
Abstract
Background
Population aging increases the economic burden of Alzheimer's disease (AD). Early screening for mild cognitive impairment (MCI) has the potential to mitigate this burden, but optimal strategies regarding screening coverage and age targeting remain unclear.
Objective
To explore the impact of varying MCI screening coverage and age-specific screening strategies on the AD population size and the associated healthcare costs in Shanghai, using a system dynamics approach.
Methods
A system dynamics model was developed to evaluate disease population and economic costs associated with MCI and AD at different coverage levels and age groups. A cost-benefit comparison was conducted to identify the screening coverage rate and age threshold that maximize cost-effectiveness, balancing reductions in AD-related costs against increases in screening expenditures.
Results
Increasing MCI screening coverage significantly reduced economic costs across the AD spectrum but also increased overall screening expenditures. Expanding screening to additional age groups produced similar effects. Cost-benefit analysis identified an optimal strategy: initiating screening at age 60 or 65 with 80% coverage, which achieves substantial cost savings while avoiding the diminishing returns and excessive expenditures associated with broader, less targeted screening approaches.
Conclusions
Strategically designed MCI screening can reduce the economic burden of AD, improve public health outcomes, and promote social well-being. To maximize societal benefit, screening scope must be balanced with cost. Policymakers and healthcare professionals should tailor strategies to local contexts and urgently adopt innovative technologies such as digital health and artificial intelligence-based solutions, to enhance accessibility and scalability of MCI screening strategy.
Introduction
With over 50 million people globally suffering from dementia, China having the highest number of Alzheimer's disease (AD) cases, and the incidence, prevalence, and mortality rates of AD continue to rise. AD is currently the fifth leading cause of death among urban and rural residents in China, and it exerts a substantial economic impact on individuals, families, and society, the strain on public health and healthcare resources is intense. 1 Mild cognitive impairment (MCI), often considered as a precursor to AD, has gained attention as a critical target for early intervention and screening strategies aimed at mitigating the progression and economic impact of AD. 2 This study applies system dynamics modeling to evaluate the effects of MCI screening coverage and age-specific screening strategies on the diagnosis and treatment costs associated with AD. The findings provide valuable insights into the potential benefits and challenges of implementing MCI screening initiatives to alleviate the economic burden of AD. 3
Despite the growing recognition of MCI as a critical stage for intervention, current screening practices face significant gaps. These include inconsistent screening protocols, limited accessibility for at-risk populations, inadequate integration of advanced diagnostic technologies, and a lack of tailored strategies to address regional disparities in healthcare resources. Leveraging digital technology as a more effective tool can help increase screening accessibility, improve screening efficiency, and reduce the burden of disease associated with cognitive impairment. 4 Furthermore, the cost-effectiveness of existing screening methods remains underexplored, particularly in balancing the trade-offs between screening coverage and financial sustainability. Addressing these gaps is essential to design targeted and economically viable screening approaches.
The economic burden of AD encompasses a range of direct and indirect costs, including medical care, caregiver support, and productivity losses. As the disease progresses, the costs escalate, placing significant strain on healthcare systems and society. 5 Early detection and intervention are critical in mitigating the economic impact of AD, with MCI screening emerging as a promising approach for identifying individuals at risk and implementing preventive measures. However, the optimal parameters for MCI screening implementation, such as coverage and the targeted age groups, remain underexplored. This study addresses this gap by using system dynamics modeling to simulate the impact of various MCI screening strategies on the economic burden of AD, with the aim of identifying the most cost-effective screening approach. 6
System dynamics modeling offers a powerful approach to understanding complex systems and their dynamic behaviors over time. 7 Some previous studies have applied system dynamics methods to assess the disease burden, including AD and other chronic diseases, and their associated economic costs.8,9 By capturing feedback loops, non-linear relationships, and time delays, this modeling approach provides a dynamic and comprehensive framework for evaluating the long-term implications of policy interventions. 10 In this study, system dynamics modeling is used to examine how changes in screening coverage and targeted age groups affect the diagnosis and treatment costs of AD at different Stages of disease progression. It also explores the trade-offs and synergies between screening, diagnosis, treatment costs, and the overall economic impact, thereby providing valuable insights into MCI screening policies.
This study contributes to the literature on the economic impact of AD and the role of MCI screening in addressing this public health issue. The findings underscore the complexity of balancing screening costs, diagnosis and treatment expenses, and social welfare to create effective MCI screening policies. By employing system dynamics modeling, this research provides a nuanced understanding of the interactions within the AD healthcare system, laying the groundwork for evidence-based policy development and strategies to reduce the economic burden of AD.
Methods
The method proposed in this study adheres to Jay Forrester's system dynamics principles from the 1960s to tackle complex, large-scale systems. The system dynamics model employs a causal loop diagram to visually represent the contributing factors and their impacts, aiding in the identification of root causes. The stock-and-flow diagram further differentiates stocks from flows, enabling the separate analysis of early screening costs from those incurred during later, more severe stages of the disease.
