
Abstract
Spinocerebellar ataxia type 8 (SCA8) is an autosomal dominant neurodegenerative disorder caused by CTG/CAG repeat expansion in ATXN8OS/ATXN8 genes. The primary clinical feature is cerebellar ataxia, but approximately 30% of patients present with cognitive impairment, characterized by attentional disturbances and executive dysfunction. These cognitive deficits remain poorly understood, and no functional neuroimaging studies have been reported. We report a case of SCA8 presenting predominantly with cognitive impairment and showing marked hypoperfusion in the posterior cingulate cortex (PCC) on N-isopropyl-p-[123I]-iodoamphetamine single-photon emission computed tomography, closely resembling early-onset Alzheimer's disease. This case suggests PCC dysfunction may contribute to cognitive decline in SCA8.
Keywords
Introduction
Spinocerebellar ataxia type 8 (SCA8) is a slowly progressive, autosomal dominant neurodegenerative disorder caused by CTG/CAG repeat expansion in the ATXN8OS/ATXN8 genes. 1 Pathogenic mechanisms involve the intracellular accumulation of toxic RNAs and proteins produced by bidirectional expression of both genes: CUG-expanded RNA transcribed from ATXN8OS, 2 polyglutamine proteins translated from ATXN8 via ATG-initiated transcription, 3 and polyalanine and polyserine proteins derived from ATXN8 through repeat-associated non-AUG (RAN) translation.4,5
While cerebellar ataxia is the most common initial manifestation of SCA8, some patients also exhibit extracerebellar symptoms such as cognitive impairment, pyramidal and extrapyramidal signs, and sensory neuropathy. 1 Although the prevalence of cognitive dysfunction in patients with SCA8 has not been systematically evaluated, a review of previously reported cases identified cognitive impairment in 26 of 88 patients (30%). 6 Among the affected cognitive domains, impairments in attention, information processing, and executive function are particularly prominent. 7 However, the neural substrates underlying cognitive dysfunction in SCA8 remain poorly understood, and to date, no studies have assessed these associations using functional neuroimaging. Furthermore, no patients have been reported in whom cognitive decline was the primary manifestation and described within the context of dementia.
Here, we report a case of SCA8 presenting with cognitive impairment, in which N-isopropyl-p-[123I]-iodoamphetamine single-photon emission computed tomography (123I-IMP-SPECT) revealed hypoperfusion in the posterior cingulate cortex (PCC), mimicking the clinical manifestations of Alzheimer's disease (AD).
Case presentation
A 59-year-old Japanese man who was employed in warehouse operations was referred to our department for evaluation of cerebellar atrophy. Approximately six months prior to presentation, he began experiencing difficulty in controlling a forklift and exhibited delayed comprehension and response to verbal instructions. He denied any speech disturbances or gait abnormalities. The patient was admitted to another hospital following a workplace accident in which he fell from a platform because of inattention, resulting in rib fractures. Head CT performed during admission revealed cerebellar atrophy, prompting a referral to our facility. His medical history was unremarkable, and he was not taking any medications regularly. Alcohol consumption was limited to occasional drinking. He had completed 12 years of formal education in Japanese, graduated from high school as his highest educational attainment, and was a monolingual Japanese speaker. He had performed well in physical education during childhood. The patient had no family history of similar symptoms. His 86-year-old mother required a walker for lumbar kyphosis without any diagnoses of neurodegenerative disorders, whereas his 88-year-old father and two younger brothers exhibited no neurological symptoms.
On examination, the patient was cooperative but showed impaired comprehension, frequently providing tangential responses to the questions. Mild ataxic dysarthria was observed; however, ocular movements were intact, and limb ataxia was not evident. Mild rigidity was detected in both the upper extremities, accompanied by bilateral freezing during finger tapping and bradykinesia during toe tapping. Sensory examination results and tendon reflexes were normal. Gait, including tandem walking, was unremarkable. The Scale for the Assessment and Rating of Ataxia (SARA) score was 4.5 out of 40. Neuropsychological testing revealed a Mini-Mental State Examination (MMSE) score of 21/30 (with losses in serial 7 s, three-step command, and construction), a Frontal Assessment Battery (FAB) score of 6/18, and an Addenbrooke's Cognitive Examination-III (ACE-III) total score of 78/100 (attention: 13/18, memory: 22/26, fluency: 7/14, language: 23/26, and visuospatial: 13/16), indicating significant impairments in attention and executive function. All tests were administered as Japanese versions with established validity and reliability.
