
Abstract
Background and Purpose
To evaluate the role of the double stent retriever (SR) technique in mechanical thrombectomy (MT) for acute ischemic stroke with bifurcation occlusions and long thrombi on magnetic resonance imaging (MRI).
Methods
The retrospective observational study was conducted between February 2023 and September 2024 on acute ischemic stroke patients with anterior circulation large vessel occlusion who underwent MT with multiple SRs. Technical success was defined as successful recanalization (mTICI ≥ 2b) without additional techniques. The primary efficacy outcome was an independent functional status (modified Rankin score 0-2) at 90 days.
Results
Sixteen patients (median age [IQR], 58.5 [47.5-67] years; males, 12/16 [75%]) underwent MT with the double SR technique. SRs were deployed into both middle cerebral artery (MCA) divisions (8/16, 50%), anterior cerebral artery and MCA (3/16, 18.8%), one division of MCA in parallel (2/16, 12.5%), M1 and M2 segments of the MCA in series (1/16, 6.3%), or internal carotid artery (ICA) and MCA in series (1/16, 6.3%). In one case, three SRs were deployed in series in the ICA and MCA. The first pass recanalization rate with the double SR technique was 60% (6/10). The technical success rate was 62.5% (10/16), and the final recanalization rate was 81.3% (13/16). Eight patients (50%) had independent functional status at 90 days, while two (12.5%) had symptomatic intracranial hemorrhage.
Conclusion
The double SR technique has a moderately high recanalization rate in patients with acute ischemic stroke when the thrombus is long or involves the ICA or MCA bifurcation on MRI.
Introduction
Acute ischemic stroke is a cause of significant morbidity and mortality, affecting 12 million people worldwide each year. 1 Large vessel occlusion is observed in one-third of the cases of acute ischemic stroke. 2 Prompt revascularization is essential in these cases to ensure a good clinical outcome. With results from multiple large trials proving its efficacy and safety, mechanical thrombectomy (MT) has become the standard of care for acute ischemic stroke with large vessel occlusion. 3 Of note, retrieval of the clot in the first attempt of MT, called the “first pass effect,” is an independent predictor of a good functional outcome. 4
Multiple techniques are employed for MT by practitioners worldwide, using aspiration catheters, stent retrievers (SRs), or a combination of both. However, successful recanalization may not be achieved in 16%-24% of cases using conventional techniques,5, 6 and failed recanalization is associated with poor functional outcomes. 7 Clot retrieval becomes challenging in specific scenarios, such as occlusions involving bifurcation points, where the deployment of the SR in one of the branches may fail to recanalize the other branch. Detection of the involvement of the bifurcation point by the thrombus on baseline imaging is, therefore, crucial for planning the technique of MT. While the involvement of the internal carotid artery (ICA) bifurcation is usually well visualized on computed tomography (CT) angiography and digital subtraction angiography (DSA), ascertaining whether the thrombus involves the bifurcation point in the middle cerebral artery (MCA) occlusion is challenging due to the non-visualization of the distal extent of the thrombus in these imaging modalities. Magnetic resonance imaging (MRI) is helpful in such cases, as blooming on susceptibility-weighted imaging (SWI) helps in determining the location and length of the clot. Simultaneous deployment of SRs into each branch can be used as a rescue strategy in clots involving the bifurcation points.8-12 Another scenario in which the conventional MT techniques may fail is when the clot is longer than the available SRs, as it may disintegrate during retrieval. Such long clots can be identified on SWI, and the deployment of multiple SRs in series may help achieve successful recanalization in such cases. However, the use of multiple SRs may have disadvantages, including a higher risk of intimal injury and increased cost.
While the efficacy of the double SR technique has been assessed in a few studies,13, 14 the role of MRI-guided patient selection remains to be studied. This study aimed to evaluate the efficacy and safety of the double SR technique in MT for large vessel occlusion with bifurcation occlusions and long thrombi, guided by the assessment of clot location and extent on MRI.