System dynamics modeling demonstrates the long-term impacts of various policy mixes on a continuous time scale, accommodating dynamic parameter variations and addressing the timing of policy interventions. 11 Unlike analytical methods that rely on linearity and simplified relationships for closed-form solutions, system dynamics incorporates nonlinearities into decision-making, making the analysis more realistic, adaptable, and reliable for specific scenarios. These advantages make system dynamics modelling a valuable tool for economic, social, and management problem-solving and policymaking. 12
The cause-and-effect relationships within the model are developed using insights from existing literature and discussions with clinical experts. These relationships are quantified using theoretical concepts and relevant parameters and coefficients estimated from secondary data sources and prior empirical studies. The model's robustness and accuracy are ensured through rigorous testing against actual data, including behavioral, structural, and sensitivity tests. Figure 1 illustrates the framework of the study's methodology, serving as the foundation for the subsequent modeling analysis and simulation process.

System dynamics modeling process: From real-world problem to simulation and validation.

Stock flow diagram.
MCI stage stability test result.

Medical costs at different stages of Alzheimer's disease (AD).
Medical costs of Alzheimer's disease (AD) at different screening coverage rates.
Economic costs of Alzheimer's disease (AD) at different age-specific screening groups.
System dynamics model of the impact of early screening for cognitive impairment on AD population and cost
System flow diagram of the impact of cognitive impairment screening strategy on AD population and cost
The causal loop diagram in system dynamics effectively analyzes the relationships between factors in a system, providing a qualitative understanding of cause-and-effect dynamics. This study focuses on six stages: Screening Population, Preclinical Stage, MCI Stage, Mild Alzheimer's Disease, Moderate Alzheimer's Disease, and Severe Alzheimer's Disease. The analysis incorporates the disease population and total costs for each stage, along with auxiliary variables and constants, forming the system flow diagram of the impact of cognitive impairment screening strategy on the AD population and cost, as shown in Figure 2.
This model captures the complex interactions influencing AD progression, providing insights into the impact of early cognitive impairment screening. It helps policymakers and healthcare professionals assess the cost-effectiveness of different screening strategies and interventions, guiding the development of efficient approaches to tackle AD. By simulating the long-term outcomes of various interventions, the model supports evidence-based decision-making, optimizing resources, and maximizing benefits for individuals and society. The comprehensive nature of the model ensures the consideration of interdependence and feedback mechanisms within the system. Changes in one stage can significantly affect other stages of disease progression, emphasizing a dynamic and integrated approach to addressing AD's challenges. By identifying leverage points for intervention, the model helps implement small changes that yield significant outcomes.
Model parameters and related equations
The utilization of data from the “Shanghai Census Yearbook,” “Shanghai Statistical Yearbook,” and “Medical Security Statistical Yearbook” ensures that the model is grounded in robust empirical evidence. These sources provide detailed information on population demographics, medical expenditures, and healthcare accessibility, allowing for a comprehensive analysis of the impact of early screening for cognitive impairment on the AD population and associated costs.
By incorporating data spanning a decade from 2010 to 2020, the model captures important trends and patterns in population dynamics and healthcare spending. This temporal scope enables the exploration of long-term projections and trends beyond the present time. The model considers various factors that influence the progression of AD, including screening rates, disease prevalence, treatment efficacy, and healthcare costs. Table 1 provides the main parameters and model settings used for the system dynamics modeling of cognitive impairment screening impact on AD population and costs.
Main parameters and model settings for system dynamics modeling of cognitive impairment screening impact on Alzheimer's disease population and costs.

The unit of variable is CNY (RMB).
The unit of variable is dimensionless (Dmnl).
To ensure the accuracy and reliability of the model, rigorous mathematical research methods are employed to analyze the available data and make informed predictions about future developments. By systematically estimating these trends and incorporating relevant literature and information, the model provides valuable insights into the potential impacts of different interventions and policies related to early screening for cognitive impairment.
It is essential to acknowledge that the model is established under certain assumptions. It assumes the system functions as an interconnected and dynamic process, where changes in one stage can have cascading effects on other stages of the disease. The focus of the model is primarily on the subsystems associated with the six stages, which allows for a detailed understanding of the factors influencing the AD population and costs. However, it does not consider external factors that may also impact the dynamics of the system.
Despite these limitations, the model serves as a valuable tool for policymakers, healthcare professionals, and researchers to evaluate the potential benefits and cost-effectiveness of early screening for cognitive impairment. It provides a basis for informed decision-making and the development of targeted strategies to mitigate the burden of AD on individuals, families, and society as a whole.
According to the basic setting rules of the system dynamics model equation, the six stages - Screening Population, Preclinical Stage, MCI Stage, Mild Alzheimer's Disease, Moderate Alzheimer's Disease, and Severe Alzheimer's Disease are represented by state variables, each associated with corresponding auxiliary quantities. For instance, the number of individuals in the MCI stage is determined by the difference between the inflows and outflows, represented by the relevant auxiliary quantities.
