
Abstract
Advanced Alzheimer's disease is a terminal illness causing more intense, prolonged suffering than clinicians generally recognize. At least 500,000 Americans are trapped in the “Dementia Gap”, a previously unidentified substage of advanced dementia. Patients lack capacity to voluntarily stop eating and drinking but can still eat and drink independently, making “dementia-specific” living wills ineffective until further disease progression requires assistance with oral feeding and hydrating. Additionally, patients experience “Non-Observable Suffering”: inner emotional angst, inexpressible physical pain, and bi-directional suffering shared with loved ones. A dangerous non sequitur fallacy can lead casual observers to extrapolate peaceful inner states from withdrawn external behavior: “She's not suffering; she's just sitting there.” To effectively relieve intolerable suffering, this article introduces “Moderate Anesthesia”—palliative sedation to unconsciousness modified to be clearly distinguishable from euthanasia. Cases demonstrate moral justification grounded in Sulmasy's “Reinvented Rule of Double Effect,” “Parsimonious Direct Sedation,” or the Principle of Proportionality. Two Dementia Gap patients the author treated are compared with two advanced cancer patients. Two withdrawn patients “awakened” through skillful interviewing, exemplifying this ethical warning: diligent efforts to detect and relieve non-observable suffering should precede implementing treatments of last resort. The article presents the “Three-Source Concordance” protocol using an illustrated patient decision aid and polling Patient Decision Committee members’ substituted judgments to confirm the clinical appropriateness of implementing POLSTs that patients completed during advance care planning. A 42% cumulative lifetime dementia risk means many of us may reach the Dementia Gap. Launching the ARISE movement—Advocate by Recognizing and Investigating Suffering's (hidden) Existence—and convening expert panels to develop practice guidelines are moral imperatives.
Keywords
Clinical semantics
“Moral” versus “ethical”: Moral refers to substantive judgments about acts being right or wrong and therefore permissible or not. Ethical refers to the systematic framework based on reasoning that strives to answer moral questions or decide between moral alternatives. The goal of this article is to alleviate physicians’ fear of moral criticism by providing an ethical path that includes compelling arguments based on widely accepted relevant principles.
Methods of nourishing: “Eating and drinking independently” means patients can recognize the substances food and fluid and put them into their mouth, which can be a social activity called “dining.” “Oral feeding and hydrating” means assistance caregivers provide for dependent patients by putting food and fluid into their mouths, often in response to physicians’ orders.
Professional disciplines: “Physicians” in this article encompasses healthcare providers who can determine decision-making capacity and sign POLST orders—in many states, advance practice nurse practitioners and physician assistants. If significant time elapses between advance care planning and implementation, the “treating physician” may differ from the advance care planning (ACP) physician. Clinicians with other backgrounds can facilitate ACP and help prepare patients’ POLSTs. They include appropriately trained psychologists, social workers, chaplains, bioethicists, and end-of-life doulas.
“Living Will”: means the part of “advance directive” documents referred to as “advance health care instructional directive.” It does not include durable power of attorney for healthcare decisions or other strategic documents.
“POLST”: a set of immediately actionable physician orders that other clinicians are usually legally required to follow and can be implemented in any treatment setting. (POLST is not an acronym.)
“Agents”: means legally recognized representatives, proxies, or decision-making surrogates—whether designated by a durable power of attorney for healthcare decisions or by the default hierarchy embodied in statutes in most states.
“Non-Observable Suffering” (N-O-S) can exist alone or in addition to observable suffering revealed by physicians’ current examinations of inarticulate or incapacitated patients. This article describes and provides examples of six sub-categories of N-O-S.
“Intolerable suffering” and “unbearable suffering” are sometimes used interchangeably. This article considers either intensity sufficient to warrant a treatment of last resort but adds the criterion of urgency to “unbearable”: patients with unbearable suffering will not want to wait for medication to be increased slowly before their awareness of suffering is relieved.
Introduction: “Sarah” (a composite patient) living in the Dementia Gap
Past history
Sarah is a “Person with Incapacity from Neurodegenerative Etiology” (
Sarah is suffering
Despite appearing peaceful or asleep most of the time, Sarah could be experiencing profound suffering that remains largely non-observable, difficult to detect and therefore goes untreated, or primarily affects her loved ones. 4 Most of her observable suffering is untreatable. Dementia caused the loss of all her important relationships since she no longer can recognize loved ones or close friends, communicate coherently and meaningfully, or recall memories of the peak life experiences they shared. Some of the consequences are difficult-to-detect loneliness and loss of sense of self that her previous relationships helped define. Dementia also disrupted her life narrative, including her roles as wife, mother, friend, and attorney. The consequence: she has lost most of her joy and meaning in life.
Sarah's loved ones are suffering
Janson et al. found that caregiver suffering includes “stress and adjustment disorders, depression, anxiety, sleep disorders, diseases of the spine and back, pain conditions, and lower quality of life.” 5 Sarah's loved ones also suffered from their “long goodbye.” As dementia progresses, her personality changed and her mind slowly died, making it impossible to enjoy her. Instead, they feel helpless as they experience profound “bi-directional empathic suffering” that acknowledges Sarah would be horrified if she had the ability to view her current condition with capacity that still understood her lifelong values. 6
To this incomplete list of sources of suffering is Sarah's haunting dread that her survivors will retain mostly tarnished memories of her final years during which she lacked dignity according to her former self's judgment. Example: caregivers must now change her diapers due to fecal incontinence.
The dismissive non sequitur fallacy
If casual observers (including healthcare professionals) conclude, “She's not suffering; she's just sitting there,” they will have wrongly extrapolated from her external state of apparent calm that her inner emotional state is mostly peace (except for her occasional episodes of agitation). This assumption could diminish the efforts of professionals and friends and relatives to investigate and treat her possible non-observable suffering (N-O-S).
Recently, Sarah's behavior changed
About a month ago, she began to repeatedly cry out, “Help me. Help me. Help me.” These vocalizations recently escalated in frequency and intensity. Increasing her dose of quetiapine and prescribing acetaminophen—first without, and then with codeine—did not help. At the institution's staff meeting, all concurred that (A) Sarah's suffering had progressed to the point where its intensity has become intolerable, and (B) non-sedating modalities of treatment cannot provide effective relief.
During advance care planning (ACP), Sarah completed an advance directive specifying Natural Dying (ND) if someday she reached an irreversible condition causing severe suffering. ND includes two physician orders: (A) cease assisted oral feeding and hydration, and (B) always place food and fluid within reach. The latter makes this treatment of last resort legal, ethical, and possible to view as moral. 7 But her current clinical state presents a challenge: ND cannot be implemented because she can still eat and drink independently. Withholding food and fluid is not an option; it is euthanasia, which is illegal in the U.S. Also, many view it as immoral.
To summarize, in the past Sarah was not quietly at peace; and now, her suffering is likely intolerable. Relief requires a treatment of last resort other than ceasing assisted feeding. She meets the criteria of living in a substage of dementia, a therapeutic desert, that has previously been rarely recognized, which this article refers to as the “Dementia Gap.”
Scenarios similar to Sarah's occur frequently across America's memory care units, skilled nursing facilities, and private homes. This article's Supplemental Material includes the estimate that about 500,000 patients are living in the Dementia Gap. Worldwide, the number is about 6 million. Therefore, characterizing advanced dementia as “a cruel, burdensome, and prolonged terminal illness” understates both individual depth and scope of challenges dementia presents to patients and their loved ones.
Fear of Alzheimer's disease among retirees ranks higher than COVID-19, cancer, heart attack and stroke” 8 despite the public's limited (if any) awareness of the additional challenges presented by the Dementia Gap and the phenomenon of N-O-S, which this article reveals.
Factors perpetuating inadequate palliative care for Dementia Gap patients
The
Yet European data challenge the characterization of rarity. Continuous deep end-of-life sedation ranged from 2.5% in Denmark to 24% in Switzerland.13–16 About one-third of residents in Dutch nursing homes received fixed-schedule prescriptions for both midazolam and morphine within 14 days of death.
17
Surveys of physician attitudes, such as Putman et al.'s study, which used Physician reluctance to implement PSU until death varies depending on the type of suffering. Heijltjes et al. found that for patients having a several-week prognosis, 22–66% of physicians would consider continuous sedation acceptable for physical suffering, but only 5–42% for psycho-existential suffering.
19
“Practitioners may be unwilling to use [Moderate Anesthesia, here] based on their fear of civil liability, disciplinary penalties, or criminal sanctions.” 20 They may also want to avoid experiencing moral distress by seeing themselves complicit in hastening patients’ deaths. 7
How this article is organized
The article's goal is to present a protocol to reduce patient suffering in the Dementia Gap that others can view as moral, so that the proposed treatment of last resort can be accepted and used based on patients’ need. Incapacitated patients who can eat and drink independently need Moderate Anesthesia. This article extends the author's previous work regarding whether orders for Natural Dying (that cease assisted oral feeding and hydration for patients whose survival depends on such assistance) can be considered moral. 7
After defining key terms, this article examines societal expectations for physicians in reducing patient suffering; operationally defines “successful” advance care planning; and explains why most living wills fail to fulfill their promise (to inform all when to implement what treatment).
The article then presents the process of making treatment decisions and moral justifications for four patients. I treated two who were living in the “Dementia Gap.” I briefly review two capacitated cases for comparison; both had advanced cancer. One is often discussed by bioethicists. The other became a Medical Aid in Dying celebrity. The fifth and sixth patients are brief anecdotes of “awakening” from long, profound withdrawal by therapists who researched patients’ personal history and used skill in their interview techniques. Comment: the clinical information available was not as complete as if each were a formal case report. One required urgent treatment and the sources of data for the other four included a book chapter and YouTube videos. But the information sufficed to treat them and to provide adequate summaries for readers to appreciate the clinical and moral challenges. Here is the list of patients (numbered to make them easy to refer to):
This article's Supplemental Material estimates the prevalence of Americans in late-stage dementia whose suffering needs a treatment of last resort other than ND when ND cannot be effective. It also compares the scholarly and financial support for Medical Aid in Dying (MAiD) with efforts to educate physicians about sedation as a legal and ethical option for patients living in the Dementia Gap.
Definitions of new key terms
The term PINE (Person with Incapacity from Neurodegenerative Etiology) was introduced with the story of Sarah. While this article acknowledges established dementia staging scales such as Clinical Dementia Rating (CDR), 21 Functional Assessment Staging (FAST), 22 and Global Deterioration Scale (GDS) 23 —treatment decisions primarily rely on judgments of intensity of suffering that planning principals made during ACP, if they later become incapacitated.
A patient-friendly explanation for PINE: “Neurodegenerative” refers to progressive disorders of mental functioning whose underlying cause (“etiology”) is brain disease. This terminology aligns with DSM-5 criteria 24 and insurance claim filing requirements.
The “Dementia Gap” is a period of time along PINEs’ progressive disease trajectory that begins when PINEs lose capacity to make the decision to Voluntarily Stop Eating and Drinking (VSED). It ends when they lose their ability to eat and drink independently. See Figure 1 (below).
