
Abstract
Background:
The relationship and mechanisms between body mass index (BMI) and cognition are complex and inconclusive. Additionally, the role of neuronal calcium dysfunction, reflected by cerebrospinal fluid (CSF) Visinin-like protein 1 (VILIP-1), in the mechanisms linked with BMI and Alzheimer's disease (AD) has not been investigated.
Objective:
To investigate the relationship between CSF VILIP-1, BMI, and AD pathologies in non-demented elderly at early stages of AD.
Methods:
Baseline CSF AD core biomarkers (amyloid-β42 [Aβ42], phosphorylated tau [P-tau], and total tau [T-tau]) were measured for 1201 non-demented participants, selected from the Alzheimer's Disease Neuroimaging Initiative (ADNI) database, among whom 128 had measurements of CSF VILIP-1. Multivariate linear regression, causal mediation analyses, and linear mixed effects models were conducted to detect these associations.
Results:
The average age of participants was 72.6. CSF VILIP-1 was decreased in A+/TN− (A-positive/T− and N− negative) group and elevated in A−/TN + (A-negative/T− or N-positive) and A+/TN + groups, as compared with A−/TN− group. In total participants, BMI was negatively related to CSF P-tau, T-tau, P-tau/Aβ42 and T-tau/Aβ42. Noticeable associations were also presented between CSF VILIP-1 and AD core biomarkers, but not with Aβ42 after stratification by A/T/N scheme. Furthermore, the influences of BMI on CSF tau pathology were mediated by CSF VILIP-1. Higher baseline CSF VILIP-1 correspond to faster longitudinal cognitive decline.
Conclusions:
Our findings indicated that CSF VILIP-1 changed dynamically and might be a key mediator in the associations between BMI and tau pathology, providing new insights into understanding the mechanisms underlying BMI-related cognitive deficits in non-demented elderly.
Keywords
Introduction
Alzheimer's disease (AD) is characterized by the extracellular accumulation of amyloid-β (Aβ) plaques and intracellular tau neurofibrillary tangles. Neuronal calcium dysfunction has been pinpointed as a notable feature of AD pathologies. 1 Visinin-like protein 1 (VILIP-1), a neuronal Ca2+-sensor protein,2,3 modulates calciumion hemeostasis and multiple Ca2+-dependent cell signaling pathways. 4 It is predominantly expressed in neuronal pericaria, dendrites and some axons, 5 and involved in the regulation of neuronal growth, differentiation, 6 as well as synaptic plasticity. 7 Previous articles provide evidential supports that elevated concentrations of CSF VILIP-1 are closely related to multiple neurological disorders, such as cerebral ischemic infarction, 4 dementia,3,4,7–9 and brain atrophy. 10 Taken together, these findings indicated CSF VILIP-1-related neuronal calcium dysfunction and injury may play a vital role in the progression of AD.
Body mass index (BMI) is regarded as a modifiable risk factor for AD, but its association with cognitive function and its role in the pathogenesis of AD remain controversial and unclear. Multiple epidemiological evidence suggested that higher BMI in midlife was associated with an increased risk of cognitive decline.11,12 Whereas in older adults, the relationship between BMI and cognitive function was more complex and the prevailing perspectives propose that overweight or obesity might serve as a potential protective factor against AD.13–15 Besides, the pathological mechanisms between BMI and AD remain poorly understood. Currently, the widely recognized mechanisms linked with BMI in the progression of AD include metabolism and nutritional supports, 16 inflammation and immune regulation, 17 neuroendocrine changes,18,19 etc. However, to our knowledge, the role of neuronal calcium dysfunction and injury, as reflected by CSF VILIP-1, in the mechanisms linked with BMI and AD pathology and cognition has not been investigated.
Hence, we aimed to (1) ascertain the relationships of CSF VILIP-1 with BMI and AD core biomarkers (Aβ42, phosphorylated tau [P-tau], and total tau [T-tau]) and cognitive function; (2) determine whether CSF VILIP-1 serves as a mediating factor in the correlation between BMI and tau pathology; and (3) explore the predictive value of CSF VILIP-1 in cognitive decline and AD risk.
Methods
Study participants
The study participants were screened from the Alzheimer's Disease Neuroimaging Initiative (ADNI) database. 20 The ADNI was launched in 2003 as a public-private partnership, led by Principal Investigator Michael W. Weiner, MD. The original goal of ADNI was to test whether serial magnetic resonance imaging, positron emission tomography (PET), other biological markers, and clinical and neuropsychological assessment can be combined to measure the progression of mild cognitive impairment (MCI) and early AD. The current goals include validating biomarkers for clinical trials, improving the generalizability of ADNI data by increasing diversity in the participant cohort, and to provide data concerning the diagnosis and progression of Alzheimer's disease to the scientific community. For up-to-date information, see https://adni.loni.usc.edu/. The detailed inclusion and exclusion criteria in ADNI are available at https://adni.loni.usc.edu/. ADNI has received approval from the institutional review board of all participating centers, and written informed consent was obtained from all participants or their authorized relatives.