We set up:

Formula (1) represents the relationship matrix, and L represents the vector form of the state variable, which is 
Due to the dynamic changing characteristics of the system, when the state variable

In the formula: t represents time,
Results
System dynamics model testing and MCI screening strategy simulation
Model testing
Stability test
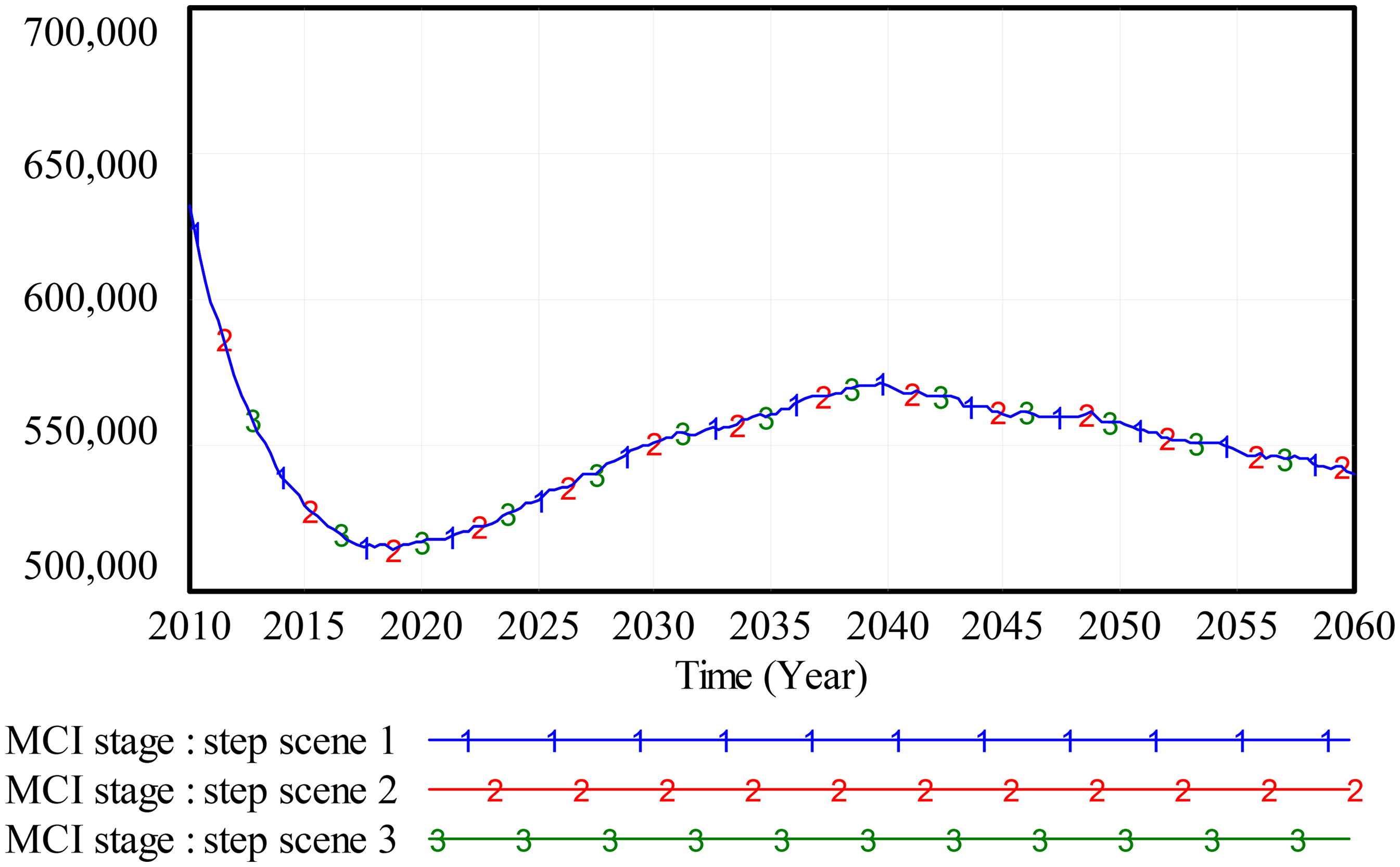
To ensure the model's reliability and accuracy for simulations, it is essential to test its stability. A fundamental aspect of this validation involves assessing the model's stability to ensure it yields consistent results across different simulation time intervals. For this stability test, the MCI stage was selected as the variable of interest. Stability tests were conducted using a one-year simulation time step, with the results depicted in the figure.
Figure 3 illustrates the MCI Stage Stability Test Result, revealing that the MCI stage charts from different time intervals almost completely overlap, indicating consistent trends regardless of the time interval used. This overlap strongly suggests that the system dynamics model is stable. Model stability is crucial as it ensures reliable and consistent results, which are essential for informed decision-making. A stable model allows policymakers, healthcare professionals, and researchers to confidently rely on its outputs to design effective interventions and strategies for AD.
Validity test
To investigate the impact of early screening for cognitive impairment on the AD population and costs, ensuring the model's reliability and validity is crucial. The data for the simulation comes from sources like the “Shanghai Census Yearbook,” “Shanghai Statistical Yearbook,” and “Medical Security Statistical Yearbook”. These datasets were analyzed using regression methods to determine model equations and parameters. The model was then simulated using Vensim software, and the results were compared with actual data. Table 2 presents the system dynamics model validity test results, showing that the simulation errors fall within an acceptable margin, thus confirming the model's reliability and accuracy. The comparison revealed that simulation errors for key indicators ranged from 0.04% to 4.33%, which is within the acceptable error margin. This indicates that the simulation results are consistent with actual data, demonstrating the model's authenticity and validity. Validating the simulation results ensures that the model accurately reflects real-world AD progression, allowing for reliable projections, these validated results can now be used for further analysis. In addition, policymakers and healthcare professionals can depend on them to develop effective interventions and strategies to mitigate the impact of AD.