Laboratory investigations revealed normal levels of vitamins B1, B12, and folate. Autoantibodies, including anti-thyroid peroxidase, anti-thyroglobulin, and anti-glutamic acid decarboxylase 65 tested negative. Brain MRI revealed mild atrophy of the superior cerebellar hemispheres and bilateral parietal lobes, with preservation of the brainstem, cerebellar peduncles, and hippocampus (Figure 1). 123I-IMP-SPECT revealed mild cerebellar and prominent PCC hypoperfusion (Figure 2). Cerebrospinal fluid (CSF) analysis revealed an amyloid-β 1-42/1-40 ratio of 0.105 (reference ≥0.067), phosphorylated tau level of 32.1 pg/mL (reference 21.5–59.0 pg/mL), and total tau level of 219 pg/mL (reference 146–410 pg/mL) —all within normal ranges. Genetic panel testing for spinocerebellar ataxia (SCA1, 2, 3, 6, 7, 8, 12, 17, 31, and dentatorubral-pallidoluysian atrophy) revealed a heterozygous CTG/CAG repeat expansion of 24/119 in the ATXN8OS/ATXN8 gene (normal: 15–50; pathogenic: > 71). 1 No pathogenic repeat expansions were detected at any of the other tested loci. Based on these findings, the diagnosis of SCA8 was established.

Brain magnetic resonance imaging (MRI). Brain MRI shows mild atrophy in the superior cerebellar hemispheres and bilateral parietal lobes. No apparent atrophy was observed in the brainstem, cerebellar peduncles, or hippocampi. (a-c) Axial T1-weighted images; (d, e) Sagittal 3D-FLAIR images; (f) Coronal 3D-FLAIR images.
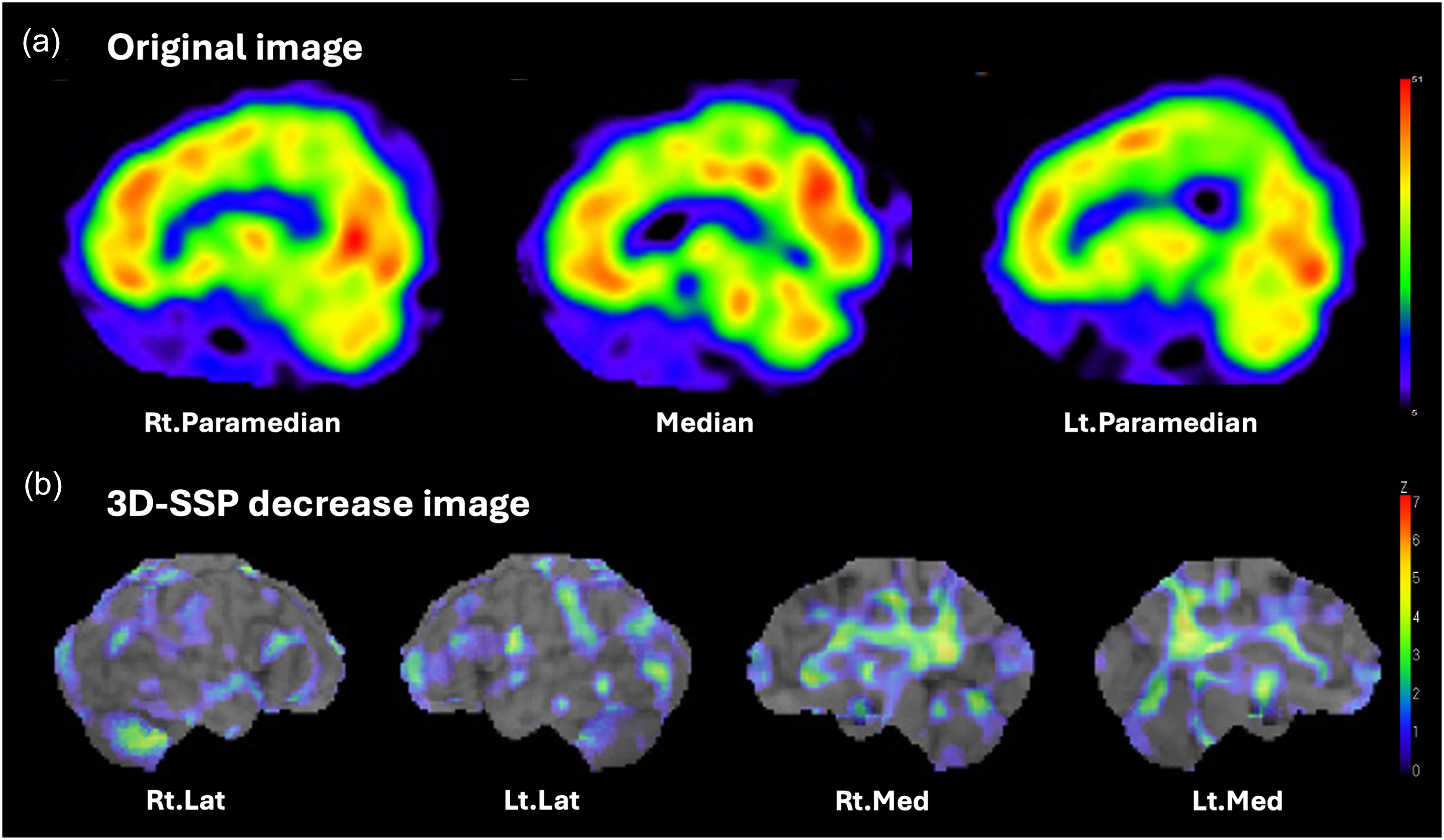
N-isopropyl-p-[123I]-iodoamphetamine single-photon emission computed tomography (123I-IMP-SPECT). 123I-IMP-SPECT revealed mild hypoperfusion of the superior cerebellum and marked hypoperfusion of the posterior cingulate cortex. (a) Sagittal view of the original image. (b) Decrease map generated by three-dimensional stereotactic surface projection (3D-SSP) with global normalization.
Discussion
The patient was diagnosed with SCA8 based on the presence of slowly progressive cerebellar ataxia and atrophy, and pathogenic heterozygous CTG/CAG repeat expansion in the ATXN8OS/ATXN8 genes. The absence of a family history may be attributed to the incomplete penetrance and intergenerational instability of ATXN8OS/ATXN8 repeat expansions.8,9 In addition to the