Participants lacking data of CSF biomarker and those with data 3 standard deviations (SDs) greater or smaller than the mean value were excluded. To study the early stages of AD, we also excluded demented participants. Ultimately, a sum of 1201 participants with baseline CSF AD core biomarkers and longitudinal scores of cognitive performance were selected from the ADNI database. Among these, 76 individuals with MCI (Mini-Mental State Examination [MMSE] > 24, Clinical Dementia Rating Sum of Boxes [CDR] = 0.5) and 52 cognitively normal individuals (CNs, MMSE > 24, CDR = 0) had available CSF VILIP-1 data to mediation analyses (refer to Supplemental Figure 1 for a detailed explanation of the sample selection process).
CSF measurements of VILIP-1 and AD core biomarkers
CSF procedural protocols in ADNI have been described in previous published literature. 21 A sandwich ELISA was approached utilizing the Erenna® immunoassay system for the detection of CSF VILIP-1. 22 CSF Aβ42, P-tau, and T-tau were detected using Roche automated immunoassay platform (Cobase601) and immunoassay reagents, as described previously.23,24 The measurements of all CSF biomarkers were duplicated, and the mean values were calculated. The interbatch coefficients of variation were 15%. The original data mentioned above and detailed assay protocols are accessible in the ADNI database.
Cognitive assessments
Cognitive function was evaluated through a range of scales. According to the neuropsychological batteries, specific cognitive tests for memory (MEM), executive function (EXF) and language (LAN) were developed and used to reflect cognitive domains.25–27 In detail, EXF measures encompass Category Fluency, WAIS-R Digit Symbol, Trails A and B, Digit Span Backwards, and clock drawing. MEM measures encompass relevant items of the Rey Auditory Verbal Learning Test, ADAS, Logical Memory, and MMSE. LAN measures encompass Boston Naming Test, the Animal Fluency test, and the naming portion of AD Assessment Scale-Cog. AD Assessment Scale 13-item cognitive subscale (ADAS13) 28 and MMSE 29 were employed to reflect the global cognitive function. Obviously, higher ADAS 13 scores and lower MEM, EF, LAN, and MMSE scores indicate worse cognitive function.
The A/T/N classification methods
Based on the A/T/N scheme 30 proposed by National Institute on Aging and Alzheimer's Association criteria in 2018, 31 “A+” was defined as CSF Aβ42 concentrations <977 pg/ml, while “T +" was defined as CSF P-tau concentrations >22 pg/ml, and “N+” was defined as CSF T-tau concentrations >245 pg/ml in this study. 32 It has been demonstrated that the establishment of these cutoff values for CSF biomarkers exhibits strong agreement with the PET classification in ADNI. 23 We combined T and N groups together for statistical convenience due to their high correlation, thus generating the TN group: “TN+“ denotes either T+or N+, and “TN−” signifies both T− and N−.32,33
Statistical analyses
First, Chi-square tests were utilized for categorical variables, while Mann-Whitney U tests were applied for continuous variables to examine inter-group variations in baseline characteristics. Skewed data of CSF biomarkers were transformed to achieve or approximate a normal distribution (p < 0.05 by the Kolmogorov-Smirnov test) using the “car” package in R software.
Analysis of covariance (ANCOVA) was approached to evaluate the difference in CSF VILIP-1 levels across the four biological groups, with subsequent Bonferroni correction conducted. Multiple linear regressions (MLR) were conducted to investigate interrelationships of BMI with CSF biomarkers and cognitive function, with adjustments for covariates (including sex, age, education, and APOE ε4 carrier status) in whole cohort. Moreover, Exploratory analyses were conducted within subgroups based on sex, APOE ε4 carrier status (non-carriers versus carriers), cognitive status (CN versus MCI), and four A/TN groups to exam the aforementioned interrelationships.
Following the methodology proposed by Baron and Kenny, 34 mediation analyses were performed to ascertain whether CSF VILIP-1 (the mediator) could mediate the correlation between BMI and CSF AD biomarkers and cognitive function. Significance was assessed through 10,000 bootstrap resamples, and the direct and indirect effects, as well as the proportion mediated were estimated accordingly. The same covariates included in the previous MLR models were also adjusted within each path of the mediation models. Sensitivity analyses were also conducted by constructing various MLR models with adjusting more potential confounding factors, including depression, anxiety, hypertension, DM2, smoking and stroke.
Linear mixed effects (LME) models were conducted to identify whether the baseline level of CSF VILIP-1 could predict longitudinal changes in cognitive function. These LME models were created using cognitive scores as dependent variables. Time since baseline (years), VILIP-1, and their interaction were included as fixed effects. Age, sex, education, APOE ε4 status, and their interactions with time were included as covariates. Finally, influence of BMI and CSF VILIP-1 on the risk of incident AD were detected with the method of Kaplan-Meier.
A two-sided p-value below 0.05 was deemed statistically significant. Data analyses and graphical representation were conducted utilizing R version 4.4.1 and GraphPad Prism 9.00 software.
