
Abstract
Background
Visual hallucinations (VH) are an important neuropsychiatric feature of dementia. The association between VH and cognition remains controversial
Objective
To investigate the differences in clinical correlates of VH and explore the associations between VH and cognitive functional decline in individuals with dementia with Lewy bodies (DLB) and Alzheimer's disease (AD).
Methods
Outpatient medical records of 154 patients with DLB and 297 patients with AD between January 2017 and December 2023 were reviewed. We collected demographic characteristics and used neuropsychological assessments and semi-structured detailed interviews to evaluate cognition and VH. Multiple linear regression and mediation analyses were employed to analyze the data, adjusting for confounding variables.
Results
DLB patients had a higher prevalence of VH than AD patients (p < 0.01). The presence of VH predicted lower Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) scores in both DLB and AD patients (p < 0.01). In DLB patients, VH were associated with lower attention function scores after adjustment (p = 0.027). In AD patients, VH were related to worsened orientation ability after adjustment (p = 0.033). Attention function partially mediated the association between VH and cognition in DLB patients (p < 0.01), whereas orientation function partially mediated this association in AD patients (p < 0.01).
Conclusions
VH may independently correlate with deterioration in global cognitive performance. In DLB patients with VH, attentional function appears to be more impaired, whereas in AD patients, orientation function is the most affected. Different cognitive domains may help distinguish between DLB and AD patients with VH.
Introduction
Visual hallucinations are a common psychotic symptom of neurodegenerative diseases. In clinical contexts, visual hallucinations refer to visual percepts experienced while awake, without any external stimulus. These hallucinations can be categorized into complex visual hallucinations (VH) and minor hallucinations (MH). VH consist of recurrent and well-formed vivid complex images. Dementia with Lewy bodies (DLB) is the most frequent form of neurodegenerative dementia after Alzheimer's disease (AD), accounting for 25% of all cases of dementia in elderly people. 1 The core clinical features of DLB include cognitive fluctuations, VH, parkinsonism, and rapid eye movement sleep behavior disorder (RBD). VH are more frequent in DLB than in AD or other dementias, particularly in the early stages of dementia.2,3 The reported prevalence of VH ranges from 55% to 78% in DLB, 18.7% to 23% in AD, and 22% to 38% in Parkinson's disease (PD), while the prevalence of VH in frontotemporal dementia is 14.4%, based on a retrospective case series.4,5 Pathophysiological investigations have revealed that patients with DLB and VH tend to exhibit a higher density of Lewy bodies in the temporal lobe. 6 Visual hallucinations can be a severely incapacitating symptom, significantly impacting patients’ quality of life, while also contributing to increased caregiver distress. 7
Numerous studies have demonstrated a close relationship between VH and cognitive performance. In advanced AD, VH is a prevalent mental health symptom that can negatively impact cognitive abilities. 8 Yet, there is a paucity of research on the precise cognitive correlates of VH in DLB. While VH can, to some extent, affect cognitive function in both AD and DLB, the cognitive traits of these patients often differ. 9 Unlike AD, the pattern of cognitive decline in DLB is often characterized by deficiencies in executive function, attention, and visual perception. Mosiman et al. found that individuals with DLB and PD dementia who experienced VH performed poorly on tasks assessing visual-perceptual abilities. 10 Although previous studies suggest that executive functioning, processing speed, and visual attention are neuropsychological predictors of VH, recent studies have yielded inconsistent results. 9 The intricate relationship between neuropsychological features and VH remains understudied, with previous studies primarily limited to comparisons of individual VH in AD or DLB. To address this knowledge gap, the present study aimed to investigate and compare the impact of VH on cognitive function in patients with DLB or AD. By integrating these clinical findings, we hope to gain a deeper understanding of the association between visual hallucinations and cognition in DLB and AD and inform better treatment strategies.
Methods
Study design and participants
Participants were consecutively recruited from the Department of Neurology of Tianjin Huanhu Hospital, a tertiary hospital in Northern China with a specialized Cognitive Disorders Senior Center, between January 2017 and December 2023. Of the 1549 initially recruited participants, 154 were classified as DLB and 287 as AD. The inclusion and exclusion criteria for participants are outlined in Supplemental Figure 1. Diagnoses of DLB were made according to the 2017 DLB Consortium criteria, which require two or more core symptoms with or without indicative biomarkers, or one core symptom with one or more indicative biomarkers. 1 AD diagnoses were based on the National Institute of Neurological Disorders and Stroke–Alzheimer's Disease and Related Disorders criteria for “probable AD”. 11 This study included only patients who had undergone a complete neuropsychological battery of tests (see below). The following exclusion criteria were applied: age < 50 years or > 90 years, severe cognitive impairment (Mini-Mental State Examination [MMSE] score < 10), comorbid neurological conditions, a previous history of psychiatric disorders with a definite diagnosis, and various systemic conditions, including malignant tumors, connective tissue disease, blood disease, and malnutrition.
Measurements
A review of clinical history, demographic data, cognitive status, clinical diagnosis at last visit, use of medications, clinical core features (fluctuating cognition, 7 VH, 12 parkinsonism, 13 and RBD14,15) was conducted, along with physical examinations and neuropsychological assessments. Global cognitive function was assessed using the MMSE 16 and Montreal Cognitive Assessment (MoCA) scales. 17 Functional abilities were assessed using the Activity of Daily Living Scale (ADL) 18 and the Clinical Dementia Rating (CDR). 19 Neuropsychiatric symptoms were evaluated using the Neuropsychiatric Inventory (NPI), with caregiver input. 12 Visuospatial function was assessed with a clock-drawing test. Neuroimaging was performed using computed tomography and magnetic resonance imaging.