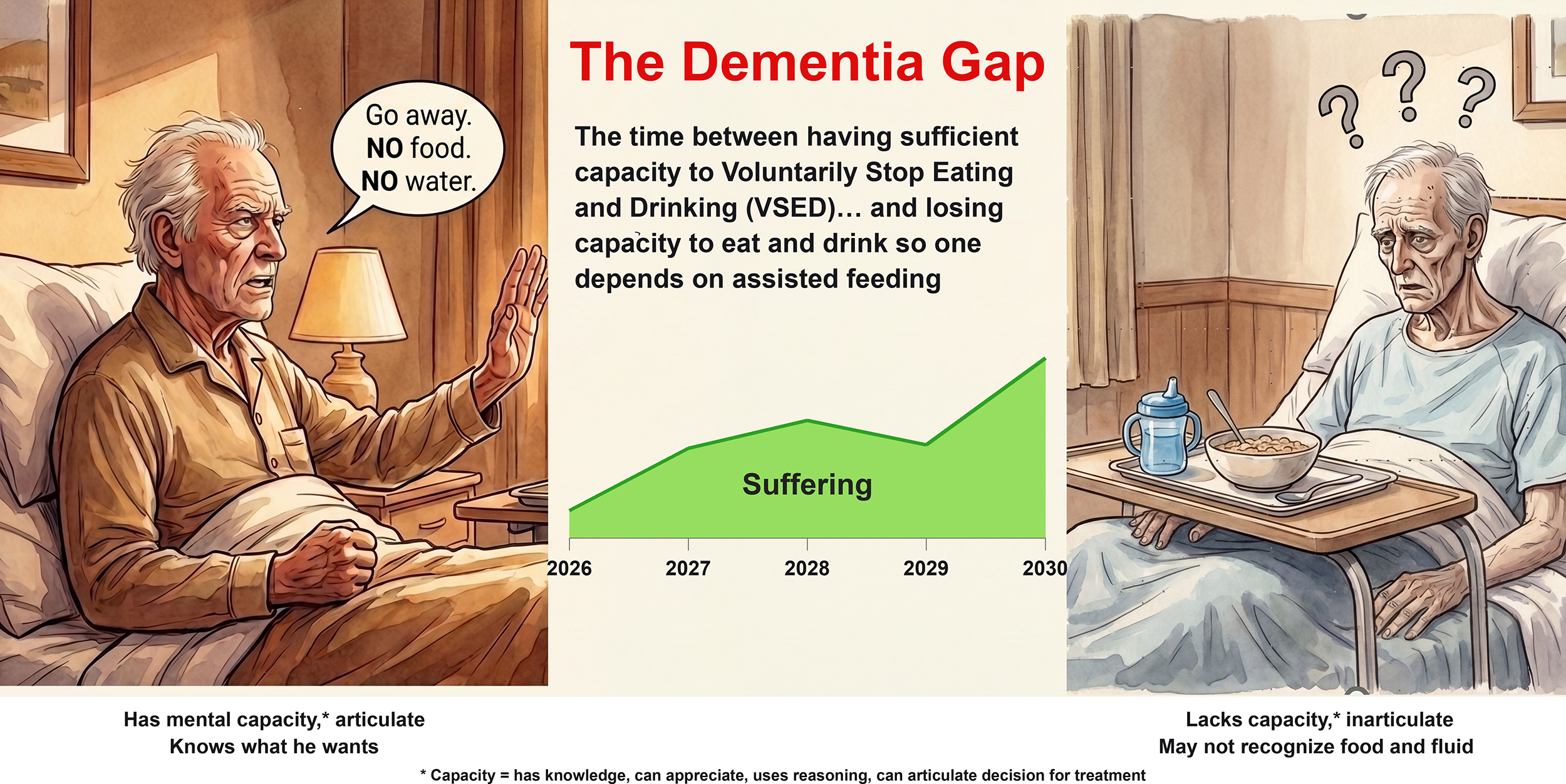
Definition and timeline of the “Dementia Gap”.
Patients in the Dementia Gap may endure prolonged suffering as they wait for their disease to progress until they become dependent on assisted feeding and qualify for Natural Dying. Ironically, their continued suffering depends on retaining the activity of daily living that allows them to survive: putting food and fluid into their mouths if placed within their reach.
The “Dementia Fear” manifests as anticipatory anxiety as capacitated patients worry about living after they have lost autonomy. They worry about their personal prolonged suffering and burdening loved ones. They experience an excruciating existential dilemma: continue to enjoy life or to orchestrate a peaceful death before they lose capacity—a predicament whose challenging timing goal is sometimes referred to as “Five Minutes to Midnight.” 25
Alice Howland in Still Alice 26 wanted to live as long as possible but waited too long to execute her plan to die, so she was forced to endure prolonged advanced dementia. Yet even if her timing had succeeded, she would have sacrificed months or years of quality life, since many aspects of enjoyable living do not require DMC. For over a decade, Davis has advocated preemptive suicide to avoid reaching advanced dementia. 27 To my knowledge, there are no estimates for its incidence.
One goal of this article is to reduce the Dementia Fear by completing ACP that gives patients confidence that others will honor their end-of-life wishes, and thereby makes premature dying unnecessary.
The physicians’ role is to reduce patients’ suffering. So, if their orders prolong suffering, or fail to mitigate suffering, are physicians causing suffering?
The American Medical Association's Code of Ethics, Section 1.1.1, begins by reflecting this primacy 28 : “The practice of medicine, and its embodiment in the clinical encounter between a patient and a physician, is fundamentally a moral activity that arises from the imperative to care for patients and to alleviate suffering.” If these two imperatives conflict, AMA's Code of Ethics Opinion 2.20 provides wise authoritative guidance: “The social commitment of the physician is to sustain life and to relieve suffering. Where the performance of one duty conflicts with the other, the preferences of the patient should prevail.” 29 That medicine arises from the imperative to alleviate suffering is also the spirit behind the ARISE Movement this article proposes later.
If physicians write or continue orders that prolong the dying process of suffering patients who expressed the opposite preference, physicians thereby violate the bioethical principle of nonmaleficence (Do No Harm) 30 —not by creating new harm, but by prolonging existing harm. Failure to prevent suffering violates nonmaleficence whether through action or inaction. Physicians are responsible for harms they cause by omission if they have (A) a duty to act (to relieve suffering), (B) the ability to act (available sedative medications), but (C) failed to act (not ordering effective treatment), thereby continuing or worsening patient suffering. 31
This guidance is consistent with: “The healthcare team members need to do as much as possible to benefit the patient (beneficence) while taking the necessary precautions not to prolong the dying person's suffering (non-maleficence),” and, “When the treatment provided by the healthcare team is medically futile or prolongs patient suffering, terminating the care and allowing the patient to die is necessary.” 32 “Physicians Obligations” include, according to Varkey (among others): “Avoidance of harm to the patient in the course of care.” 33
AMA's Opinion 2.20 is unequivocal: patients’ preferences must prevail. Therefore, physicians must implement treatment that aligns with patients’ known wishes—whether learned from patients’ current capacitated expression, their legally designated agents’ current instructions, or past living wills. Opinion 2.20 can justify two physicians’ orders for treatments of last resort: (A) cease assistance with oral feeding and hydration, and provide adequate sedation if non-sedating methods of treatment failed to provide relief. In 2023, Gilbertson et al. wrote: “Dying patients…should not be left to suffer.” 34 This sentiment echoes Freshwater's 1999 statement: “Patients must never be left to suffer so that doctors ‘stay out of trouble.’” 35
Moderate Anesthesia: definition and ethical justification
Moderate Anesthesia (MA) is a treatment of last resort for PINEs living in the Dementia Gap who (A) experience intolerable suffering, (B) cannot obtain relief through any non-sedating treatment (or, are very unlikely to), (C) have lost decision-making capacity, and (D) can still independently eat and drink—regardless of their estimated life expectancy.
MA's consent form, which planning principals discuss and sign during ACP, has three key features. First, it
Second, the consent form explicitly acknowledges two identified risks. As Twycross stated generally about palliative sedation to unconsciousness, MA can end “biographical life” (meaningful human interaction); and shorten “biological life.” 37
Third, the separate advance decision to refuse artificial nutrition and hydration aligns with recommendations from the Choosing Wisely Workgroup, 38 the Alzheimer's Association, 39 and Terman et al. 40
Clinical aspects of Moderate Anesthesia
The goal is to administer sedative medications at the minimum dose necessary to relieve suffering, ideally light sedation that targets the source of suffering that allows eating and drinking to continue. Higher doses of medication for deeper sedation may be needed to depress patients’ awareness of suffering; however, the level used is often similar to that used for colonoscopy, deeper than “moderate sedation,” but not as deep as “deep sedation or analgesia” (in one recognized classification system 41 ).
The consent form was written so many early-stage dementia patients can understand it. Example: “We will give you more medicine only if a smaller amount does not calm you down or relieve your pain. Then, you will be in a deep sleep, like during surgery. You will not feel anything or be able to talk. This could last until you die. You may die sooner. If you might be able to make the decision to live longer, we will let you wake up to ask you what you want.” (Note: this explanation has a fifth grade reading level per Flesch-Kincaid. 42 )
The relevance of considering life expectancy when considering MA
In 2007, de Graeff et al. reviewed the controversial practice of continuous deep palliative sedation. Their recommended practice standards included: “Death should be expected within hours to days. 43 Gilbertson et al. later extended life expectancy to six months. 34
This article posits two points to argue that specifying any duration of time is arbitrary: First, several European countries and Canada use the criterion of unbearable suffering for medical aid in dying (MAiD), usually, with no other path available for relief that is tolerable, to which both patient and physician agree. 44
Second, a precedent was established for the right of non-terminally ill capacitated patients to express their legal right to refuse food and fluid. Elizabeth Bouvia had cerebral palsy from birth. When she was 28, Bouvia challenged her physicians and hospital who were keeping her alive against her verbal, capacitated expressed will by force feeding her through a nasogastric tube. A 1986 California Court of Appeals set the precedent for the legality of refusing food and fluid. 45 The ruling explained, “The fact that she is young and not terminally ill does not negate her right to refuse medical treatment; it only lengthens the time during which she must endure the very suffering and indignities she seeks to avoid if treatment is imposed against her will.”
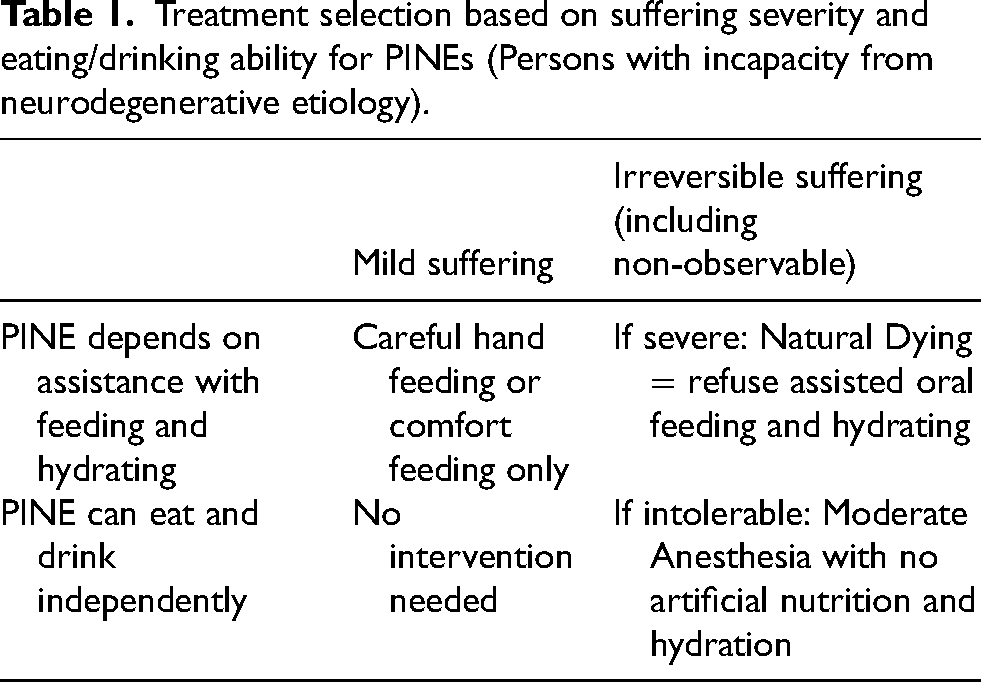
Table 1, a decision matrix, clarifies key terms. The middle row covers typical “dementia-specific” living wills for patients who require assisted feeding. The bottom row covers patients in the Dementia Gap who retain independent eating and drinking ability.
Treatment selection based on suffering severity and eating/drinking ability for PINEs (Persons with incapacity from neurodegenerative etiology).