Materials and Methods
This retrospective observational study was conducted after obtaining approval from the Institutional Ethics Committee with a waiver of written informed consent. Consecutive patients with acute ischemic stroke who underwent MT using the double SR technique between January 2023 and December 2024 were included in the study. The inclusion criteria were an anterior circulation territory acute ischemic infarct with large vessel occlusion presenting within 24 h of onset, an Alberta Stroke Program Early CT Score (ASPECTS) of six or higher, a National Institutes of Health Stroke Scale (NIHSS) score of six or higher, and a perfusion-core or clinical-core mismatch. 3 Patients with hemorrhagic transformation of the infarct on baseline MRI were excluded.
Clinical Data Collection and Imaging
Detailed patient information was collected from hospital records, including demographic details, presenting complaints, time from onset to arrival, associated comorbidities, and the NIHSS at presentation. MRI was performed on a 3T MRI machine (Skyra, Siemens Healthcare, Erlangen, Germany). The imaging sequences used were diffusion-weighted imaging, 3D time-of-flight (TOF) angiography of the brain and neck, fluid-attenuation inversion recovery, and SWI. The source images of TOF MRI angiography were reviewed to identify large vessel occlusion. Imaging findings on baseline MRI recorded were the ASPECTS score, the site of occlusion, and the presence of blooming on SWI in the artery at the site of occlusion (susceptibility vessel sign). The double SR technique was used in patients with ICA bifurcation occlusion on TOF MRI angiography, MCA bifurcation thrombus extending into both divisions on SWI, and long thrombus involving occupying the entire length of the M1 segment of the MCA and extending into either the terminal ICA or the M2 segment.
Procedure Details
The procedure was performed on a biplane DSA system (Artis Zee, Siemens Healthcare, Erlangen, Germany) under local anesthesia or conscious sedation, unless the patient was unable to obey verbal commands, in which case general anesthesia was used. All MTs were performed by one of the three interventional radiologists with at least 8 years’ experience in neurovascular interventions. Common femoral artery access was taken and secured with an 8F short sheath (Cordis, Florida, USA). An 8F, 70 cm long sheath (Flexor Raabe, Cook Medical, Indiana, USA) was used in the case of ICA occlusions. An 8F guide sheath (Cerebase, Le Locle, Switzerland) was placed in the cervical ICA. An aspiration catheter (React 71, Medtronic, California, USA) was used for the treatment of MCA occlusions. The occlusion was crossed using a microcatheter (Phenom 21, Medtronic, California, USA) and a wire (Traxcess EX, Terumo Neuro, Saint-Germain-en-Laye, France), and SRs (Solitaire, Medtronic, California, USA) were deployed across the occlusion. They were deployed into each branch for bifurcation clots. If the microcatheters could not be negotiated into both branches, the SRs were deployed in parallel in the same branch. In the case of a long clot, the SRs were deployed in series. While 6 × 40 mm SRs were used for the ICA, 4 × 40 mm SRs were used for the M1 and M2 segments of the MCA, and the anterior cerebral artery (ACA). The microcatheters were removed entirely, and continuous suction was applied through the guide sheath and the aspiration catheter, if used, during thrombus retrieval. Rescue techniques used in the event of failed recanalization with the double SR technique were direct aspiration and the Solumbra technique with a single SR. Tirofiban was used in cases of carotid bulb or intracranial atherosclerotic stenosis or distal emboli into cortical branches. An intra-arterial or intravenous bolus of 10 µg/kg tirofiban was administered, followed by an intravenous infusion of 0.1 µg/kg/h. For high-grade stenosis (>70%), angioplasty was done using a coronary balloon (Accuforce, Terumo, Tokyo, Japan) with a diameter of at least 0.25 mm less than the target vessel diameter. Rescue stenting was not required in any of the patients. CT was done 24 h after the procedure or earlier if the patient had a worsening of symptoms to look for new infarcts and hemorrhagic transformation.