motor symptoms, the patient exhibited cognitive dysfunction, particularly in attention and executive functions. Neuroimaging revealed bilateral parietal lobe atrophy on MRI and marked PCC hypoperfusion on 123I-IMP-SPECT. Common etiologies of treatable dementia were excluded, and CSF biomarkers for amyloid pathology did not support the diagnosis of AD. These findings suggest that cognitive impairments can be attributed to SCA8.
PCC dysfunction may contribute to cognitive impairment in SCA8. The PCC is a highly connected and metabolically active brain region that functions as a central hub for information integration across the brain. 10 The ventral PCC is closely connected to the default mode network and plays a key role in internally directed cognition such as memory retrieval and planning. 11 In contrast, the dorsal PCC is strongly linked to dorsal attention and frontoparietal control networks, contributing to externally directed attention and executive control. 11 By modulating activity across these networks, the PCC is thought to regulate the dynamic balance of attention along both the internal-external and broad-narrow dimensions. 12 Clinically, structural disruption of the PCC is associated with deficits in sustained attention following traumatic brain injury. 13 Notably, PCC hypoperfusion observed in the present case may reflect either direct structural pathology within the PCC, as observed in AD, or diaschisis due to connected network pathology. 12 Postmortem studies of SCA8 have revealed widespread neuronal loss and gliosis in the cerebral cortex, along with polyglutamine-positive cytoplasmic inclusions. 14 Additional reports have described the accumulation of polyserine proteins due to RAN translation in the frontal white matter, which causes demyelination and axonal degeneration. 5 However, a direct pathology of PCC has not been documented. Although brain functional alterations in patients with SCA8 remain poorly understood, a mouse model of SCA8 has shown marked alterations in functional connectivity in the retrosplenial cortex, analogous to the human PCC. 15 Therefore, cognitive impairment in patients with SCA8 may result from degenerative changes affecting the PCC or associated neural networks.
