
Abstract
Background
“Unités de réadaptation cognitivo-comportementale (URCC)” are specialized units for patients with Alzheimer's disease or related dementias presenting behavioral disorders. Falls are frequent in these settings, with dementia increasing fall risk six-fold. Detection remains difficult, especially at night when staff presence is reduced. Automated telesurveillance systems (ATS) may help improve fall detection and prevention.
Objective
To assess the impact of ATS on the prevention of serious nocturnal falls in URCC.
Methods
We conducted a prospective, multicenter, randomized clinical trial including 344 patients in the URCC units of Brive and Limoges. Patients in the intervention group were monitored with ATS, while controls stayed in rooms without ATS.
Results
Patients had a mean age of 83.6 years (SD = 6.1), with 58% women. The cumulative incidence of serious nocturnal falls was 0.01 (SD = 0.02) per patient per stay, with no difference between groups (U = 13,739; p = 0.262). For non-serious nocturnal falls, incidence was 0.03 (SD = 0.07) in the intervention group versus 0.01 (SD = 0.04) in control group (U = 15,391; p = 0.054). Total nocturnal falls were similar (0.03 versus 0.02; U = 14,684; p = 0.529).
Conclusions
ATS allowed detection of more non-serious nocturnal falls, potentially enabling tailored prevention strategies to reduce future falls. Further studies are needed to evaluate the effectiveness of these interventions.
Trial registration
ClinicalTrials.gov NCT01561872 (registered 13/02/2015).
Introduction
The aging of the population is accompanied by an increase in the problems of loss of autonomy, dependence, 1 and the risk of falls. 2 The latter represents a major public health issue due to its frequency and potential severity. 3 In France, one in three adults over the age of 65 and one in two over the age of 80 falls every year.4,5 Falls are the main cause of physical trauma in older adults aged 70 and over. They also have psychological and social consequences on autonomy, quality of life and well-being. 6 The societal cost of falls in France is estimated at 2 billion euros, including 1.5 billion euros for the French health insurance system. 4
The incidence of falls varies according to where the older adult lives. In hospitals, it varies between 1.1 and 9.1/1000 patient days, 7 while in retirement homes, more than half of all residents fall every year. 8 Between 30% and 35% of falls occur in the hospital setting, with 42% occurring during ambulation to the toilet and 7% to 14% during transfers from bed to chair.9,10 However, although falls in hospitals are among the most frequent serious adverse events, they are also preventable. 7
Fall prevention involves managing risk factors. In fact, falls are multifactorial: a history of falls, gait, balance and mobility disorders, visual impairment, fear of falling, muscle weakness, environmental factors and major neurocognitive disorders (mNCD). 11 The latter increases the risk of falls in older adults by a factor of 6. 12
mNCD, predominantly resulting from Alzheimer's disease (AD) and vascular neurocognitive disorders (vNCD), are strongly associated with an elevated risk of falls in older adults, with annual incidence rates estimated between 40% and 60%. In addition to this high frequency, falls in older adults with mNCD are more likely to result in severe injuries, poorer prognoses, reduced likelihood of complete recovery, and increased rates of hospitalization.12,13 This is explained by the gait and balance disorders that are highly increased in mNCD, with a prevalence of 9 to 52% in AD, compared with 71% in vNCD. 12 Furthermore, these older adults are the least likely to call for help when they find themselves on the ground, 14 and 50% of them with a prolonged ground stay of more than an hour die within six months. 15 Hence, there is a need for rapid, specific care for patients with mNCD who are prone to falls.
To this end, specific hospitalization units were created as part of the Alzheimer's plan between 2008 and 2012: dementia specialized care unit (“unités de réadaptation cognitivo-comportementale, URCC”). These units aim to provide rapid, effective care for AD patients with behavioral disorders. 16 These units could help to detect falls and prevent their serious consequences. However, like all hospital wards, in URCC, there are fewer medical staff on duty at night, and nocturnal falls could have serious consequences, such as prolonged standing on the floor. 17 To detect these complications at an early stage, a solution could be to set up an automated telesurveillance system (ATS) with a behavioral algorithm.
However, there is little evidence on the prevention and detection of falls in older adults with mNCD hospitalized in URCC, since most studies focus on preventing falls in older adults at home or in nursing homes. The aim of this first study, conducted as part of the GET BETTER (“Geriatric Environmental Telecare – Behavioral Engineering Technology To Enhance Rehabilitation”) project, was to investigate the impact of an ATS on serious nocturnal falls prevention in URCC.
Methods
Study design
This was a prospective, randomized study in two parallel groups between 2012 and 2014, multicentric (URCC of Brive and URCC of Limoges), unblinded for the health professional and blinded for the patient between entry into the URCC and the discharge decided by the geriatrician of the patient with mNCD. The research sponsor was the clinical gerontology unit of the University Hospital Centre (UHC) in Limoges.
