
Abstract
Objective:
To estimate adherence to the Mediterranean diet in a sample of chronic community-dwelling stroke survivors.
Design:
Cross-sectional survey.
Participants:
Convenience sample of 63 chronic (≥6 months) community-dwelling stroke survivors.
Main Outcome Measure:
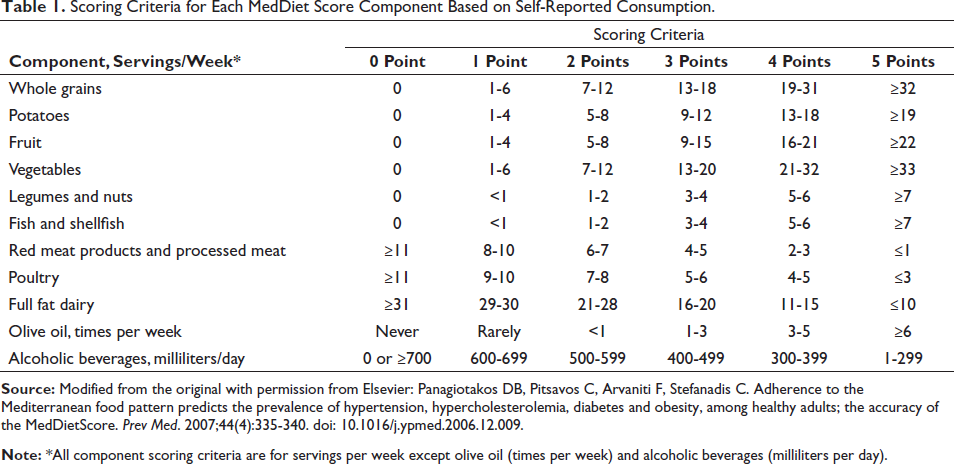
MedDiet Score, a self-report screening tool that measures adherence to the Mediterranean diet based on consumption of 11 dietary components (ie, whole grains, potatoes, fruits, vegetables, legumes and nuts, fish and shellfish, red meat products and processed meat, poultry, full fat dairy, olive oil, and alcohol beverages), measured using a 6-point Likert scale (0 = low adherence, 5 = high adherence, max score = 55).
Results:
The mean MedDiet score was 27.2 ± 4.7; males scored higher than females (28.5 ± 4.9 vs 26.0 ± 4.2, P = .031). Participants reported more adherence for red meat products and processed meat, poultry, and full fat dairy and less adherence for whole grains, potatoes, fruits, vegetables, fish and shellfish, and alcoholic beverages.
Conclusions:
Adherence to the Mediterranean diet, a healthy dietary pattern recommended for secondary stroke prevention, was moderate in this sample of stroke survivors, and results were consistent with previous research on quality of dietary intake. Findings indicate the need for effective dietary interventions for stroke survivors to improve cardiometabolic health and reduce recurrent stroke risk.
Keywords
Introduction
Stroke survivors experience increased risk for recurrent stroke and poor cardiometabolic health. 1 Stroke recurrence is associated with increased mortality and disability; 2 thus, secondary stroke prevention is essential for this population. The American Heart Association recommends following a healthy dietary pattern, such as the Mediterranean diet, which includes the consumption of fruits, vegetables, legumes, whole grains, fish, and monounsaturated fats (ie, olive oil, nuts) to reduce cardiovascular disease and recurrent stroke risk. 1 As demonstrated by the PREDIMED study, adherence to a Mediterranean diet can improve blood pressure, lipid profiles, and insulin resistance, 3 which is important because cardiovascular risk factors among stroke survivors are prevalent, including hypertension (58%), hypercholesterolemia (47%), and diabetes (23%). 4 Despite the American Heart Association’s recommendation, the majority of community-dwelling stroke survivors report poor adherence to a healthy dietary pattern with respect to fruit and vegetable, whole grains, and sodium consumption.4, 5 Additionally, no published report has yet reported on stroke survivor adherence to the Mediterranean diet.
To inform the development of a dietary intervention, we recently conducted an online survey to examine current dietary behaviors (eg, transportation, grocery shopping, meal preparation, cooking, eating healthily) among chronic community-dwelling stroke survivors (publication forthcoming). We also queried dietary intake using the MedDiet Score6, 7, a screening tool to estimate adherence to the Mediterranean diet. For this report, we examined MedDiet scores and explored participant characteristics associated with MedDiet scores. Consistent with prior research findings regarding poor diet, we hypothesized that MedDiet scores would be low.