Outcome Measures
Technical success was defined as recanalization of the occluded artery with modified treatment in cerebral ischemia (mTICI) score ≥2b, without the use of additional techniques. The first pass recanalization rate when the double SR technique was used for the first pass, and the final successful recanalization (mTICI score ≥2b) rate with or without additional techniques were also noted. The primary efficacy outcome measure was an independent functional status, defined as a modified Rankin score of 0-2 at 90 days after the procedure. The primary safety outcome measure was symptomatic intracranial hemorrhage within 24 h, resulting in a reduction in the NIHSS score by ≥4 points. Secondary safety outcome measures were neurological deterioration with a drop in the NIHSS by ≥4 points, unrelated to intracranial hemorrhage or sedation, distal embolus into the same or different vascular territory, and death within 30 days. Any other procedure-related adverse events were noted and classified according to the Society of Interventional Radiology adverse event classification system. 15
Statistical Analysis
Statistical analysis was done using Stata data analysis software, version 18 (StataCorp, Texas, USA). Categorical variables were reported as frequencies with proportions, and numeric variables were reported as mean ± standard deviation (SD) or median with interquartile range (IQR).
Results
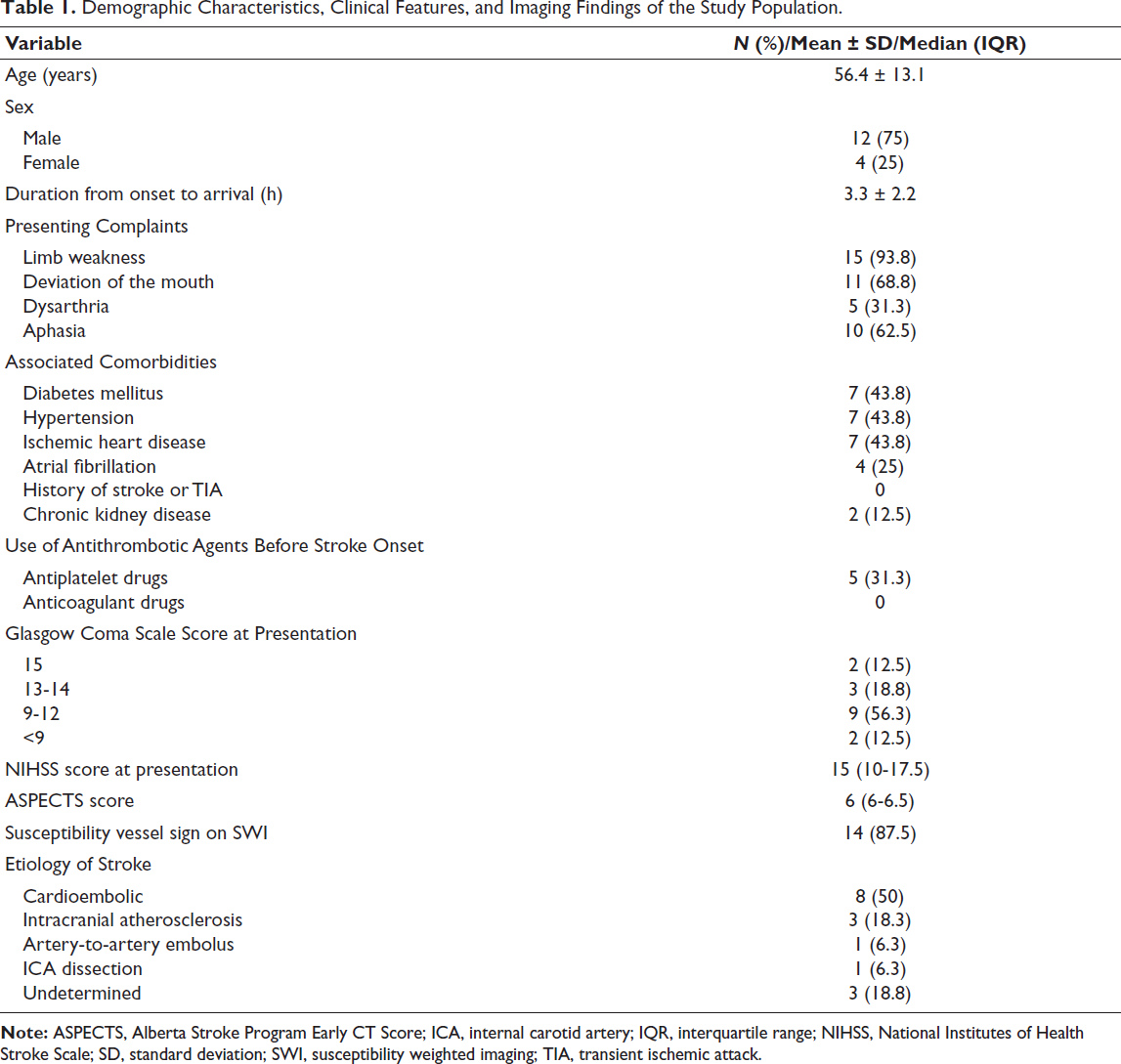
A total of 16 patients underwent MT using the double SR technique during the study period. The demographic characteristics, clinical features, and imaging findings of the study population are mentioned in Table 1. The susceptibility vessel sign was present in all cases except in two with occlusion of the ICA bifurcation. MT was performed under local anesthesia or conscious sedation in 14 patients (87.5%), and general anesthesia was administered for two patients (12.5%). One patient (6.3%) had received intravenous thrombolysis at another center before being transferred to our center for MT. The mean door-to-puncture time was 95.4 ± 38.2 (SD) min. An aspiration catheter was used in four patients (25%).
