related hypercoagulability rather than stroke-related complications.