Two groups were compared in the study:
The intervention group was made up of patients who benefited from a camera-type sensor in their room. This ATS was activated at night between 8:00 p.m. and 8:00 a.m., 7 days a week. In the event of fall, the ATS transferred an alert to the healthcare professionals’ central computer and their service phones, sending an image of the alert. The professional then immediately went to the patient's room to verify the alert; helped lift the patient if necessary and implement personalized and adapted curative and preventive measures. The detection of non-serious falls by ATS also encouraged the use of this type of measure to prevent future falls. To better understand the circumstances and mechanism of the fall, the multidisciplinary commission for access to images was called upon. This commission could or could not authorize access to the sequence of images recorded by ATS.
The control group was made up of patients living in rooms where ATS are not activated.
Ethical considerations
GET-BETTER research has received a positive opinion from the “Comité de Protection des Personnes (CPP) du Sud-Ouest et Outre-Mer IV” on 28/07/2011. The promoter and investigators undertook that this research will be carried out in compliance with French law n°2004-806 of August 9, 2004, as well as in accordance with Good Clinical Practice (I.C.H. version 4 of May 1, 1996, and decision of November 24, 2006) and the Declaration of Helsinki (Ethical Principles for Medical Research Involving Human Subjects, Tokyo 2004).
The pre-inclusion visit was carried out by the investigating geriatrician. The pre-inclusion visit took place between 1 day before the inclusion visit and no later than the day of the inclusion visit. Before any research-related examination, the investigator obtained free, informed and written consent from the patient (or his/her legal representative) after a 24-h reflection period. During the pre-inclusion visit, the investigating physician informed the patient and his or her trusted support person or legal representative, who had a reflection time of at least 24 h in which to give consent if necessary and answered any questions they might have had about the objective, the nature of the constraints, the foreseeable risks and the expected benefits of the research. He also explained the patient's rights in the context of biomedical research and verified eligibility criteria. A copy of the information notes and consent form was then given to the patient by the investigating physician. After this information session, the patient had a 24-h reflection period before the inclusion visit.
The investigating physician was responsible for obtaining the patient's written informed consent. The consent form had to be signed before any clinical examination was undertaken for research.
If the patient or his/her trusted support person or legal representative agreed to participate, these persons and the investigator entered their first and last names, dated and signed the consent form. The various copies of the information notes and consent form were then distributed as follows:
- a copy of the information notes and signed consent form is given to the patient. - an original copy is kept by the investigating physician (even if the patient moves during the research) in a locked, secure place inaccessible to third parties. - At the end of the research, a copy of each consent form is sent to the sponsor or its representative, according to procedures communicated to the investigators in good time.
This search was registered on http://clinicaltrials.gov/ under the number NCT 01561872.
Procedure and data collection
This study included two visits: the inclusion visit (V1) and the exit or end-of-study visit (V2). The latter was decided by the URCC's geriatrician-investigator. The same data were collected at both visits, making it possible to map the patient's health at baseline and at the end of the study. Patients could have left the study for a variety of reasons: patient's decision, patient's discharge from the URCC without the investigating physician's agreement, study discharge decided by the investigating physician in the patient's interest, particularly in the event of a serious adverse event, and death. In addition, when the difference between the V1 and V2 was less than 3 days, the patient was considered to have left the study, as there was less variation in medical data over such a short period.
Eligibility criteria
Inclusion criteria
The patients included in the study were over 65 years of age and were admitted to the URCC of Limoges or Brive. They gave informed consent to participate in the study. In addition, consent could be given by the patient's legal representative. Finally, patients benefited from French health insurance.
Exclusion criteria
Patients excluded from the study had not benefited from French health insurance or had critical short-term conditions.
Randomization
Randomization was carried out after verification of the selection criteria. It was stratified by center and was conducted electronically by connecting to the online platform of the Clinical Research and Biostatistics Functional Unit (CRBFU) from the geriatric clinical research unit of the UHC of Limoges.
The list was compiled by the University Hospital Center in the form of blocks of variable size for each center. All actions performed out on this platform and the patient's identity were automatically archived (audit trail procedure). After randomization, the room's ATS was activated for patients in the intervention group, or deactivated for patients in the control group, with conventional follow-up by the nursing staff to prevent falls.
Procedures
Figure 1 showed the patients’ flow chart for the study. From April 3, 2012, to September 29, 2014, 347 patients were pre-included in our study. Three of them were not randomized. Thus, the actual number of patients in the study was 344 (99.13%), 175 (50.87%) in the intervention group and 169 (49.13%) in the control group of the 344 patients were randomized, 6 (1.74%) patients did not benefit from a final evaluation at discharge: 4 (2.30%) in the intervention group and 2 (1.2%) in the control group. Five (1.45%) of these patients did not benefit from a final evaluation because the duration of hospitalization was too short (<3 days): 3 (1.74%) patients in the intervention group and 2 (1.18%) in the control group. One (0.57%) patient in the intervention group died during hospitalization. In the control group, however, no deaths occurred during the study.