Demographic Characteristics, Clinical Features, and Imaging Findings of the Study Population.
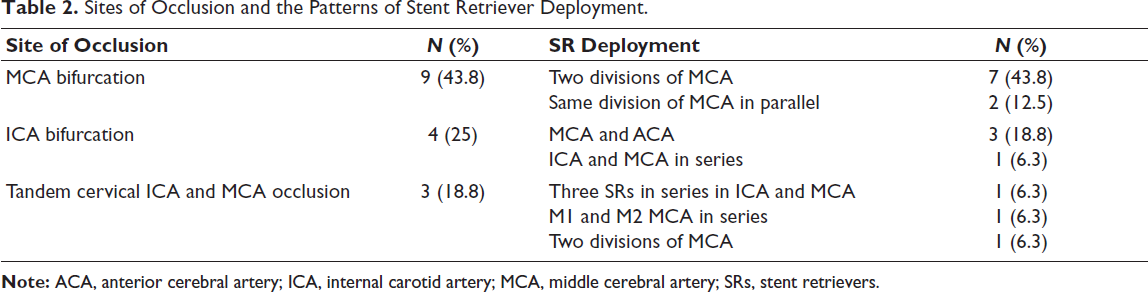
The sites of occlusion and the patterns of SR deployment are described in Table 2. Deployment into the two divisions of the MCA was the most common configuration (Figure 1). In two cases of MCA bifurcation occlusion, the microcatheters could not be advanced into both MCA divisions, and therefore, the SRs were deployed in the same division. In one of these two cases, mTICI 3 recanalization was achieved on the first attempt, whereas no recanalization could be achieved in the other case, despite the use of rescue techniques. In two cases of ICA bifurcation occlusions with an absent susceptibility vessel sign, SRs were deployed into the ACA and MCA. Three SRs were deployed in series in the intracranial ICA and MCA, in a case of a cervical ICA with a long clot extending distally from the site of dissection. In a total of three cases in which the SRs were deployed in series, successful recanalization was achieved in two (66.6%).
Sites of Occlusion and the Patterns of Stent Retriever Deployment.