System dynamics model validity test results of the impact of MCI screening strategy on AD population and costs.

Simulation analysis
After successfully passing the validation tests, the system dynamics model was deemed suitable for predictive simulations. In this study, simulations were conducted using Vensim PLE, with a step size of 1 year, spanning the period from 2010 to 2060. The variables measured include medical expenses for mild, moderate, and severe AD, along with total AD treatment costs. Figure 4 illustrates the medical costs across the AD spectrum, showing a gradual increase in all medical expenses and total treatment costs over time. This upward trend aligns with the expected growth of the aging population and the rising prevalence of AD. These results establish a baseline for future policy simulations, allowing researchers to assess the effectiveness of proposed interventions by comparing them against current data. Such analyses will help policymakers in developing targeted public health strategies for cognitive impairment screening strategies.
The simulation results highlight the cost variations across different stages of AD in the context of early screening's impact. Specifically, the findings reveal distinct patterns for medical expenses across Mild, Moderate, and Severe AD. For Mild AD, the simulation shows a gradual decrease in medical expenses over time, eventually reaching a dynamic equilibrium. This decline is attributed to the effectiveness of early screening and timely interventions, which manage disease progression and reduce the need for intensive care. In contrast, medical expenses for Moderate AD exhibit consistent growth, indicating a sustained demand for medical services. This increase is particularly significant for individuals aged 60 and older, as it is influenced by the aging population, advancements in medical treatments and health technologies, and caregiving costs. Severe AD medical expenses initially decrease but then steadily increase in later stages. This pattern suggests that as the disease progresses, the need for specialized and intensive care rises, eventually stabilizing due to a balance between care needs and available resources.
These trends are closely linked to population aging, particularly in older demographics, and per capita treatment costs. As Shanghai's population ages and AD diagnoses increase, overall costs for AD diagnosis and treatment will continue to rise. This underscores the importance of effective early screening measures to identify cognitive impairment early and provide appropriate interventions to manage economic costs of AD. Targeting high-risk age groups, such as those aged 60 and above, in early screening policies could optimize cost-effectiveness and improve resource allocation.
Screening strategy simulation
Simulation 1: MCI screening coverage strategy
MCI screening, as an early diagnosis method for AD, is effective in reducing its incidence but increases medical costs, necessitating comprehensive analysis. Early MCI screening facilitates early diagnosis and intervention, delaying or reducing AD development, allowing more patients to receive treatment before symptoms appear and reducing morbidity. Early intervention improves quality of life and reduces pressure on the healthcare system.
