
Abstract
Background
Identification of Alzheimer's disease (AD) needs inexpensive, noninvasive novel biomarkers. autoimmunity plays a key role in the pathogenesis of AD.
Objective
This study aims to screen innovative diagnostic biomarkers for AD from the perspective of autoantibodies.
Methods
The study consisted of two screening phases and two validation phases. AD serum autoantibody-related biomarkers were discovered and validated using serum samples from four independent cohorts encompassing 241 participants, i.e., AD patients, healthy controls, and other dementia-related diseases. First, to identify biomarkers for AD, a phage displayed random peptide library (Ph.D.12) was applied to screen specific autoantibodies in a total of 71 serum samples from 39 AD patients and 32 healthy controls. After further screening by polypeptide microarray, Then, for validation, three peptides were analyzed in another two independent cohorts, which included AD patients, healthy controls, and other dementia-related diseases, Enzyme-linked immunosorbent assay (ELISA) was finally used to evaluate their sensitivity and specificity for AD diagnosis.
Results
Our results show that both AD2024Val03, AD2024Val70, and AD2024Val72 showed a statistically significant ability to discriminate AD patients from controls and other dementia-related diseases. Additionally, combination of these three peptides, AD2024Val, could greatly improve the diagnostic performance (AUC is above 0.95, sensitivity ∼100%, specificity ∼79%).
Conclusions
the peptides we identified could serve as promising blood biomarkers for AD clinical diagnosis, which also might provide new insights into the potential pathogenesis of AD.
Introduction
Alzheimer's disease (AD) is the most common dementia, which is a neurodegenerative disease characterized by memory impairment and cognitive dysfunction. 1 AD is a progressive and devastating disease, which poses a serious threat to the health of the older with an increasing prevalence as the population ages.1,2 The primary pathological features of AD consist of extracellular amyloid-β (Aβ) plaques, intracellular neurofibrillary tangles, and chronic neuroinflammation.3–5 Previous research found that neuropathological changes may precede clinical dementia by a decade or more. 6 Therefore, early identification of AD is critical for prevention and treatment.
Currently, AD diagnosis relies on a comprehensive approach incorporating symptom assessment, clinical examination, neuroimaging, cognitive testing, and biomarker analysis. 7 Positron emission tomography (PET) imaging and cerebrospinal fluid (CSF) analysis of Aβ42 and T-tau are widely recommended for AD diagnosis in clinical and research settings. 8 However, the high cost of PET limits its wide application in the clinic. Postmortem studies have demonstrated an association between CSF Aβ42 levels and pathological alterations. 9 However, lumbar puncture is an invasive examination and cannot be performed well in AD patients with psycho-behavioral abnormalities, which means that clinical implementation is also difficult. Recently, Zetterberg et al. found that plasma levels of pTau181 and Aβ42/40 could be considered an alternative ATN biomarker for AD diagnosis. 10 Nevertheless, plasma levels of pTau181 and Aβ are so low that only could be measured by ultrasensitive single molecule array (Somia), which was considered unacceptable in many communities. Overall, there is an urgent need for an innovative, noninvasive biomarker which could assist in diagnosis and treatment for AD.
AT(N) framework, reflecting presence and degree of Aβ deposition (A), pathologic tau (T), and neuronal injury (N), aims to distinguish AD pathology from the resulting clinical syndrome for a more sensitive and specific case identification. 11 In addition, neuroinflammation is an early event during the process of AD pathologic changes. 12 Lately, mounting scientific evidence suggested that autoimmune mechanisms contribute significantly to AD development and autoantibodies can serve as a reflection of brain injury.13–16 Fetissov et al. found that galanin autoantibodies were increased and were associated with clinical characteristics of AD patients. 17 In addition, in 5XFAD mouse models, Bieberich et al. observed an age-dependent rise in ceramide-targeting antibodies, finding that both these antibodies and exosome levels accelerate amyloid plaque development. 18 Taken together, the above shows that autoantibodies in body fluid could be used as biomarkers for AD. Excitingly, Shen et al. identified seven potential AD-specific autoantibodies that could differentiate AD from other neurodegenerative disorders and were more predictive of cognitive decline than CSF amyloid or tau levels. 13 But one limitation of their research is that the potential AD-associated autoantigens were chosen based on prior research findings. In fact, for many diseases, including AD, the antigens responsible for initiating the immune response remain unknown. Therefore, no definitive antigenic target has been established. 19 Although Kandiah Professor’ research team screened out six autoantibodies, using a functional protein microarray containing >1600 potential human autoantigens, which could serve as diagnostic biomarkers for AD. 20 However, recent studies suggested that immune-triggering components may extend beyond proteins. 21 Notably, phage random display peptide library boasts a diversity of 109, surpassing traditional proteome-specific libraries by 104∼105 fold, enabling comprehensive coverage of binding space regardless of the original antigen. Additionally, well-characterized phage display libraries can be obtained commercially. In recent years, Phage random display peptide library has become a new strategy in the research field of autoantibody biomarkers.
In this study, we combinate M13 phage display library of random peptides 22 and next generation sequencing to discover peptides which could be specifically identified by IgG in the sera of AD patients. After screening phase I, and screening phase II performed by peptide microarray, the peptide candidates were selected for further validation in another independent cohorts. Finally, our study successfully discovered novel serum biomarkers with high sensitivity and specificity for AD clinical diagnosis.