Results
Baseline participants characteristics
The detailed demographic features, cognitive scores and CSF biomarker levels stratified by cognitive status were showed in Table 1 and Supplemental Table 1. A cohort with a total of 1201 non-demented participants (51.9% males, 72.6 ± 7.0 years, Supplemental Table 1) were selected, among whom 128 participants (64.8% males, 75.2 ± 6.1 years, Table 1) with CSF VILIP-1 data available were incorporated into the mediation analysis.
Characteristics of participants with available CSF VILIP-1 data.
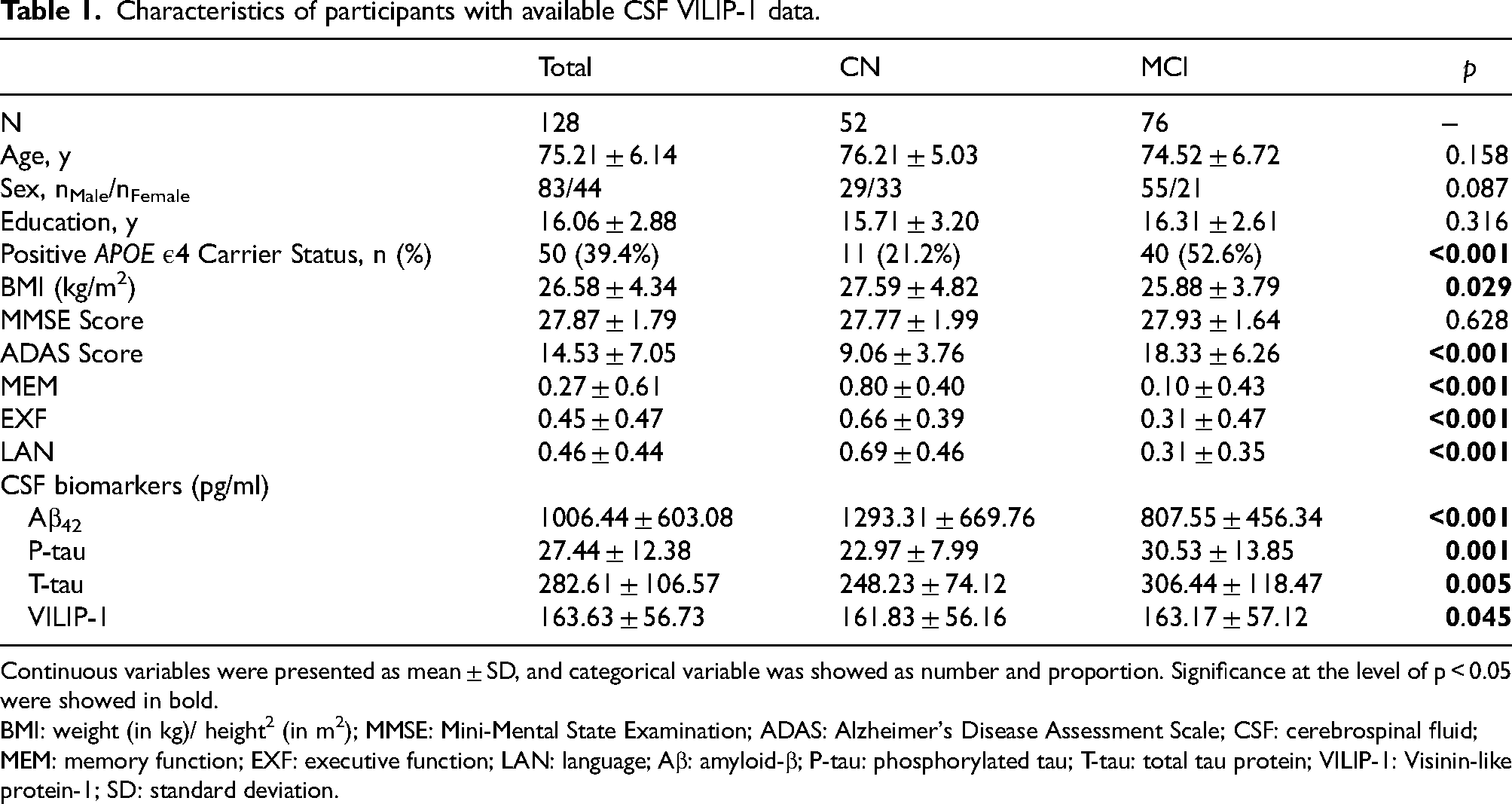
Continuous variables were presented as mean ± SD, and categorical variable was showed as number and proportion. Significance at the level of p < 0.05 were showed in bold.
BMI: weight (in kg)/ height2 (in m2); MMSE: Mini-Mental State Examination; ADAS: Alzheimer's Disease Assessment Scale; CSF: cerebrospinal fluid; MEM: memory function; EXF: executive function; LAN: language; Aβ: amyloid-β; P-tau: phosphorylated tau; T-tau: total tau protein; VILIP-1: Visinin-like protein-1; SD: standard deviation.