Cognition was assessed using the MMSE and MoCA scales. The total scores for both assessments ranged from 0 to 30, with lower scores indicating greater cognitive impairment. Dementia was identified using education-specific cutoff points for MMSE total scores (MMSE ≤ 17 for illiterate individuals, ≤ 20 for participants with elementary school education, and ≤ 22 for those with middle school education and above). According to Chinese MoCA norms, a MoCA score < 26 was considered indicative of impaired cognitive function or risk for dementia, 21 ≤ MoCA ≤ 25 was classified as mild cognitive impairment, 10 ≤ MoCA ≤ 20 was classified as moderate cognitive impairment, and MoCA <10 was classified as severe cognitive impairment. The use of only MMSE or MoCA for cognitive domains assessment is significantly restrictive, therefore, in our study the different domain scores mainly stemmed from MoCA (including ability and delayed recall, attention, language, execution Capability, visuo-spatial ability) and harmonized with MMSE (including attention and calculation, Language, delayed recall, immediate recall, execution, visuo-spatial ability and Orientation Ability, shown in Supplemental Material).
All patients were initially assessed for VH using the hallucinations domain of the NPI, which rates eight individual forms of hallucinations. The NPI is useful for identifying and determining the frequency and severity of VH. To provide a more detailed description of VH, a further classification of the phenomenology of VH was conducted using the North-East Visual Hallucinations Interview (NEVHI), a semi-structured, face-to-face interview approach. 20
The study was approved by the ethics committee of the Tianjin Huanhu Hospital (2023-158). Written informed consent was obtained from participants or their guardians. The study protocol complied with the principles enshrined in the Declaration of Helsinki. All data were anonymized.
Statistical analyses
Continuous variables (age, years of education, disease duration, and scores on the MMSE, MoCA, NPI, and ADL) were presented as mean ± standard deviation for normally distributed data. For non-normally distributed data, median (interquartile range [IQR]) was also provided. Categorical variables (sex, marital status, smoking, alcohol consumption, hypertension, type 2 diabetes mellitus [DM], cardiovascular disease, VH, RBD, cognitive fluctuation, parkinsonism, and medications used (such as cholinesterase inhibitors [ChEIs], neuroleptics, levodopa, dopamine agonists) were presented as frequency counts and percentages. The Chi-square test was used for comparing categorical variables, while the independent-sample t-test or analysis of variance were used for comparing normally distributed continuous variables. The Mann–Whitney U-test and Kruskal–Wallis test were used for comparing non-normally distributed continuous variables. Multi-group comparisons were performed using the Kruskal-Wallis test with post hoc Bonferroni correction. Multiple linear regression analysis was employed to investigate the association of cognitive function scores and VH with DLB and AD. The multivariate linear regression models controlled for various confounding variables, including age, sex, education, disease duration, marital status, stroke, DM, heart disease, hypertension, and cognitive subitems. Mediation analysis and sensitivity analyses were conducted to examine how cognitive domains mediated the relationship between VH and global cognitive function. A significance level of p < 0.05 was set for all analyses. Statistical analyses were performed using SPSS 26.0 (IBM Corp., Armonk, NY, USA) and RStudio 4.3.
Results
Characteristics of the study population and prevalence of VH
A total of 441 patients (mean age: 70.10 ± 8.68 years; 47.6% males) were included in this study. The demographic and clinical characteristics of patients with probable AD (n = 287; 131 males, 156 females) and probable DLB (n = 154; 79 males, 75 females) are summarized in Table 1. Patients in the DLB group were significantly older than the AD group (average age at first evaluation: 72.40 ± 7.56 years versus 69.60 ± 9.46 years, p < 0.05). The DLB group had a longer disease duration and a higher proportion of smokers and alcohol consumers than the AD group (p < 0.01). Patients in the DLB group had higher ADL scores compared to those in the AD group (32.81 ± 12.76 versus 27.13 ± 7.56, p < 0.01), indicating greater functional impairment in the former. There was no significant between-group difference with respect to sex distribution, years of education, marital status, MMSE score, MoCA score, or the prevalence of stroke, DM, heart disease, and hypertension.
Comparison of demographic, clinical and personal background characteristics between DLB and AD patients.
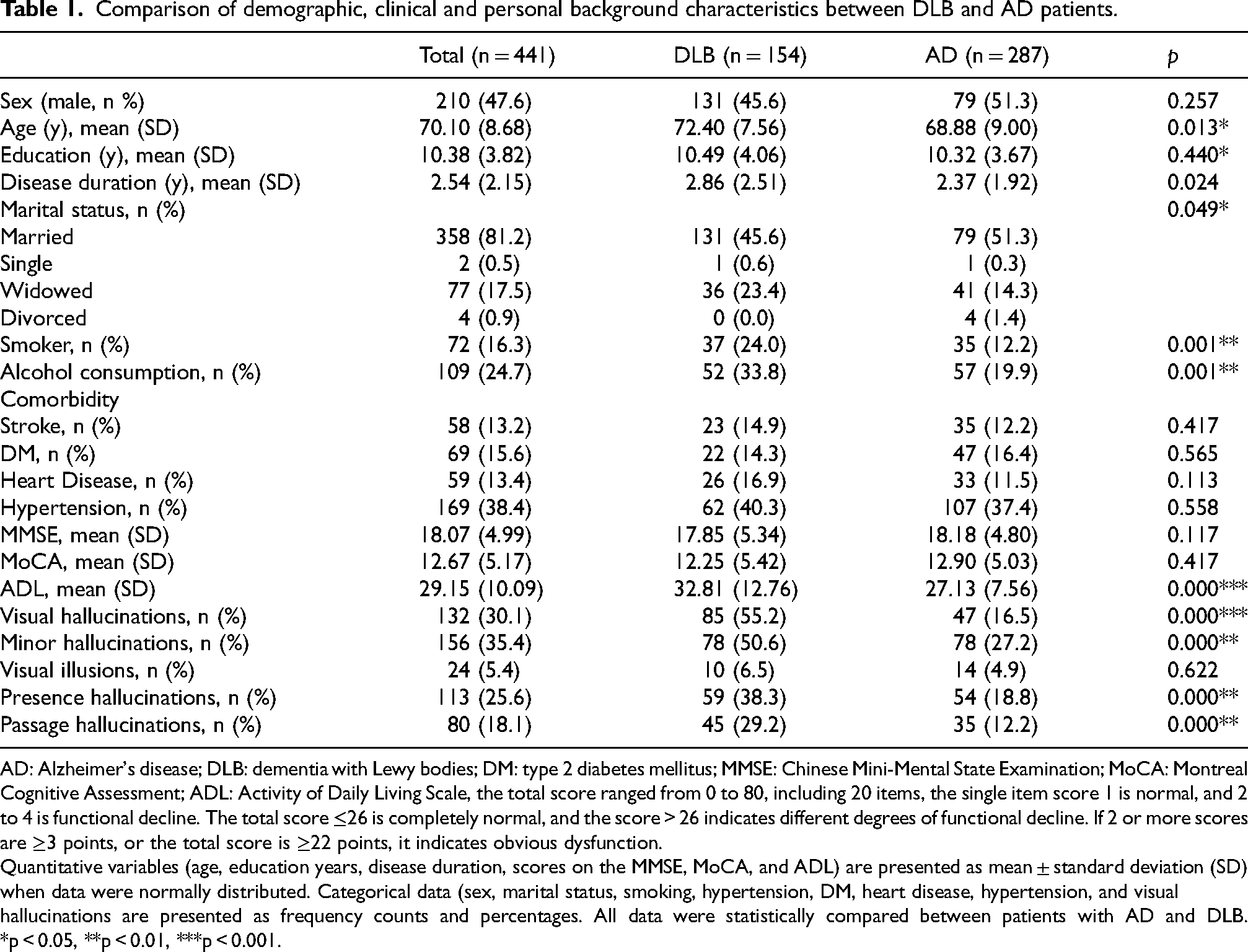