Methods
Study population and serum sample collection
The study consisted of two screening phases and two validation phases. 107 AD patients, 101 matched healthy controls, 14 Parkinson's disease (PD) patients, 10 cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL) patients and 9 acute cerebral infarction (ACI) patients were included in this study. Inclusion criteria: all enrolled AD patients met the current NINCDS-ADRDA diagnostic criteria. 7 Normal subjects were demographically matched (age, sex, race) to the AD cohort. PD, CADASIL, and ACI patients were diagnosed based on their respective criteria.23–25 The exclusion criteria were consistent with our previous study. 26 Blood samples were obtained from patients who meet the screening criteria. Written informed consent was acquired from all participants or legal guardians, and the research protocol received ethical approval from the Institutional Review Board of Zhengzhou University People's Hospital (No. HNEECKY-2020-76). All the sera samples were collected into vacutainer tubes from all subjects in the morning after a 12-h fast. The sera were extracted by standard procedures and frozen at −80°C.
Phage immunoprecipitation
The library of phage displayed random peptides (Ph.D.12) was stored at −80°C. The IgG concentration of serum samples was measured by the Human IgG ELISA kits (eBioscience, MA, USA). For all samples, the final amount of IgG added to 100 μL immunoprecipitation mix was 0.5 μg. We set three replications on 96-well plate. Besides, we also added anti-6×His antibody and phosphate-buffered saline (PBS) buffer as positive and negative control, respectively. The immunoprecipitation mixture was supplemented with approximately 1 × 109 M13 phage particles. The plate was carefully sealed and then rotated 14 h at 4°C. 10 μL/well of protein G Dynabeads (Invitrogen, MA, USA) was finally added. The sealed plate underwent 6-h rotation at 4°C, followed by five successive bead washes using 200 μL wash buffer. Finally, the beads were resuspended in 30 μL ddH2O and then heated at 95°C for 10 min.
Library preparation for next generation sequencing
The library for next generation sequencing was prepared through two consecutive PCR amplifications of phage DNA. The primer set for the first PCR amplification consisted of S5XX-23R and N7XX-18 (Supplemental Table 1). The “XXXXXXXX” represents an 8-nucleotide barcode sequence employed for sample multiplexing. Secondary PCR amplification was performed using primers S710 and N910 (Supplemental Table 1). The primary PCR was performed in a 50 μL reaction volume using phage DNA as template. PCR products were then gel purified individually. A 25 μL amplification volume was used for the second round PCR, with purified first-round PCR product as template. The system and procedure of the first and second rounds of PCR are as described previously. 21 After gel purification and the concentration measurement. The library pool was sequenced using a 2 × 150 paired-end approach (Illumina HiSeq platform).
Bioinformatics analysis
With an insert size of 103 bp, this library was entirely covered by the paired sequencing reads. The insert sequence consisted of an 8-bp N barcode, an 8-bp S barcode, and a 36-bp variable DNA region. Paired N and S barcodes uniquely tagged the serum sample for each insert. The 36-bp region, representing the phage peptide sequence, was converted to a 12-residue peptide and assigned to the matching serum sample using the barcode pair. Subsequently, peptide counts were tallied and ranked within each serum sample. Each sample has three replications to obtain the average count. Finally, peptide counts were normalized to the total count per serum sample, then subjected to unpaired Student's t-test analysis between AD and healthy cohorts for every peptide. Following statistical adjustment (Bonferroni p < 0.05), 69 AD-enriched peptides were advanced to the next stage of analysis.
To identify the most discriminative peptides between AD and healthy controls, the 69 candidates were analyzed using a caret-based multilayer perceptron model, with classification performance visualized via receiver-operating-characteristic (ROC) curves (generated by ROCR).
Peptide microarray fabrication
The C-terminal amidated peptides screened from screening phase I were synthesized. Following the manufacturer's protocol, all peptides were independently conjugated to bovine serum albumin (BSA) using Sulfo-SMCC 27 In brief, BSA was first activated with Sulfo-SMCC at a 1:30 molar ratio and dialyzed in (1x) PBS buffer. Cysteine-containing peptides were then added (1:1 w/w), incubated for 4 h at RT, and dialyzed again to eliminate unbound peptides. Several conjugates were randomly selected and analyzed via SDS-PAGE. The peptide-BSA conjugates and controls (BSA and human IgG) were arrayed in triplicate on PATH substrate slides using a non-contact Super Marathon printer, creating identical 2 × 7 subarrays. Processed slides were incubated overnight at 4°C, then stored at −80°C.
Microarray-based serum analysis
To create discrete subarray compartments, a 14-well rubber gasket was attached to every slide. The microarray was employed for serum profiling based on an established method, with minor adjustments. 28 Briefly, the microarrays stored at −80°C and incubated with blocking buffer for 2 h after gradient rewarming. Subsequently, 200 μL serum was diluted into 1:50 with 1%BSA-PBST and incubated with the subarray overnight at 4°C. The arrays were then incubated with Cy3-conjugated goat anti-human IgG at RT for 1 h and scanned by luxscan 10k-A with 95% laser power/PMT480. Fluorescence intensity data were acquired using GenePix Pro 6.0 software. Finally, the average signal intensity was calculated from triplicate spots for each peptide. Normalization was applied to microarray slides for all serum samples. The area under the curve (AUC) values were calculated by GraphPad Prism 8.0.