CSF VILIP-1 levels in different biological stages of AD
Participants were categorized into four biological groups based on the A/T/N framework. In order to evaluate the correlation between CSF VILIP-1 and AD pathologies, we first explored the variations in CSF VILIP-1 concentrations and found significant disparities among the four groups (p = 7.7 × 10−15, Figure 1). Specifically, A+/TN− (n = 20) had the significantly lower levels of CSF VILIP-1 compared to the A−/TN− group (n = 27) (p < 0.001), whereas the A−/TN + (n = 23) revealed a significant increase (p < 0.0001), followed by A+/TN + group (n = 58) (p < 0.001). However, the results did not unveil notable difference between the A−/TN + and the A+/TN + group (p > 0.05).

Dynamic changes of CSF VILIP-1 in the preclinical phase of AD stratified by A/T/N criteria.
Associations between BMI and CSF AD core biomarkers and cognitive function
In all participants, MLR models showed that continuous BMI variables were negatively correlated with the concentration of CSF P-tau (β = −0.29, p = 3.76 × 10−5), T-tau (β = −2.51, p = 8.53 × 10−5), P-tau/Aβ42 (β = −6.51 × 10−4, p = 3.39 × 10−6), and T-tau/Aβ42 (β = −5.60 × 10−3, p = 2.71 × 10−6), but the positive association with CSF Aβ42 was at the threshold of significance (β = 6.31, p = 0.059) after controlling for aforementioned covariates (Figure 2 and Supplemental Table 2A). Subgroup analyses (stratified by cognitive diagnosis, gender or APOE ε4 carrier status) indicated that positive relationships of continuous BMI variables with tau pathology remained significant (all p<0.05, Figure 2) except in CN group. But the positive association with CSF Aβ42 was statistically significant only in MCI (β = 9.16, p = 0.03) and APOE ε4 carrier group (β = 17.52, p = 1.68 × 10−5). As for cognitive function, any association between continuous BMI variables and cognitive scores was observed across all participants. Further subgroup analyses showed that BMI had noticeable correlation with ADAS13 score in female, MCI and APOE ɛ4 carrier subgroups. Furthermore, higher BMI was positively related to MMSE only in MCI group (Figure 2 and Supplemental Table 2A). Within different biological groups, significant correlations with P-tau/Aβ42 and T-tau/Aβ42 were only observed in A+/TN + group (Supplemental Table 2B). The abovementioned significant results were barely changed when BMI was considered as a categorical variable in the correlation analysis (Supplemental Table 3). We also found older adults with obesity exhibited a decreased risk of AD utilizing the Kaplan-Meier method (p = 0.044, Supplemental Figure 3A).
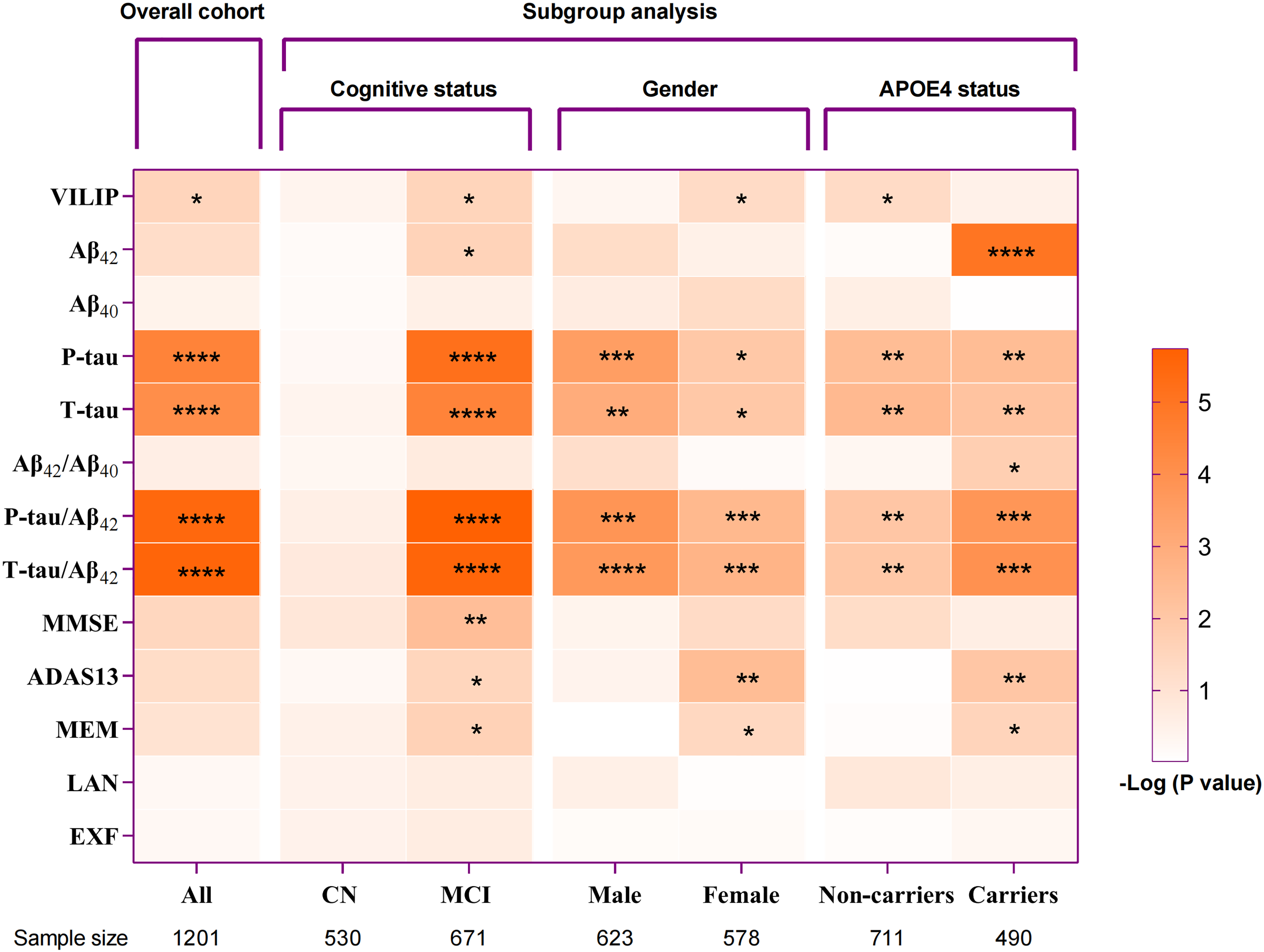
Association of BMI with CSF biomarkers and cognitive function.