AD: Alzheimer's disease; DLB: dementia with Lewy bodies; DM: type 2 diabetes mellitus; MMSE: Chinese Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; ADL: Activity of Daily Living Scale, the total score ranged from 0 to 80, including 20 items, the single item score 1 is normal, and 2 to 4 is functional decline. The total score ≤26 is completely normal, and the score > 26 indicates different degrees of functional decline. If 2 or more scores are ≥3 points, or the total score is ≥22 points, it indicates obvious dysfunction.
Quantitative variables (age, education years, disease duration, scores on the MMSE, MoCA, and ADL) are presented as mean ± standard deviation (SD) when data were normally distributed. Categorical data (sex, marital status, smoking, hypertension, DM, heart disease, hypertension, and visual hallucinations are presented as frequency counts and percentages. All data were statistically compared between patients with AD and DLB. *p < 0.05, **p < 0.01, ***p < 0.001.
The prevalence of VH (55.2% versus 16.5%, p < 0.01) and MH (50.6% versus 27.7%, p < 0.01) was significantly greater in the DLB group compared to the AD group (Table 1). As for the MH subtype, the DLB group also had a significantly higher prevalence of presence hallucinations (PrH) (38.3% versus 18.8%, p < 0.01) and passage hallucinations (PH) (29.2% versus 12.2%, p < 0.01) compared to the AD group. Phenomenological profiles of VH exhibited distinct patterns between diagnostic groups. For participants who reported VH in both AD and DLB, the majority of VH consisted of human figures and were considered pleasant, there were also some differences in some items between the two groups (shown in Supplemental Table 1). VH in the DLB group manifested earlier, persisted longer, and had a higher frequency and severity compared to the AD group. However, there was no significant between-group difference regarding the caregiver distress caused by VH (Supplemental Table 2).
Association of VH with demographic and clinical features
The demographic and clinical features of DLB and AD patients with and without VH are summarized in Table 2. In both DLB and AD groups, patients’ age, sex, distribution, disease duration, years of education, and comorbidities were similar between VH and non-visual hallucination (NVH) groups. We further investigated the relationship between VH and other major symptoms of dementia. Within the DLB group, patients with VH had a higher prevalence of cognitive fluctuation symptoms (58.8% versus 33.3%, p < 0.01) but a lower prevalence of parkinsonism symptoms (63.5% versus 84.1%, p < 0.01) compared to NVH patients. In contrast, within the AD group, VH patients only had a significantly higher prevalence of RBD symptoms (14.9% versus 5.1%, p < 0.01). Cognitive fluctuation and parkinsonism symptoms did not differ significantly between VH and NVH patients in the AD group. Notably, DLB patients with VH and without VH both had a higher prevalence of cognitive fluctuation symptoms, parkinsonism symptoms, and RBD compared to the AD group (p < 0.01). Regarding drug treatments, notable differences were observed between DLB patients with and without VH. Levodopa was used more frequently by DLB patients without VH (14.5% versus 9.4%) compared to DLB patients with VH. In contrast, neuroleptics were used more frequently by DLB patients with VH (27.1% versus 18.8%) compared to DLB patients without VH. ChEIs drugs were used in a similar proportion of VH and NVH patients in the DLB group (69.4% and 58%, respectively), as well as in the AD group, and all were on stable therapeutic doses.
Demographic and clinical characteristics of patients in DLB and AD groups with or without VH.

AD: Alzheimer's disease; ADL: Activity of Daily Living Scale; DLB: dementia with Lewy bodies; DM: type 2 diabetes mellitus; RBD: rapid eye movement sleep behavior disorder; CDR: Clinical Dementia Rating: which is developed to measure the severity of dementia ranging from 0 to 3, with normal cognition being 0 and MCI being 0.5, and dementia being 1–3, higher CDR cores indicate more severity cognitive impairment; NPI: Neuropsychiatric Inventory: which is used to assess the presence and severity of specific Behavioral and Psychological Symptoms of Dementia (BPSD) experienced. BPSD symptoms assessed in the NPI (possible score 1–144) and caregiver stress (possible score 0–60). NPI-patients, NPI score of caregiver stress in caregiver; NPI-patients, NPI score of BPSD symptoms in patients. P1 refers to the comparison between “DLB without NVH” and “DLB with VH”; P2 refers to the comparison between “AD without NVH” and “AD with VH”; P3 refers to the comparison between “DLB with VH” and “AD with VH”. *p < 0.05, **p < 0.01, ***p < 0.001
As shown in Table 2 and Figure 1A, patients with VH in both the DLB and AD groups had higher ADL scores. This indicates that VH patients had a poorer ability to perform daily activities compared to NVH patients (DLB VH, 35.73 ± 12.76 versus DLB NVH 29.22 ± 10.71, and AD VH 31.85 ± 8.58 versus AD NVH 27.13 ± 7.56, p < 0.01). In the DLB group, VH patients had higher CDR scores (p < 0.05) than NVH patients, suggesting that VH may be associated with the overall disease severity. However, in the AD group, there was no significant difference in CDR scores between VH and NVH patients.