However, expanding MCI screening coverage requires more resources, including medical institutions, professional training, and equipment, which increases overall economic costs, to evaluate the benefits and costs of increased MCI screening coverage, a cost-benefit analysis is essential. This analysis considers costs and benefits, including improved patient quality of life and reduced healthcare resource utilization from early intervention. The economic benefit of MCI screening can be assessed by comparing screening costs to avoided treatment and associated economic costs. Additionally, the feasibility of MCI screening must be considered, as it involves assessing general populations and requires sufficient manpower, time, and technology and technical support. Effective information management systems are needed to protect privacy and data security. These factors must be considered when developing strategies and plans.
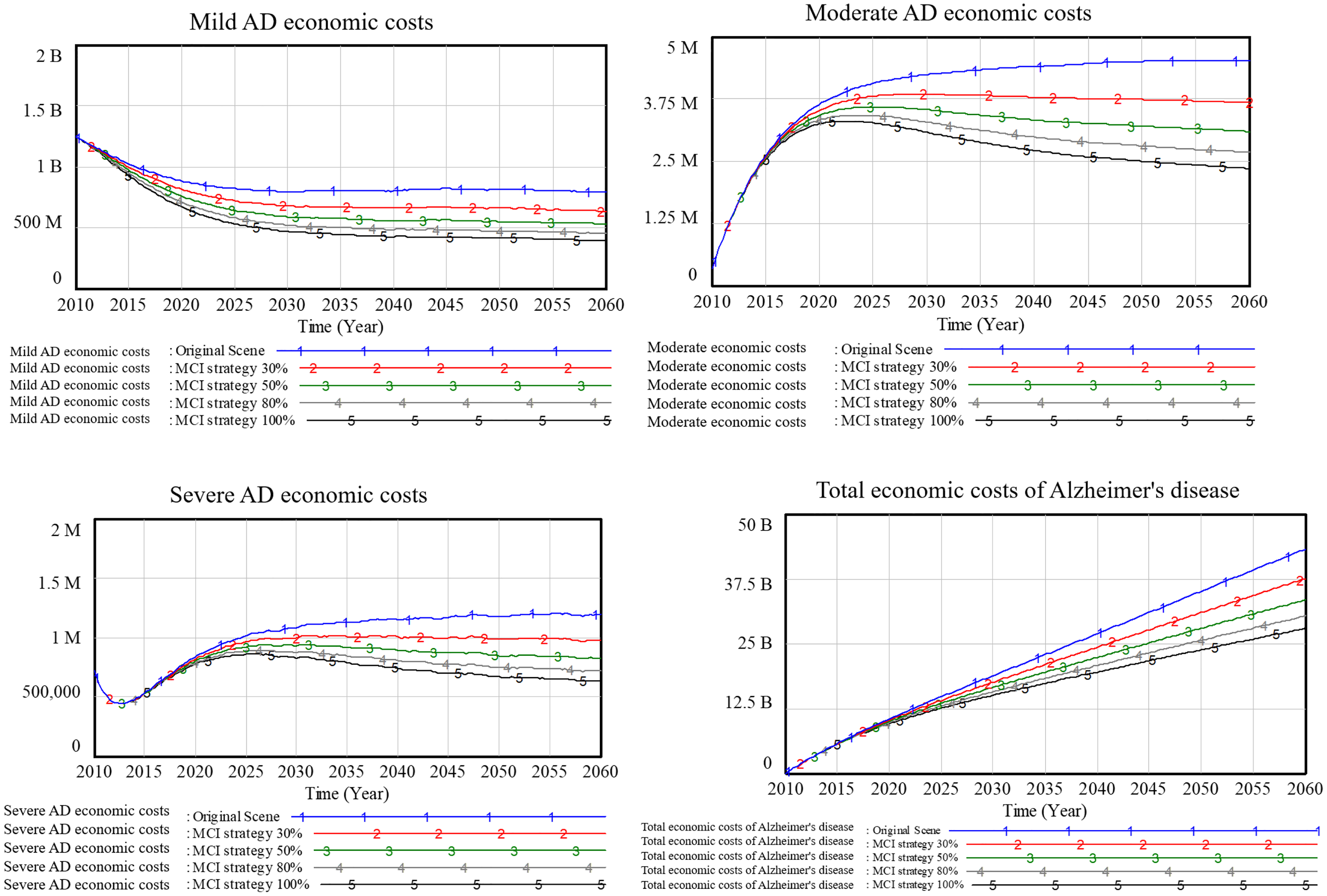
MCI screening is crucial for the early diagnosis and treatment of AD, as it delays disease progression and reduces medical costs. Figure 5 illustrates the medical costs of AD at different screening coverage rates, emphasizing the cost-saving potential of early screening across various stages of the disease. The most significant cost impact is observed in Mild AD, where early detection and intervention slow disease progression and lower treatment costs. For Moderate AD, although treatment costs are higher, early detection still reduces expenses and enhances quality of life. For Severe AD, the impact is smaller, but early detection still contributes to cost reduction.
Simulation results in Table 3 presents the changes in economic costs at different MCI screening coverage rates, demonstrating that higher MCI screening coverage reduces healthcare costs across all stages of AD, despite increased expenditures for screening. This effect is most notable at the MCI stage, where early detection prevents costly treatments in later stages. Enhanced coverage ensures timely diagnosis and early intervention, slowing disease progression and reducing long-term costs. Early interventions at the MCI stage include cognitive training, exercise, dietary changes, and managing comorbid conditions such as hypertension and diabetes, these measures reduce complications and advanced-stage economic costs. Additionally, patients at this stage tend to adhere better to treatment plans, further improving disease management and lowering overall costs.
Changes in economic costs at different MCI screening coverage rates.

MCI screening coverage rate - Increasing MCI screening coverage from 0% to 80% significantly reduces total AD-related medical costs by approximately 29.83%. However, increasing coverage from 80% to 100% results in diminishing returns, achieving only an additional 5.59% cost reduction while requiring substantially higher screening expenditures. Therefore, a screening coverage rate of approximately 80% is the most cost-effective, maximizing economic benefits while avoiding excessive costs. This analysis highlights the importance of balancing screening expansion with economic feasibility. Targeted MCI screening at an optimal coverage level ensures that more at-risk individuals receive early diagnosis and intervention while maintaining sustainable healthcare costs on AD.