Associations between CSF VILIP-1 and AD core biomarkers and cognitive function
As shown in Figure 3 and Supplemental Table 4, baseline level of CSF VILIP-1 was associated with AD core biomarkers (Aβ42, β = 2.41, p < 8.63 × 10−3; P-tau, β = 0.16, p < 2 × 10−16; T-tau, β = 1.48, p < 2 × 10−16; P-tau/Aβ42, β = 1.76 × 10−4, p < 1.68 × 10−4 and T-tau/Aβ42, β = 1.50 × 10−3, p < 3.16 × 10−4), but not with cognitive function (MMSE, ADAS13, MEM, EXF, or LAN scores) in all participants. All results exhibited negligible alterations in the sensitivity analyses after controlling for the potential confounders, such as depression, anxiety, hypertension, DM2, smoking, and stroke (Supplemental Table 4). Subgroup analyses revealed that abovementioned significant associations were persistent both within the CN and MCI groups (Figure 3A–E). However, elevated CSF VILIP-1 were linked exclusively to CSF tau pathology, but not with CSF Aβ42 in all different biological groups (Figure 3F and G). Significant correlations with P-tau/Aβ42 and T-tau/Aβ42 were only observed in A+/TN + group (Figure 3I and J). Our findings suggested that CSF VILIP-1-related disturbed calciumion homeostasis might be accompanied by the pathogenesis of AD.
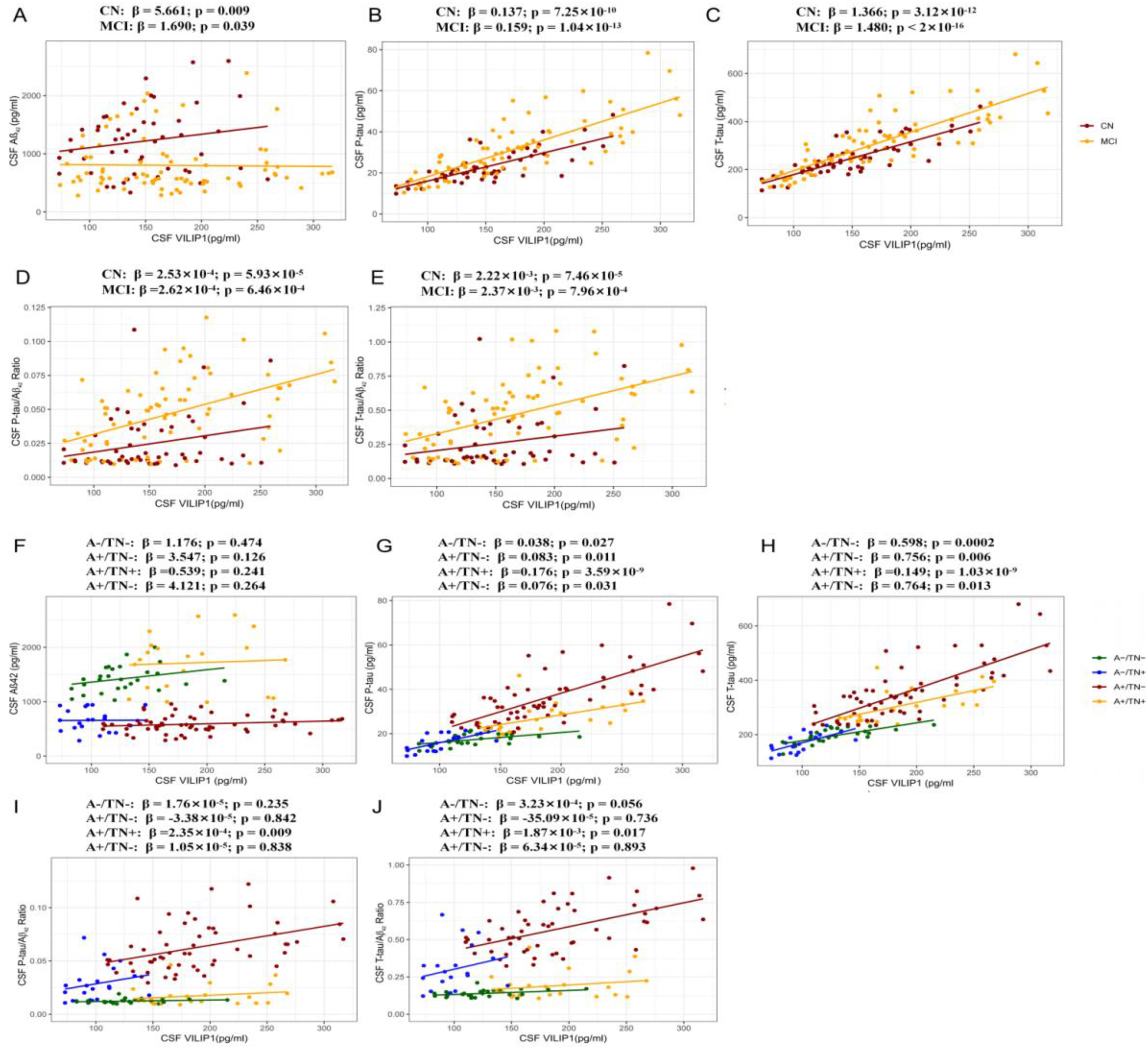
Relationship of CSF VILIP-1 with CSF AD biomarkers.