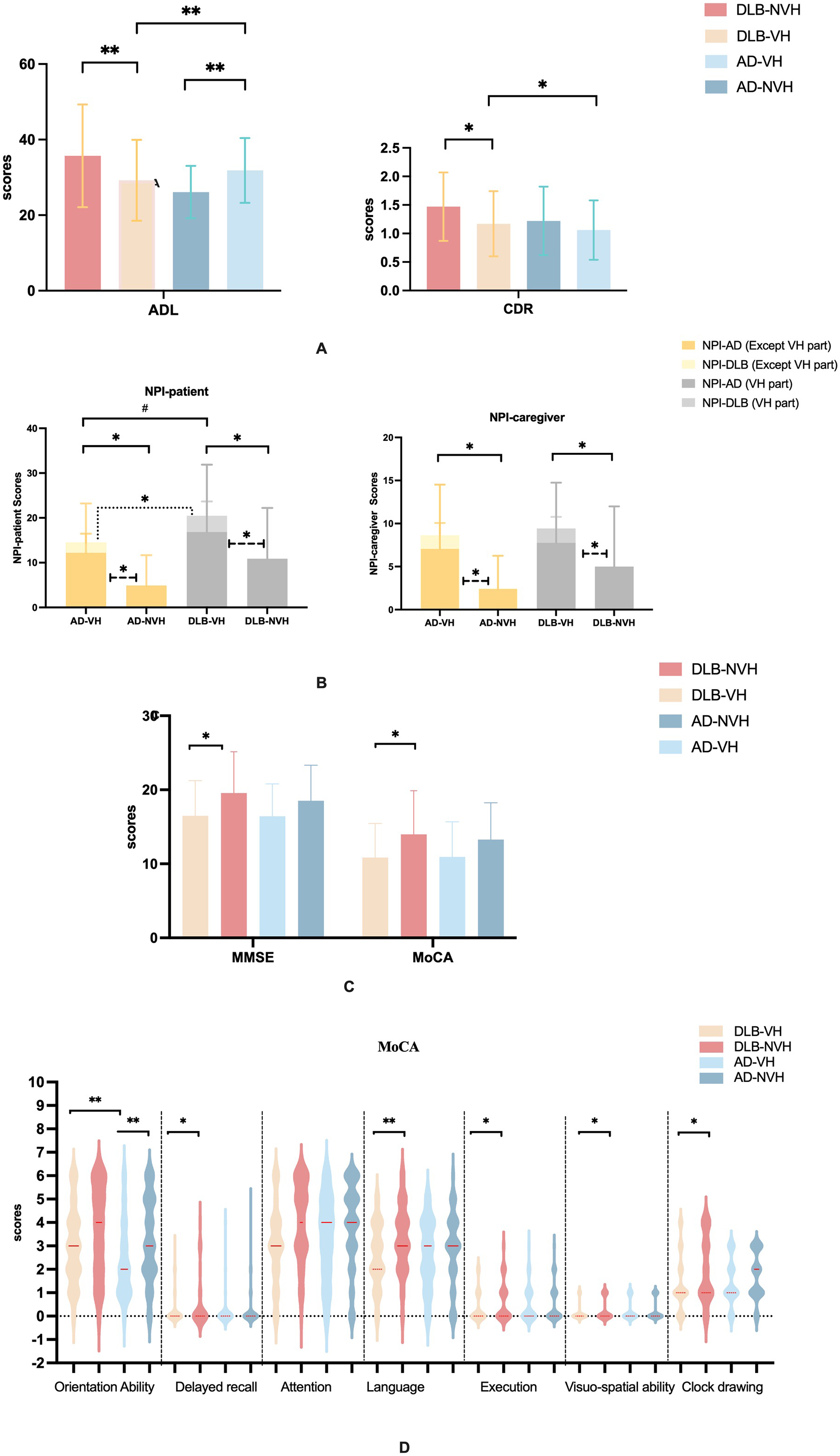
Neuropsychological assessments scores in DLB and AD patients with and without VH. Neuropsychological assessment scores in AD and DLB patients. The results of non-memory cognition neuropsychological (ADL and CDR) assessment scores between those with VH and NVH in AD and DLB groups are described in (A). The results neuropsychiatric disturbances (NPI) assessment scores between those with VH and NVH in AD and DLB groups are described in (B). The results of global cognition (MMSE and MoCA) assessment scores between those with VH and NVH in AD and DLB groups are described in (C). The results of different cognitive domains assessment scores between those with VH and NVH in AD and DLB groups are described in (D). AD: Alzheimer's disease; ADL: Activity of Daily Living Scale; CDR: Clinical Dementia Rating; DLB: dementia with Lewy bodies; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; NPI: Neuropsychiatric Inventory; NVH: non-visual hallucination; VH: visual hallucinations. *p < 0.01, **p < 0.05, ***p < 0.001.
As shown in Table 2 and Figure 1B, VH patients had higher total NPI scores than NVH patients in both the DLB (p < 0.01) and AD (p < 0.01) groups. Furthermore, the DLB VH group had higher NPI scores than the AD VH group (p < 0.05). After deducting the VH score from the NPI score, VH patients still had higher scores than NVH patients in both the DLB (p < 0.01) and AD (p < 0.01) groups. Furthermore, VH patients had higher total NPI caregiver scores and NPI caregiver scores with VH part deducted, compared to NVH patients, in both DLB (p < 0.05) and AD (p < 0.01) groups. Notably, our research suggests that VH may not be a specific neuropsychiatric symptom of AD, as VH patients in the AD group exhibited a wider range of neuropsychiatric disturbances than those in the DLB group (Supplemental Figure 2).
