
Abstract
Subjective cognitive decline (SCD) is an early risk marker for dementia. This study examined the 3-year incidence and predictors of SCD using the Medical Outcomes Study Cognitive Functioning Scale-Revised in a national sample of 1858 U.S. military veterans aged ≥60. Clinically significant SCD occurred in 5.4% of veterans, with an average decline of 1.73 standard deviations. Lower perceived resilience—specifically lower endorsement of “I bounce back after hardship” (35.1% relative variance explained) and “Coping with stress can make me stronger” (33.8%)—chronic pain (18.7%) and sleep difficulties (12.4%) emerged as the strongest predictors of SCD. Interventions targeting these risk factors may help mitigate SCD in veterans.
Introduction
Subjective cognitive decline (SCD) refers to self-reported concerns of worsening cognitive abilities, such as memory, attention, and concentration, from previously normal cognitive function, marked by worry about those self-reported changes. 1 Previous studies of SCD used similar terminology (e.g., subjective cognitive complaints, subjective cognitive impairment, subjective cognitive concerns) to describe the same phenomenon. 2 Meta-analyses have shown that SCD is associated with increased risk of developing mild cognitive impairment (MCI) and dementia,3–5 and may serve as a symptomatic indicator of preclinical Alzheimer's disease (AD).6,7 Individuals with SCD and AD biomarkers exhibit a higher prevalence of preclinical AD5,6; as well as a greater risk for objective cognitive decline and progression to Alzheimer's disease and related dementias (ADRD).5–7
Military veterans experience disproportionately higher rates of SCD than non-veterans.8,9 Several modifiable risk factors, such as lower educational attainment, cardiometabolic and chronic health conditions, mental health status, and unemployment, have been linked to elevated SCD risk.10,11 Psychological resilience, 12 defined as the ability to “bounce back” after traumatic events and other challenges, 13 sleep disorders, 14 and chronic pain 15 have also emerged as important risk factors for MCI and ADRD. One study found that high SCD levels were associated with greater amyloid and tau burden and worse cognitive performance among veterans without posttraumatic stress disorder (PTSD). 16 Given the high healthcare utilization and cognitive burden among veterans, understanding modifiable risk factors for SCD is essential for prevention and intervention planning in this population.17,18
Previous studies of SCD among veterans have almost all been cross-sectional, with limited sociodemographic, lifestyle, health, and psychosocial factors, which we included as potential predictors in the analyses. The present study is one of few that examine SCD longitudinally. We analyzed data from a contemporary, nationally representative sample of older U.S. military veterans to: (1) estimate the incidence of SCD over a three-year follow-up period, and (2) identify sociodemographic, military, health, and psychosocial predictors of incident SCD.
Methods
Participants
The National Health and Resilience in Veterans Study (NHRVS) is an ongoing longitudinal nationally representative survey of U.S. veterans, with a total sample of 4069. The current study focuses on a sub-cohort of veterans aged 60 years or older (N = 1858) who completed a baseline and 3-year follow-up assessment. To ensure the results are representative of the entire U.S. veteran population, post-stratification weights were applied using baseline data from the U.S. Census Bureau Current Population Survey Veterans Supplement. Additional information about the NHVRS is provided in Supplemental Methods 1.
Measures
Subjective cognitive decline
At baseline and follow-up, participants completed the Medical Outcomes Study Cognitive Functioning Scale-Revised (MOS-COG-R),19,20 a self-report measure that assesses subjective cognitive difficulties across six domains: reasoning, concentration and thinking, confusion, memory, attention and reaction time. Scores range from 1 to 6 for each of the items, with higher scores reflecting better cognitive function. Scores are standardized using T-score transformation procedures, yielding a mean of 50 and a standard deviation of 10 to facilitate comparison with population norms. The psychometric properties of the MOS-COG-R have been reported with good reliability and validity. 20 SCD was operationalized as a decline in the MOS-COG-R score of at least 1 standard deviation from baseline to 3 years, consistent with previous studies.21–23
Potential correlates of subjective cognitive decline
Sociodemographic, military, physical health, mental health, and psychosocial variables were examined as potential correlates of subjective cognitive decline. Supplemental Table 1 provides details of all measures and specific scales used in the study. All potential correlates were measured at baseline. Physical health, mental health, and psychosocial variables were assessed using self-report measures.