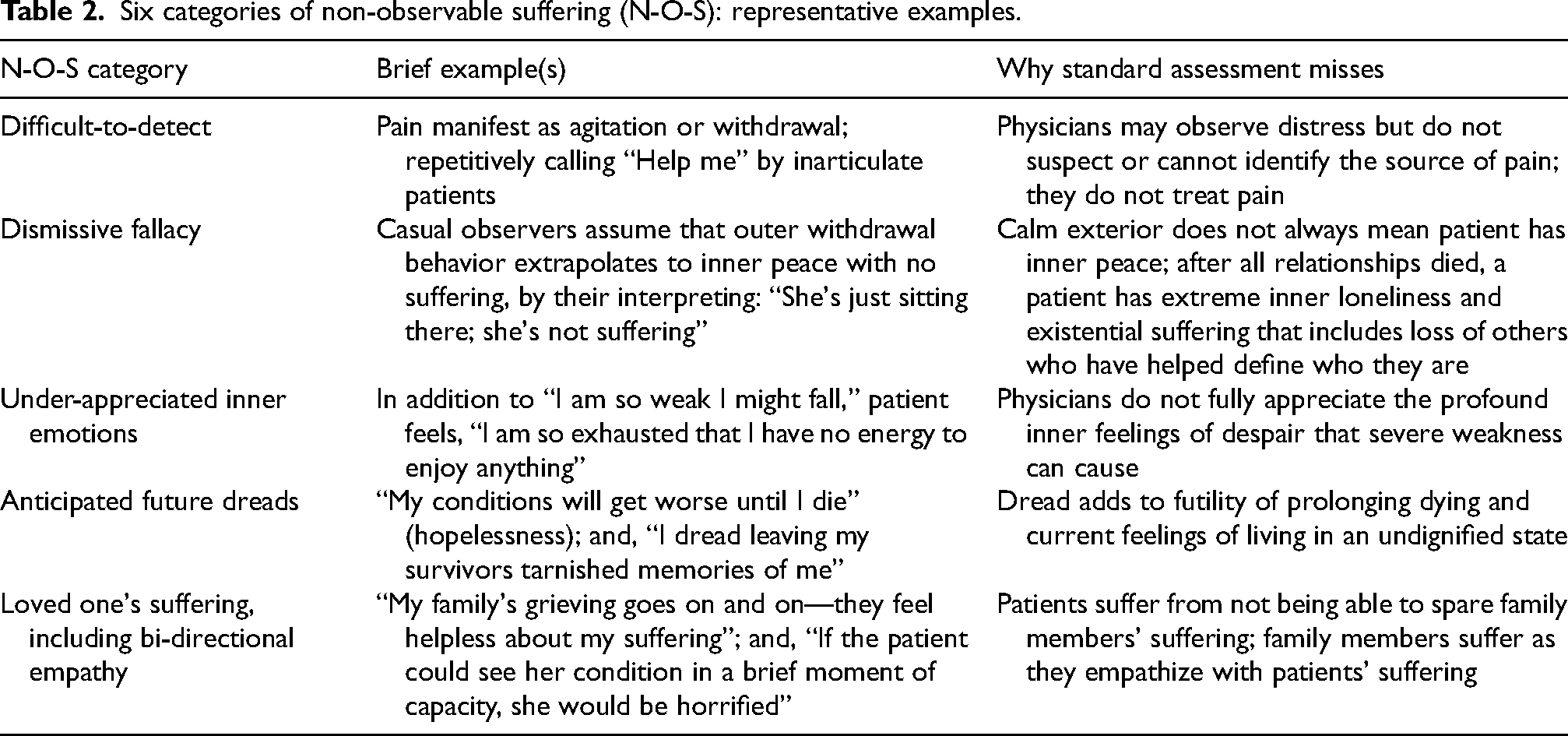
Six types of non-observable suffering (N-O-S) in late-stage dementia
In Table 2, “N-O-S” means “Non-Observable Suffering.” Like S-O-S that signals urgent need for rescue, “N-O-S” signals urgent need for suffering relief—even if not visible by standard assessment. Awareness of N-O-S could improve reducing suffering of inarticulate patients.
Six categories of non-observable suffering (N-O-S): representative examples.
“Success”: a behavioral definition for advance care planning
ACP can be considered successful if, after patients reach their previously judged “qualifying condition(s),” their treating physicians promptly write and implement orders for treatment that, in patients’ opinion, delivers goal-concordant end-of-life care.
During ACP, planning principals are responsible for judging suffering that 36 conditions would cause them or their loved ones—based on their lifelong values and current treatment preferences. Example: “If I reach a condition where I cannot interact with other human beings, even at my own birthday party, then I want either Natural Dying or Moderate Anesthesia—depending on whether I can still eat and drink without help.”
Four clinical cases: making end-of-life decisions based on suffering intensity
Note: Cases 1 and 2 are presented in the first person, since this author was the treating physician. Case 2 is presented in detail since it demonstrates how incapacitated patients’ agents can UPGRADE the options to include Moderate Anesthesia if not present in existing living wills.
Case 1, “BB”: Moderate Anesthesia for intolerable suffering
How BB became my patient
An end-of-life doula requested I evaluate an 85-year-old woman with Alzheimer's disease. It was urgent since her agitation recently escalated despite treatment with antidepressants and antipsychotics. One month earlier, she attempted to VSED but resumed drinking fluids and eating food (mostly chocolate). Timing was challenging: an extended holiday weekend was beginning. Also, neither the agent nor I could reach her designated hospice.
I entered BB's bedroom where stale air filled the dark room. As soon as I identified myself as a psychiatrist, she interrupted my introduction, bolted upright, and declared, “I wanted to die yesterday.” Her emaciated frame contrasted starkly with the wild energy of her movements. Her agent had warned me she might strike out, though she was too weak to leave her bed unassisted. I considered her agitation, aggression, and anger to be visible manifestations of profound inner torment from dementia, depression, and existential anxiety. Based on her current presentation and her agent's description of her recent behavior, I judged her dementia stage as moderately severe to advanced (CDR Stage 2 21 or FAST Stage 6 22 ). Given the crisis nature of her intolerable suffering from which she desperately wanted relief, I began titrating sedative medications, starting with a low dose. Meanwhile, I continued to try to contact her hospice.
Making the decision to implement MA
To assess BB's current treatment preferences, I selected 12 of 36 conditions from the patient decision aid I have been using since 2009. After reading the words aloud twice for each condition, I asked BB whether she would want to continue life-sustaining treatment if she were living in this condition. All her responses were “No”; she shouted half of them.
I routinely assess decision-making capacity (DMC) by asking patients to explain their reasoning for judging intensity of suffering for each condition. But BB could not, or would not, explain. Instead, she angrily asked, “Why are you asking me all these questions? I just want to die.” Absent demonstration of logical reasoning, I judged she lacked DMC to consent to treatment. Yet her passion and consistency in expressing her desire for relief from suffering led me to judge she had sufficient capacity to assent. (Consent requires demonstrating understanding and reasoning, while assent requires only agreement based on understanding the consequences of the decision.) Her legally authorized agent's substituted judgment was certain BB would want MA now.
BB met the clinical criteria for MA: (1) lacked capacity to decide on VSED; (2) preserved ability to eat and drink independently (that placed her in the Dementia Gap); (3) intolerable suffering; and (4) failure of non-sedating interventions to provide relief. I explained the two main risks of MA to which BB assented and her agent consented.
I completed a MA-POLST that focused on comfort care, added orders for slowly increasing the dose of sedative medications, and refused artificial nutrition and hydration. BB's agent and I signed the POLST, to make it legally valid. POLSTs are sets of portable, immediately actionable medical orders that the law in most states require other providers to honor 46 with only two, uncommon exceptions. 47
Initial sedation with moderate doses of oral clonazepam and quetiapine did not relieve her agitation. Increased doses provided sedation but diminished her consciousness. Comfort measures to address thirst and dryness were provided. The end-of-life doula used OTC agents to reduce thirst. She also coordinated friends’ visits. BB died peacefully after four days.
Three (not mutually exclusive) possible causes of death are: progression of severe malnutrition, electrolyte disturbances from medical dehydration, and cardiovascular effects from quetiapine—a known risk, though lower than that of similar antipsychotics. 48 The four-day timeline is consistent with sedatives not being the proximate cause of death.
Ethical considerations
BB's statement “I just want to die” presents an interpretive challenge. If it represents her literal desire to hasten her death, others could characterize my treatment as complicit in her wish for voluntary euthanasia. But I interpret this statement as BB's hyperbolic, desperate request for suffering relief. Her agent confirmed she was often prone to use dramatic language and I had just seen other instances. Terminally ill patients commonly voice wish-to-die statements that they retract if symptom management is effective. My goal was to use a moderate dose of sedation to calm her down and relieve her depression so she could resume enjoying chocolate and visiting with friends. Unfortunately, I could not find a “sweet spot” dose to accomplish this.
For “people at the margins of autonomy,” Peterson et al. suggest supportive, collaborative decision-making. 49 Peterson's goal remains “consent,” so patients are still responsible for making advance treatment decisions. In contrast, my work with BB invited supportive collaboration with her agent to allow BB to voice her end-of-life wishes as fully as she could; but ultimately relied on her agent to legally consent to MA on her behalf based on the accepted practice of substituted judgment that in turn requires knowing her end-of-life wishes well based on discussions before she lost DMC.
Moral considerations
The primary moral justification relies on the Rule of Double Effect. I followed Sulmasy's (“reinvented”) protocol. 50 My intent was solely to relieve BB's intolerable suffering through proportionate, gradual increase of sedative medications. When initial moderate doses failed to control her symptoms, I administered higher doses, which caused sedation. While I foresaw the potential for unconsciousness and earlier death, I did not intend these consequences. The action of prescribing quetiapine could be considered morally good or at least neutral: its aim was to treat BB's agitation by targeting its underlying psychiatric sources. I did not use the bad side effect of death as the means to relieve suffering. I transparently documented the decision-making process and subsequent clinical course. I alone bear moral responsibility for her treatment.
BB's condition also fulfilled the Principle of Proportionality. 51 Dementia had rendered BB's consciousness almost entirely negative in the shadow of intolerable suffering, making relief through unconsciousness proportionally beneficial compared to the harm of continued awareness of suffering.
Moral summary
The Rule of Double Effect and the Principle of Proportionality morally justified the decision to implement MA. I acknowledge the inherent limitation when a treating physician evaluates the morality of his own clinical behavior. Transparent reporting may help but cannot solve this obstacle. I invite others to retrospectively review and judge my actions. Comment: Hypothetically, had BB's suffering not required such urgent relief, I would have requested a second clinical opinion from a hospice medical director or ethics committee member before starting sedation, especially since BB had not previously consented to sedation as a treatment of last resort.
Clinically effective, moral end-of-life decision making for patient “AK” (below) differed from BB's case in three ways: First, AK had completed a dementia-specific living will, though it did not include MA. Second, I polled the substituted judgments of her Patient Decision Committee (PDC) members rather than relying solely on a single proxy. Third, her husband and I had a well-considered reason to proceed without engaging hospice, which the Discussion section explains.
Case 2, “AK”: Polling AK's PDC members to decide on MA. Establishing moral justification when the Rule of Double Effect could not apply. Understanding the source of her husband's unexpectedly profound grief
As I entered her home, AK was gracefully poised on a tufted leather couch. Her physical presence had changed little in the five years since I helped her complete ACP. As I approached, she made eye contact and smiled, but with no hint of recognition. She fluidly rose and extended her hand. Yet each time I tried to let go, she held on and shook again. After five shakes, I exerted enough effort to withdraw my hand.
Her husband's exhausted eyes were surrounded by deep creases, not surprising as he reported fourteen hours of daily vigilant caregiving. When I remarked on how well AK appeared, he shared that she still walked four miles a day. In other circumstances, this fact would be celebrated as a sign of vitality. But here, it starkly warned that physical longevity could prolong her existence with prolonged and devastating loss of cognition and suffering.
AK's first signs of dementia appeared seven years earlier. Her deterioration accelerated in the past year. Her husband requested my reevaluation for two reasons. First, their three children and several close friends spontaneously shared that AK would not want to prolong her dying in her current mental state due to loss of dignity and imposing burdens on others. Second, authorities at two recently visited memory units refused to implement Natural Dying if she became dependent on assisted feeding in the future. While they admitted this option was legal, they refused to allow it on their watch.
Non-sedating treatments, including antidepressants and antipsychotics, provided little relief from emotional lability that sometimes manifested as combativeness toward caregivers. Several weeks ago, she eloped: She managed to sneak out of their home, find the keys hidden in their truck, and take a “joy drive.” —Shocking, amazing, but dangerous. A repeat performance might cause serious harm to herself and others.