Flowchart of the GET BETTER randomized controlled trial.
Data collection
Global geriatric assessment
Patients underwent a global geriatric assessment as performed in routine care on admission to a geriatric ward. The assessment lasted approximately 1.5 h. The overall assessment covered several dimensions. It first included sociodemographic data such as age, gender, previous occupation, level of education, family situation, and legal protection. Functional autonomy was assessed using the Activities of Daily Living (ADL), 18 Instrumental Activities of Daily Living (IADL), 19 “Autonomy, Gerontology, Iso-Ressource Groups (AGGIR)”, 20 and functional autonomy measurement system (SMAF), 21 while cognitive status was assessed using the Mini-Mental State Examination (MMSE), 22 Dubois 5-word test, 23 clock test, and Geriatric Depression Scale (GDS). 24 Nutritional status was analyzed with the Mini Nutritional Assessment (MNA), 25 body mass index (BMI), albumin, and weight loss. Physical abilities were measured according to Fried's criteria 26 and the Short Physical Performance Battery (SPPB). 27 Balance was examined based on history of falls, the unipodal stance test, 28 and the Timed Up and Go test. 29 Behavioral disorders were identified using the Neuropsychiatric Inventory (NPI), 30 and quality of life was assessed using the European Quality of Life 5 Dimensions 3 Level Version (EQ5D3L) questionnaire. 31 The sensory examination included visual, auditory, communication, and skin problems. General medical status was supplemented by a review of medical history, comorbidities, current treatments, and medical follow-up. Finally, an assessment of cardiovascular risks and continence was carried out.
Fall data
A fall was defined as an event that resulted in a patient inadvertently falling to the ground or another surface lower than where he or she had previously been standing. Serious falls in this study were characterized by the following consequences: Fracture, Luxation, voluminous intracranial or peripheral hematoma, facial trauma, skin lesions, subcutaneous hematoma, increased creatine phosphokinase, body temperature ≤35°C or ≥38°C, bedsore, inhalation lung disease, dehydration, post-fall syndrome, malaise or loss of consciousness at the time of the fall, neurological focal sign. Thus, all falls that did not meet these criteria were considered non-serious.
In the intervention group, the fall detected at night by the ATS was analyzed and processed by healthcare professionals. An immediate action plan was then put in place to help the patient. Subsequently, a personalized secondary prevention program was initiated to prevent future falls. All falls in this group were recorded in a database. In the control group, fall screening was carried out solely by healthcare staff. In the event of fall, immediate care was also provided. In addition, a secondary prevention program was implemented, as in the intervention group, and falls are recorded on fall reporting forms. In both groups, all falls were recorded in an end-of-study observation book.
Measures
The primary endpoint was the cumulative incidence of serious nocturnal falls per stay in the URCC. Secondary endpoints included the cumulative incidence of non-serious nocturnal falls and the total number of nocturnal falls. We also analyzed the incidence of falls (serious, non-serious, and total) occurring at other times of the day (morning, afternoon, and evening). Finally, to estimate the overall incidence of falls in both groups, we considered all falls that occurred throughout the day. Since ATS was only active at night, daytime falls were recorded exclusively by paramedical professionals.
Statistical analysis
Size
The number of patients in the study was calculated based on the following hypothesis. At the start of the study, there was no epidemiological data on the frequency of falls among older adults with dementia admitted to the URCC. The study by Nyberg et al. 32 seemed closest to the objective of the GET BETTER research project. Considering the psychogeriatric data from Nyberg's study, it was estimated that older adults with dementia had around 6 times more falls with serious consequences than those without dementia, with a cumulative annual incidence of around 38%. This study was based on a population that most closely resembled that of older adults admitted to URCC. Data from the fall reports showed that one in four demented older adults fell at least once during hospitalization.
Considering a monthly incidence of falls with serious consequences of around 25% in older adults with dementia, and assuming a 50% reduction in the risk of falls (based on the study by Jensen et al., 33 a risk α of 0.05 and a risk β of 20%, the calculated number of patients per group was 168. Given the risk of secondary exclusion, 175 patients were included per group. The number of patients required for the study was therefore 350.
Descriptive analysis
Most quantitative variables were reported as means with standard deviations (SD). Patient length of stay in the URCC, also a quantitative variable, was illustrated using a box plot. Qualitative variables were described as frequencies and percentages. The cumulative incidence of falls per patient stay was determined by dividing the total number of falls recorded by the length of each patient's stay in days.
Comparative analysis
Comparisons between quantitative variables were performed using Student's T-test when normality was confirmed. Otherwise, the Mann-Whitney U test was applied. For qualitative variables, the chi-square or Fisher's exact test was employed to compare observations between the two groups. Statistical analyses were conducted using SigmaStat 3.5 software (SigmaStat, San Jose, CA, USA). The significance level for all analyses was set at 5%.
