
Abstract
We investigated the effects of an orexin receptor antagonist on sleep profiles assessed by actigraphy, and cognitive function in patients with dementia with Lewy bodies (DLB). Thirteen probable DLB patients who were taking an orexin receptor antagonist for insomnia were recruited and underwent actigraphy before and after taking lemborexant. Cognitive function and severity of sleep disturbance were compared before and after taking lemborexant. No significant differences in sleep quality and cognitive function were observed in DLB patients between before and after taking lemborexant. These results suggest the tolerability of lemborexant in patients with DLB.
Introduction
Dementia with Lewy bodies (DLB) is recognized as the second most common cause of degenerative dementia in older people. 1 As generally known, sleep disturbance represented as REM sleep behavior disorder (RBD) is a common characteristic observed in DLB patients. Thus, RBD is described as a clinical feature in the diagnostic criteria for DLB. 1
In the daily clinical setting, physicians often do not use orexin receptor antagonists for DLB patients, because they induce nightmares and RBD. A recent study 2 reported that DLB patients with RBD have higher plasma orexin A levels than those without RBD. Moreover, we reported that there is a significant positive correlation between the severity of sleep disturbance including RBD and cerebrospinal fluid orexin A level in DLB patients. 3 If these results are true, there is the possibility that orexin A is an important cause of RBD in patients with DLB. In other words, there is a possibility that orexin receptor antagonists may be a potential treatment for RBD in patients with DLB.
Assessment of sleep quality including RBD is commonly performed by polysomnography (PSG). However, as PSG is difficult to perform in patients with dementia, actigraphy is used as a simple alternative method to assess their sleep quality. 4 One drawback is that although actigraphy can evaluate seep quality, it cannot evaluate detailed sleep stages, including REM sleep. As a first step towards analyzing the efficacy of orexin receptor antagonists in patients with DLB, the main aim of this study was to confirm the tolerability of the orexin receptor antagonist lemborexant in DLB patients. This is the first study demonstrating the tolerability of an orexin receptor antagonist in patients with DLB using actigraphy.
Methods
Thirteen probable DLB 1 patients taking lemborexant (5 mg/day) for insomnia underwent actigraphy both before and after taking lemborexant. All patients underwent general physical, neurological, and psychiatric examinations, extensive laboratory tests, and computed tomography or magnetic resonance imaging to establish a clinical diagnosis and to exclude other potential causes of dementia. None of the patients had a history of psychiatric disease or psychiatric medication use. Some patients were taking anti-Parkinson drugs and donepezil. However, no medication changes were made during participation in this study.
Cognitive function was assessed by the Mini-Mental State Examination (MMSE), 5 Montreal Cognitive Assessment (MoCA), 6 and Alzheimer's Disease Assessment Scale-cognitive subscale (ADAS-cog). 7 The severity of sleep disturbance was assessed by the Japanese version of the Epworth sleepiness scale (JESS), 8 Japanese version of the Athens Insomnia Scale (AIS-J), 9 and the Japanese version of the REM sleep behavior disorder screening questionnaire (RBDSQ-J). 10 All participants wore an Actigraphy (ActiWatch, Ambulatory Monitoring Inc., NY, USA) around their wrist for 7 consecutive days. Sleep variables, including total sleep time, sleep efficiency, wake state after sleep onset (WASO, expressed in minutes), and the number of awakenings during sleep were calculated using Action W 2 software (Ambulatory Monitoring Inc.) based on 7-day records. This study was approved by the Ethics Committee of Tokyo Medical University (study approval no.: SH4045).
Results
Table 1 shows the results of the efficacy of lemborexant on various parameters in DLB patients. There were no significant changes in cognitive function (i.e., MMSE, MoCA, ADAS-cog scores) between before and after taking lemborexant in DLB patients. Questionnaires on sleep quality (i.e., JESS, AIS-J, and RBDSQ-J scores) showed no significant changes between before and after lemborexant intake. Regarding the results of actigraphy, there were no significant changes in all sleep variables after taking lemborexant.
Sleep quality and cognitive function of DLB patients after taking lemborexant.