Methods
This cross-sectional study consisted of an online survey exploring dietary behaviors among chronic (ie, ≥6 months) community-dwelling stroke survivors. The study was deemed exempt by the University of Utah (Salt Lake City, Utah, USA) Institutional Review Board due to the exclusive use of survey procedures (IRB reference number: 00146762). A convenience sample of 63 participants was recruited between November 2021 and February 2022 from 201 community-based support groups identified through the American Heart Association Online Stroke Group Finder website (
The online survey was hosted on a HIPAA-secure Qualtrics platform (Qualtrics International; Seattle, WA, USA). Prior to beginning the survey, potential participants were presented with a description of the survey, eligibility criteria, and a statement explaining that completion of the survey implied consent to voluntarily participate in the study. Participants were eligible if they lived in the community, were ≥6 months post-stroke, aged 30 to 70 years, had a modified Rankin score ≤3 indicating absent to moderate disability, and had absent to mild aphasia and cognitive impairment (self-reported). All data were self-reported.
Participants provided demographic information and answered questions on dietary behaviors, results of which are reported elsewhere (publication forthcoming). The online survey did not collect any clinical information (eg, past medical history, stroke etiology, treatment, discharge education). Participants also completed the MedDiet Score, a valid and reliable screening tool developed for use in the general population that estimates adherence to the Mediterranean diet by quantifying weekly consumption of 11 dietary components: whole grains, potatoes, fruits, vegetables, legumes and nuts, fish and shellfish, red meat products and processed meat, poultry, full fat dairy, olive oil, and alcoholic beverages. For each component, adherence to the Mediterranean diet is ranked on a 6-point Likert scale (0 = low adherence, 5 = high adherence, see Table 1 for scoring criteria). 6 Scores for each item are summed to obtain a MedDiet score (max = 55). The MedDiet score is predictive of cardiovascular disease risk. 7
Scoring Criteria for Each MedDiet Score Component Based on Self-Reported Consumption.
Data analysis was completed using IBM SPSS Statistics Version 28 (IBM Corp., Armonk, NY). We computed the MedDiet total score and individual component scores across participants. We also examined the association of participant characteristics with the total score using 1-way ANOVAs and Pearson correlations.
Results
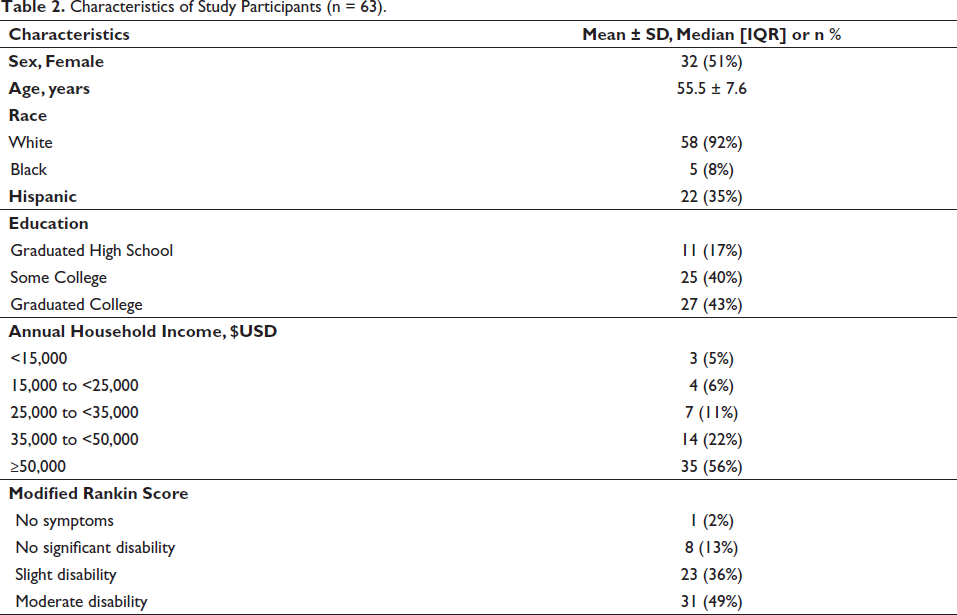
One-hundred thirty surveys were initiated but only 63 were completed. Demographic characteristics of the 63 study participants include 55.5 ± 7.6 years, 51% male, 92% white, 35% Hispanic, 43% graduated college, and 56% had an annual household income ≥$50,000 USD. Per the modified Rankin score, participants reported moderate disability (49%), slight disability (36%), no significant disability (13%), and no symptoms (2%). Detailed participant characteristics are displayed in Table 2.
Characteristics of Study Participants (n = 63).