ELISA validation of the identified peptides
The C-terminal amidated peptides screened from screening phase II were synthesized by GL Biochem. The ELISA was used for validation as described previously with a few modifications. 21 In brief, high-binding 96-well ELISA plates were coated overnight at 4°C with 100 μL of BSA-conjugated peptide (50 μg/ml), followed by 2-h blocking at RT. 100 μL of the diluted serum was added into the wells and then incubated at 37°C for 2 h. Following eight PBST washes, plates were incubated with HRP-conjugated anti-human IgG at 37°C for 1.5 h. Each well of the plates was added with 100 μL tetramethylbenzidine and incubated at 37°C for 0.5 h. Finally, the reaction above was stopped with 2 M H2SO4. Optical density was measured by Behring EL311 ELISA microplate reader at 450 nm. Standard curve fitting for ELISA data employed a three-parameter logistic nonlinear regression approach.
Statistical analysis
All statistical analysis was conducted with SPSS 23.0 and GraphPad Prism 8.0. Calculations were performed independently for both the screening and validation phases. For categorical data, intergroup differences were analyzed using χ2 test. For numerical data, the Mann-Whitney U test was employed to compare the mean values of un-transformed ELISA binding data. Multiple group comparisons were performed using the Kruskal–Wallis test, followed by Dunn's post hoc analysis. The significant difference was set at p < 0.05.
Results
Study design for the discovery of AD-specific peptides
This study consisted of four phases: two screening phases and two validation phases (Figure 1). The demographic characteristics of patients and healthy subjects are shown in Table 1. In the screening phase I, phage-displayed peptide libraries coupled with next generation sequencing were employed to identify peptides specifically recognized by serum IgG from AD patients (Figure 1A). In brief, screening was performed to recognize peptides which specifically bind to antibodies in dividual serum sample. The enrichment of IgG-binding peptides/phages was achieved with Protein G beads. The enriched peptides/phages from each serum sample were subsequently sequenced using a barcoded library. The quality control of this experimental approach was done as described previously. 21 In the screening phase II, we made peptide microarray to further screen for peptides with stronger IgG binding strength in the serum of AD patients (Figure 1A). Briefly, the C-terminal amidated peptides screened from screening phase I were synthesized and printed on PATH substrate slides. Then, the subarray of peptide microarray was incubated with the AD serum which came from another sample cohort to select the peptides for further validation.

Schematic diagram and workflow. A. The schematic for phage display screening, next generation sequencing, peptide microarray and ELISA validation. B. This study is composed of four major phases, i.e., screening phase I, screening phase II, validation phase I, and validation phase II.
Characteristics of all participants in this study.
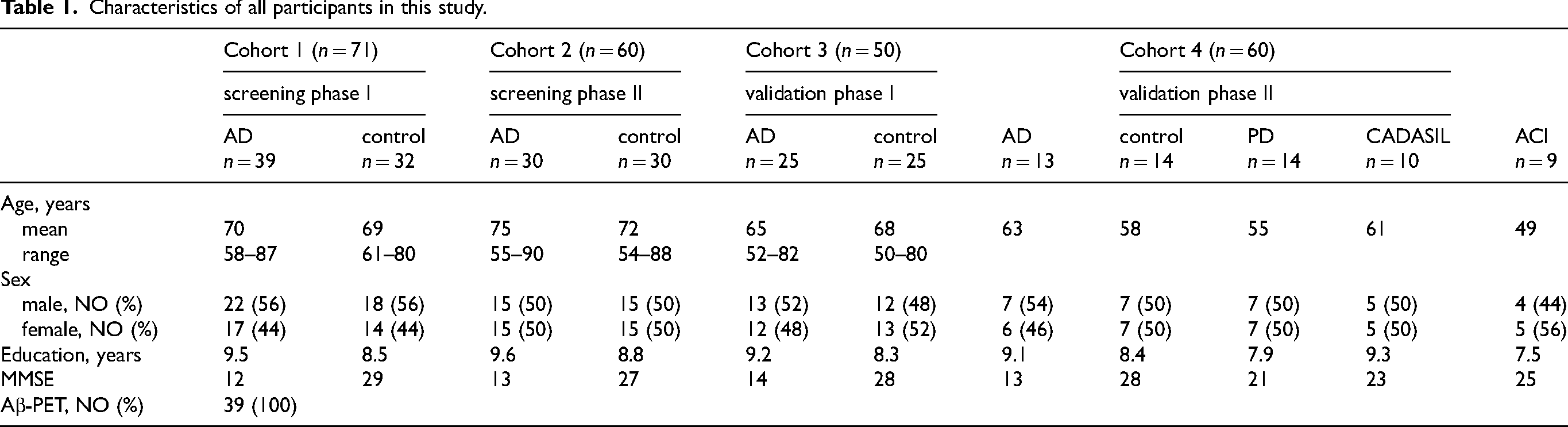
Following the two rounds of screening, serum samples from another cohort were then evaluated. Antibody-bound peptides from both AD patients and healthy individuals were examined. Subsequently, we identified peptides exhibiting significant differential binding between AD patients and healthy controls. A total of 107 AD patients and 101 healthy volunteers provided serum samples for all experimental stages, including screening and validation phases (Figure 1B, Table 1). In Validation II, in order to evaluate the diagnostic specificity of the identified serum autoantibody biomarker for AD diagnosis, we examined sera from 33 patients with other dementia disorders (PD, CADASIL, ACI) alongside the AD cohort (Table 1).