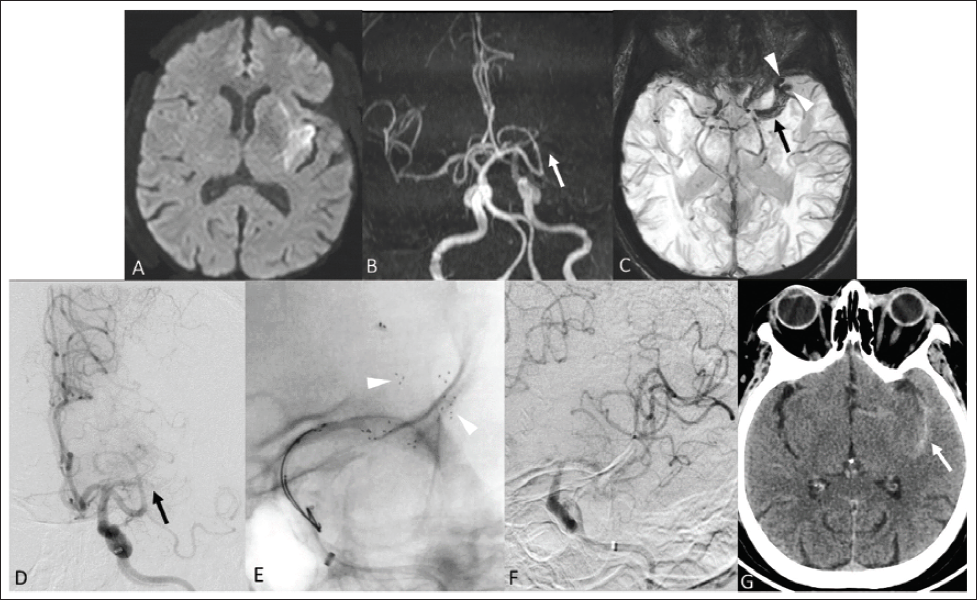
Double Stent Retriever (SR) Technique for Occlusion of the Middle Cerebral Artery (MCA) Bifurcation. (A) Diffusion-weighted Imaging of a 74-year-old Lady Who Presented with Right-sided Weakness and Aphasia for 3 h Showed Acute Infarcts in the Left MCA Territory. (B) Time of Flight Imaging Showed Occlusion of the Left MCA (Arrow). (C) Susceptibility-weighted Imaging Showed Blooming in the M1 Segment of the Left MCA (Arrow) with Extension into Both Its Divisions (Arrowheads). (D) Left Internal Carotid Artery Angiogram Confirmed Occlusion of the Left MCA (Arrow). Following Failed Recanalization After Using the Solumbra Technique with a Single SR, the Double SR Technique was Employed as a Rescue Measure. (E) Fluoroscopy Image Showing Two SRs Deployed in the Two Divisions of the Left MCA (Arrowheads). (F) Angiogram After Thrombectomy with the Double SR Technique Showed Modified Treatment in Cerebral Ischemia (mTICI) 2b Recanalization. (G) Computed Tomography Performed After 24 h Showed a Thin Subarachnoid Hemorrhage in the Left Sylvian Fissure (Arrow) with No New Infarcts or Reperfusion Hemorrhage. The Patient had a Good Functional Outcome with a Modified Rankin Scale Score of 0 at 90 Days.
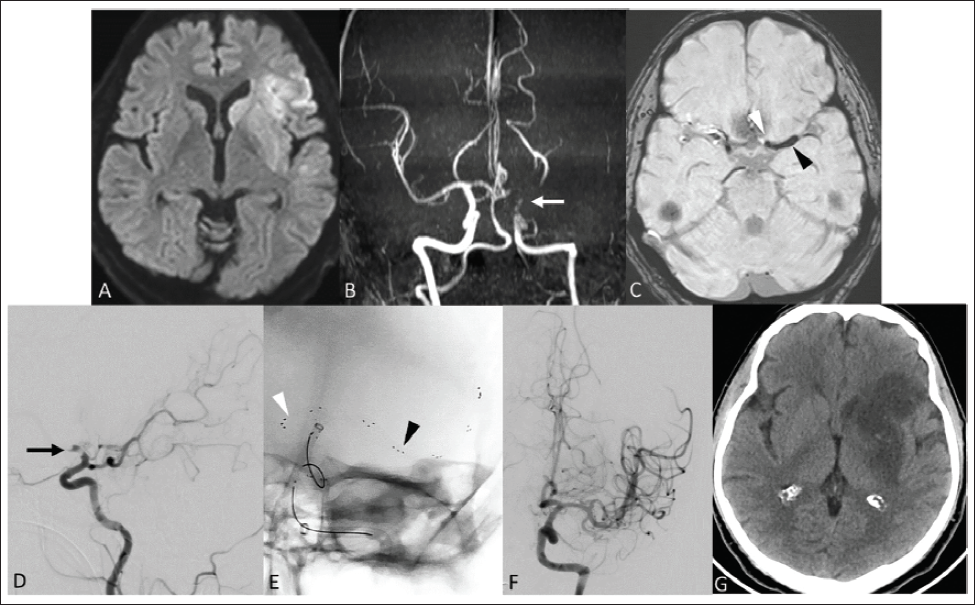
Double Stent Retriever (SR) Technique for Occlusion of the Internal Carotid Artery (ICA) Bifurcation. (A) Diffusion-weighted Imaging of a 39-year-old Man with Right-sided Weakness and Aphasia for 2 h Showed Acute Infarcts in the Left Middle Cerebral Artery (MCA) Territory. (B) Time of Flight Imaging Showed Occlusion of the Left Terminal ICA (Arrow). (C) Susceptibility-weighted Imaging Showed Blooming in the Terminal ICA Extending into the M1 Segment of the Left MCA (Black Arrowhead) and the A1 Segment of the Left Anterior Cerebral Artery (ACA) (White Arrowhead). (D) The Left ICA Angiogram Confirmed Occlusion of the Left Terminal ICA (Arrow). (E) Double SR Technique was Used for the First Pass, with Fluoroscopy Image Showing Two SRs Deployed in the Left MCA and ACA (Arrowheads). (F) Post-thrombectomy Angiogram Showed Modified Treatment in Cerebral Ischemia (mTICI) 3 Recanalization. (G) Computed Tomography Performed After 24 h Showed No New Infarcts or Reperfusion Hemorrhage. The Patient had a Modified Rankin Scale Score of 5 at 90 Days Due to Underlying Severe Congestive Heart Failure.