Results
Characteristics of the population
Table 1 showed the characteristics of the patients in the study. The study population was composed of 344 patients. The average age was 83.58 years (SD = 6.11). Two hundred patients (58%) were women, and 69 (20.06%) had worked as “company employee” during their professional career. One hundred and sixty-seven (48.41%) patients were married at the time of the study, and 157 (45.51%) lived with their spouse. 143 (41.45%) patients had primary school education, and 302 (87.54%) were not under legal protection. In terms of dependency, 109 (31.78%) patients were in the Iso-Resource group (GIR) 4. The mean scores for ADL and IADL were 3.71 (SD =1.44) and 1.15 (SD =1.55), respectively. The patients’ mean SMAF was 43.02 (SD =12.32). In terms of frailty, the mean Fried score was 2.5 (SD =1.04). In terms of physical abilities, the mean score of participants in the SPPB was 4.54 (SD = 3.27). A completion time greater than 20 s on the “timed up-and-go” test was observed in 200 patients (58.1%). Similarly, an inability to maintain one-leg balance for more than 5 s was found in 249 patients (72.38%). Three hundred twenty-one (94.41%) patients had no abdominal problems, 289 (85%) had no musculoskeletal problems, and 204 (60%) had no nutritional problems. In the area of nutrition, the mean MNA score for the population was 20.16 (SD = 3.85), and the mean BMI was 24.53 (SD = 4.11). On cognitive status, 340 (98.8%) patients failed the clock test. The mean score of participants on the MMSE was 12.30 (SD = 5.96). In terms of thymic status, no problems were detected in 227 (66.76%) patients. The mean score on the GDS was 11.53 (SD = 6.12). The mean utility score was 0.57 (SD = 0.33). The patients’ mean global health score was 63.74 (SD = 20.28). For behavioral disorders, patients’ mean NPI was 21.60 (SD = 17.95). In terms of cardiovascular risk, 223 (64.83%) of patients had hypertension, 284 (82.56%) did not have diabetes, 238 (69.19%) did not have dyslipidemia, 325 (94.48%) did not smoke tobacco at the time of the study, 324 (94.19%) were