Simulation 2: MCI screening age strategy
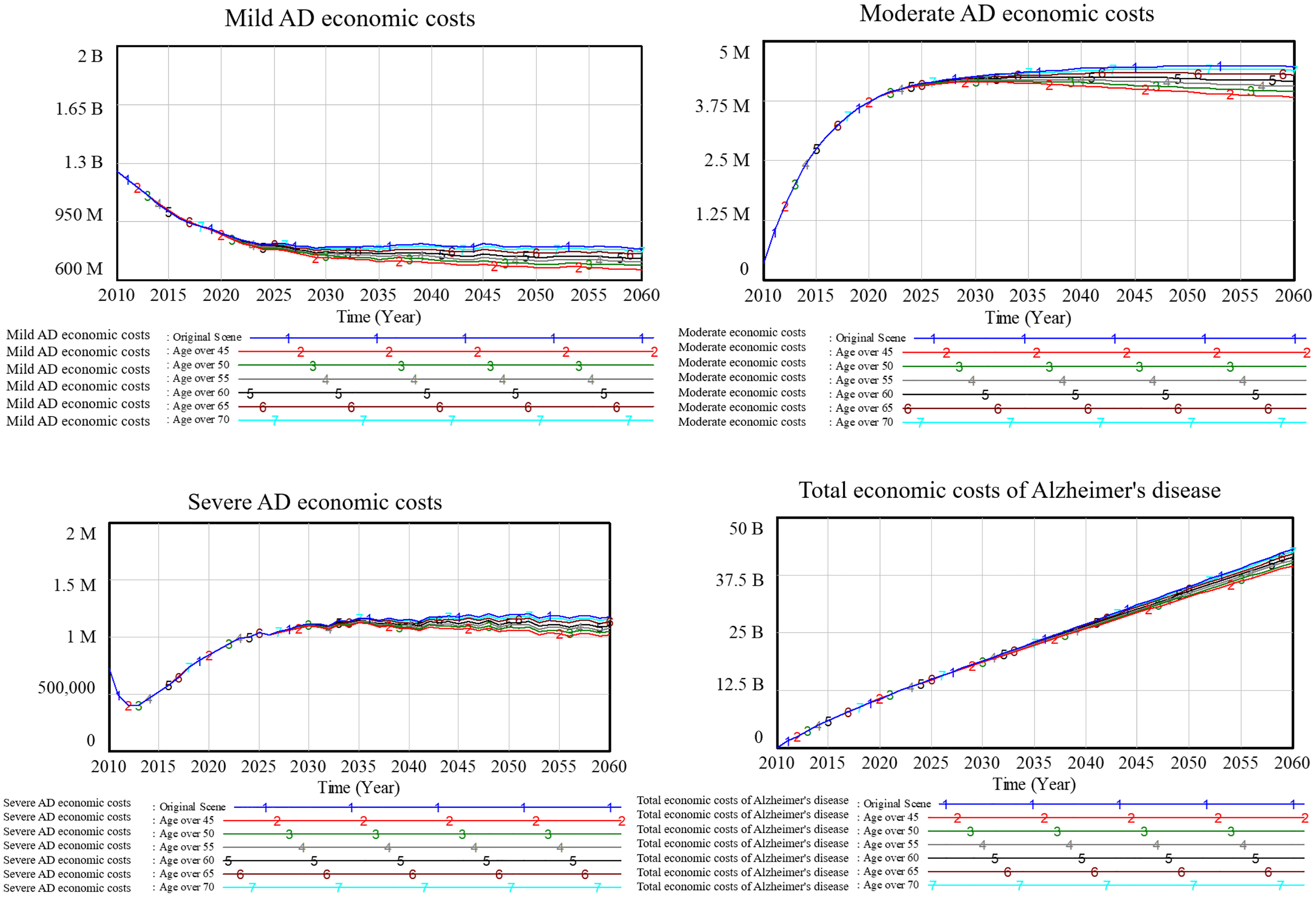
MCI screening is crucial for early AD diagnosis, enabling timely intervention to delay or reduce disease progression and lower medical costs. However, increasing the number of people screened also raises screening costs and impacts medical resource allocation. Figure 6 illustrates the economic costs of AD across different age-specific screening groups, revealing that targeting specific age groups can enhance early diagnosis, reduce total economic costs, and improve the allocation of healthcare resources. However, as screening numbers increase, the associated costs rise, requiring optimization to achieve the best balance between effectiveness and affordability.
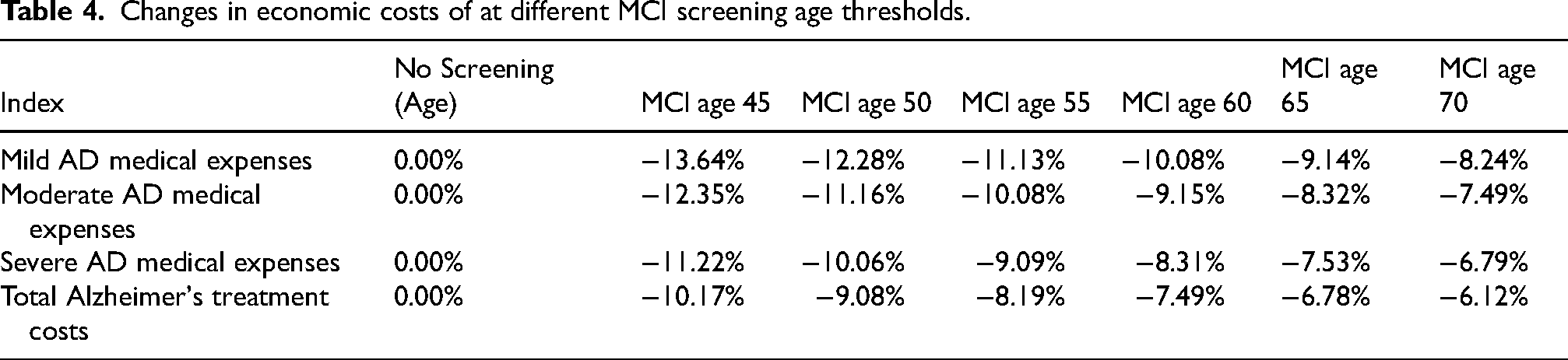
This study examines the impact of various MCI screening age thresholds (45, 50, 55, 60, 65, and 70) on AD-related medical costs. Simulation results in Table 4 demonstrate a gradual decline in the reduction of AD-related medical costs as the screening age increases, from 10.17% at age 45 to 6.12% at age 70. This suggests that earlier screening and intervention lead to greater cost savings, while later detection and treatment result in smaller cost reductions. Specifically, compared to no screening at any age, screening individuals over 45 yields the greatest reduction in mild AD treatment costs, with a decrease of 13.64%. In contrast, initiating screening at older ages, particularly at 70, focuses on a higher-risk population but leads to a smaller reduction in mild AD costs (8.24%). While screening at older ages allows for more targeted resource allocation and is more economically efficient, it risks missing early intervention opportunities.