Data analysis
Item-level missing data (<5%) were imputed using chained equations. Data analyses proceeded in four steps, as described below.
First, to compare sample characteristics and MOS-COG-R scores by SCD status at 3-year follow-up (−1 SD or lower versus > −1 SD), we used independent-samples t-tests and chi-squares.
Second, to identify independent correlates of SCD at 3-year follow-up, we entered variables associated with SCD at the p < 0.20 level in bivariate analyses were entered into a multivariable binary logistic regression model. 24 Third, planned post-hoc analyses at the p < 0.20 level were conducted to examine individual component measures (e.g., Connor–Davidson Resilience Scale, Insomnia Severity Index, count of number of medical conditions; see Supplemental Table 1) that drove associations with SCD. All regression models included baseline MOS-COG-R scores.
Fourth, statistically significant predictors from the multivariable analysis were entered into a relative importance analysis, 25 which partitions the model's explained variance among predictors while accounting for intercorrelations, thereby estimating each predictor's unique and shared contribution to the outcome. 25
All analyses were performed in SPSS Statistics v30.
Results
Incidence of SCD
Among the 1858 veterans, 88 (weighted 5.4%) showed a decline of one standard deviation or more in MOS-COG-R scores at the 3-year follow-up. At baseline, MOS-COG-R scores did not differ between those who developed SCD versus those who did not (M = 93.1, SD = 10.9 versus M = 93.5, SD = 9.4; t = 0.32, p = 0.75). Over the 3-year period, veterans with SCD at the 3-year follow-up showed a marked decline in MOS-COG-R scores, with an average decrease of 1.73 standard deviations (95% CI: −1.91 to −1.54; decliners: M = 64.0, SD = 18.7 versus non-decliners: M = 93.5, SD = 9.9).
Baseline predictors of SCD
Table 1 shows results of bivariate and multivariable analyses of sociodemographic, military, health, and psychosocial correlates of SCD over the 3-year study period. Bivariate analyses showed that veterans who experienced SCD at 3-year follow-up reported higher baseline levels of insomnia and loneliness, as well as greater symptoms of PTSD and generalized anxiety disorder symptoms. These veterans also reported lower baseline levels of resilience, purpose in life, optimism, and grit, compared to those without SCD.
Sample characteristics by subjective cognitive decline status among older U.S. veterans.

Statistically significant association: *p < 0.05; **p < 0.001.
Multivariable model includes all variables associated with SCD at the p < 0.20 level in bivariate analyses: year of military service, number of medical conditions, and scores on measures of insomnia severity, PTSD symptoms, MDD symptoms, GAD symptoms, resilience, purpose in life, dispositional optimism, grit, and loneliness.
When variables associated with SCD at p < 0.20 in bivariate analyses were entered into a multivariable logistic regression model, a greater number of baseline medical conditions, higher insomnia severity, and lower resilience scores were independently associated with SCD at the 3-year follow-up.
Planned post hoc analyses revealed that a self-reported diagnosis of chronic pain (from number of medical conditions (see Supplemental Table 1); OR = 1.74, 95% CI: 1.09–2.80), scores on the difficulty falling asleep item of the insomnia severity index (OR = 1.29, 95% CI: 1.03–1.61), and two Connor–Davidson Resilience Scale items: “I tend to bounce back after illness, injury, or other hardships” (OR = 0.62, 95% CI: 0.46–0.83) and “Having to cope with stress can make me stronger” (OR = 0.70, 95% CI: 0.55–0.90) were significantly associated with SCD. Figure 1 shows the association of these two statistically significant resilience items and probability of SCD over the study period (dashed horizontal black lines represent the mean probability of 1SD SCD in the full sample). Relative importance analysis revealed that these two resilience items accounted for the majority of explained variance in SCD: 35.1% and 33.8%, respectively. Chronic pain (18.7%) and difficulty falling asleep (12.4%) accounted for the remaining variance.