In SCA8, cognitive impairment can occasionally be more pronounced than cerebellar ataxia. The clinical manifestations of SCA8 are highly variable. Previous reports have described cases of minimal cerebellar ataxia that mimicked spastic paraplegia, amyotrophic lateral sclerosis, or Parkinson's disease.16,17 Although no case of SCA8 with cognitive decline as the predominant symptom has been reported, a dissociation between the severity of cognitive and motor symptoms has been observed in a case series of SCA8. 7 For the present patient, we used Crawford and Howell's modified t-test 18 to accurately quantify the degree of abnormality in each neurological assessment score (Table 1). For normative references, we selected datasets from the available sources that most closely matched the patient's demographic profile: SARA from 53 healthy controls aged 50–59 years 19 ; MMSE from 203 healthy Japanese controls aged 55–59 years with 6–12 years of education 20 ; FAB from 25 healthy Japanese controls aged 63.7 ± 2.4 years with 12.0 ± 2.5 years of education 21 ; and ACE-III from 74 healthy Japanese controls aged 72.1 ± 7.1 years with 12.9 ± 2.3 years of education. 22 The results showed that MMSE and FAB scores were more abnormal than the SARA score (t = −6.52, −5.52 and 4.62, respectively), which indicates that cognitive impairment was more pronounced than cerebellar ataxia. Domain-specific analysis of ACE-III revealed substantial deficits in attention and visuospatial functions, while memory was relatively preserved (t = −3.88 and −3.69, and −0.72, respectively).
Neurological and cognitive assessment scores of the patient compared with normative data.

SARA: Scale for the Assessment and Rating of Ataxia; MMSE: Mini-Mental State Examination; FAB: Frontal Assessment Battery; ACE-III: Addenbrooke's Cognitive Examination-III; SD: standard deviation; N: number.
*Normative data sources are indicated in the Reference column.
†p values calculated using Crawford & Howell's modified t-test (one-tailed).
The clinical presentation of SCA8 resembles that of early-onset AD. Unlike late-onset AD, which is typically characterized by memory impairment, early-onset AD (<65 years) often presents with atypical phenotypic variants. 23 It is characterized by relatively mild memory deficits and prominent impairments in attention, executive function, and visuospatial skills. Neuroimaging in such cases typically reveals less hippocampal atrophy but more marked parietal-dominant neocortical atrophy on MRI and more pronounced parietal hypometabolism on FDG-PET. Although the mild cerebellar ataxia in the present patient provided a clue for the differential diagnosis of SCA, the neuropsychological test results and neuroimaging findings were consistent with the characteristic features of early-onset AD.
Conclusion
Cognitive impairment is a relatively common but underexplored manifestation of SCA8. The present case highlights the potential contribution of PCC dysfunction to cognitive decline in this disorder. Furthermore, this case expands the clinical spectrum of SCA8 by closely mimicking early-onset AD with prominent cognitive deficits accompanied by minimal cerebellar ataxia. Such atypical presentations may easily be overlooked in clinical practice, underscoring the importance of comprehensive neurological assessments, including careful evaluation of cerebellar signs, in the diagnostic workup for dementia.
Footnotes
Acknowledgements
This work was partly supported by grants-in-aid from the Research Committee of Ataxia, Health Labor Sciences Research Grant, and the Ministry of Health, Labor and Welfare, Japan (grant no. JPMH20FC1041) and the Japan Agency for Medical Research and Development (AMED) under Grant Number: JP21ek0109532h0001. The authors thank the patient for kindly agreeing to participate in this case report. We also would like to thank Editage (![]() ) for English language editing.
) for English language editing.
Ethical considerations
This study followed the ethical guidelines of the Declaration of Helsinki.
Consent to participate
Informed consent was obtained from the patient, who was an adult with sufficient decision-making capacity.
Consent for publication
Written informed consent was obtained from the patient for the publication of this case report and the accompanying images.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Any data not published in the article will be anonymously shared upon reasonable request by a qualified investigator.