not obese, 328 (95.39%) did not consume alcohol, and 323 (93.89%) did not suffer from any allergies. The cardiovascular examination revealed no problems in 287 (84.41%) patients. Two hundred and fifty-nine (76.40%) patients had no dental problems. The pulmonary examination revealed no problems in 313 (92.33%) patients. The neurological examination revealed problems in 207 (60.88%) patients. Three hundred and five (89.71%) patients had no skin problems, 235 (69.12%) had vision problems, and 202 (54.41%) had no hearing problems.
Functional, cognitive, nutritional, and clinical characteristics of the population.
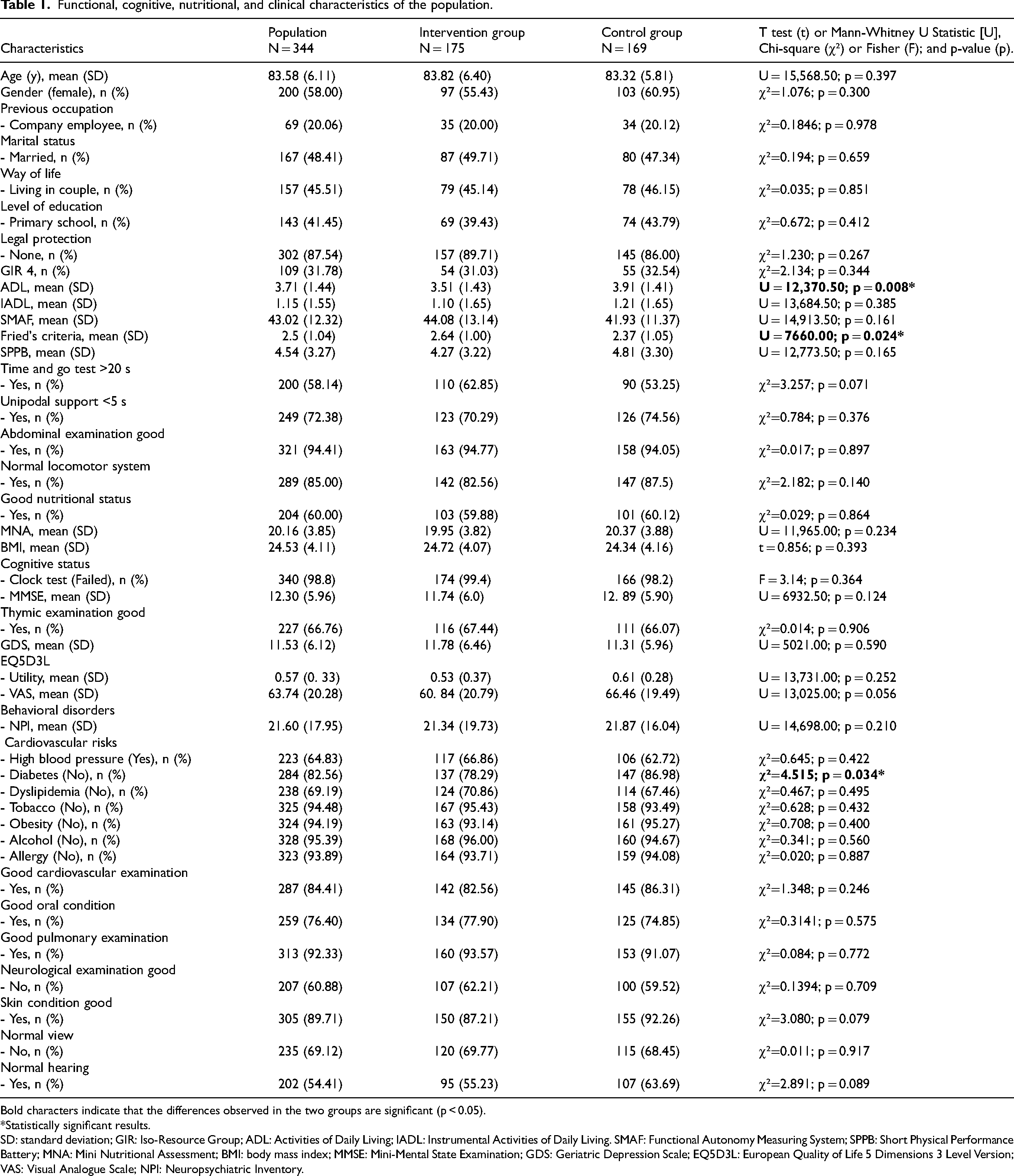
Bold characters indicate that the differences observed in the two groups are significant (p < 0.05).
*Statistically significant results.
SD: standard deviation; GIR: Iso-Resource Group; ADL: Activities of Daily Living; IADL: Instrumental Activities of Daily Living. SMAF: Functional Autonomy Measuring System; SPPB: Short Physical Performance Battery; MNA: Mini Nutritional Assessment; BMI: body mass index; MMSE: Mini-Mental State Examination; GDS: Geriatric Depression Scale; EQ5D3L: European Quality of Life 5 Dimensions 3 Level Version; VAS: Visual Analogue Scale; NPI: Neuropsychiatric Inventory.
Apart from the ADL score (Mann-Whitney U Statistic [U] = 12,370.50; p = 0.008), Fried's criteria (U = 7660.00; p = 0.024) and diabetes (χ² = 4.515; p = 0.034), no significant differences were observed between the two groups.
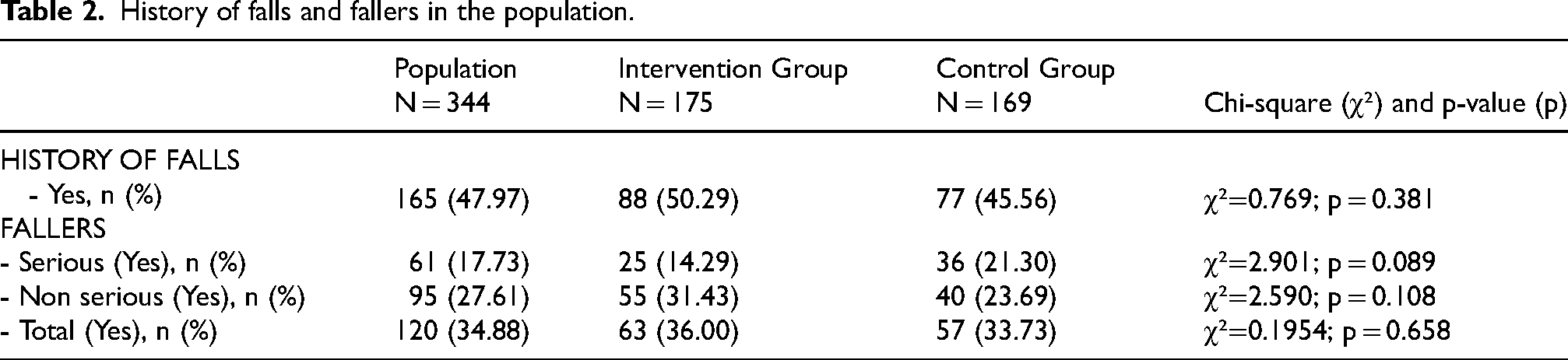
History of falls and fallers in the study
Table 2 showed patients with a history of falls during the 12 months prior to study inclusion, as well as those who had experienced falls during the study. Among the participants, 165 (47.97%) had a history of falls. Sixty-one (17.73%) patients had experienced at least one serious fall, while 95 (27.61%) had experienced at least one non-serious fall. Overall, 120 (34.88%) patients had experienced at least one fall, regardless of severity. No significant differences were observed between the groups (p > 0.05).