Identification of serum autoantibody binding peptides in the screening phase I
In the screening phase I, to identify the serum autoantibody binding peptides, we analyzed serum samples from 39 AD and 32 healthy individuals. No significant differences in age or gender distribution were observed between the AD patient cohort and health control group (Table 1). Screening was performed using 100× coverage of the phage peptide library to detect autoantibody-specific peptide interactions in each serum sample. Subsequently, next-generation sequencing was employed to identify the enriched phage/peptides. Potential biomarkers were defined as peptides with a p-value <0.05 and ratio (AD/Health) above 1.2. We detected 69 peptides showing high binding affinity to serum antibodies in AD patients (Figure 2A, Supplemental Table 2). Bioinformatic analysis revealed that some of the 69 candidate peptides exhibited statistically significant discriminatory power between AD and control groups (p < 0.002) (Figure 2B). We next calculated receiver-operating-characteristic (ROC) curves for all the 69 peptides. The results revealed that AUC values ranging from 0.53 to 0.76. The AUC for three peptides was above 0.7, 65.2% (45/69) were above 0.6 (Figure 2C, Supplemental Table 3).
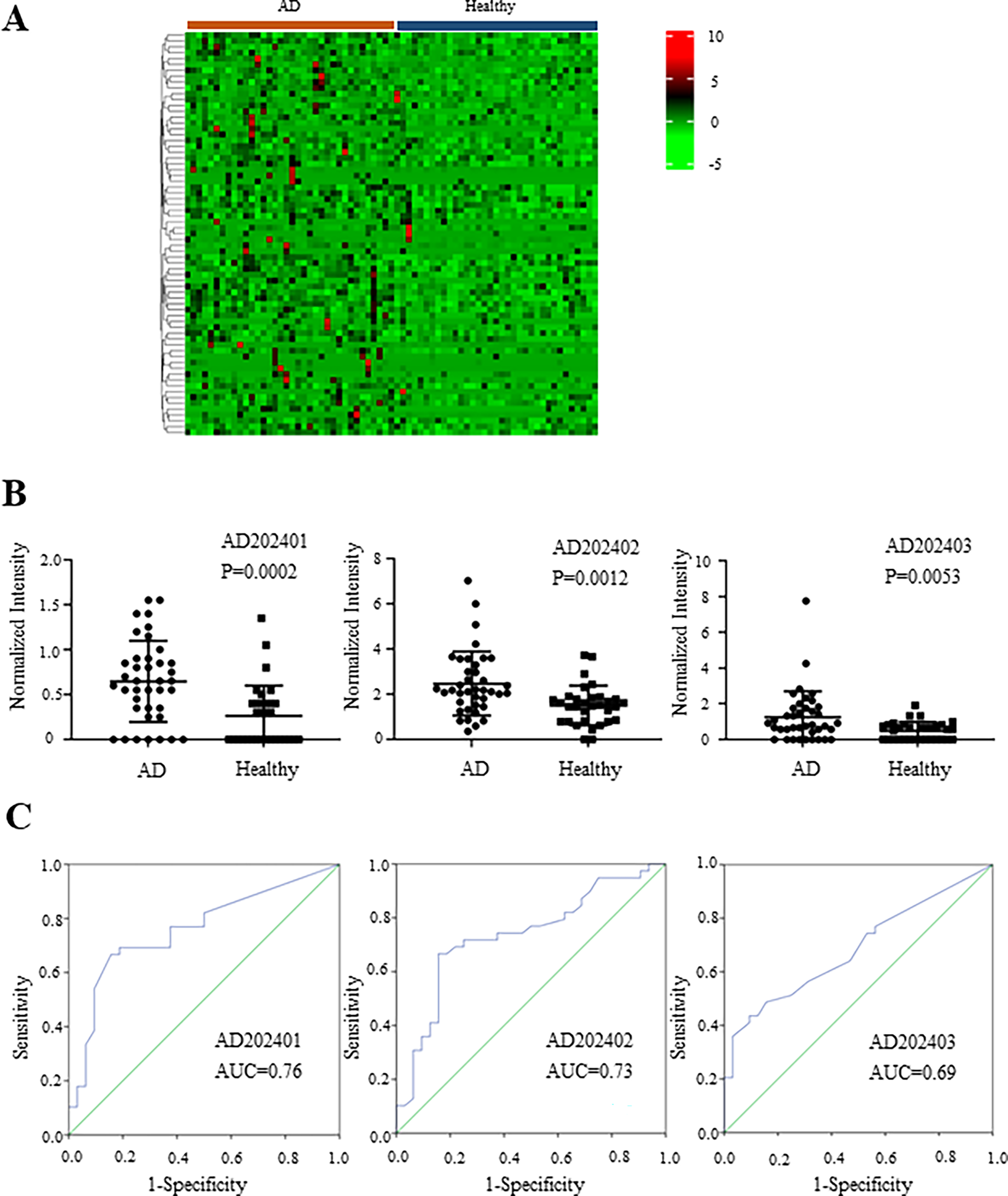
The candidate peptide biomarkers were discovered in the screening phase I. A. The peptides which could differentiate AD patients from healthy controls were discovered using next generation sequencing. B. Reactivity of the candidate peptides with AD patients and healthy controls. C. ROC curve analysis of the candidate peptides between AD patients and healthy controls.
Identification of the peptide candidates in the screening phase II
Subsequently, to evaluate the diagnostic utility of these peptides for AD, complete validation would be optimal. However, to minimize costs and preserve samples, we introduced a secondary screening phase before proceeding to validation. We selected the top 15 peptides with a higher differentiation capability (AUC values) and AD202470-AD202477, filtered by another algorithm, for screening phase II (Supplemental Table 4). In addition, in order to further improve efficiency, given the wide application of polypeptide microarrays, we plan to apply this technology in this screening phase. During the screening phase II, 30 AD patients and 30 healthy controls participated, and age and sex distributions were balanced across groups (Table 1). Based on the results of the peptides microarray (Supplemental Table 5), we selected the top 3 peptides for the next validation phase (AD202403, AD202470 and AD202472) (Figure 3A, B).