AK's memory deficit was so profound that she could not state her lifelong career had been nursing. Her once-precise medical vocabulary and passionate political discussions had deteriorated into strings of words lacking logical connection or meaning (word salad). While she could still grab a sandwich from across a table, she remained silent unless someone talked to her. Then, her verbal responses were incoherent; she could not engage in responsive, relevant, meaningful conversation. She rarely recognized anyone except perhaps her husband on occasion, although she was usually calmer if sitting next to him. She was in CDR-3 21 and FAST Stage 7. 22
During their visit to two memory care units, AK became agitated—an unusual response for her. Her husband heeded the advice of her experienced caregiver: AK would not tolerate institutional care well. She would need to give up the comfort and personal attention of home to live among strangers. Yet her elopements demanded vigilance: she was no longer safe at home.
Prior advance care planning: the framework for making a current decision
Five years earlier, in early-stage dementia, AK had sufficient DMC to complete ACP and she judged 17 of 36 conditions would cause her loved ones or herself severe suffering, based on her lifelong values and treatment preferences. The video interview that memorialized her decisions was now invaluable to understand her current suffering assessments. The ACP protocol had translated her judgments into “Future POLSTs” that required consistency between her past living will. AK had established a PDC consisting of her agent and alternates: her husband and three children. Recently, all members agreed to add her caregiver.
The Dementia Gap problem
AK's case revealed a gap in my current clinical experience. Patients who can still eat and drink independently have no legal path to withdraw/withhold food and fluid unless they are at risk for aspiration. Otherwise, withdrawal constitutes illegal euthanasia. AK swallowed normally.
AK qualified for Natural Dying based on her irreversible severe suffering, but her current POLST remained Selective/Limited Treatment since she could eat and drink independently. She was living in the Dementia Gap.
Why was AK not offered the option, Moderate Anesthesia, during ACP
Five years earlier, the ACP protocol did not include MA. AK's video interview only showed 17 conditions she judged would cause severe suffering. Yet she consistently prioritized reducing suffering over prolonging life, in keeping with AMA Ethics Opinion 2.20. 29
AK had been courageously autonomous. After I shared AMA's definition of existential suffering as “death anxiety, isolation, or loss of control,” and AMA's advice against treating with sedation, 52 AK still insisted on receiving sedation if non-pharmacological treatment failed. She also spontaneously expressed the preference of dying earlier rather than later, if decision-makers were uncertain. Finally, she placed not burdening her husband and others at the highest priority.
Using patient decision committee members’ substituted judgment
I polled members of her PDC after explaining the process of substituted judgment decision-making: Their task was to answer, “From your knowledge of AK's life values and treatment preferences, has she now reached any condition that she previously judged would cause intolerable suffering—if this option had been offered during ACP?”
Reasons to expedite polling
Although AK's suffering had not yet reached the threshold of urgency, relief was warranted for several converging reasons. A repeat elopement risked serious harm to herself and others. Her husband recognized that his current authority to implement her end-of-life wishes could be abruptly curtailed, by further dementia progression requiring placement in a memory unit, or by a fall and fracture necessitating hospitalization. In either setting, institutional authorities might refuse to honor her living will, as had the two memory units he had already visited.
The Discussion section addresses the often-overlooked risk, “to delay is to deny”: institutional placement and home hospice engagement that leads to conflict can prevent prompt relief from suffering as effectively as outright refusal. Three risks—elopement, institutional placement, and living will override—informed my decision (with which AK's husband agreed) to seek two independent clinical opinions before proceeding to MA, but not to enroll AK in hospice.
Polling PDC members: do AK's current conditions qualify her for MA?
PDC members’ polling resulted in unanimous agreement: 6 current conditions were causing intolerable suffering and thus qualified her for MA, as shown in Table 3 and Figures 2–7.

Loss of ability to recognize close relatives and friends.

Depends on others to change diapers due to fecal incontinence.
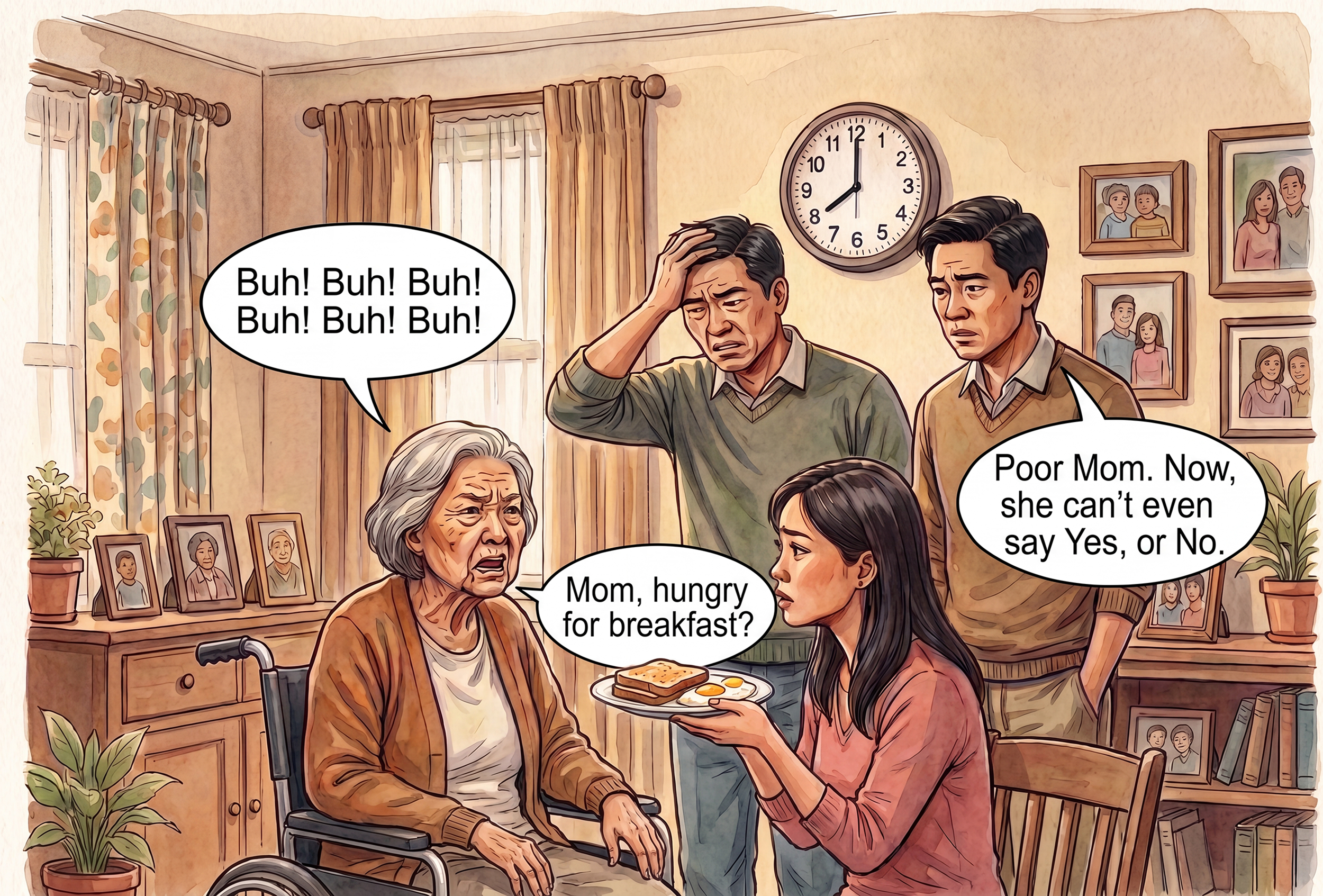
Cannot communicate—even to say “Yes” or “No”.
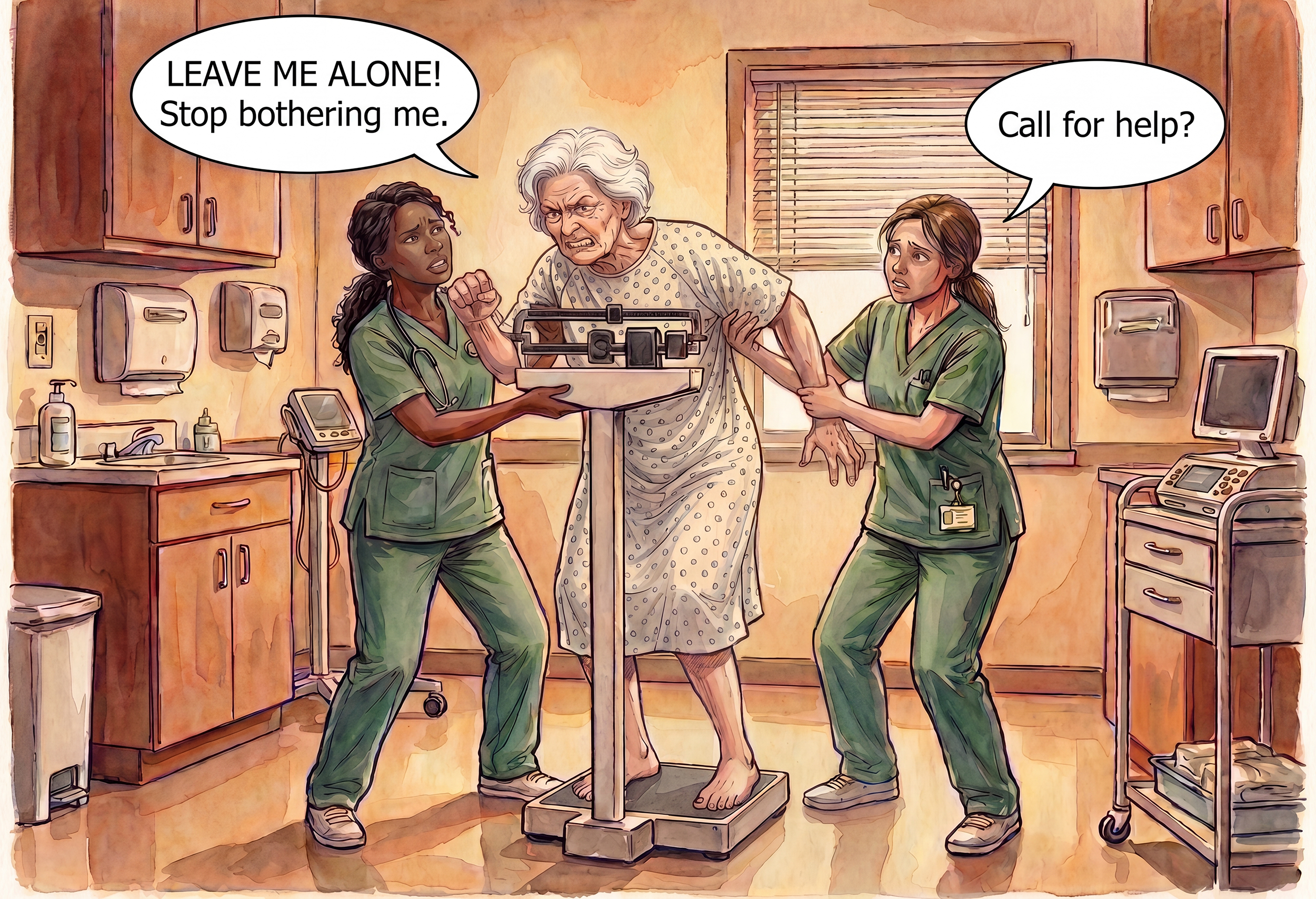
Fighting caregivers.