CSF VILIP-1 mediated the association between BMI and tau pathology
Mediation analyses were performed on CSF P-tau and T-tau rather than Aβ42 or cognitive functions, due to their non-robust significance in relation to BMI. The mediation analyses showed that CSF VILIP-1 partially mediated the association between BMI and P-tau (the mediation proportion: 53.7%, p = 0.018), and completely mediated the association with T-tau (the mediation proportion: 64.2%, p = 0.014) in total participants (Figure 4A and B). Subgroup analyses revealed that, for MCI group, CSF VILIP-1 mediated completely the effect of BMI on tau pathology (Supplemental Figure 2). Owing to the constraint of sample size, it was not feasible to perform meaningful analyses within the different biological subgroups. To better control for potential confounding factors, we conducted sensitivity analyses and found the mediating role of CSF VILIP-1 in total participants and MCI group were persistent and robust (Supplemental Table 6A–C).

CSF VILIP-1 mediated association between BMI and tau pathology.
Association between baseline CSF VILIP-1 levels and longitudinal cognitive changes and risk of AD
Given the above findings, we postulated that CSF VILIP-1 might have a predictive role in cognitive changes or AD risk. In order to confirm our assumption, LME models were performed. Baseline levels of CSF VILIP-1 showed an inverse relationship with MMSE, MEM, EXF, and LAN scores (p = 4 × 10−4, 0.036, 0.004 and 6 × 10−4, respectively, Table 2), and positively associated with ADAS13 scores (p = 0.009) during the follow-up. However, Kaplan–Meier test showed baseline CSF VILIP-1 failed to predict the risk of incident AD as revealed by a 10-year follow-up of 128 non-demented participants (Supplemental Figure 3B).
Association of CSF VILIP-1 with longitudinal cognitive changes.

p-values were evaluated via mixed-effect models controlling for age, sex, education, and APOE ε4 status. The results revealed the protective influence of lower baseline levels of CSF VILIP-1 on the deterioration of cognitive functions, as reflected by MMSE, ADAS13, MEM, EXF, and LAN. Significance at the level of p < 0.05 were showed in bold.
MMSE: Mini-Mental State Examination; ADAS13: Alzheimer's Disease Assessment Scale 13; MEM: memory function; EF: executive function; LAN: language.
Discussion
In our study, we probed the dynamic alterations of CSF VILIP-1 and found the concentration exhibited an initial decline, reaching a nadir in the A+/TN- group, followed by a gradual ascent across various biological stages of AD. Mediation analysis indicated that CSF VILIP-1 played a mediating part in the pertinence of BMI and tau pathology (CSF P-tau and T-tau) especially amongst MCI group. Longitudinal data revealed that individuals with lower CSF VILIP-1 had less cognitive decline. Overall, our results suggested that CSF VILIP-1, which could be implicated in the interplay between BMI and AD pathology, was predominantly active in the early stages of AD and potentially affected subsequent cognitive function.
In line with prior research, the present study consolidated that a higher BMI served as a protective factor in cognitive function among elderly non-demented individuals. Specifically, subgroup analyses demonstrated that significant correlations were observed with CSF AD core biomarkers in MCI, 35 whereas not in CN group. 15 These results indicated that MCI with normal or low BMI might be more prone to have amyloid and tau-induced cognitive impairment. The above significant correlations were barely changed after further grouping by sex or APOE ε4 carrier status. However, no correlation with CSF Aβ42 was observed in all different biological groups. A potential explanation for the lack of statistical difference is the limited sample size in each biomarker-specific subgroup.