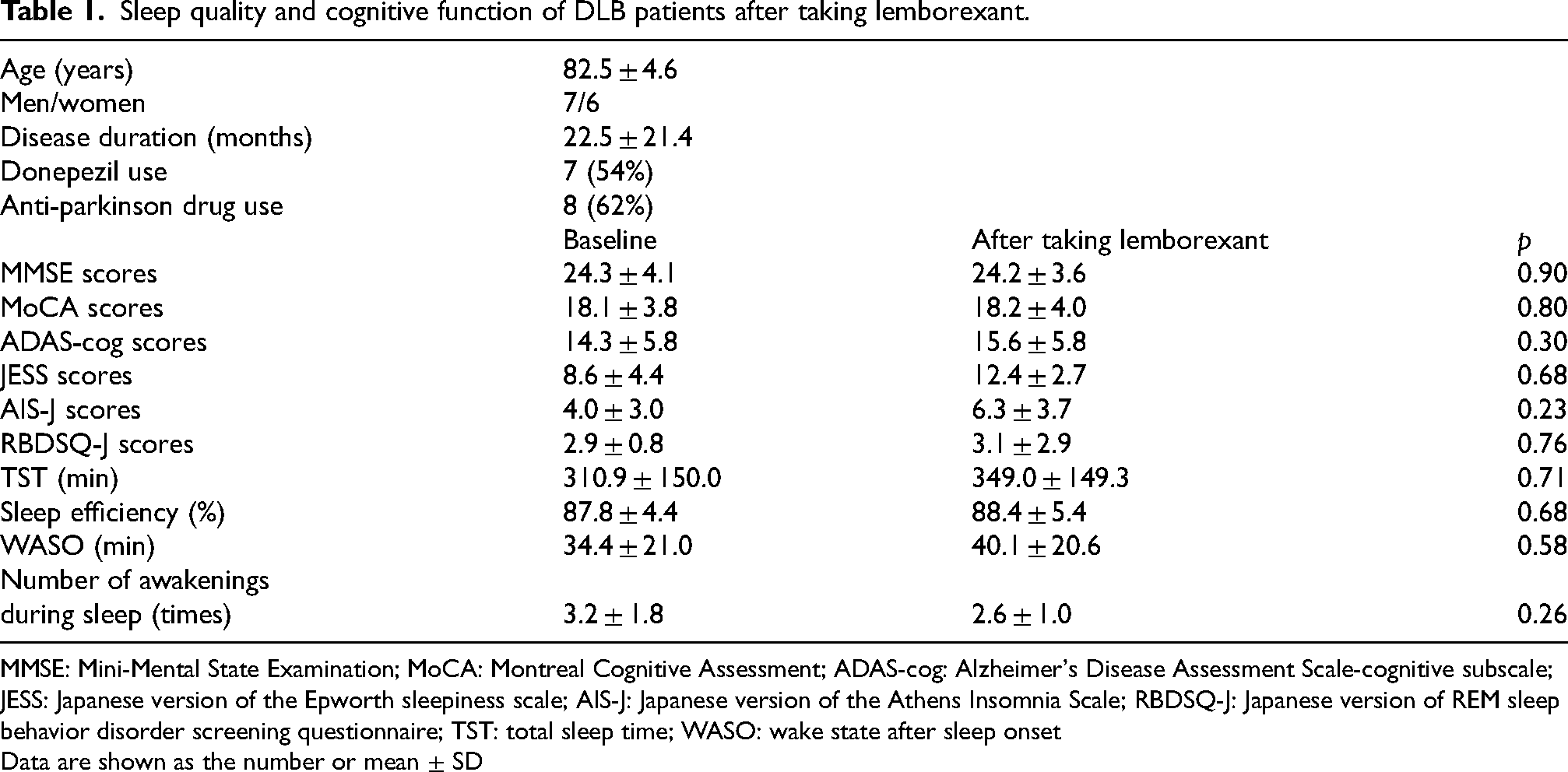
MMSE: Mini-Mental State Examination; MoCA: Montreal Cognitive Assessment; ADAS-cog: Alzheimer's Disease Assessment Scale-cognitive subscale; JESS: Japanese version of the Epworth sleepiness scale; AIS-J: Japanese version of the Athens Insomnia Scale; RBDSQ-J: Japanese version of REM sleep behavior disorder screening questionnaire; TST: total sleep time; WASO: wake state after sleep onset
Data are shown as the number or mean ± SD
Discussion
In contrast to our hypothesis, lemborexant did not improve sleep quality in patients with DLB. Moreover, there was no significant difference in the cognitive function of DLB patients after taking lemborexant. At first glance, these results appear to be negative data. However, they can be considered as positive data showing that lemborexant does not worsen cognitive function and sleep quality in patients with DLB. Therefore, these results suggest that orexin receptor antagonists are well tolerated in patients with DLB.