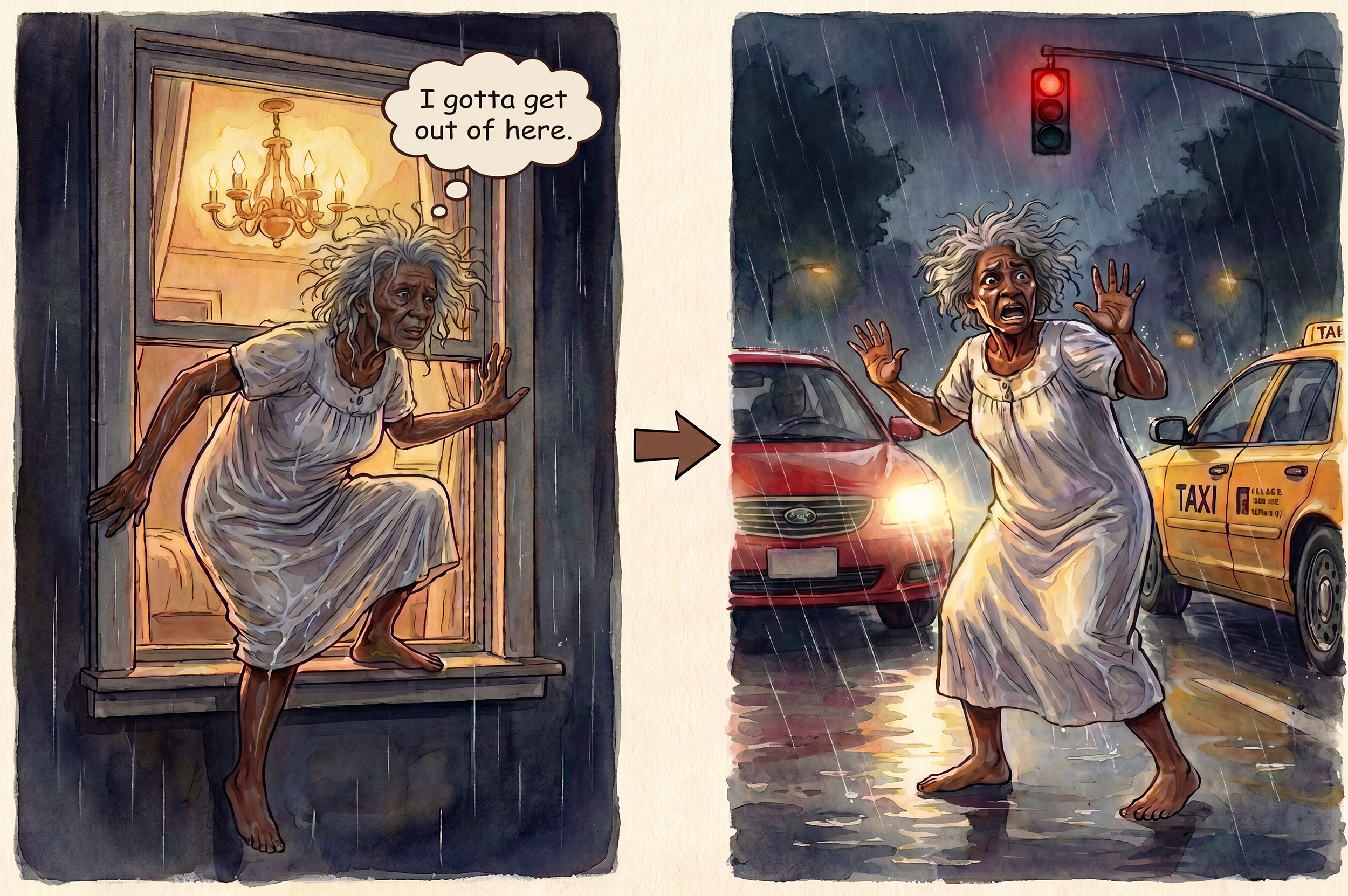
Elopement risk.
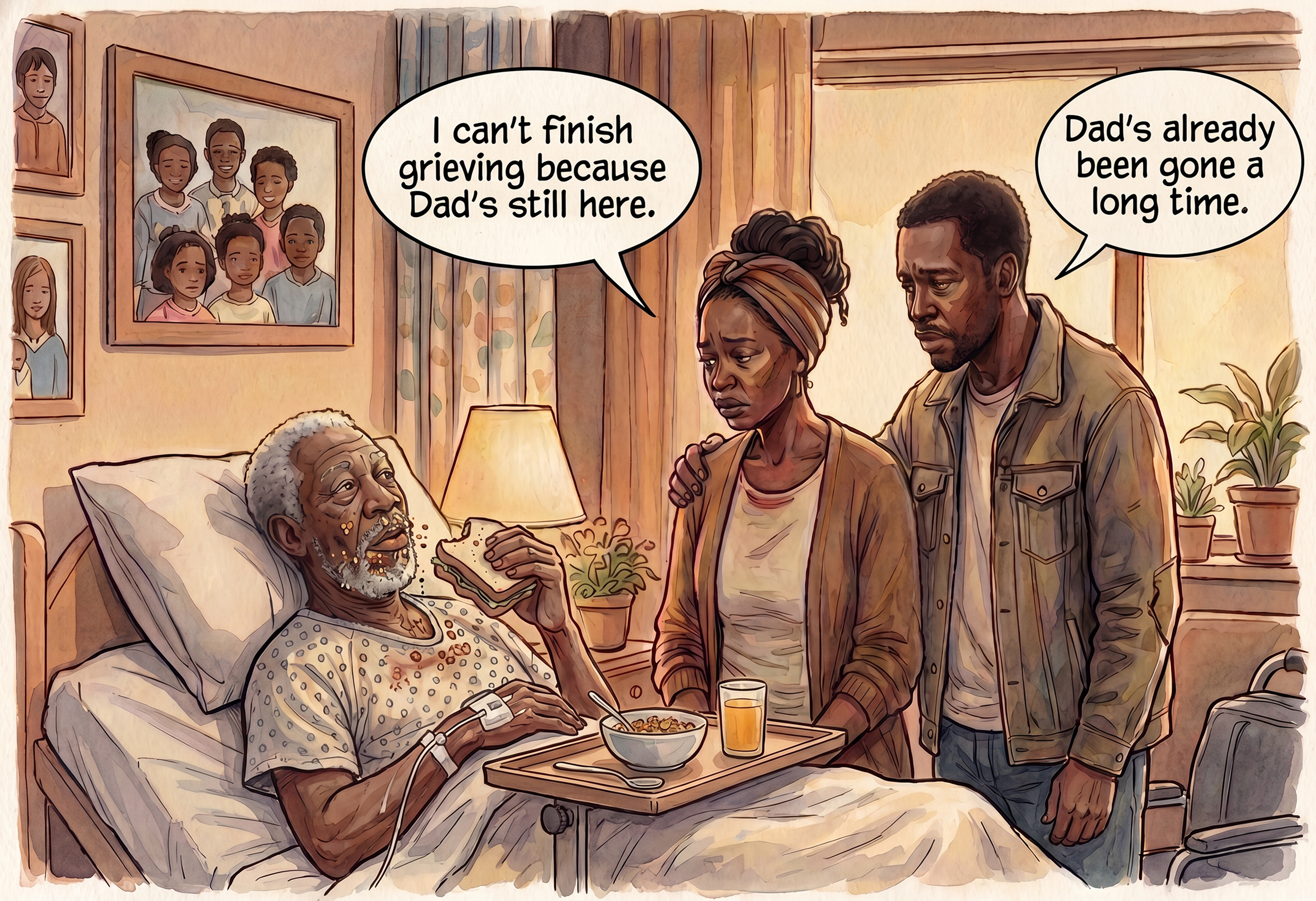
Loved ones’ suffering includes “ambiguous loss” for patients who can self-feed and self-drink—who are living in the Dementia Gap.
Polling patient decision committee members’ substituted judgment for conditions AK would have judged are currently causing her intolerable suffering.
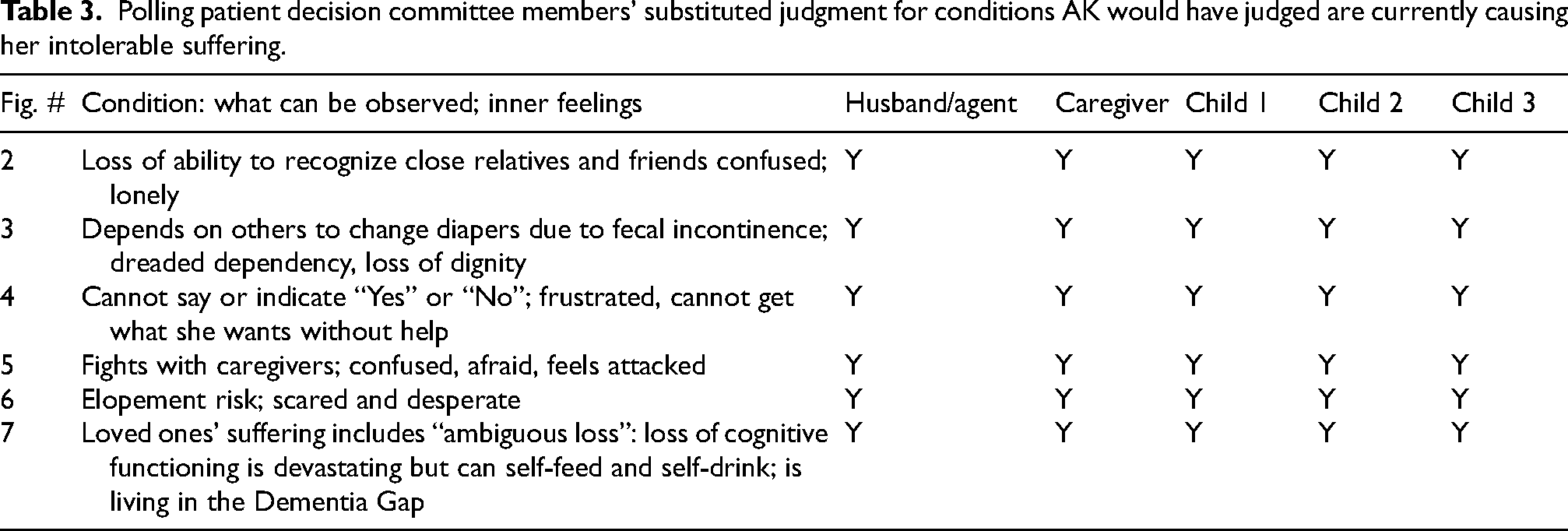
Comments: Figure 1, readers will recall, shows the Dementia Gap. Each condition was presented with verbal descriptions written at grade-three level reading comprehension. While AK and members of her PDC were originally shown black and white line drawings, this article presents the 2026 color upgrades.
These illustrations demonstrate how high-resolution color images help planning principals express, and PDC members and physicians understand and appreciate, the intensity of suffering that conditions cause: (A) facial expressions that convey recognizable emotions with immediacy, and (B) thought bubbles containing words that reveal the inner experiences of patients and others affected. Together, these elements enable those concerned to identify sources of N-O-S.
Criteria are stricter for Moderate Anesthesia than for Natural Dying
As a treatment of last resort, MA is more controversial than ND. Therefore, to implement MA for AK, these stricter criteria were used:
Suffering must be judged “intolerable” (rather than severe) Two conditions must currently be met (rather than one, if patient prefers safety) Polling result of substituted judgments must be unanimous (rather than “all but one”) The consent form states: “You will most likely die earlier with Moderate Anesthesia if you also refuse artificial nutrition and hydration” (not applicable for Natural Dying)
Table 3 presents the polling of substituted judgment among PDC members that was considered when decision to implement MA.
Clinical course of Moderate Anesthesia
Since members of AK's PDC confirmed their unanimous substituted judgment that AK met the clinical qualifications of six conditions of late-stage dementia, with which I agreed, I completed her MA-POLST. First, I engaged her agent/husband in a POLST Conversation. I signed the form after he signed on her behalf to give consent, thereby making its orders legally valid and immediately actionable.
Treatment began with oral disintegrating clonazepam tablets and oral, slow-release quetiapine. Telehealth technology permitted me to assess AK several times a day. The end-of-life doula provided on-site, 24-hour, on-call care. At my request, she positioned her phone at varying distances from AK: a few inches from her face to hear her breath sounds; a couple of feet away to observe her facial expression; and further back to view her whole-body responses. Her husband validated AK's signs of increased suffering, such as furrowed brows and restless limbs.