History of falls and fallers in the population.
Length of stay in URCC
Figure 2 showed the length of stay of patients in the URCC. The mean length of stay for patients was 22.52 (SD =14.83). In the intervention group, it was 21.77 (SD = 13.39) versus 23.29 (SD = 13.39) in the control group (U = 14, 234.50; p = 0.961). The maximum length of stay was 87 days, and the minimum was 3 days in both groups. The median length of stay was 19 days for the entire population.
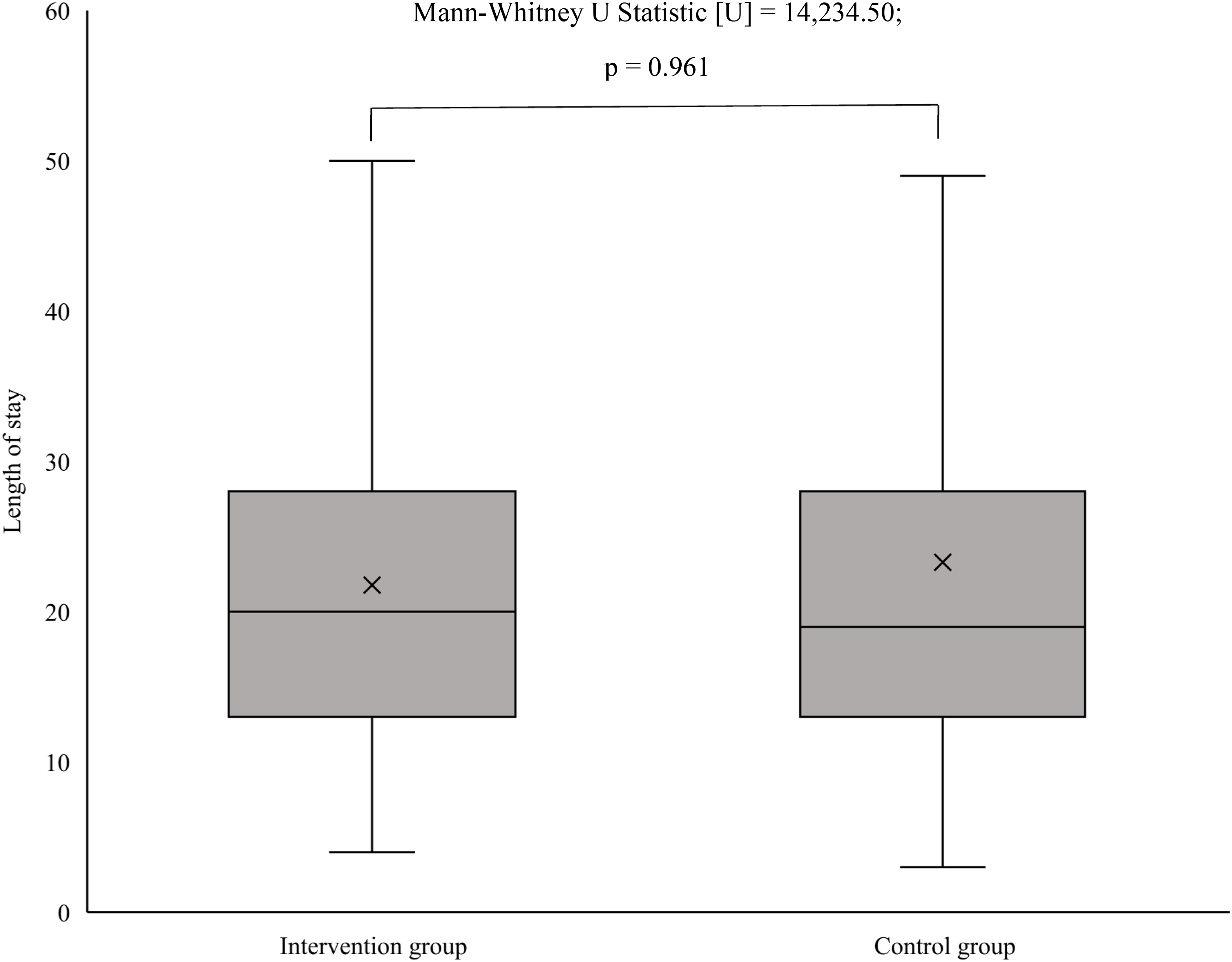
Box plot of patient lengths of stay in two groups.