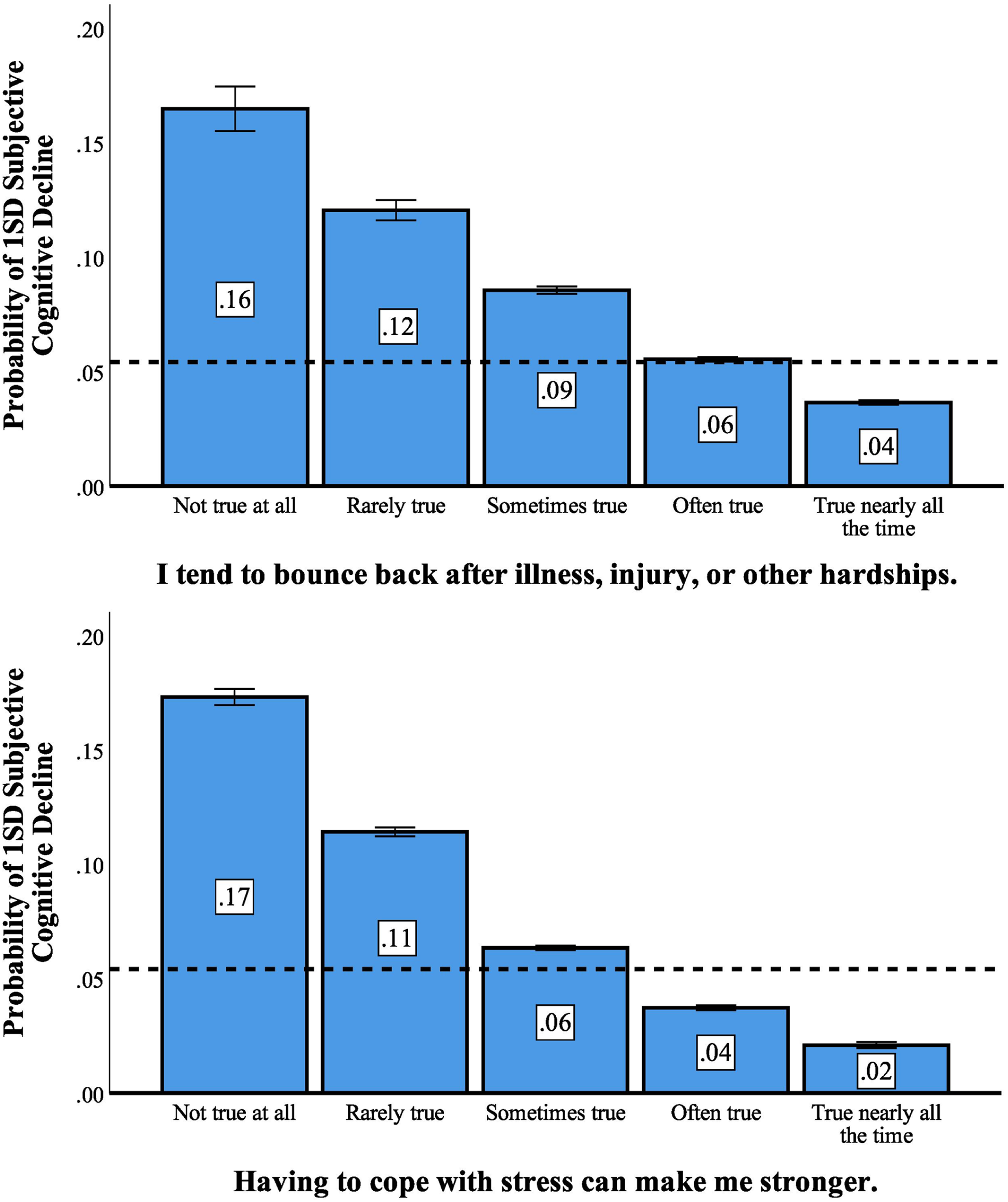
Association of perceived resilience items and subjective cognitive decline.