The goal of sedation was to dissociate her mind from suffering and prevent further suffering, not to cause her death. Previously, she was confused, sometimes fighting, and a dangerous elopement risk. Now she was comfortable, calm, and safe in her own bed.
By the third day, administering medications orally risked aspiration due to swallowing difficulty. Phenobarbital was administered rectally. AK showed no signs of distress until what turned out to be her last day of life when I treated her air hunger with sublingual morphine drops. Fentanyl patches were available but not needed. Eight days after beginning MA, AK died peacefully.
Justifying MA as moral when the Rule of Double Effect could not apply
The Rule of Double Effect cannot justify my treatment of AK since her loss of consciousness was not “a possible foreseen effect;” it was the intended therapeutic goal, to deliberately depress her consciousness to dissociate her mind from current and future suffering.
My treatment attempted to follow Sulmasy's protocol of parsimonious/proportionate direct sedation. 53 AK's conscious mind no longer could access what Sulmasy calls “the goods of consciousness.” 10 Her consciousness could not “exercise freedom and moral agency, [] grasp the finite and the infinite, [] reason, appreciate humor and morality, assist other human beings,” or “pray, [exercise] moral choice, speculative thought, or [enjoy] aesthetic experiences”—yet her consciousness could experience suffering.
Loss of consciousness still incurred costs, such as loss of AK's kind, gentle, and loving personality when it emerged. Yet based on her ACP decisions and PDC members’ substituted judgment, she would now choose unconsciousness for relief from suffering over consciousness with her suffering and its burdens on others. Her treatment currently fulfilled the Principle of Proportionality. Also, all agreed that her prognosis was grim.
Moral justification of MA regarding possible earlier dying
I next summarize my interpretation of Sulmasy's moral framework. (Comment: his nuanced philosophical position warrants further reading.) In Parsimonious Direct Sedation, there is a chain of effects: “administering the sedative causes loss of consciousness, which in turn may be a contributing cause of the patient's death … [but the physician's] intention … is satisfied when the patient is unconscious and symptom-free.” 10 Sedation fulfills the physician's intention to reduce suffering—but it may also unintentionally initiate a cascade of events leading to death. What leads to death is this: the craft of medicine reached its limits in the progression of the patient's terminal illness. Appreciating this point fulfills the Canon of Discretion.
Justifying the decision to withhold artificial nutrition and hydration (ANH)
Withholding ANH is consistent with the four principles of medical ethics
30
:
Explaining AK's husband experience of unexpectedly profound grief
After AK's death, her husband's grief was more intense than either he or I anticipated. In retrospect, I neither warned him about this possibility nor suggested he begin anticipatory grief work. I frankly admitted to him that I had not previously encountered this phenomenon. Typically, relatives experience anticipatory grief by watching patients deteriorate physically. But AK experienced vast diminishment in cognitive functioning while retaining her physical ability to self-feed/drink. Pauline Boss (among others) calls this “ambiguous loss,” 54 so what follows death can be termed, “ambiguous grief.”
To explain this phenomenon, Figure 7 illustrates two views that different relatives may hold. Suffering could be worse when one person oscillates between both views that cause a sustained internal conflict. AK's husband felt connected when they ate out after her caregiver groomed her—except when her vacant responses reflected her diminished cognitive functioning. He struggled with her deterioration when changing her diapers.
AK's husband strived to find meaning in his remaining connection with AK. During their evenings, he seated her next to him as they listened to music or viewed movies. When he took her to restaurants, she was usually silent; if a waitress asked her a question, he answered for her, thereby masking her severe cognitive impairment, even to himself, which permitted his partial denial. He could still feel he was with the woman he married 40 years ago since it was partially true. While he appropriately complained about the physical toll of caregiving, it also provided him purpose and meaning. No one expressed this better than St Francis of Assisi: “It is in giving that we receive.” 55 Her husband did not fully appreciate this positive aspect of caregiving until AK no longer needed his caregiving. Then, lack of life-purpose added to his loneliness and grief.
Few resources on ambiguous loss exist for lay people. One is an Alzheimer Society of Canada's booklet that recommends group therapy. 56 There, relatives can share similar experiences, give and receive emotional support, and may feel less alone.
Relevance of dying patients’ method of eating
For patients who required months of assisted oral feeding, survivors do not usually deeply mourn the ending of this burdensome task. If patients become emaciated due to physiological inability to absorb food, the trajectory of physical wasting prepares relatives emotionally for an attitude as survivors share, “Death provided her welcome peace,” or, “She's in a better place.”
In contrast, dining can remain a meaningful social activity for PINEs if they eat independently, which in turn creates a cruel irony: the more joy caregiving spouses experience sharing meals with their loved one, the more intense their grief will be after such pleasure is gone. This factor was likely significant in causing AK's husband's profound mourning.
Other factors mitigated his grief. They included AK's statements during ACP and PDC members’ recent unanimous agreement. Both reduced remaining ambivalence about timing, when to initiate sedation, which was his responsibility. At AK's celebration of life ceremony a few months later, several family members and close friends independently opined the husband had waited too long.
Regarding when to implement MA, AK's husband did not view his role as participating in a process that led to her dying. Instead, he viewed the goal of MA treatment as reducing her suffering. Having fully accepted her dying as inevitable, he fulfilled his role for which he explicitly promised in their bilateral durable power of attorney for healthcare decisions: he promised to advocate for her wishes to mitigate her suffering before she died. He honored AK's wishes.
Sometimes he wondered if he would have felt better for a while had he delayed MA to enjoy her limited being longer. But he never questioned whether his timing differed from what AK would have preferred for herself.
AK's transition illustrates dying can sometimes be dramatically abrupt and other times insidiously slow. AK's change in physical activity was abrupt: one day she walked four miles; the next, she was too sleepy to get out of bed. But her change in communication was incremental: one day her verbal output was a meaningless word salad; the next, no meaning was possible since she was asleep.
* * *
To provide ethical contrast, consider two terminal cancer patients. Unlike BB and AK, they possessed DMC and made their own decision about when to die. Neither lived nor died in isolation: they were aware of professional influence and their relatives’ love.
Case 3, Terry Matthews: Rapid induction of deep sedation to unconsciousness for intolerable pain caused by advanced cancer
Terry Matthews was a 31-year-old wife and mother who died of advanced cancer more than a quarter-century ago. Her treating physician, Ira Byock, published her sad story in his 1997 book. 57 Today, it still inspires ethical and moral debates.
Terry's fight with cancer began six years before her death. After initial therapeutic success, she believed (hoped) she was cured and adopted a child. Sadly, her cancer recurred. Toward her end, despite increasing pain, she refused to accept that dying was inevitable, let alone imminent. Instead, she tenaciously held onto life through her relationships with her husband and children. The price she paid became unbearable pain, which Byock noted was the worst he had seen in his then-fifteen years of providing palliative care.
Terry's oncologist bluntly confronted her by predicting she would die within three weeks. This was likely his attempt to motivate her to accept her grim prognosis so she would consider available treatments of last resort to relieve end-of-life suffering. But Terry took no action until she characterized her pain as “paralytic” and a “crisis” that caused her to shriek, “I feel like I’m on fire.” After she extraordinarily depleted local pharmacies’ supplies of IV Dilaudid and found 900 mg per hour of morphine ineffective to provide relief, Terry finally admitted to Byock that her pain had become unbearable. About that time, Terry's oncologist called Byock to suggest implementing a treatment of last resort that a group of local physicians had thoroughly discussed but used only once: administer the rapidly acting anesthetic thiopental IV to eliminate Terry's conscious awareness of pain.
How Byock obtained Terry's consent. Her clinical treatment and outcome.
“Will I wake up sometimes and be in pain?”
“Not if you don’t want to.”
“I just want to go to Heaven. Please make it [the pain] go away.”
“I promise.”
Byock then called in the prescription. {Page 209}
Byock recounted, “The seventy minutes it took for the medicine to arrive and to be set up felt like seven years … The sedative took just minutes to work.” {Pages 209–210.} Soon after sedation began, Terry's family experienced a sense of peace for the first time in weeks. “She slept for 30 hours” and “never regained consciousness” before she died. {Page 212}.
Retrospective analysis and implications for end-of-life dementia care
Had the treatment plan for a potential crescendo of suffering been discussed earlier in her care, Terry might have been spared several days of unbearable agony. She could have given consent in two stages: first, what treatment she would agree to, and second, when to implement it—once suffering became unbearable. Calm deliberation usually results in better decisions than responses given during a crisis.
Why did earlier advance discussion and consent not occur? Two reasons. First, the patient's own denial or reluctance. Second, Byock's attitude, about which he provided this hint: “The idea of sedation is controversial when caring for the dying, because some people believe it is tantamount to euthanasia” {Page 207–208}, and “What may appear philosophically to be a fine line is, in practice, a chasm” {Page 216}.
If concern about distinguishing palliative sedation from euthanasia delayed Byock's discussing a treatment that Terry might have needed earlier, then—however important it is to consider this philosophical concern—the delay did not serve Terry well.
Must suffering become unbearable before physicians discuss sedation?
Terry's care raises a critical question: Could delaying a critically important end-of-life discussion have led to crisis-driven consent after she was in agony? Here is a similar question for dementia patients who lose capacity years before they need sedation: Could delaying discussion eliminate the opportunity for informed consent due to loss of DMC? For both, advance care planning should discuss the option of sedation for patients who want to avoid prolonged, intolerable suffering.
Distinguishing Moderate Anesthesia from euthanasia
Orentlicher used the term “slow euthanasia” in 1997 to criticize the U.S. Supreme Court for rejecting physician-assisted suicide while embracing terminal sedation. 58 The shorter the time between sedation and death, the easier it is to argue sedation was the proximate cause of death.
Byock's intentional rendering of Terry unconscious to eliminate her awareness of unbearable pain followed an established ethical protocol and was clinically appropriate, compassionate, and consistent with Gilbertson et al.'s opinion, “Dying patients should not be left to suffer.” 34
Yet critics could argue Byock violated the Rule of Double Effect based on stating he used the bad effect (hastening death) as the means to achieve the good effect (relieving suffering). 50 Critics can also note that 30 hours is short enough to blame thiopental infusion as the proximate cause of death. Yet this question could be posed to Byock's critics: “Do your living wills explicitly reject rapid induction of deep unconsciousness if you face unbearable pain for which urgent treatment would be the humanitarian, compassionate response?”
Physicians resist intentional sedation to unconsciousness more than proportionate palliative sedation where unconsciousness is an unintended side effect. 18 Yet the public accepts intentional sedation when suffering is unbearable. 59 Research needs to focus on dementia so bioethical debates do not delay treatment for suffering patients.
Case 4, Brittany Maynard: Her decision on timing Medical Aid in Dying
After months of headaches, newlywed Brittany Maynard received a diagnosis of incurable glioblastoma. Adamant about dying on her own terms, she relocated her family from California to Oregon—then one of three states where “Death With Dignity” was legal. She ultimately ingested a lethal dose of physician-prescribed medications. She died shortly before her thirtieth birthday.
Brittany became a volunteer advocate with Compassion & Choices, the largest right-to-die organization in the U.S. With their support, she created a goodbye video 60 that 12 million people viewed. It stated Oregon's law required “unbearable suffering.” Yet Brittany admitted, “I still laugh and smile and enjoy walks,” which her video demonstrated.
Brittany's main worry was waiting too long to die: “If I wait too long, my autonomy may be taken away from me.” This concern parallels the Dementia Fear. Her suffering was mostly anticipatory: fear of developing morphine-resistant pain, personality changes, verbal, cognitive and motor loss, and intractable seizures. None of these conditions had yet occurred, but they do afflict some glioblastoma patients. Even so, they might have been treatable for several months.
Brittany ended her life while she still enjoyed living. Her dying was reported to be peaceful with full support from her husband and mother. They continued to advocate to legalize Medical Aid in Dying.
Brittany thus prioritized preserving her autonomy over maximizing her time to enjoy living
Critical distinctions between MAiD and Moderate Anesthesia
Brittany's case illuminates why patients living with advanced dementia cannot use Medical Aid in Dying, and require alternative approaches like Moderate Anesthesia for suffering relief. Few dementia patients can meet all four MAiD requirements:
(1) Decision-making capacity to request a prescription evaluated by two physicians (2) Prognosis of living less than six months (in the United States) (3) Ability to determine the timing of ingestion (after receiving the lethal dose of medications) (4) Physical and cognitive ability to self-administer the medication (after receiving medications)
Patients who fail to meet even one requirement cannot qualify for MAiD—but they may still qualify for PSU if their suffering is intolerable.