Cognitive neuropsychological findings
The results of the global cognition test for patients with AD and DLB are presented in Table 3 and Figure 1C. A comparison of DLB patients with and without VH revealed significant differences in cognitive function. Specifically, DLB patients with VH had lower MMSE scores (16.49 ± 4.74 versus 19.54 ± 5.59, p < 0.05) and lower MoCA scores (10.85 ± 4.59 versus 13.97 ± 5.88, p < 0.01) compared to DLB patients without VH. However, a comparison of VH and NVH groups in patients with AD revealed no significant differences in MMSE scores (p = 0.34) and MoCA scores (p = 0.98).
Global and different cognitive domain scores in neuropsychological tests of DLB and AD patients with and without VH.
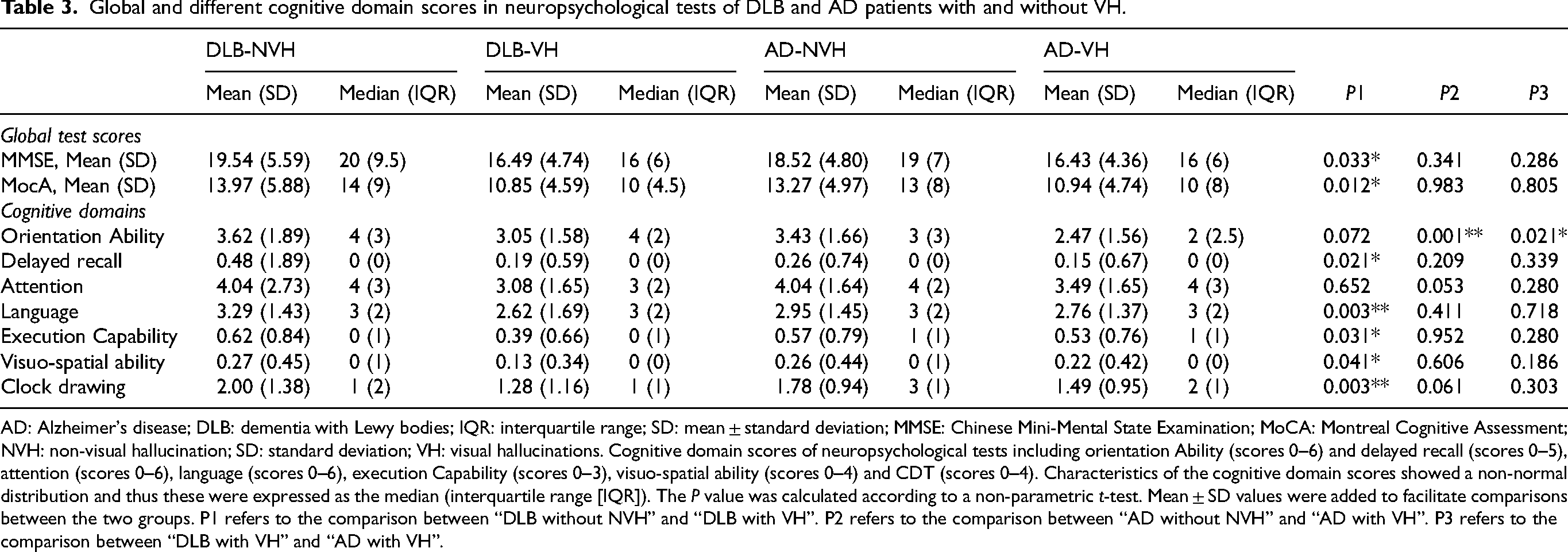
AD: Alzheimer's disease; DLB: dementia with Lewy bodies; IQR: interquartile range; SD: mean ± standard deviation; MMSE: Chinese Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; NVH: non-visual hallucination; SD: standard deviation; VH: visual hallucinations. Cognitive domain scores of neuropsychological tests including orientation Ability (scores 0–6) and delayed recall (scores 0–5), attention (scores 0–6), language (scores 0–6), execution Capability (scores 0–3), visuo-spatial ability (scores 0–4) and CDT (scores 0–4). Characteristics of the cognitive domain scores showed a non-normal distribution and thus these were expressed as the median (interquartile range [IQR]). The P value was calculated according to a non-parametric t-test. Mean ± SD values were added to facilitate comparisons between the two groups. P1 refers to the comparison between “DLB without NVH” and “DLB with VH”. P2 refers to the comparison between “AD without NVH” and “AD with VH”. P3 refers to the comparison between “DLB with VH” and “AD with VH”.
The characteristics of the main subitems of MoCA are summarized in Table 2 and Figure 1D. In patients with DLB, those with VH had significantly lower scores in the Language subitem and Clock drawing subitem compared to those without VH (DLB-NVH) (p < 0.01). Additionally, DLB-VH patients had lower scores for visuo-spatial ability and Delayed recall and Execution Capability subitem compared to DLB-NVH patients (p < 0.05). However, no significant differences were found between the DLB-VH and DLB-NVH groups regarding Orientation Ability and Attention subitems. In patients with AD, no significant differences were found between those with VH and those without VH for most MoCA subitems. The only exception was the Orientation Ability subitem for which the score was significantly lower in AD-VH patients (p < 0.05). Comparing patients with VH across DLB and AD groups, those with DLB showed lower scores only in the Orientation Ability subitem compared to those with AD (p < 0.05). The scores for the main subitems are summarized in Supplemental Figure 3.