Three candidates of AD serum biomarkers were selected in the screening phase II. A. Reactivity of the serum biomarkers with sera of AD patients and healthy controls in the screening phase II. B. Receiver operating characteristic curve analysis of the four candidate peptides with AD patients and healthy controls.
Validation I of the three peptide candidates using ELISA
Then, to verify the diagnostic value of the newly identified peptides for AD, ELISA was developed given its widespread clinical applicability. The peptide candidates were initially synthesized, which were selected from screening phases. ELISA validation was performed using serum samples from another independent cohort comprising 25 AD patients and 25 healthy subjects (Table 1). After coating wells with individual peptides, plates were incubated with sera at a 1:50 dilution. The signals were detected and amplified with an HRP-conjugated anti-human IgG. The data indicated that all three peptides had statistically significant discriminatory capacity in distinguishing AD cases from healthy controls (Figure 4A). ROC analysis was performed to further assess the diagnostic performance of these peptides. The AUC values of three peptides were above 0.68, with two (AD2024Val03/70) exceeding 0.7 (Figure 4B). These findings suggested that antibodies targeting these peptides may serve as promising biomarkers for AD diagnosis.
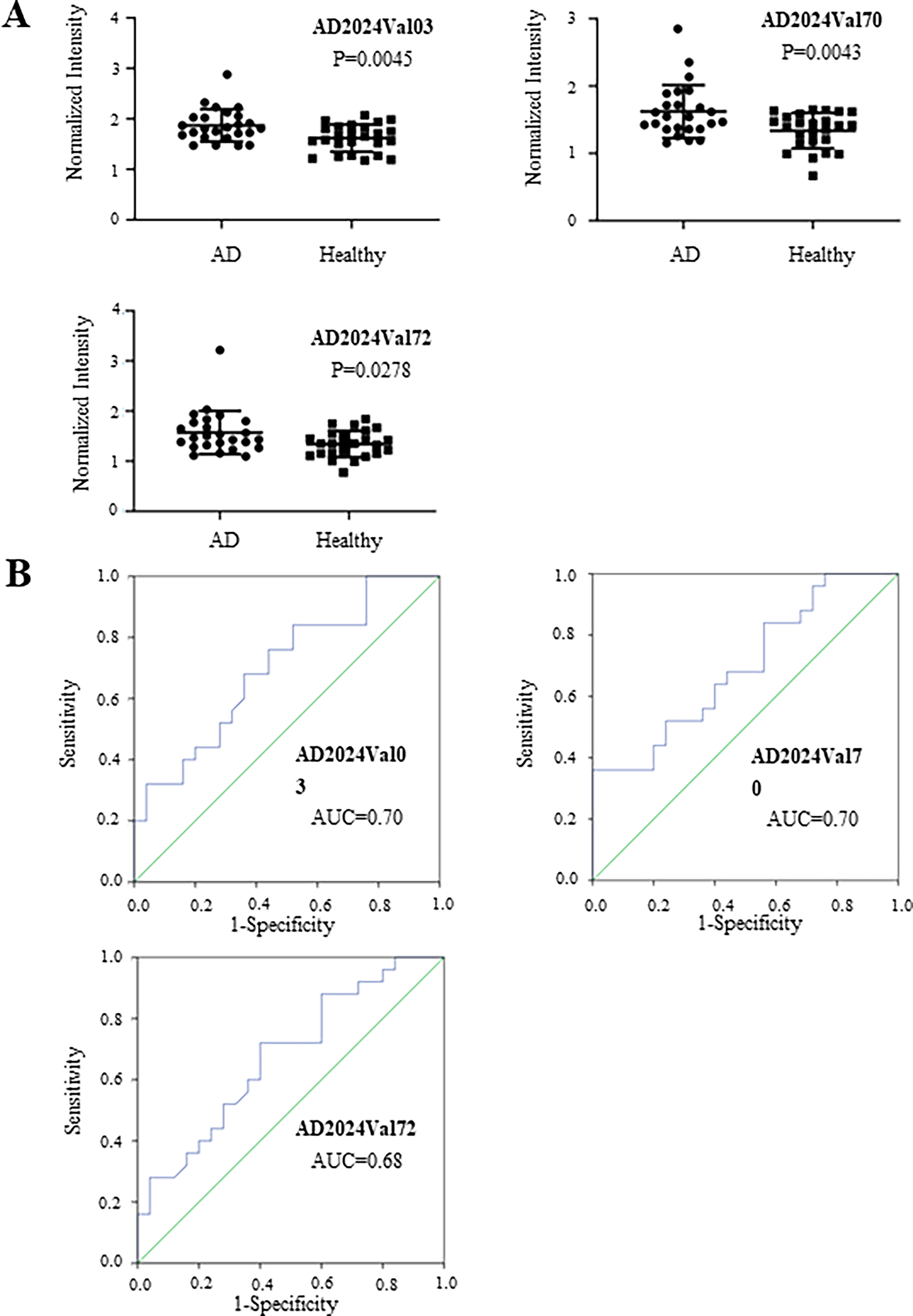
Three candidates of AD serum biomarker were confirmed in the validation phase I. A. Reactivity of the serum biomarkers with sera of AD patients and healthy controls in the validation phase I. B. ROC curve analysis of the three candidate peptides with AD patients and healthy controls.