Changes in economic costs of at different MCI screening age thresholds.
Early screening facilitates risk management and lifestyle modifications, but its incremental benefits diminish with age. Older adults often have comorbidities and more limited intervention windows, reducing the effectiveness of early detection and treatment. Therefore, although screening at younger ages can lead to larger reductions in treatment costs, it also includes more cognitively healthy individuals, increasing the likelihood of overdiagnosis and unnecessary follow-up exams, especially in the context of current limited AD clinical intervention options, which increases anxiety and concerns among individuals in the mild to moderate stage.
MCI screening age threshold - Initiating MCI screening at younger ages, such as 45 or 50, leads to the highest reductions in AD-related economic costs, with reductions of 10.17% and 9.08%, respectively, due to earlier and more widespread diagnosis and intervention. However, this also leads to significantly higher screening and treatment expenditures in AD care, especially among lower-risk populations. The marginal reduction in cost steadily declines as the starting age increases. Starting screening at age 60 or 65 results in smaller reductions in total treatment costs (7.49% and 6.78%, respectively) while still capturing a substantial portion of the at-risk population, indicating a more cost-efficient balance between early detection and financial sustainability. Therefore, initiating MCI screening at age 60 or 65 is recommended as the most economically reasonable threshold, allowing timely intervention for high-risk individuals while minimizing unnecessary financial burdens on the healthcare system and reducing anxiety associated with AD. This analysis highlights the importance of targeting screening to high-risk populations at the appropriate time to optimize both economic outcomes and resource allocation in AD care.
Comparative analysis of different screening strategies
Based on the policy scenario simulation results from above, the MCI screening coverage rate and screening age threshold strategies were compared. The results indicate that both strategies reduce diagnosis and treatment costs across the AD spectrum, but their impacts vary.
For the MCI screening coverage strategy, higher coverage level increases diagnosis and treatment costs across all AD stages but increases the cost of MCI screening. Through continuous Monte Carlo sensitivity analysis simulation, we find that in the continuous simulation result, cost-benefit comparison reveals that the maximum benefit occurs at a ratio of 1.73, meaning that for every RMB invested in screening, AD diagnosis and treatment costs are reduced by 1.73 RMB. However, this effect diminishes as MCI screening coverage increases.
For the MCI age-specific screening range strategy, broader age group coverage increases AD screening, diagnosis and treatment costs. Through continuous Monte Carlo sensitivity analysis simulation as above, we find that the maximum benefit in this strategy is a ratio of 1.15, indicating that for every RMB invested in earlier screening, AD diagnosis and treatment costs are increased by 1.15 RMB. This effect also diminishes as the starting age for MCI screening increases.
Both strategies exhibit a typical diminishing marginal effect, where the policy effect decreases as the policy is intensified. Therefore, in practice, it is crucial to find the optimal cost-benefit breakeven point. However, because AD treatment and MCI screening have social welfare implications, the analysis should not be limited to a cost-benefit perspective alone, more social factors need to be considered, making the above conclusions primarily applicable from an economic evaluation standpoint.
Discussion
The findings of this study provide valuable insights into the dynamics of AD progression and the potential of early intervention strategies. A recent 20-year multicenter, nested case-control study on AD biomarkers conducted among cognitively normal participants involved approximately 30,000 individuals who underwent cerebrospinal fluid (CSF) examination, cognitive assessment, and brain imaging every 2–3 years from baseline (2000) until they were diagnosed with AD, died, were lost to follow-up, withdrew from the study, or until the study endpoint. Ultimately, 648 participants who developed AD and 648 matched participants who remained cognitively normal were included. The study compared the temporal trajectories of AD-related CSF biomarkers between the two groups. The results indicated the sequence and timing of biomarker differences between the AD group and the cognitively normal group as follows: Aβ (18 years before diagnosis), Aβ42/40 (14 years before diagnosis), p-tau 181 (11 years before diagnosis), t-tau (10 years before diagnosis), neurofilament light chain (9 years before diagnosis), hippocampal atrophy (8 years before diagnosis), and cognitive decline (6 years before diagnosis). 13 Additionally, another cross-sectional study demonstrated that dementia and MCI are prevalent among individuals aged 60 years or older in China, emphasizing the significant need for improved management of the preclinical phase. 14 These findings underscore the prolonged preclinical phase of AD, highlighting the clinical significance of early biomarker identification and the necessity of sensitive screening methods to detect individuals at risk and enable timely and early intervention before irreversible cognitive decline.