The effects of VH on the cognitive function of patients in the DLB and AD groups were evaluated using multiple linear regression analysis (Figure 2). After adjusting for common dementia risk factors, including sex, age, education, disease duration, stroke, DM, heart disease, hypertension, RBD, parkinsonism, and cognitive fluctuation (model 2), the presence of VH was identified as a predictor of lower MMSE scores in patients with DLB or AD (Beta: −2.377, p < 0.01 and Beta: −2.365, p < 0.01). Furthermore, the VH group was associated with lower MoCA scores in both DLB (Beta: −2.588, p < 0.01) and AD groups (Beta: −2.590, p < 0.01), compared to the NVH group. Furthermore, we included cognitive domain variables of MoCA, which were significant in model 2, in the regression analysis. For patients with DLB, further adjustments were made in model 3 for Attention, Language, Clock drawing test, and Visuo-spatial ability. The results showed that VH were responsible for lower scores in Attention (Beta: −0.531, p = 0.045). In AD, the association between Orientation Ability subitems and VH remained significant (Beta: −0.635, p = 0.013), after adjusting for age, sex, education, disease duration, marital status, stroke, DM, heart disease, hypertension, RBD, parkinsonism, cognitive fluctuation, and attention. Furthermore, the association between the orientation ability subitems of the MMSE and VH in AD remained significant after adjustment (Beta: −0.153, p < 0.05), which verified the stability of this finding (Supplemental Figure 4).

Association between neuropsychological test scores and VH in patients with DLB or AD. The standardized coefficient and 95% confidence interval results of the association of cognitive scores between VH and DLB groups are described. AD: Alzheimer's disease; DLB: dementia with Lewy bodies; MMSE: Chinese Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; VH: visual hallucination. *p < 0.05, **p < 0.01, ***p < 0.001. Model 1: unadjusted model. Model 2: adjustment for sex, age, education, disease duration, stroke, DM, heart disease, hypertension, RBD, Parkinsonism and Cognitive fluctuation. Model 3 in DLB: adjustment for sex, age, education, disease duration, stroke, DM, heart disease, hypertension, RBD, Parkinsonism, Cognitive fluctuation, Attention, Language, Clock drawing, and Visuo-spatial ability of MMSE. Model 3 in AD: adjustment for sex, age, education, disease duration, stroke, DM, heart disease, hypertension, RBD, Parkinsonism, Cognitive fluctuation, Attention, Orientation Ability and Visuo-spatial ability of MMSE.
The impact of MH on the cognitive function in DLB and AD groups was also examined using multiple linear regression analysis (Supplemental Figure 5). Compared to patients without MH, those with MH had significantly lower MMSE and MoCA scores (p < 0.01) in both DLB and AD groups, even after adjusting for confounding factors. However, when cognitive domain variables were further included in the analysis, there was no significant association between MH and the cognitive domains.
Cognitive domains mediate the relationship between VH and global cognitive function
The mediation analysis results are presented in Figure 3. In DLB patients, the association between VH and cognition was partially mediated by attention function. In AD patients, the association between VH and cognition was partially mediated by orientation function. In DLB patients, attention function significantly mediated the relationship between VH and global cognition function, as measured by both MMSE and MoCA scores, accounting for 85.9% and 85.3% (respectively) of the effect after adjustment (p < 0.05) (Figure 3(a)). In AD patients, orientation function significantly mediated the relationship between VH and global cognitive function. As shown in Figure 3(b), the orientation function of MoCA mediated 86.9% and 69.3% of the effects of VH on global cognitive function, as measured by MMSE and MoCA scores, respectively (p < 0.05). Similar results were obtained using the orientation function of MMSE, which mediated 80.4% and 62.0% of the association between VH and global cognitive function (p < 0.05), as shown in Figure 3(c). Furthermore, the analysis explored the mediating effect of core symptoms on the relationship between VH and cognitive function. The results showed no mediating effect of RBD and parkinsonism. However, VH was found to mediate the relationship between cognitive fluctuation and cognitive function in both DLB (Figure 3(d)) and AD (Figure 3(e)) patients. Detailed descriptions of the mediation analyses and sensitivity analyses are provided in Supplemental Tables 3 and 4 and Supplemental Figure 6.

Mediation factor of VH and global cognition functional in DLB and AD patients. Mediation analysis model adjusted for the common risk factors of dementia, including sex, age, education, disease duration, stroke, diabetes mellitus, heart disease, hypertension, rapid eye movement sleep behavior disorder, parkinsonism, and cognitive fluctuation. (a) DLB: Mediation models of VH, attention, and global cognitive function (MMSE/MoCA scores): Direct effect (−0.352, p = 0.654) / (−2.097, p < 0.001) of VH on MMSE/MoCA scores. Indirect effect (−0.442, p = 0.574) / (−2.321, p < 0.001) of VH on MMSE/MoCA scores through attention. (b) AD: Mediation models of VH, orientation (MoCA), and global cognitive function (MMSE and MoCA scores): Direct effect (−0.682, p = 0.420) / (−0.760, p = 0.184) of VH on MMSE/MoCA scores. Indirect effect (−1;704, p = 0.004) / (−1.819, p = 0.002) of VH on MMSE/MoCA scores through orientation. (c) AD: Mediation models of VH, orientation (MMSE), and global cognitive function (MMSE and MoCA scores): Direct effect (−0.456, p = 0.390) / (−1.001, p = 0.090) of VH on MMSE/MoCA scores. Indirect effect (−1.993, p < 0.001) / (−1.574, p = 0.002) of VH on MMSE/MoCA scores through orientation (MMSE). (d) DLB: Mediation models of cognitive fluctuation, VH, and global cognitive function (MMSE and MoCA scores): Direct effect (−1.249, p = 0.168) / (−0.790, p = 0.430) of VH on MMSE/MoCA scores. Indirect effect (−0.559, p = 0.024) / (−0.610, p = 0.030) of VH on MMSE/MoCA scores through cognitive fluctuation. (e) AD. Mediation models of cognitive fluctuation, VH, and global cognitive function (MMSE and MoCA scores): Direct effect (−1.205, p = 0.10) / (−2.767, p = 0.016) of VH on MMSE/MoCA scores. Indirect effect (−0.650, p = 0.020) / (−0.653; p = 0.020) of VH on MMSE/MoCA scores through cognitive fluctuation. AD: Alzheimer's disease; DLB: dementia with Lewy bodies; MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; VH: visual hallucinations. *p < 0.01, **p < 0.05, ***p < 0.001.