Independent validation of the peptides with other dementia-related diseases
In addition, another independent serum cohort comprising PD (n = 14), CADASIL (n = 10), and ACI (n = 9) (Table 1), was used to additionally verify the diagnostic specificity of these AD-associated autoantibodies. The results showed that two of the three peptide candidates, i.e., AD2024Val03 and AD2024Val72, have significant reaction signals with AD patients as compared with that of other dementia-related diseases, such as PD, CADASIL, and healthy subjects (Figure 5). However, no significant discriminatory power was found between AD and ACI cohorts. In addition, AD2024Val70 showed significant differences between AD patients and healthy controls but not with other dementia groups, except for only a trend-level difference with PD. Notably, the average values of these three peptides in AD were generally higher than those in healthy individuals and other dementia-related patients (excluding ACI). Non-significant p values may be due to the limited number of samples. Thus, the diagnostic differentiation power is expected to improve with expanded sampling of other dementia-related diseases. All in all, our results showed that at least two autoantibody biomarker candidates, AD2024Val03 and AD2024Val72, are relatively specific for AD.
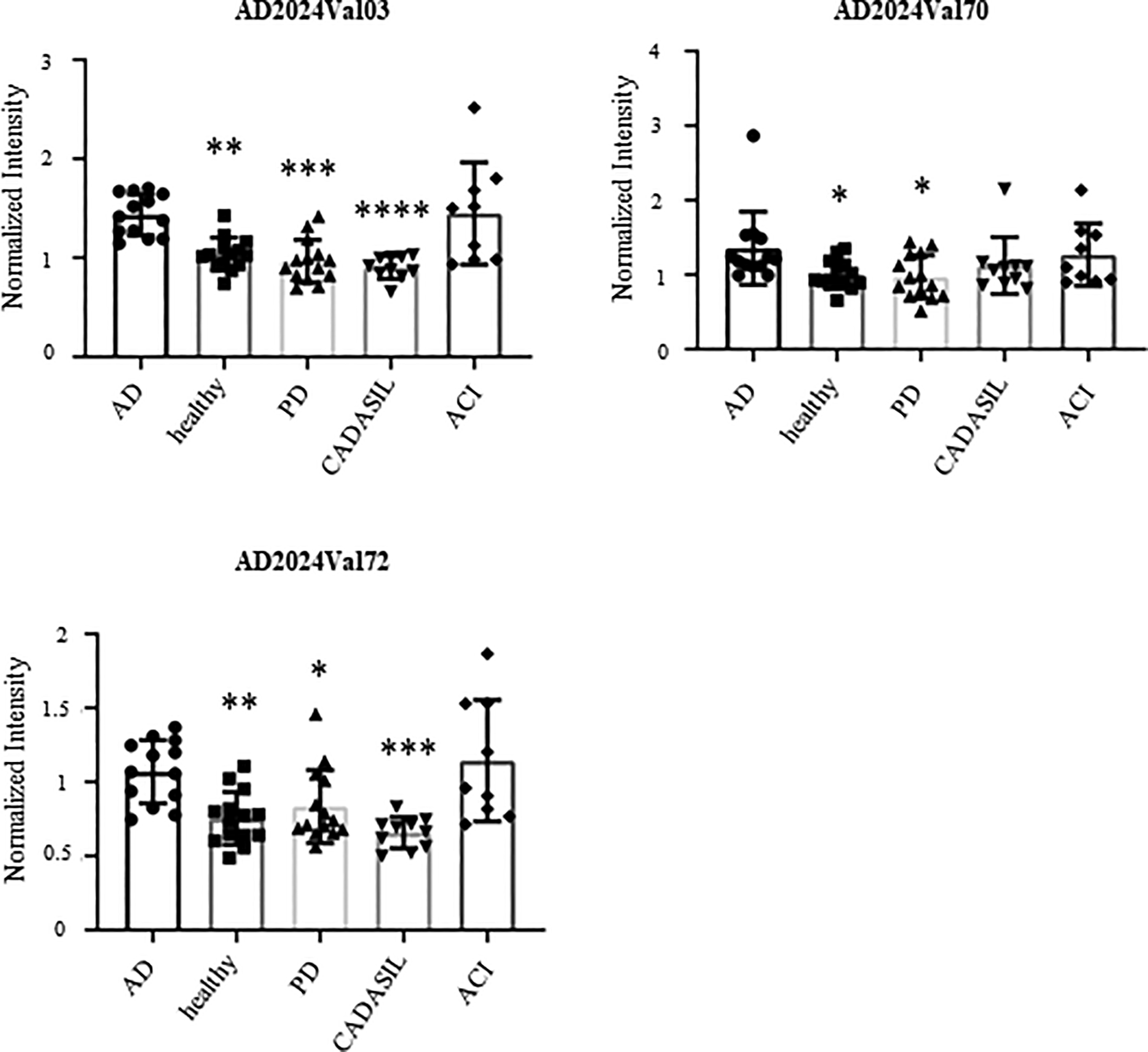
Assessment of the specificity of the three biomarkers with other dementia-related diseases. Comparison of the AD patients, healthy controls, and other dementia-related patients, i.e., PD, CADASIL and ACI. Asterisks indicate statistical difference as compared with the AD group (P < 0.05).
Analysis of the combination of the three peptide candidates
Notably, none of the individual peptides demonstrated sufficiently high specificity when used alone. We further tested whether AD2024Val03, AD2024Val70, and AD2024Val72 in combination as composite biomarker was more powerful for the AD diagnosis. The composite biomarker was evaluated by logistic regression analysis and then compared by ROC analyses (Figure 6A). Use of the three-peptide (AD2024Val03/70/72) model, named AD2024Val, enabled discrimination of AD patients from healthy controls with an AUC of 0.95 (sensitivity ∼100%, specificity ∼79%). Next, we analyzed the candidate biomarker AD2024Val against other dementia-related diseases. Similarly, AD2024Val could discriminate AD from other diseases, i.e., the AUC of PD, CADASIL, and ACI was 0.93, 1, and 0.62, respectively (Figure 6B). Taken together, these results demonstrate that the panel of three peptides (AD2024Val) could serve as a novel clinical biomarker for AD diagnosis.