In the daily clinical setting, clinical physicians often do not prescribe orexin receptor antagonists for DLB patients because they induce nightmares and RBD. However, a phase 3 clinical trial of orexin A receptor antagonists such as suvorexant and lemborexant demonstrated that orexin A receptor antagonists do not significantly increase nightmares compared with placebo in DLB patients.11,12 Moreover, a previous review showed that orexin receptor antagonists are not included in medications that reported to accentuate nightmares. 13 Furthermore, our results showed that lemborexant did not worsen sleep quality (i.e., RBDSQ-J score and WASO) in patients with DLB. Furthermore, regarding cognitive function, we found that lemborexant does not worsen cognitive function in patients with DLB, similar to in Alzheimer's disease patients. 14 Previous studies have shown that orexin receptor antagonists improve insomnia and sleepiness scores in patients with insomnia.15–17 In contrast with previous studies, we found that in DLB patients, slight decreases in JESS and AIS-J scores occurred after taking lemborexant, although the changes were not statistically significant. Notably, lemborexant did not worsen cognitive function in DLB patients, despite causing a slight decrease in sleep quality questionnaire scores. As mentioned above, our present results suggest the tolerability of lemborexant in DLB patients.
Our previous study 3 showed that there is a significant positive correlation between the severity of sleep disturbance, including RBD, and cerebrospinal fluid orexin A level in DLB patients. To test our hypothesis that orexin receptor antagonists may be a potential treatment for RBD in DLB, it is necessary to assess RBD by PSG in patients with DLB. However, in our previous and present studies, we assessed RBD only using RBDSQ-J. Because PSG was difficult to perform on the participants in our study (patients with DLB), we used questionnaires and actigraphy. RBD-SQJ is a screening questionnaire, and it is generally known that questionnaire assessments have reproducibility issues in cognitively impaired participants. Moreover, actigraphy cannot record electroencephalography (EEG), and infers sleep quality from movement. Although PSG remains the “gold standard” for sleep assessment, PSG has some disadvantages when used in dementia patients. Patients with cognitive impairment have low tolerance to sleep testing in a sleep laboratory, and as the induction of delirium can exacerbate the “first-night effect,” it is difficult to accurately assess their sleep patterns. Furthermore, although PSG can only record one night of sleep in a specialized environment of a sleep laboratory, actigraphy enables evaluation over multiple days in a familiar environment. Recently, there have been substantial advances in in-home sleep EEG devices. 18 In the future, we plan to utilize these devices to perform accurate RBD assessments of DLB patients to further test our hypothesis.
This study has several limitations. First, this study was carried out in a single memory disorder clinic, and the number of patients enrolled was relatively small. Therefore, potential type II errors caused by minimal detectable effect size should be considered. Second, no significant difference in cognitive function and sleep quality was detected between before and after taking lembotrexant in DLB. However, the absence of significant differences cannot strictly be interpreted as confirming the tolerability of lembotrexant for DLB. Therefore, considering statistical power, further studies with larger sample sizes are needed to verify the results of this study. Second, sleep parameters were measured only by actigraphy in this study, although ideally, PSG is recommended for the detailed evaluation of sleep architecture. Third, it is necessary to conduct comparison studies with other sleeping medications to clearly demonstrate the effectiveness of orexin receptor antagonists. Finally, another limitation of the present study is the lack of autopsy confirmation of DLB in all patients. We carefully applied rigorous standardized sets of diagnostic criteria for DLB, all of which have been shown to have a positive predictive value of greater than 80%, as judged by postmortem diagnosis. 19 Further large patient number and multicenter studies, with more detailed evaluation of sleep parameters by PSG and consideration of the results of pathological examinations are required to confirm our results.
In conclusion, our results suggest that orexin receptor antagonists may be useful as sleep-inducing drugs that do not worsen cognitive function and sleep quality in DLB patients. In other words, lemborexant may be well tolerated in patients with DLB.
Footnotes
Acknowledgements
We are grateful to the medical editors of the Center for International Education and Research of Tokyo Medical University for reviewing the manuscript.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Tokyo Medical University (study approval no.: SH4045) on April 2, 2024, with the need for written informed consent being waived.
Consent to participate
Not applicable
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
As the data includes personal information of the patients, it cannot be made publicly available in its entirety. We have uploaded the minimum anonymized data (i.e., demographic data, scores of questionnaires, and raw actigraphy data) necessary to reproduce the research (DOI: 10.6084/m9.figshare.31568938).