System dynamics modeling revealed that increasing MCI screening coverage and expanding age-specific screening groups significantly reduces AD-related treatment and diagnosis costs. The rationale for these results lies in the ability of early detection and intervention to slow disease progression, thereby reducing the burden of advanced-stage AD. However, the economic feasibility of implementing such strategies on a large scale remains a challenge, necessitating a balance between cost-effectiveness and comprehensive coverage. Moreover, broader age-range screening captures at-risk individuals who might otherwise remain undiagnosed, aligning with public health objectives of prevention and early intervention. These findings emphasize the importance of targeting high-risk populations and tailoring strategies based on demographic and healthcare resource availability.
In the context of Shanghai, the most economically effective MCI screening strategy is to initiate screening at age 60 or 65 to balance AD-related cost reduction with manageable screening expenditures, targeting high-risk populations efficiently. A screening coverage rate of 80% is recommended as the optimal level, significantly lowering long-term AD treatment costs while avoiding the diminishing returns of near-universal screening. Together, these strategies ensure cost-effective and sustainable resource allocation, aligned with Shanghai's demographic and healthcare infrastructure to maximize both economic and public health outcomes.
It is important to note that the current model was constructed based on population demographics and healthcare data specific to Shanghai, making it most applicable to regions with similar characteristics. When applied to other contexts, adjustments to key parameters such as demographic structure, healthcare accessibility, and policy interventions would be essential. Although parameters are presently updated annually based on the latest available data, future improvements could include real-time integration of broader data sources (e.g., electronic health records, national databases, and live surveillance data) as well as advanced methodologies like machine learning and artificial intelligence (AI)-driven algorithms (e.g., ChatGPT, DeepSeek, etc.) to enhance the model's adaptability and continuously refine parameter estimates.
Additionally, the broader societal benefits of early screening, such as improved quality of life for patients and reduced caregiver burden, provide a compelling rationale for investment in these strategies.15,16 However, reaching an 80% coverage rate remains challenging with current clinical screening and assessment tools. This highlights the urgent need for more effective and innovative approaches, such as digital therapeutics, community-based models, and AI-assisted cognitive assessments to achieve accessibility, scalability, and the real-world implementation of MCI screening strategies. Future research should explore how these findings can be translated into scalable, evidence-based public health screening and interventions that address both the economic and social dimensions of AD care, guiding policies for efficient resource utilization and improved health outcomes in AD.
Conclusion
This study used system dynamics modeling to evaluate MCI screening strategies, revealing that both increased coverage and broader age-range screening significantly reduce AD-related costs while increasing screening expenses. The analysis explores an optimal strategy that balances coverage and age-group targeting, achieving maximum cost-effectiveness by prioritizing high-risk populations for early detection. Identifying the optimal balance between coverage rates and age groups is essential for effective screening, resource allocation, and cost containment.
The findings offer actionable insights for healthcare institutions and public health authorities to refine evidence-based strategies. By prioritizing high-risk age groups and maximizing early detection, healthcare systems can slow disease progression, enhance clinical decision-making, and reduce long-term costs. This study provides practical recommendations for implementing targeted MCI screening policies, emphasizing the importance of integrating early screening into healthcare planning to reduce AD's overall economic burden. These strategies also contribute to public health policy development, promoting efficient resource utilization and improved health outcomes.
To ensure effective implementation, policymakers should prioritize MCI screening at age 60, as this approach optimally balances AD-related cost reduction with manageable screening expenditures. This targets high-risk populations while avoiding unnecessary costs from over-screening lower-risk individuals. Additionally, a screening coverage rate of approximately 80% is recommended as the most cost-effective strategy. This level significantly reduces overall AD-related medical costs while avoiding the diminishing returns observed at near-universal coverage levels (100%). Screening strategies should also be adapted to regional demographic trends, healthcare infrastructure, and resource availability to optimize efficiency. Moreover, leveraging real-time data from electronic health records and integrating digital technologies and AI-driven predictive models can enhance risk stratification and screening effectiveness. These measures will enhance screening effectiveness, ensuring a sustainable and cost-efficient approach to managing AD in Shanghai's aging population.
In conclusion, optimizing MCI screening strategies by identifying the optimal screening coverage rate and age threshold enhances early detection, slows disease progression, and reduces the overall economic burden of AD. Policymakers should consider both economic feasibility and social implications, focusing on high-risk populations and tailoring interventions to local demographic and healthcare system needs. Integrating digital technologies and artificial intelligence can further address broader challenges of cognitive impairment screening and prevention, ensuring sustainable cognitive care solutions for aging populations.
Footnotes
Ethical considerations
Not applicable
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contributions/CRediT
Grace Yuange Zang (Conceptualization; Data curation; Formal analysis; Methodology; Software; Writing – original draft); Zongjiu Zhang (Conceptualization; Methodology; Supervision; Validation; Writing – review & editing); Yi Tang (Conceptualization; Supervision; Validation; Writing – review & editing); Keqin Rao (Conceptualization; Data curation; Supervision; Writing – review & editing); Anthony Ting-yuk Wu (Conceptualization; Project administration; Resources; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Key R&D Program of China (Project Title: Research on the Current Situation and Development Trends of Elderly Disease in China, No. 2022YFC3603000).
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data used in this study were obtained from publicly available sources, which are clearly cited within the manuscript. The datasets generated and analyzed in the study are available from the corresponding author upon reasonable request.