Discussion
Our study found a significantly higher prevalence of VH and MH in patients with DLB compared to those with AD, which is consistent with previous studies. Matar et al. reported a 50% prevalence of VH in patients with DLB.21,22 Earlier research has shown that patients with DLB tend to have higher NPI scores and are more likely to experience VH than those with AD. 23 Regarding MH, a previous study found that 21.1% of AD patients experienced MH, with the most common types being PrH (16.7%), followed by PH (10.0%) and illusions (0.7%), which is similar to our study. 24 The lack of research on MH in DLB patients may be attributable to the presence of VH masking the findings of MH. The presence of VH in AD patients can lead to a misdiagnosis of DLB, especially when combined with other core symptoms such as RBD and parkinsonism. In the present study, 44.8% of patients who met the diagnostic criteria for DLB did not experience VH. Impaired visual acuity is strongly associated with VH in many eye diseases, such as Charles Bonnet syndrome. Therefore, patients with uncorrected visual dysfunction were excluded from this study to avoid confounding.
In this study, the presence of VH in patients with DLB was associated with parkinsonism and cognitive alterations, whereas in AD patients, the presence of VH was associated with RBD, but not with older age, later illness onset, or longer disease duration. Additionally, caregivers of patients with VH in both DLB and AD groups reported significantly higher scores on the NPI, indicating greater caregiving stress. This is consistent with existing literature, which suggests that caregiver distress increases as patients’ cognition declines. 25 The occurrence of VH can have significant implications for patients and caregivers, particularly in the early stages of the disease when insight and cognitive function are still preserved. As the disease progresses, VH can precipitate a transition from independent living to care. 26 The study highlights the importance of providing support to both patients and caregivers, focusing on raising awareness of VH and treatment options through early intervention. As the disease progresses, support should shift to addressing caregiver needs and alternative strategies to reassure individuals experiencing VH. 27
The main finding of our study was the association of VH with poorer cognitive functions in patients with DLB and AD. In patients with DLB, this association was mainly observed in attentional executive function, whereas in patients with AD, it was primarily seen in orientation. Previous studies have reported similar findings, indicating that VH in patients with DLB are associated with deficits in visual attention and executive functions, against a background of slightly worse global cognitive performance. 28 Some studies have also shown that DLB patients with VH perform worse on visual-perception tests, independent of visual attention abilities. 29 Consistently, research has identified verbal immediate memory performance as a predictor of VH development in DLB patients. 30 Our study extends these findings by demonstrating that different cognitive domains mediate the relationship between VH and global cognitive function in DLB and AD patients. In fact, Onofrj et al. characterized DLB and Parkinson's disease as attentional, executive, and visual-perception dementias, which aligns with our findings. 7 However, few studies have specifically investigated VH in patients with AD. One study in AD patients reported associations of VH with more severe impairments in executive functioning, verbal, visuo-spatial, and semantic memory, as well as more severe global cognitive impairment. 31 Our research confirms the association between VH and global cognitive functional decline in both DLB and AD patients. However, the relationship between VH and specific cognitive domains is still debatable, necessitating further prospective investigations. Notably, our study found that DLB and AD patients exhibit different cognitive profiles for minor and complex hallucinations, suggesting differences in pathophysiology. However, the association between MH and cognitive characteristics remains unclear and warrants further research.
Research on degenerative dementia has identified several neuroanatomical correlates of VH. Medial temporal lobe atrophy exhibited a modest association with VH, while white matter lesions have shown a strong association with neuropsychiatric symptoms, including VH, in AD and DLB. 32 A previous study found regions of smaller gray matter volume in hallucinating patients in occipital, occipitotemporal, medial frontal, and inferior parietal areas, predominantly along the midline of the brain. 33 Functional imaging studies have reported abnormalities in brain activity and blood flow in hallucinating patients. Occipital and occipitotemporal hypometabolism or hypoperfusion have been observed in hallucinating patients with PD and DLB.34,35 Cagnin et al. found that DLB patients with VH had a higher burden of Lewy body pathology in the inferior temporal and parahippocampal cortex, and the amygdala. 28 One study found a correlation between tangle density in the frontal cortex and psychosis in AD patients, although this study included patients with both delusions and hallucinations. 36 Another study revealed that, even in AD, VH were associated with cortical alpha-synucleinopathy. 37 The destruction of brain structure and extensive pathological deposits in VH patients may contribute to cognitive decline. Mixed degenerative pathologies, such as AD or Lewy body disease combined with cerebrovascular disease, are highly prevalent according to pathological studies.38,39 Some of these studies also revealed a high prevalence of cerebrovascular pathologies in the brains of patients with AD and Lewy body disease.32,40 The deposition of cerebrovascular lesions in the brain areas related to visual hallucinations may contribute to VH in AD. Lewy body pathology has been found in some patients with AD, suggesting the existence of an AD + Lewy body phenotype characterized by dementia, delusions, hallucinations, and severe motor impairment. Visual hallucinations have been identified as the most specific clinical symptom differentiating DLB from AD in the early stages. They are also the only feature suggesting the presence of Lewy bodies in cases with mixed AD/LB pathology.41–43 This may provide possible hypothesis for us to study the underlying neuropathology of VH.
In this study, we found differences between patients with AD and DLB regarding the association between VH and specific cognitive domains, suggesting potential similarities or differences in the underlying processes of VH between these patient groups. The phenomenological characteristics of hallucinations are not solely attributed to pathology within specific regions, such as specific cortical sites or sensory end organs. Instead, they are thought to arise from dysfunction across networks that integrate and assess information. 44 Eight models of VH have been published since 2000, including Deafferentation, Reality Monitoring, Perception and Attention Deficit (PAD), Activation, Input, and Modulation, Hodological, Attentional Networks, Active Inference, and Thalamocortical Dysrhythmia Default Mode Network Decoupling. The most widely accepted model is the PAD model or related variants. The PAD model suggests that VH results from combined impairments in distributed perceptual and attentional networks, leading to disturbed balances between top-down and bottom-up processes (or priors and sensory evidence). The production of hallucinations is significantly influenced by neurotransmitters.45,46 Each of these models has its advantages and may overlap to some extent. To reconcile different approaches to explaining VH, Collerton et al. developed a new conceptual VH framework. This framework sets boundaries around relevant cognitive systems, allowing theories to be compared or integrated more easily. 47 A previous study has found that impairment of orientation in AD may relate to functional connectivity changes between the posterior cingulate cortex and ventral attention network, as well as hypoperfusion of the posterior cingulate cortex. The dysfunction across networks integrating and assessing information caused by VH may differ between AD and DLB. 48 Notably, the location and spread of pathologic deposits differ between AD and DLB. In AD, tangle density begins in the transition zone between the entorhinal cortex and the hippocampus, then travels through the cingulate gyrus, lateral temporal lobe, frontal lobe, and parietal lobe, and finally to the occipital lobe. This difference in pathology may contribute to the distinct associations between cognitive domains and VH observed in AD and DLB. 49 Further clinical studies are required to elucidate the cognitive mechanisms underlying VH in DLB and AD.