CSF VILIP-1 reflects disrupted calciumion homeostasis and neuronal injury and may potentially be involved in signal transduction and neurotransmission.2,3 Its expression was reduced in the intracellular compartments of AD neurons yet markedly increased in extracellular plaques and neurofibrillary tangles. 3 Accumulating evidence from AD subjects showed there existed a growing trend of CSF VILIP-1.8,9 The loss of neurons expressing VILIP-1, 2 as well as the pathological decrease in VILIP-1 mRNA levels 36 were observed in animal models with AD pathology. Coincidentally, individuals with MCI displayed higher concentrations of CSF VILIP-1 than those with cognitively normal status in our study. 37 Our cross-sectional analysis also provided additional evidence that CSF VILIP-1 levels exhibit dynamic alterations, 9 as opposed to a sustained upward or downward trend, inferring it declined with the formation of amyloid plaques in the earliest stage and subsequently increased with the formation of tau pathology in the late stages of AD pathology. One potential explanation for the early reduction of CSF VILIP-1 level may be that neurons expressing VILIP-1 appear to be selectively vulnerable against disturbed calciumion homeostasis induced by Aβ plaque, 7 and VILIP-1 is involved in the formation of Aβ plaque aggregates. 3 Another possible hypothesis is that microglia, in the initial phases, downregulate their own exaggerated response to noxious Aβ plaques, thereby providing neuroprotective effects. 38 However, in later phases, overloaded pathological burdens foster more severe neuroinflammatory responses, eventually inducing neuronal injuries and contributing to an increase in CSF VILIP-1. It was also plausible to deduce that CSF VILIP-1 might be involved in neuronal damage in other neurodegenerative diseases apart from AD,3,9 since it was found to be the most concentrated in A-/TN + group.
Significant positive correlations between CSF VILIP-1 and tau pathology were detected both in the whole cohort and in different subgroups. All results were negligible alteration in sensitivity analyses after further adjustments. These results were favored by the previous findings that VILIP-1 enhanced the hyperphosphorylation of tau protein and the formation of neurofibrillary tangles.4,9,39 Additionally, we observed that CSF VILIP-1 was positively associated with Aβ42, which seemed counterintuitive. In our further analysis, this correlation was observed in both the CN group and MCI group (albeit weak), yet this correlation did not prove statistically significant within any of the biological groups. Further studies with larger sample size are warranted to validate our findings.
In light of CSF VILIP-1 reflecting neuronal impairment, we propose that its higher concentrations could be linked to the progression or severity of dementia. Indeed, our findings revealed no correlation between the CSF VILIP-1 and cognitive function at baseline, differing from the findings of Lee et al., which reported an association with MMSE score. 8 Our cohort excluded patients with dementia and had a higher mean age, but Lee's study encompassed a significant portion of AD patients. Differences in the subjects and age profiles in these cohorts may explain this inconsistency. Interestingly, analyses of the longitudinal follow-up data revealed that baseline lower levels of CSF VILIP-1 were indicative of preserved longitudinal cognitive functions. 22 Those findings were in line with a study conducted from the memory clinic-based Amsterdam Dementia Cohort. 40 The mechanism by which CSF VILIP-1 was involved in the cognitive decline might be through the regulation of signal transduction, 2 neuronal growth and differentiation, 6 synaptic plasticity, dendritic spine density, 7 and nAChR activity in the hippocampus. 41
Our findings suggested that CSF VILIP-1 acted as a mediator in the relationship between BMI and tau pathology and provided further support for the underlying mechanism. Previous studies demonstrated that body weight and fat were positively associated with leptin in obese individuals. 18 Leptin regulates tau phosphorylation by activating downstream signaling pathways, such as the phosphoinositide 3-kinase 42 and adenosine monophosphate-activated protein kinase 43 pathways, which are essential in regulating the opening of calcium ion channels and maintaining calcium homeostasis in neurons. 44 In mouse models, exogenous leptin confers protection to hippocampal and hypothalamic cell lines against neurotoxic effects by inhibiting calcium elevation. 45 In light of CSF VILIP-1 being a hallmark of neuronal injury and calcium overload,3,4 it is reasonable to postulate that calciumion homeostasis may have a mediating role in the relationship between BMI and the progression of AD. Besides, our observations provide evidence that interventions targeting at CSF VILIP-1-related neuronal calcium dysfunction may benefit the prevention of tau pathology. Future studies combining different omics fields such as metabolomics, proteomics, and genomics may provide a more comprehensive understanding of the biomolecular mechanisms of BMI, VILIP-1, and other factors including adiponectin signaling, 18 insulin resistance, 19 and nutritional status 16 in the progression of AD.
This study is the first to explore the correlations between CSF VILIP-1 and BMI, AD pathologies and cognition in a non-demented population at early stages of AD. However, several limitations should be addressed. Firstly, BMI is a non-specific index that cannot fully represent the distribution of fat and the basic components of body composition in older adults. Nonetheless, it remains a universally applied health evaluation metric due to its simplicity and accessibility. Future studies with other body composition measures like waist circumference, body roundness index or waist-to-hip ratio (not accessible in ADNI), are needed to deeply examine the role of body weight in AD. 46 Secondly, the potential for a reverse causal relationship between BMI and AD cannot be dismissed. Future researches involving other confounding factors such as inflammation, 17 insulin resistance, 19 and chronic diseases 47 are necessary to elucidate the causal link. Thirdly, it is important to note that mediating associations are only indicative but not synonymous with causation. Thus, more validations in cross-sectional and longitudinal cohorts with larger sample sizes should be conducted in forthcoming studies. Finally, CSF VILIP-1 only provides an indirect measurement to assessing cerebral disturbed calciumion homeostasis and neuronal injuries, unless confirmed by autopsy. Therefore, additional in vitro and in vivo research might help to better elucidate the role of neuronal injuries and disturbed calciumion homeostasis in the mechanism between BMI and primary AD pathologies.