The double SR technique was used for the first pass in 10 patients, and successful recanalization was achieved in six of them (first pass recanalization rate, 60%) (Figure 2). It was used as a rescue technique in six patients (37.5%). The technical success rate of the double SR technique was 62.5% (10/16). Only one pass was done with the double SR technique in 15 patients (93.8%). Two passes were done with multiple SRs in a patient with occlusion at the MCA bifurcation. Despite two passes, only mTICI 2a recanalization was achieved in this patient. Rescue techniques were required in eight cases (50%) after using the double SR technique. The direct aspiration technique was used in two cases, the Solumbra technique with a single SR in four cases, and both techniques were used in two cases. Tirofiban was administered in eight patients (50%), and angioplasty for carotid bulb or intracranial stenosis was done in three patients (18.8%). The final successful recanalization rate with or without additional techniques was 81.3% (13/16).
The primary efficacy outcome of independent functional status at 90 days was observed in eight patients (50%). Asymptomatic subarachnoid hemorrhage was observed in seven patients (43.8%), while symptomatic intracranial hemorrhage occurred in two patients (12.5%). New infarcts were observed in the 24-h follow-up CT in four patients (25%), out of which two had a successful recanalization. A total of three patients (18.8%) underwent decompressive craniectomy, including two with reperfusion hemorrhage and one with malignant cerebral edema. Four patients (25%) died, of which two had symptomatic intracranial hemorrhage following recanalization, resulting in a procedure-related mortality rate of 12.5%, while two died of ventilator-associated pneumonia and sepsis.
Discussion
MT improves the functional outcome in acute ischemic stroke with large vessel occlusion. 3 While conventional techniques of MT are successful in most patients, their use may fail to recanalize the vessel in certain conditions, such as occlusion at bifurcation points and long clots. While occlusion of the ICA bifurcation is easily visualized on MRI angiography, the extent of the thrombus in isolated or tandem MCA occlusion cannot be determined using MRI angiography alone. Occlusion of the ICA bifurcation can result in pseudo-occlusion in the cervical ICA on MRI angiography due to the slow flow, making it difficult to ascertain the exact location of the thrombus. Similarly, the distal extent of the thrombus into the MCA bifurcation in cases of M1 MCA occlusion cannot be made out on MRI angiography. SWI is helpful in such cases, as the susceptibility vessel sign produced by an erythrocyte-rich thrombus allows for the determination of its location and the vessels involved. In this study, we evaluated the role of the double SR technique in bifurcation occlusions and long thrombi, with patient selection guided by MRI.