Incidence of nocturnal falls by length of stay
Table 3 shows the cumulative incidence of nocturnal falls per patient stay in the URCC. The cumulative incidence of serious nocturnal falls was 0.01 (SD = 0.02) per patient per length of stay. In the intervention group, it was 0.01 (SD = 0.02) compared to 0.01 (SD = 0.02) in the control group (U = 13,739.00; p = 0.262). For non-serious nocturnal falls, the cumulative incidence was 0.02 (SD = 0.06). In the intervention group, it was 0.03 (SD = 0.07) and in the control group, 0.01 (SD = 0.04) (U = 15,391.00; p = 0.054). For all nocturnal falls, the cumulative incidence was 0.03 (SD = 0.07). In the intervention group, it was 0.03 (SD = 0.09) contrasted with 0.02 (SD = 0.06) in the control group (U = 14,683.50; p = 0.529).
Cumulative incidence of falls by length of stay.

Bold characters indicate that the differences observed in the two groups are significant (p < 0.05).
*Statistically significant results.
Incidence of falls occurring in the morning, afternoon, and evening by length of stay
The cumulative incidence of serious falls occurring in the morning, afternoon, and evening was 0.01 (SD = 0.03) per patient per length of stay. In the intervention group, it was 0.01 (SD = 0.02) compared to 0.01 (SD = 0.03) in the control group (U = 13,800.00; p = 0.288). For non-serious falls, the cumulative incidence was 0.01 (SD = 0.04). In the intervention group, it was 0.02 (SD = 0.04) and in the control group, 0.01 (SD = 0.03), (U = 15,249.50; p = 0.118). For all falls, the cumulative incidence was 0.02 (SD: 0.05). In the intervention group, it was 0.02 (SD = 0.05) contrasted with 0.02 (SD = 0.04) in the control group (U = 14,702. 00; p = 0.531).
Incidence of falls by time of day and length of stay
The cumulative incidence of serious falls, regardless of when they occurred, was 0.01 (SD = 0.03) per patient per length of stay, 0.01 (SD = 0.03) in the intervention group and 0.02 (SD = 0.04) in the control group (U = 13,196.00; p = 0.074). The incidence of non-serious falls was 0.03 (SD = 0.07). In the intervention group, it was 0.04 (SD = 0.09) and in the control group, 0.02 (SD = 0.05). The difference between the two groups in terms of non-serious falls was significant (U = 15,797.00; p = 0.033). The total incidence of falls was 0.05 (SD = 0.10), 0.06 (SD = 0.12) in the intervention group and 0.04 (SD = 0.08) in the control group (U = 14,879.00; p = 0.434).
Discussion
This study aimed to investigate the impact of an ATS on the incidence of serious nocturnal falls in URCC, considering the length of stay. Behavioral disorders were assessed using the NPI scale. This is a multidimensional scale most often used in current practice to assess behavioral disorders in older adults with AD and related disorders. 30
The study involved 344 patients. The mean age was 83.58 (SD = 6.11). Two hundred (58.00%) patients were women.
The results were similar for both groups in terms of the history of falls (χ² = 0.769; p = 0.381) and percentage of patients who had had at least one serious (χ² = 2.901; p = 0.089) or non-serious fall (χ² = 2.590; p = 0.108). The same was true for falls overall (χ² = 0.1954; p = 0.658).
The cumulative incidence of serious nocturnal falls was 0.01 (SD = 0.02) per patient per length of stay, with identical values observed in both the intervention and control groups, 0.01 (SD = 0.02) (U = 13,739.00; p = 0.262). Regarding non-serious nocturnal falls, the total cumulative incidence was 0.02 (SD = 0.06), with a slightly higher incidence in the intervention group, 0.03 (SD = 0.07) compared to the control group, 0.01 (SD = 0.04), approaching statistical significance (U = 15,391.00; p = 0.054). When considering all nocturnal falls, the cumulative incidence was 0.03 (SD = 0.07), with 0.03 (SD = 0.09) in the intervention group and 0.02 (SD = 0.06) in the control group (U = 14,683.50; p = 0.529). Similar results were found in the literature. Indeed, the study by Barker et al. used several types of intervention, including the camera alert system, and found a similar incidence in both groups (0.96; 0.72 to 1.27; p = 0.766), which was non-significant as in our study. 34 We also found the same results in the study by Visvanathan et al. Their percentage of total falls was higher in the intervention group, with a non-significant difference, and their rate of serious falls was similar in both groups. 35
In addition to the incidence of nocturnal falls, we also assessed the incidence of falls occurring at any time of the day to obtain an overall view of fall distribution in both groups.
The cumulative incidence of serious falls was 0.01 (SD = 0.03) per patient length of stay, 0.01 (SD = 0.03) in the intervention group and 0.02 (SD = 0.04) in the control group (U = 13,196.00; p = 0.074). The incidence of non-serious falls was 0.03 (SD = 0.07). In the intervention group, it was 0.04 (SD = 0.09) and in the control group, 0.02 (SD = 0.05) (U = 15, 797.00; p = 0.033). For the total number of falls, the incidence was 0.05 (SD = 0.10). In the intervention group, it was 0.06 (SD = 0.12). In the control group, it was 0.04 (SD = 0.08). The difference between the two groups was not significant (U = 14,879.00; p = 0.434).