* * *
Cases 5 and 6 demonstrate an important moral lesson: The extra clinical effort to thoroughly investigate patients’ historical interests and to apply skillful interviewing techniques can “awaken” some withdrawn patients so they can enjoy life.
The dismissive “She's not suffering; she's just sitting there” fallacy can lead to two opposite tragic errors. One is abandoning suffering patients for the rest of their lives. The other is premature implementation of a treatment of last resort that thereby sacrifices some of their remaining time to enjoy living. Both outcomes violate physicians’ moral duty to honor the lives of vulnerable patients.
Case 5, Gladys Wilson: Skillful, compassionate human connection awakened her human and spiritual passion
Gladys Wilson, an 87-year-old institutionalized PINE had not spoken in six months. She exhibited repetitive behavior—hitting the arm of her chair—apparently without purpose. Then, Naomi Feil interviewed her using Validation Therapy, the therapeutic approach Feil founded. 62
Feil began the six-minute video excerpt of their interview with a clinical, educational statement: “When no one enters their world and they are just sitting there, they will withdraw inward more and more, and their desperate need for human connection is all inside.”
63
Technically, Feil combined empathetic listening, sustained and intense eye contact, and therapeutic touch. She cupped Gladys’ head in her hands and sang hymns that she knew would be familiar to Gladys, given her strong religious background.
First, Gladys shed one small tear. Then she changed her repetitive banging behavior to match Feil's speaking volume and tempo that reflected her changing mood, sometimes calm, other times passionate (as Feil changed). At one point, Gladys stopped banging and reached over to touch Feil's shoulder—an action consistent with appreciating Feil's contact. As Feil sang the next hymn, Gladys broke her long silence—first in whispers, as expected for someone who had rarely vocalized—and then more loudly. When Feil asked: “Do you feel safe with Jesus?” and, “Do you feel safe with me?” Gladys answered “Yes” to both, with conviction.
A speculation about Gladys's repetitive arm banging: While several neurological etiologies are possible, it might have been her only available means to communicate feeling ignored, lonely, and desperate for human contact. If arm banging signaled such distress, dismissing it as meaningless, as part of the “just sitting there” fallacy, profoundly dishonors her and deeply increases her suffering.
Some of Gladys's previous casual observers might be astonished if they viewed this video since Feil's skilled intervention demonstrated Gladys's ability to connect personally and spiritually.
Three haunting questions remain:
Was the intensity of Gladys's suffering during her silent months proportional to her passion when Feil made contact? How many other withdrawn patients sit in institutions while others dismiss their existential suffering simply because no one has dedicated the skill and time needed to transcend their apparent detachment? Will institutions provide staff training and sufficient time to apply new interviewing skills with patients so that some can someday be referred to as “formerly withdrawn”?
Case 6, Henry Dryer: Awakening his hidden passion by personal investigation
Casual observers dismissed the withdrawn behavior of 94-year-old nursing home resident Henry Dryer as typical for patients living with dementia. For endless hours, he remained slumped over in his chair, head down, hands clasped. Some described him as “disconnected from his environment.” They were proven wrong when a recreational therapist discovered, through research and experimentation, that Henry responded to jazz music of his era. 64
When headphones playing jazz were placed over his ears, Henry had a dramatic awakening. He played jazz drums on dishes with silverware as he moved his body to the rhythm of the music. And for those willing to listen, he clearly, coherently, and meaningfully expressed how important jazz was to him. Example: “The Lord came to me and made me holy, giving me these sounds.” 65
The passion that music evoked in Henry 65 was memorialized in the aptly named documentary, “Alive Inside.” 64 The intensity of his response invites this question: Was the intensity of Henry's suffering during his months of silence proportionate to the passion that music now awakened? If so, how many other patients sit in institutions while others dismiss their withdrawal simply because no one has dedicated the skills and time to discover areas of special interest that might awaken them?
The cases of Gladys and Henry inspire hope that professionals and family members will not make dismissive assumptions about patients “just sitting there,” but instead will try to discover their passion and awaken their capacity to engage. As the database of successful awakenings increases, it may become easier to motivate clinicians to increase their therapeutic efforts and to inspire an educational movement grounded in this universally accepted principle: Every patient deserves treating clinicians and caregivers who recognize their unique humanity, who seek to understand their individual needs, and who work diligently to connect with them—especially when patients no longer can advocate for themselves.
Before implementing a treatment of last resort, follow the proposed Hidden Suffering Detection Protocol
Designed to enhance the principle—never implement a treatment of last resort for patients who can still enjoy life—here is an initial draft of the four-step Hidden Suffering Detection Protocol:
Review with agents and family members, the consents patients sign during ACP. The strategic ACP protocol now includes MA for (A) intolerable suffering refractory to less-sedating treatments; and (B) for severe suffering of patients who can still independently eat and drink. Teaching all concerned about the “just sitting there” fallacy can prepare them to react appropriately if future professionals invoke it. Poll PDC members before implementing treatments of last resort. ACP counselors can engage PDC members in a group meeting whose purposes are to discover patients’ past interests and preferred ways to make physical and emotional contact that can include spiritual practices, music, other media, and movement. Investigate hidden suffering. PDC members can brainstorm possible sources of N-O-S for which treatment trials are reasonable. If such efforts fail: Start low-dose sedation. Begin with low doses of sedation and increase slowly—proportionate to their suffering—to allow time for suffering relief while preserving consciousness. Increase the dose of medications to attain unconsciousness only if necessary to reduce patients’ suffering.
Summary
Educational programs for healthcare professionals must emphasize this principle: sedating patients to unconsciousness—if they can still enjoy meaningful living based on their current values—could be considered clinically wrong, illegal, unethical, and immoral.
Discussion
Discovering the Dementia Gap—a huge, hidden humanitarian crisis; and appreciating the magnitude of non-observable suffering (N-O-S)
This article is likely the first to describe a newly defined substage of dementia, which it refers to as the “Dementia Gap,” and which is characterized by four clinical criteria: Patients have (1) reached late-stage Alzheimer's disease or related dementia (which implies they have lost decision-making capacity); (2) retained their ability to eat and drink independently; (3) experienced intolerable suffering from combined observable and non-observable sources; and (4) failed or would likely fail to respond to any non-sedating treatment.
After our 2022 critical review of the then-available “dementia-specific” advance directives, 66 continued monitoring of newly published living will offerings has, to date, yielded none that recognizes the existence of the Dementia Gap and its additional challenge to reduce patients’ suffering. If so, then defining the “Dementia Gap” is a truly new discovery.
In turn, this discovery provokes a three-fold educational event: first, the Dementia Gap exists; second, it affects an estimated 500,000 or more Americans; and third, a proposed treatment to relieve suffering is challenging since it must be both effective and morally justified.
Living wills that omit the Dementia Gap risk this dire result: All the diligent work planning patients invest in completing their living wills can fail; surprise and disappoint family; and leave patients ineffectively treated for as long as they remain in the Dementia Gap.
This Discussion strives to answer four crucial questions: Why has the Dementia Gap not been previously recognized? What treatment would be effective? Can it be morally justified? What other obstacles need to be overcome so the proposed treatment can be widely accepted and thereby reduce the suffering of these vulnerable, inarticulate, incapacitated patients?
Why has the “Dementia Gap” substage previously not been recognized?
The pool of patients who can sound the alarm of living in a therapeutic desert is small, even though the total number of Dementia Gap patients is large. First, they must manifest this clinical disparity: great loss of cognitive functioning but minimal loss of self-feeding and drinking abilities. Second, patients must endure suffering to desire a treatment of last resort sufficient to accept the two risks of sedation: permanent loss of communication ability and possible earlier dying. Third, their agents and family must be impacted by this stark discovery: their existing living will—despite being touted as “dementia-specific” by its drafters—cannot reduce patients’ suffering until the patient becomes dependent on assisted oral feeding and hydrating—a disease progression that might take months, even years.
Non-Observable Suffering: a greatly needed, enhanced clinical insight
Interest in this article's second clinical contribution, N-O-S, was inspired in part by a healthcare provider sharing (in 2015) the story 67 of a memory care unit patient who seemed to be “sitting there peacefully” but as all eventually learned, she was not just withdrawn; dementia had evidently destroyed her ability to speak and move. Hot coffee had been accidentally spilled in her lap, but she was unable to complain and did not writhe in pain. Yet the resulting second-degree burns required weeks of rehabilitation. She suffered untreated in silence for the first two post-burn days, until staff discovered the pathognomonic welts during routine continence care. In retrospect, when she most needed palliation, she received none.
In 2024, we broadened the concept of suffering in an article 4 whose Table 1 lists five general categories and examples of hard-to-observe or non-observable suffering: physical pain; psychic or emotional pain; existential suffering; disruption of life narrative, and burdening loved ones.
N-O-S is more frequently the source of severe to unbearable suffering than previously recognized. It hides in plain sight, masking itself as withdrawn behavior that clinicians and caregivers often mistake for calmness that some clinicians describe as: “She's not suffering; she's just sitting there.” Sometimes, N-O-S appears alongside observable suffering, but accounts for far more of the patient's total suffering than observable sources. Finally, N-O-S may exist entirely on its own, with nothing visible to betray its presence, such as living without jazz music, singing religious hymns, or enduring pain from second-degree hot coffee burns. To reduce how much and how long patients and family must endure suffering requires a living will that deliberately strives to identify these sources so they can be treated—otherwise, a huge population of patients will not be identified as needing treatment for their suffering. This article describes an illustrated patient decision aid (IPDA) designed to accomplish this goal.
The relationship between Dementia Gap and N-O-S: overlap and differences
In common, both are greatly underappreciated, and no existing living will, to my knowledge, includes ways to recognize, investigate, or treat the suffering each can cause.
They differ because the Dementia Gap is a duration of time that warrants recognition as a substage of late-stage dementia, based on patients fulfilling its clinical criteria. In contrast, N-O-S is a specific category of suffering that causes patients to endure severe, intolerable, or unbearable experiences that can be as intense as or greater than observable suffering, whether or not any observable suffering is present, but its source is either hidden or difficult to discover. Physicians do not treat what they cannot observe.
These two terms have some overlap. Both describe situations that rank among the most difficult to treat. The Dementia Gap thwarts the effectiveness of “dementia-specific” living wills that do not address patients who retain the ability to feed and hydrate themselves. N-O-S can occur at any stage of dementia, but its incidence increases as patients gradually lose more of their abilities to complain and manifest behavior consistent with the experience of pain or suffering, such as writhing or agitation. The greatest challenge emerges when their behavior becomes withdrawn.
The iceberg phenomenon
The extent of PINEs’ suffering in the Dementia Gap fits the epidemiological “iceberg phenomenon:” the observable burden represents only the tip. 68 The exact N-O-S to observable ratio is unknown. The studies quoted in Supplemental Material lead to a conservative estimate that more than 500,000 Americans currently live in the Dementia Gap with intolerable suffering. The number who experience severe but not intolerable suffering must be much greater. Applying my estimate of 12:1 global-to-U.S. ratio for all advanced dementias from several sources including Cavaco et al., 69 approximately 6 million patients worldwide live in the Dementia Gap. These numbers may double by 2060. 70 Thus, the scale of this crisis is huge.