Cognitive function demonstrates significant clinical associations with MH in neurological patients. Neuropsychological assessments reveal a correlation between poorer cognitive performance scales (MoCA/MMSE) and MH. The neurocognitive mechanism underlying this association involves three key pathways: 1) Impaired sensory integration from degraded prefrontal cortex filtering, leading to stimulus misinterpretation; 2) Compromised reality monitoring in temporal-parietal networks causing self-awareness deficits; 3) Dysfunctional thalamocortical gating permitting intrusive mental imagery.50,51 This neural dysregulation creates a cognitive-perceptual mismatch where internally generated representations are erroneously attributed to external sources. Despite these pathophysiological insights, MH research faces many challenges. The neurocognitive mechanisms linking MH to specific cognitive domains remain poorly characterized, necessitating enhanced standardized assessment protocols to advance mechanistic investigations in this understudied field.
Our study's strengths lie in its large sample size of patients with DLB, which was well balanced for the presence of VH, and the comparison with AD patients as a control group. VH are a common psychiatric behavioral symptom in patients with AD and DLB. However, previous research on VH has primarily involved patients with PD, leaving a knowledge gap regarding VH in AD and DLB patients. Our study addressed this gap by investigating the relationship between VH and overall cognitive functioning in patients with AD and DLB. We further analyzed the effects of different sub-cognitive domains using the MoCA scale, which is a widely used neuropsychological assessment in clinical settings. The use of the MoCA scale enhances the generalizability and clinical usability of our findings. While this study has yielded important insights, it is essential to consider the limitations of our research to inform future studies. First, our study only included patients who underwent an initial assessment, and we lacked relevant follow-up data to examine the longitudinal relationship between VH and cognitive decline. Second, our study relied solely on MoCA and MMSE subitems to investigate the cognitive domains associated with VH and lacked a more comprehensive cognitive domain and VH assessment scale. Drawing conclusions based solely on MoCA and MMSE items is insufficient, while the MoCA and MMSE demonstrate moderate diagnostic generalizability and clinical utility, their suboptimal accuracy in cognitive impairment detection limits their reliability as standalone diagnostic tools. The neuropsychological assessment landscape necessitates expanded domain-specific instrumentation, exemplified by attentional metrics like the Digit Span Test and executive function evaluations such as the Behavioral Assessment of Dysexecutive Syndrome and so on. Our future studies would make efforts to develop comprehensive cognitive domain and establish standardized VH assessment, as well as conducting thorough follow-up investigations.
Conclusion
Our study provides preliminary evidence that VH are more prevalent in patients with DLB compared to those with AD. We found that VH may be independently associated with global cognitive functional decline in both DLB and AD patients. Our results suggest that impairment in attentional function is more pronounced in DLB patients with hallucinations, whereas in AD patients, it primarily affects orientation function. This distinction in cognitive domain impairment may help differentiate between DLB and AD patients with VH, facilitating research into the underlying mechanisms of VH production in these two conditions. Future longitudinal studies are necessary to investigate the potential causative role of VH in DLB and AD.
Supplemental Material
sj-docx-1-alr-10.1177_25424823251339132 - Supplemental material for Association between visual hallucinations and cognitive performance in Lewy body dementia and Alzheimer's disease: A cross-sectional study
Supplemental material, sj-docx-1-alr-10.1177_25424823251339132 for Association between visual hallucinations and cognitive performance in Lewy body dementia and Alzheimer's disease: A cross-sectional study by Yaqi Yang, Fan Yang, Jinghuan Gan, Shuai Liu, Chen Wen, Lixin Liu, Tianjiao Ren, Jiarui Wang and Yong Ji in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
All authors would like to thank the study participants for their generous participation and contribution of time. The present study was supported by the Tianjin Science and Technology Plan Project [grant number 22ZYCGSY00840], Science and Technology Project of Tianjin Municipal Health Committee [grant number ZC20121], National Natural Science Foundation of China [grant number 82171182] and Tianjin Key Medical Discipline (Specialty) Construction Project (grant number TJYXZDXK-052B).
ORCID iDs
Ethical considerations
The study was approved by the ethics committees of Tianjin Huanhu Hospital (2023-158) and the Tianjin Health Bureau. Consent was obtained from all participants in the study.
Consent to participate
All the participants declared their consent to this research.
Consent for publication
Not applicable.
Author contributions
Yaqi Yang (Data curation; Formal analysis; Investigation; Methodology; Writing – original draft; Writing – review & editing); Fan Yang (Data curation; Formal analysis; Writing – review & editing); Jinghuan Gan (Conceptualization; Validation; Writing – review & editing); Shuai Liu (Data curation; Funding acquisition; Writing – review & editing); Chen Wen (Investigation); Lixin Liu (Investigation; Methodology); Tianjiao Ren (Investigation); Jiarui Wang (Investigation); Yong Ji (Conceptualization; Funding acquisition).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present study was supported by the National Natural Science Foundation of China (82171182), the Tianjin Science and Technology Plan Project (22ZYCGSY00840), Tianjin Municipal Education Commission Research projects [grant number 2023KJ060], Tianjin Health Research Project [grant number TJWJ2022MS032 and TJWJ2023QN060), and Tianjin Key Medical Discipline (Specialty) Construction Project [grant number TJYXZDXK-052B]. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.