In our study, the incidence of non-serious falls was higher than that of serious falls. This result highlighted the difficulty of detecting non-serious falls without the presence of an ATS on hospital wards, especially at night. This observation was also made by Bayen et al. 36 Indeed, they found that the presence of ATS made it possible to detect more nocturnal falls. Around 50% of non-serious nocturnal falls were not detected in the control group, making it difficult, if not impossible, to manage and implement personalized prevention programs to avoid future serious falls.
This study had both limitations and strengths.
One of the main limitations of this study was undoubtedly the underestimation of the number of non-serious falls in the control group. In fact, as this group did not have ATS, these falls were only detected by healthcare personnel. As a result, some non-serious falls, particularly those occurring at night, went unnoticed because staff had limited access to the rooms. In addition, there was generally a shortage of staff at night. They were also unable to move from room to room to detect adverse events, as this would have risked waking patients. The underestimation of non-serious falls was reinforced by the fact that the study was conducted in institutions where many patients suffered from behavioral disorders. Thus, due to forgetfulness or negligence, some falls were not reported by patients. Moreover, ATS for fall detection in URCC was only active at night, which significantly limited patient monitoring. Indeed, falls can occur at any time of the day, particularly during movements, group activities, or care routines. Restricting ATS to the nighttime period therefore led to under-detection of daytime falls, reducing the reliability of the collected data. Furthermore, this limitation compromised the development of appropriate prevention strategies, as a substantial portion of events went unnoticed. Importantly, the burden of monitoring during the day fell primarily on the paramedical staff, increasing the risk of underreporting or omission of certain falls, particularly minor ones, which are nevertheless important for anticipating future serious falls.
Finally, the population was homogeneous except for ADL, Fried's criterion and diabetes. Adjustments were therefore necessary.
Despite its limitations, this study had several strong points. Chief among these is the fact that it was a randomized controlled trial. It was carried out between 2012 and 2014. At the time, it was the first in the field of falls prevention in older adults with neurocognitive disorders. In addition, a good number of studies had been carried out on this topic. Indeed, many studies had focused on other prevention models, but the use of ATS in falls prevention had not been sufficiently exploited at the time. This was therefore one of the first studies of technologies used to detect and prevent falls in older adults with neurocognitive disorders admitted to URCC. In addition, the study was supported by URCC healthcare staff, patients and their families. Data collection in both groups was carried out systematically, using standardized geriatric assessment questionnaires. These questionnaires were administered face-to-face to patients. To avoid differential errors and minimize inter-rater variability in the surveys, each investigating physician assessed as many patients in the control group as in the intervention group. Finally, the sample size was calculated based on the incidence of falls among hospitalized patients with mNCD.
Conclusions
In this study, the use of an ATS for fall detection in URCC did not significantly reduce the incidence of serious nocturnal falls compared to standard care. However, ATS contributed to a higher detection rate of non-serious nocturnal falls, which are often underreported in the absence of continuous monitoring. These findings highlight the difficulty of identifying nocturnal falls in older adults with mNCD, particularly due to limited nighttime staffing and patients’ behavioral or cognitive impairments. Although ATS was only active at night, its implementation allowed earlier intervention after falls and the initiation of personalized preventive measures. Overall, while ATS did not significantly impact serious nocturnal fall rates, it enhanced the monitoring and documentation of nocturnal falls, providing valuable information to inform prevention strategies and improve patient safety in URCC settings.
Footnotes
Acknowledgements
We would like to thank the heads of the URCCs at the Jean Robeyrol hospitals in Limoges and Brive, the healthcare staff, the patients and their families and/or friends.
Ethical considerations
With regard to ethical considerations concerning patients, GET-BETTER research received a favorable opinion from the protection committee in the South-West and Overseas IV on 28/07/2011. The promoter and investigators have undertaken that this research will be carried out in compliance with French law n°2004-806 of August 9, 2004, as well as in accordance with Good Clinical Practice (I.C.H. version 4 of May 1, 1996 and decision of November 24, 2006) and the Declaration of Helsinki (Ethical Principles for Medical Research Involving Human Subjects, Tokyo 2004). This research was registered at ![]() on 13/02/2015 under the number NCT 01561872.
on 13/02/2015 under the number NCT 01561872.
Consent to participate
Patients or their representatives (trustworthy person, guardian or curator) signed a consent form authorizing the adults mandated by the research promoter to have access to the information in the strictest respect of confidentiality.
Consent for publication
Not applicable.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets analyzed during the current study and the study protocol are available from the corresponding author on reasonable request.