Discussion
This study examined the incidence and predictors of SCD over a 3-year period in a nationally representative sample of older U.S. military veterans. Results showed that lower levels of two indicators of psychological resilience—“I tend to bounce back after hardship” and “coping with stress can make me stronger”—accounted for nearly 69% of the explained variance in SCD, with chronic pain and sleep disturbances accounting for the remainder. These findings are consistent with prior research linking resilience, chronic pain, and sleep difficulties to increased risk of cognitive decline.12,14,15
Previous studies have also investigated mechanistic pathways with each of our significant predictors of SCD. Chronic pain may indirectly increase SCD risk through neuroinflammation, 26 attentional fatigue,27–29 and mood disturbances.30,31 Sleep difficulties could contribute to SCD through neurophysiologic (glymphatic dysfunction),32,33 cognitive,34,35 and emotional pathways.36,37 Finally, resilience may buffer or moderate the relationship between chronic stress-related conditions (chronic pain38,39 and sleep problems40,41) and SCD.
Our findings underscore the importance of interventions aimed at assessing, monitoring, and enhancing resilience as well as managing chronic pain and sleep difficulties among veterans at risk for SCD. Previous research has indicated that interventions for MCI and AD are also effective for those with SCD. 42 Several systematic reviews and meta-analyses have demonstrated that cognitive behavioral therapy (CBT) combined with mindfulness techniques and digital resilience interventions can improve resilience, reduce psychological distress, and enhance overall mental health.43,44 CBT has also proven effective for treating insomnia in individuals with chronic musculoskeletal pain, 45 while personalized multimodal lifestyle programs—incorporating physical activity, sleep training, stress management, nutrition, and weight management—have shown benefit for chronic pain. 46
The current study has several notable strengths, including the nationally representative sample of U.S. military veterans with a 3-year follow-up period; examination of a range of potential predictors of SCD; and use of multiple analytic strategies (e.g., multivariable and relative importance analyses) to identify robust baseline predictors of SCD. Nevertheless, several limitations should be acknowledged. First, the study relied on self-report measures, which may introduce reporting bias, and objective cognitive performance was not assessed. Second, the observational design precludes causal inference. Third, loss to follow-up may have introduced selection bias. Fourth, although the sample reflects the broader demographic profile of the U.S. veteran population (older, predominantly White, and male), findings may not generalize to more diverse or higher-risk veteran subgroups.
Conclusions
Results of this nationally representative study of older U.S. veterans highlight the importance of screening for and addressing perceived resilience, chronic pain, and sleep problems in older U.S. military veterans at risk for cognitive decline. Future research should incorporate objective cognitive measures to complement self-report data and provide a more comprehensive understanding of cognitive decline. Studies should also aim to replicate these findings in more demographically diverse veteran populations, including greater representation of women and racial/ethnic minority groups. Finally, longitudinal intervention studies are needed to evaluate the effectiveness of resilience-enhancing, pain management, and sleep-focused interventions in preventing or delaying cognitive decline and progression to more severe cognitive impairment in veterans and other populations at risk for dementia.
Supplemental Material
sj-docx-1-alr-10.1177_25424823251407258 - Supplemental material for Subjective cognitive decline among older U.S. military veterans: A 3-year, nationally representative, longitudinal study
Supplemental material, sj-docx-1-alr-10.1177_25424823251407258 for Subjective cognitive decline among older U.S. military veterans: A 3-year, nationally representative, longitudinal study by Michael F Georgescu, Ian C Fischer, May A Beydoun, Viola Vaccarino and Robert H Pietrzak in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
The authors express their gratitude to the Ipsos staff who organized data collection and the veterans who took part in the National Health and Resilience in Veterans Study. This research was supported in part by the Intramural Research Program of the National Institutes of Health (NIH). The contributions of the NIH authors were made as part of their official duties as NIH federal employees, are in compliance with agency policy requirements, and are considered Works of the United States Government. However, the findings and conclusions presented in this paper are those of the author's and do not necessarily reflect the views of the NIH, U.S. Department of Health and Human Services, or the U.S Department of Veteran Affairs.
Ethical considerations
The Human Subjects Committee of the VA Connecticut Healthcare System approved the study methods.
Consent to participate
For inclusion, electronic informed consent was obtained by all participants.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data is not available to the public due to privacy and ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.