ROC curve analysis using the combinational panel of the three biomarkers. A. The best model and the classifier for AD against healthy controls, based on the final three-peptide panel using logistic regression analysis from the SPSS software. B. The best model and the classifier for AD to PD, CADASIL and ACI.
Discussion
In this study, we identified noninvasive and novel blood biomarkers for AD diagnosis, with high specificity and sensitivity. Briefly, we demonstrated that the serum autoantibodies concentrations of AD2024Val03, AD2024Val70, and AD2024Val72 were significantly different in AD and control groups. Additionally, we found that the composite biomarker, AD2024Val, enabled discrimination of AD patients from healthy subjects with an AUC of 0.95 (sensitivity ∼ 100%, specificity ∼ 79%), and also had the high power of differential diagnosis, which could discriminate AD from PD and CADASIL.
At present, the most widely studied biomarkers for AD were mainly focused on imaging, CSF, and blood. 29 Mosconi et al. showed that FDG-PET can be used to differentiate AD patients from healthy subjects with 99% sensitivity and 98% specificity.30,31 However, FDG-PET is highly expensive and involves exposure to radiation, which is unrealistic in community setting. While CSF Aβ42 reduction combined with elevated T-tau and P-tau demonstrates >80% specificity and sensitivity for symptomatic AD detection,32,33 whose application was affected because of the invasive nature of lumbar puncture, which is considered unacceptable. Blood biomarkers show promising associations with standard AD biomarkers (Aβ PET and CSF biomarkers), but challenges persist in achieving comparable sensitivity and specificity, particularly for Aβ assessment. 34 Fortunately, from a clinical perspective, the biomarkers we found are convenient, noninvasive and reliable, which could aid physicians in making an accurate diagnosis for AD patients. Therefore, these autoantibody-based biomarkers we identified have the considerable potential for use in clinical practice due to high specificity and sensitivity for the diagnosis of AD, as well as minimal invasiveness. In addition, further studies may enhance their utility as an accessible biomarker for community-based AD detection.
Four independent cohorts were enrolled in this study. Briefly, For the screening phase I, we applied M13 phage displayed random peptide library and deep sequencing together to identify peptides which could be specifically recognized by IgG in the sera of AD patients. Compared with the health controls, a set of 69 peptides showed marked enrichment in AD serum. In order to improve efficiency and reduce costs, screening phase II used peptide microarrays for serum analysis, and the top 3 peptides then were selected for further validation. Next, to test their diagnostic power, we did the first round of validation and found that both AD2024Val03, AD2024Val70 and AD2024Val72 had relatively high AUC, revealing significantly different auto-antibodies levels between AD patients and healthy controls, means that they were promising diagnostic biomarkers for AD. Our findings are consistent with existing literature. A single center study reported that autoantibodies could distinguish AD from other neurodegenerative diseases. 13 This evidence supports the potential of blood autoantibodies as effective biomarker vehicles for AD screening. However, most of the studies did not verify the differential diagnostic efficacy of diagnostic markers. Diagnosing neurodegenerative diseases remains challenging because of their clinical variability. Finally, in order to further validate the sensitivity and specificity of the candidate biomarkers and make the results more convincing, the cohort IV, an additional set of sera from AD, healthy control, PD, CADASIL, and ACI, was used, and we found that AD2024Val03 and AD2024Val72 can distinguish AD patients from healthy controls, PD and CADASIL. AD2024Val70 can distinguish AD from healthy subjects and PD. Excitingly, we found that AD2024Val enabled discrimination of AD patients from healthy subjects with an AUC of 0.95 (sensitivity ∼ 100%, specificity ∼79%) and also could discriminate AD from PD and CADASIL. Given the heterogeneity and complexity of AD pathogenesis, relying on a single biomarker cannot fully capture disease pathology or enable accurate diagnosis. The synergistic effect of multiple immune markers might better reflect AD's complex pathology, which could explain why their combination significantly improves diagnostic accuracy. Taken together, these results demonstrate that three individual and combined (AD2024Val) peptides could serve as promising peripheral biomarkers for AD.
In addition, we developed a new strategy which combined M13 phage displayed random peptide library, deep sequencing, peptide microarray, with ELISA for discovering and validating serum autoantibody biomarkers for AD patients. The reliability of patient versus healthy control comparisons was ensured by ELISA-based measurement of total IgG in serum samples. Interestingly, we describe a broad, unbiased method for detecting diagnostically relevant antibodies without needing to identify target antigens. Up to now, phage display, a highly versatile platform, enables the screening and discovery of high-affinity, target-specific peptides, offering promising solutions to current diagnostic and therapeutic challenges. 35 Shen et al. identified seven candidate AD-specific autoantibodies using a custom-made immunoassay. 13 Kandiah et al. found that six autoantibodies had elevated responses in AD sera, using a microarray containing >1600 potential human autoantigens, 20 the utility of these arrays is bounded by their inclusion of only known protein autoantigens. Previous research recognized 57 phages, which showed higher seroreactivity in AD, using the T7 phage display libraries.36,37 However, it still needs to go through a complicated purification process. Particularly, in this study, we selected an M13 phage-displayed random peptide library comprising 1 × 109 different peptides, 21 and identified 69 peptides which were highly enriched in the serum of AD patients. Higher library diversity translates to more comprehensive epitope representation, improving unbiased biomarker discovery and potentially explaining our identification of 69 candidate peptides in the screening phase.