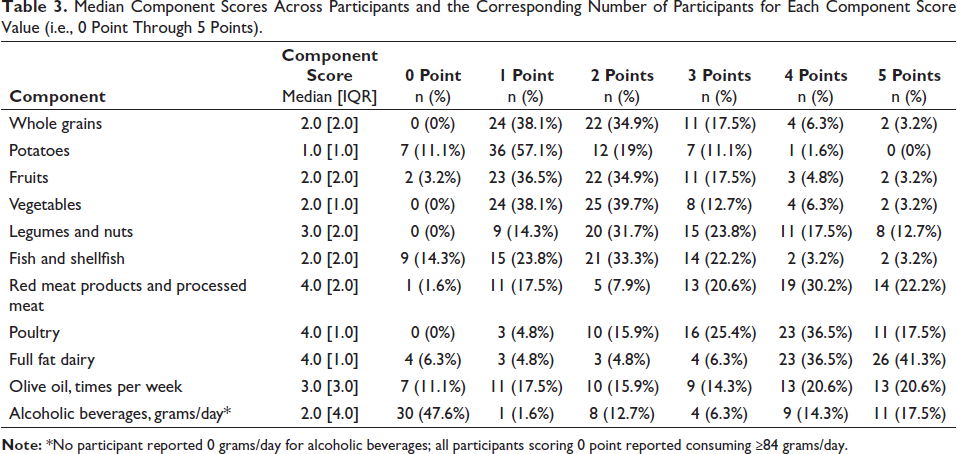
The mean MedDiet total score was 27.2 ± 4.7 (max = 55), which corresponds to 49% adherence (ie, 27.2/55) to the Mediterranean diet based on the MedDiet score. There was no association between the MedDiet total score and any participant characteristic except sex; males scored 2.5 points higher than females (males: 28.5 ± 4.9, females: 26.0 ± 4.2, P = .031). Individual MedDiet component scores are displayed in Table 3 and show that adherence to the Mediterranean diet was highest (ie, limited consumption) for red meat products and processed meat, poultry, and full fat dairy, and least compliant (ie, insufficient consumption) for whole grains, potatoes, fruits, vegetables, fish and shellfish, and alcoholic beverages.
Median Component Scores Across Participants and the Corresponding Number of Participants for Each Component Score Value (i.e., 0 Point Through 5 Points).
Discussion
Results indicate that this sample of community-dwelling stroke survivors reported moderate adherence (ie, 49%) to the Mediterranean diet as quantified by frequency of self-reported consumption of 11 distinct dietary components. A MedDiet Score of 27 is consistent with a Framingham 10-year Coronary Heart Disease Risk Score of up to 6% for females and up to 11% for males. 7 Although this risk may be slightly attenuated for males because they had higher MedDiet Scores than females, there remains room for improvement in the consumption of foods consistent with a healthy dietary pattern to reduce risk of recurrent stroke as recommended by the American Heart Association. 1 Despite recommendations to follow a healthy dietary pattern, only 22% of stroke survivors report consuming an “ideal” diet with respect to fruits and vegetables, whole grains, and sodium, 5 and mixed results have been reported for interventions seeking to improving dietary intake in community-dwelling stroke survivors. 8 Thus, effective dietary interventions for stroke survivors need to be developed and tested. 9
Study Limitations
Several limitations are inherent to this study. First, dietary intake was self-reported; dietary intake is frequently underreported 10 and accuracy may be further complicated by post-stroke cognitive impairment. Second, the study sample included a majority of white, non-Hispanic, middle-aged, chronic community-dwelling stroke survivors with no more than moderate disability; thus, findings may not generalize to other racial/ethnic groups, institutionalized stroke-survivors, and survivors experiencing more than moderate disability. Third, the online survey did not query information on cultural backgrounds, vascular risk factors, or stroke etiology; thus, the presence of selection bias and the effect of unknown factors (eg, cultural food preferences, stroke type) on dietary intake cannot be determined. Fourth, participants were not asked if they received dietary education as part of their inpatient or outpatient stroke care; receipt of such education could influence post-stroke dietary intake and bias results.
Lastly, the choice of the outcome measure, the MedDiet Score, should be taken into consideration. In addition to the MedDiet Score used in this study, numerous indices of adherence to the Mediterranean diet exist, including the Mediterranean Diet Scale, the Mediterranean Food Pattern, the Mediterranean Diet Score, and the Short Mediterranean Diet Questionnaire (see Aoun et al 11 for a comparison of these indices). 11 Across all indices, there is a lack of uniformity in the included dietary components and serving size cut-offs; thus, had a different outcome measure been used in this study, the results may have differed. Our choice to use the MedDiet score was based on its ability to predict cardiovascular disease risk validated against the Framingham Risk score 7 and because it offers six ordinal response categories for each dietary component rather than dichotomous “adherent/non-adherent” categories, which allows for more variability in participant responses. Because the MedDiet Score has not been validated in stroke survivors, its validity and reliability in this population should be validated against an objective measure of energy intake (ie, doubly labeled water) or against the gold-standard 24-Hour Dietary Recall.
Conclusions
This sample of chronic community-dwelling stroke survivors reported only moderate adherence to the Mediterranean diet, a healthy dietary pattern recommended for stroke survivors. 1 Findings indicate an increased need for dietary intervention among stroke survivors to improve cardiometabolic health and reduce recurrent stroke risk.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.