In our study, the double SR technique had a moderately high technical success rate of 62.5% and a final recanalization rate of 81.3%. The use of multiple SRs increases the chance of interaction with the clot, resulting in a higher recanalization rate and a lower risk of distal embolism. In the TWIN2WIN randomized controlled trial, which assessed the safety and efficacy of the double SR technique, a significantly higher first-pass recanalization rate of 46% was found compared to 24% with the single SR technique (odds ratio, 2.72 [95% CI, 1.19-6.46]). The final recanalization rate was 84% in the single SR group and 89% in the double SR group in the trial, with no significant difference between them (odds ratio, 1.74 [95% CI, 0.5-5.76]). 13 The recanalization rate with the double SR technique was higher in our study compared to that reported in the trial, likely due to the use of MRI to determine thrombus location and extent, which facilitated better patient selection for the double SR technique. A multicenter prospective study and a meta-analysis of 17 studies have reported high first-pass and final recanalization rates of 72.7%-76.6% and 92.6%-99.5%, respectively, for the double SR technique.14, 16 The incidence of an independent functional outcome in our study was 50%, similar to 46% reported in the meta-analysis of randomized controlled trials on the conventional techniques of MT. 17 Newer dual-layered SRs can potentially have a higher recanalization due to a more effective clot capture mechanism. 18 Whether the double SR technique enhances the recanalization rate in bifurcation occlusions and long thrombi over these newer SRs needs to be evaluated in comparative studies.
In occlusions involving a bifurcation, navigating microcatheters into the different divisions can be challenging due to the lack of direct visualization. We faced this challenge in two patients with MCA bifurcation occlusion, and the SRs were deployed in the same division of the MCA. Although complete recanalization was achieved in one patient, no recanalization was achieved in the other patient, despite the use of rescue techniques. The deployment of two SRs in parallel may increase the chance of retrieving the clot, as it gets sandwiched between the two SRs. 19 However, there is a risk of persistent occlusion or distal embolism in the other division. Using a shallow curve on the microwire and cannulation of the second division after deployment of one SR are potentially useful strategies in such a scenario. 19
In addition to the parallel configuration of double SR deployment in bifurcation occlusions, we evaluated the efficacy of its series configuration for retrieving long clots. Out of the three patients in whom SRs were deployed in series, successful recanalization was achieved in two. To the best of our knowledge, the utility of this technique has not been evaluated in prior studies. The deployment of SRs in series increases the area of contact with the clot, thereby reducing the risk of distal embolism during retrieval.
Subarachnoid hemorrhage was observed in nearly half of our patients, indicating that the high shear force created by the use of multiple SRs results in vessel injury. A study performed by Hernández et al. in a swine model revealed that the occurrence of vessel wall injury is higher with double SR compared to the single SR technique. 20 Nevertheless, the incidence of symptomatic intracranial hemorrhage was only 12.5% in our study, similar to the 10% occurrence observed in the TWIN2WIN trial. 13 It is, however, higher than the incidence of 4.4% reported with the conventional techniques of MT. 17 Therefore, appropriate patient selection is important to avoid unnecessary vessel injury.
The limitations of this study are its retrospective design and small sample size. Case selection based on the susceptibility vessel sign would have excluded cases with non-erythrocyte-rich thrombi that do not show blooming. Direct aspiration through the guide sheath was performed in most cases instead of using an aspiration catheter, which may have adversely affected the recanalization rate. As patients with long clots were very few, definite conclusions cannot be drawn on the efficacy of this technique in this subset of patients. Further comparative studies are needed to determine the benefits of the double SR technique over the conventional Solumbra technique in bifurcation occlusions and long clots.
Conclusion
The double SR technique for MT has a moderately high recanalization rate for acute ischemic stroke with anterior circulation large vessel occlusions, particularly when the thrombus is long or involves bifurcations. Visualization of the location and extent of the thrombus on MRI helps in selecting patients for the double SR technique.
Footnotes
Authors Contribution
Mathew Cherian: Guarantor, conceptualization, methodology, supervision, validation, writing—review and editing.
Santhosh Poyyamoli: Conceptualization, methodology, supervision, validation, writing—review and editing.
Pankaj Mehta: Conceptualization, methodology, supervision, validation, writing—review and editing.
Vishnu Prasad Pulappadi: Data curation, formal analysis, investigation, methodology, writing—original draft.
Data Availability Statement
All relevant data have been included as text and tables in the manuscript
Declaration of Conflicting Interests
The authors declared no conflict of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from Kovai Medical Center and Hospital Ethics Committee, approval letter ref no. EC/AP/1222/06/2025 dated June 6, 2025.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Need for informed consent was waived off by the Institute Ethics Committee because of the retrospective study design.