In conclusion, the present study demonstrated that CSF VILIP-1 changed dynamically and might play a role in mediating the associations of BMI with tau pathology. This provides a novel theoretical basis for advocating older adults maintaining a higher weight at early stages of AD, since targeting CSF VILIP-1 may reduce tau deposition. Our results indicated that CSF VILIP-1-related disruption of calcium homeostasis could as a promising target for future management of AD.
Supplemental Material
sj-docx-1-alr-10.1177_25424823251331000 - Supplemental material for Cerebrospinal fluid Visinin-like protein-1 was associated with the relationship of body mass index with Alzheimer’s disease pathology and cognition in non-demented elderly
Supplemental material, sj-docx-1-alr-10.1177_25424823251331000 for Cerebrospinal fluid Visinin-like protein-1 was associated with the relationship of body mass index with Alzheimer’s disease pathology and cognition in non-demented elderly by Yayu Wang, Siqi Yu, Man Zhang, Huaiyuan Zhu, Shujian Chen, Yajun Zhou, Xia Zhou, Zhongwu Sun, Xianfeng Yu, Xiaoqun Zhu and in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgments
We want to thank all participants from the Alzheimer's Disease Neuroimaging Initiative (ADNI) (National Institutes of Health Grant U01 AG024904) and DOD ADNI (Department of Defense award number W81XWH-12-2-0012).
ADNI is supported by the National Institute on Aging and the National Institute of Biomedical Imaging and Bioengineering, and makes possible by the generous contributions from the following: AbbVie, Alzheimer's Association; Alzheimer's Drug Discovery Foundation; Araclon Biotech; BioClinica, Inc.; Biogen; Bristol-Myers Squibb Company; CereSpir, Inc.; Cogstate; Eisai Inc.; Elan Pharmaceuticals, Inc.; Eli Lilly and Company; EuroImmun; F. Hoffmann-La Roche Ltd and its affiliated company Genentech, Inc.; Fujirebio; GE Healthcare; IXICO Ltd; Janssen Alzheimer Immunotherapy Research & Development, (![]() ). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer's Therapeutic Research Institute at the University of Southern California. ADNI data are announced by the Laboratory for Neuro Imaging at the University of Southern California. LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. The Foundation for the National Institutes of Health facilitates the donation process for the private sector.
). The grantee organization is the Northern California Institute for Research and Education, and the study is coordinated by the Alzheimer's Therapeutic Research Institute at the University of Southern California. ADNI data are announced by the Laboratory for Neuro Imaging at the University of Southern California. LLC.; Johnson & Johnson Pharmaceutical Research & Development LLC.; Lumosity; Lundbeck; Merck & Co., Inc.; Meso Scale Diagnostics, LLC.; NeuroRx Research; Neurotrack Technologies; Novartis Pharmaceuticals Corporation; Pfizer Inc.; Piramal Imaging; Servier; Takeda Pharmaceutical Company; and Transition Therapeutics. The Canadian Institutes of Health Research is providing funds to support ADNI clinical sites in Canada. The Foundation for the National Institutes of Health facilitates the donation process for the private sector.
ORCID iDs
Ethical considerations
The research received approval from the institutional review boards of all participating institutions.
Consent to participant
Written informed consent was obtained from all participants or their legal guardians in accordance with the Declaration of Helsinki (Research Consent).
Author contributions/CRediT
Ya-Yu Wang (Data curation; Formal analysis; Investigation; Writing – original draft; Writing – review & editing); Si-Qi Yu (Formal analysis); Man Zhang (Formal analysis); Huai-Yuan Zhu (Formal analysis); Shu-Jian Chen (Investigation); Ya-Jun Zhou (Investigation); Xia Zhou (Investigation); Zhong-Wu Sun (Investigation); Xian-Feng Yu (Conceptualization; Formal analysis; Investigation; Methodology; Visualization; Writing – original draft; Writing – review & editing); Xiao-Qun Zhu (Conceptualization; Formal analysis; Investigation; Methodology; Visualization; Writing – original draft; Writing – review & editing).
Funding
This study was supported by the Natural Science Foundation of Anhui Province (Grant number: 2108085MH274); the Scientific Research Projects of universities in Anhui Province, major projects (Grant number: 2022AH040159); the Domestic and International Visiting Scholar and Research Training Program for Outstanding Young Backbone Talents in Higher Education Institutions (Grant number: gxgwfx2020027); and Henan Provice Key Subjects of Medical (other Disciplines of Pharmacy, Clinical Pharmacy).
Conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.