Limitations
Our failure to identify recurring motifs despite high peptide diversity implies AD's autoimmune mechanisms involve multiple antigenic targets. Additionally, during screening, most peptides showing significant antibody reactivity were sample-specific, suggesting individuals may have distinct autoantibody profiles. These findings suggest that phenotype and disease history may influence autoimmunity and warrant further investigation. Additionally, protein BLAST analysis revealed no exact matches between our validated peptides (Supplemental Table 6) and known human antigens, implying that the immune triggers could be non-protein in nature. 21 On the other hand, our validated peptides may provide deeper insights into the pathogenesis of AD, which corresponding antigens could be further studied to assess their potential as therapeutic targets.
Conclusions
In summary, the present study identified and verified a panel of three individual and combined (AD2024Val) peptides as promising serum biomarkers for AD. Exhibiting robust sensitivity and specificity, these autoantibody markers successfully discriminated between AD and healthy subjects, demonstrating potential for clinical diagnosis through single or panel-based approaches. Together, our findings expand the spectrum of peripheral blood biomarkers for AD and may provide deeper insights into the pathogenesis of AD. Future research could optimize its application as a novel biomarker for the community screening of AD patients.
Supplemental Material
sj-xlsx-1-alr-10.1177_25424823261432141 - Supplemental material for Identification of novel serum biomarkers for Alzheimer's disease screened by phage display library of random peptides
Supplemental material, sj-xlsx-1-alr-10.1177_25424823261432141 for Identification of novel serum biomarkers for Alzheimer's disease screened by phage display library of random peptides by Dandan Gao, Zhicheng Han, Xiaoyang Ai, Fengyu Wang, Danyun Lai, Chenhao Gao, Zhaohui Zhang, Shengce Tao, Junkui Shang and Jiewen Zhang in Journal of Alzheimer's Disease Reports
Supplemental Material
sj-xlsx-2-alr-10.1177_25424823261432141 - Supplemental material for Identification of novel serum biomarkers for Alzheimer's disease screened by phage display library of random peptides
Supplemental material, sj-xlsx-2-alr-10.1177_25424823261432141 for Identification of novel serum biomarkers for Alzheimer's disease screened by phage display library of random peptides by Dandan Gao, Zhicheng Han, Xiaoyang Ai, Fengyu Wang, Danyun Lai, Chenhao Gao, Zhaohui Zhang, Shengce Tao, Junkui Shang and Jiewen Zhang in Journal of Alzheimer's Disease Reports
Supplemental Material
sj-xlsx-3-alr-10.1177_25424823261432141 - Supplemental material for Identification of novel serum biomarkers for Alzheimer's disease screened by phage display library of random peptides
Supplemental material, sj-xlsx-3-alr-10.1177_25424823261432141 for Identification of novel serum biomarkers for Alzheimer's disease screened by phage display library of random peptides by Dandan Gao, Zhicheng Han, Xiaoyang Ai, Fengyu Wang, Danyun Lai, Chenhao Gao, Zhaohui Zhang, Shengce Tao, Junkui Shang and Jiewen Zhang in Journal of Alzheimer's Disease Reports
Supplemental Material
sj-xlsx-4-alr-10.1177_25424823261432141 - Supplemental material for Identification of novel serum biomarkers for Alzheimer's disease screened by phage display library of random peptides
Supplemental material, sj-xlsx-4-alr-10.1177_25424823261432141 for Identification of novel serum biomarkers for Alzheimer's disease screened by phage display library of random peptides by Dandan Gao, Zhicheng Han, Xiaoyang Ai, Fengyu Wang, Danyun Lai, Chenhao Gao, Zhaohui Zhang, Shengce Tao, Junkui Shang and Jiewen Zhang in Journal of Alzheimer's Disease Reports
Supplemental Material
sj-xlsx-5-alr-10.1177_25424823261432141 - Supplemental material for Identification of novel serum biomarkers for Alzheimer's disease screened by phage display library of random peptides
Supplemental material, sj-xlsx-5-alr-10.1177_25424823261432141 for Identification of novel serum biomarkers for Alzheimer's disease screened by phage display library of random peptides by Dandan Gao, Zhicheng Han, Xiaoyang Ai, Fengyu Wang, Danyun Lai, Chenhao Gao, Zhaohui Zhang, Shengce Tao, Junkui Shang and Jiewen Zhang in Journal of Alzheimer's Disease Reports
Supplemental Material
sj-xlsx-6-alr-10.1177_25424823261432141 - Supplemental material for Identification of novel serum biomarkers for Alzheimer's disease screened by phage display library of random peptides
Supplemental material, sj-xlsx-6-alr-10.1177_25424823261432141 for Identification of novel serum biomarkers for Alzheimer's disease screened by phage display library of random peptides by Dandan Gao, Zhicheng Han, Xiaoyang Ai, Fengyu Wang, Danyun Lai, Chenhao Gao, Zhaohui Zhang, Shengce Tao, Junkui Shang and Jiewen Zhang in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
We would like to thank clinical team members. Moreover, we thank Dr Chao Jiang for excellent technical assistance.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by The Ethics Committee of Zhengzhou University People's Hospital (Approval No. HNEECKY-2020-76).
Consent to participate
The participates provided their written informed consent to participate in this study.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China Grants, the Key R&D Program of Henan Province, (grant number 81873727, 82171196, 241111313500).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The original contributions presented in the study are included in the article/supplemental materials, further inquiries can be directed to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.