Multiple lines of evidence validate the existence of Non-Observable Suffering
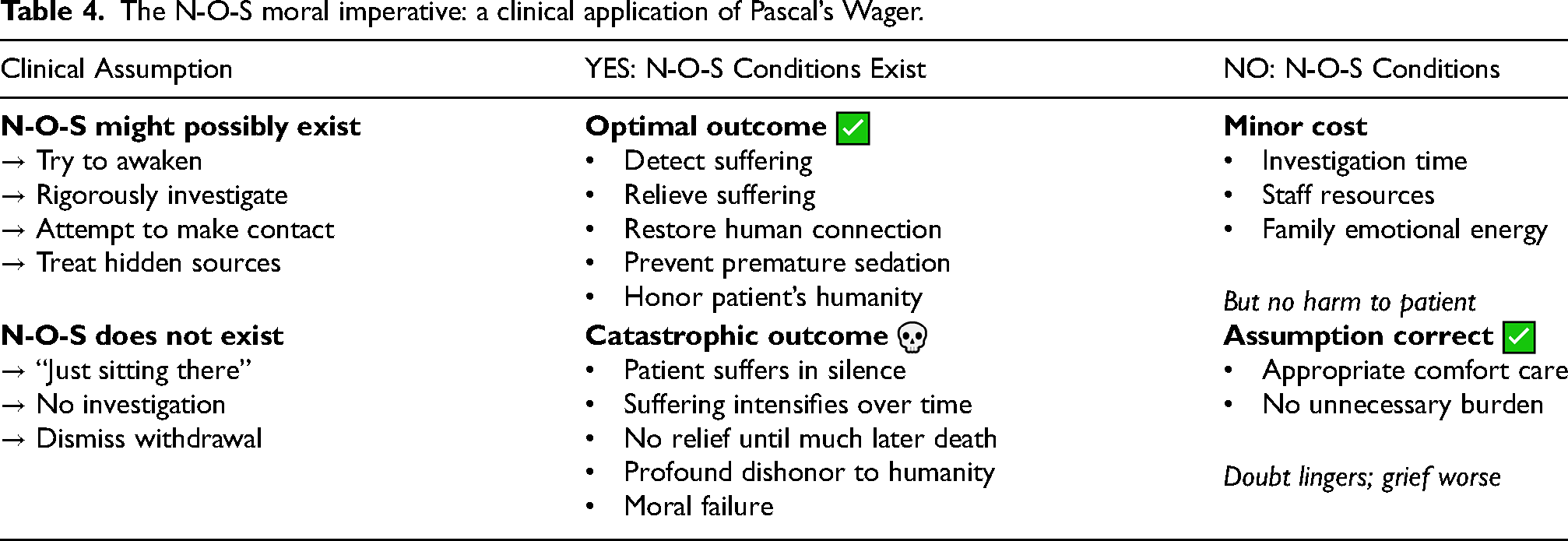
Pascal's logic depends on both outcome probabilities and magnitudes of what is at stake. Table 4 shows that if clinicians wrongly assume “She's not suffering” when N-O-S exists, the consequence can be catastrophic (like Hell): intolerable suffering for months to years until death. If clinicians assume N-O-S might exist andthey thoroughly investigate it but fail to “awaken” the patient, then the cost of failure—including time, money, and frustration—is modest (like being a good person living a good life who eventually learns Heaven does not exist). Pascal's logic applies to all inarticulate patients, including post-stroke, ALS, and locked-in syndrome patients.
The N-O-S moral imperative: a clinical application of Pascal’s Wager.
A history lesson: advocating for voiceless sufferers—the anti-vivisection movement
Research animals in vivisection experiments share four devastating characteristics with PINEs:
The anti-vivisection movement demonstrates both the possibility and difficulty of protecting voiceless populations. Advocates challenged dismissals of animal suffering beginning in the 1860s in the UK with mass demonstrations including the “Brown Dog” riots. Yet a century later, a new law was still needed: the UK's 1986 Animals Act. 75 The lesson: those opposed to protecting the voiceless vulnerable can require a sustained movement across generations.
There is one crucial difference: Suffering inflicted in animal research has decreased considerably, but the number of PINEs experiencing N-O-S will double by 2060. Without an effective movement, millions of humans will suffer in silence.
This article calls on clinicians, educators, and institutions to ARISE—to fulfill their moral obligation to vulnerable, inarticulate patients by serving as their Advocates, Recognizing that Non-Observable Suffering exists, and Investigating Suffering's hidden Existence by applying the required skills, time, and compassion for withdrawn patients who are NOT “just sitting there.”
Comment: “(hidden)”—in Italicized font and parentheses in the definition and acronym signals that the suffering on which the movement focuses is hidden. While “h” is not included in the acronym, hidden is implied by focusing on “all” suffering.
Limitations
My direct clinical experience implementing MA for patients in the Dementia Gap is limited to a half-dozen cases since 2023. Knowledge of this substage is in its infancy. More research is needed to answer such basic questions as: How long do patients typically remain in the Dementia Gap? Can clinical factors predict when patients will lose their ability to eat and drink?
As an advocate for implementing MA to treat intolerable suffering, I acknowledge my bias may have influenced my case selection and ethical analysis, despite my efforts toward balance. This article's arguments and recommendations are my observations and opinions—not established guidelines derived from established consensus. I explicitly welcome critical evaluation and alternative perspectives. A main goal in writing this article is to inspire debate among experts with diverse backgrounds that will hopefully lead to panels of leaders who convene to develop practice guidelines designed to provide patient safety without prolonging their suffering.
Moral issues: potential opposition
Can Moderate Anesthesia be moral?
Regarding the moral argument, “foreseeability equals intended”
Critics could argue: sedated patients cannot eat or drink, and no artificial nutrition and hydration is provided; therefore, dying is inevitable—not merely a foreseeable possibility. How then can earlier death not be intended? Here are two counterarguments:
First, if light sedation does relieve suffering, the protocol's next step is to allow patients to resume eating and drinking or, if then needed, provide oral assisted feeding and hydration.
Second, this “inevitability objection” subjects MA to a higher ethical standard than withholding or withdrawing other life-sustaining treatments from terminally ill patients. Clinicians and ethicists rarely argue that withdrawing ventilatory support, dialysis, or pacemakers intentionally cause death. Instead, this is the prevailing ethical position: withholding and withdrawing non-beneficial, futile treatments for terminally ill patients—especially if such treatment prolongs severe suffering—is ethical, legal, and a patient “claim right” (a right that imposes a correlated duty on others).
How did surrogate decision-makers decide to implement treatments of last resort and can their decisions be considered moral?
Designated agents for BB (who had moderately severe dementia) and for AK (advanced dementia) decided on MA; Terry Matthews gave verbal consent herself. Table 5 compares how these decisions were made and morally justified. Additional highlights and Comments are below.
Clinical decision-making and moral justification for three patients administered Moderate Anesthesia.
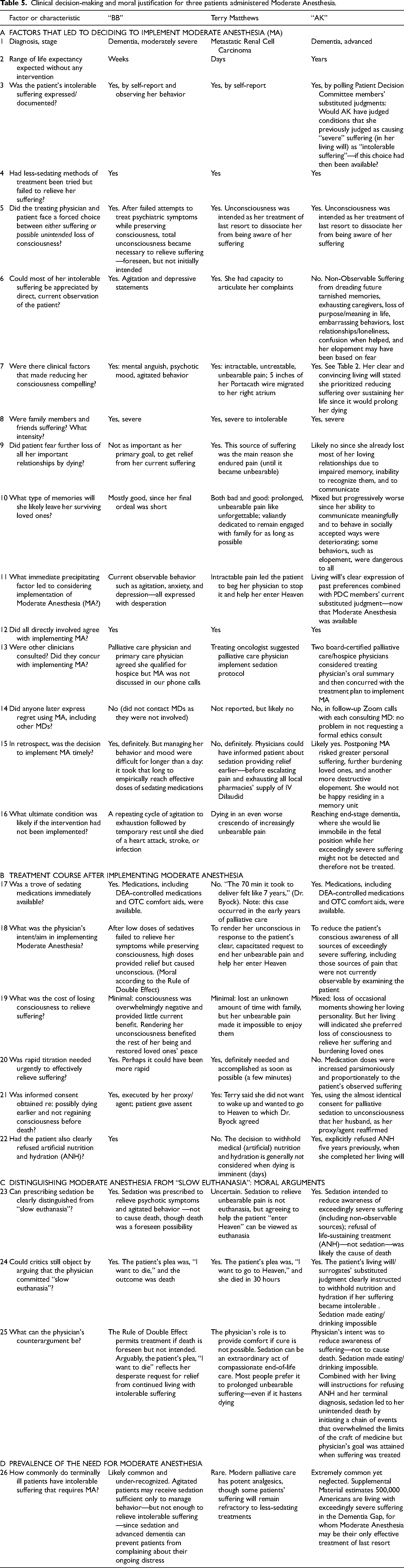
AK met the clinical criteria for receiving MA based on combining her past judgments of severe suffering intensity for each condition memorialized in her living will, and the current unanimous consensus of substituted judgments of her PDC members who all agreed to this: If during ACP, AK had been asked if these six conditions would cause intolerable suffering, she would have judged yes. AK also consented to palliative sedation to unconsciousness (PSU)—a treatment of last resort with the same risks as MA, so her consent given during ACP sufficed for both.
Byock assumed Terry had sufficient DMC to give verbal consent for Rapid Sedation to Unconsciousness. While cognitively intact, her judgment might have been impaired due to being in a crisis state caused by unbearable pain and impending loss of family that caused depression. Consider this thought experiment: Had Byock given Terry enough IV Dilaudid to partially relieve her pain before asking if she were willing to consent to sedation that would begin in one hour, she might have declined. If so, she would have continued her previous priority and behavior: to remain with her family as long as possible.
Brittany Maynard's forced choice was based on anticipatory rather than current suffering. She could have continued living since consciousness still offered her meaningful and pleasant experiences. She stated unwillingness to risk future loss of capacity from progression of her brain disease that could prevent her from having sufficient capacity to make the decision to die later. So, she chose to exercise her current autonomy to die now, sacrificing weeks to months of somewhat satisfying living. To my knowledge, no one explained and then asked her to consider this third choice: Complete an effective strategic living will that would allow her to live until her condition deteriorated to a well-defined point where she judged her suffering would become intolerable.
For all four patients, the forced-choice perspective helps justify their treatment decisions as moral. In the case of Brittany Maynard, clinicians and bioethicists could reasonably ask whether the informed consent she was provided was adequate.
Is dying by VSED by capacitated patients moral or suicide? Is it moral for advance directives to conditionally request ceasing assisted feeding and hydrating, or sedation—be it Moderate Anesthesia or Rapid Sedation to Unconsciousness?
Note: Brief answers to these two questions were inspired by Farr Curlin's opinions embodied in the text of some of the arguments he presented during a “Point–Counterpoint Session on Dementia-Specific VSED Directives” held on 2026 Apr 30 at the American Geriatrics Society Annual Scientific Meeting. (Personal communication by email, May 29, 2026.)
In contrast to physicians’ obligation to respect and respond to capacitated autonomous decisions to withhold or withdraw burdensome treatment, Curlin argued that physicians remain responsible to care for their current patients through basic care of assisted feeding and hydrating, which he considered an “expression of ordinary human solidarity.” Curlin could well have then quoted Matthew 25:35 (which I confirmed in our email exchange).
Referring to VSED requests, Curlin stated living wills “that request actions fundamentally contrary to a patient's basic interests—especially those that are self-destructive in nature—do not bind clinicians or surrogates in the same way as refusals of medical treatment.” He particularly noted that requests that “amount to self-harm, in this case by starvation and dehydration, fall outside what a reasonable person standard would require others to carry out.” (Out of context, this opinion does not consider either current or future harm patients can experience due to longer and greater suffering.) Curlin concluded that even where VSED by advance directive is legally permitted, physicians and family members are not ethically obligated to implement it.
I favor comprehensively expanding the concept of suffering as long as the requested implemented interventions are moral.4,7 My fundamental belief is that a primary societal function of physicians is to reduce suffering, a priority I strive to fulfill as I treat my patients and how I want to be treated myself. The imperative to reduce suffering can become relevant, compelling, and sometimes urgent when two conditions converge. First, an incapacitated patient may no longer understand that continued feeding and hydrating will prolong suffering as their terminal illness progresses. Second, a terminal illness causes suffering from multiple sources, some of which are non-observable, so that, when combined with observable suffering, patients can experience a suffering intensity that is severe, intolerable, or unbearable, even when the act itself—careful hand-feeding by another person—contributes no additional suffering.4
Curlin has revealed that he recognizes suffering can be severe enough to warrant palliative sedation to unconsciousness. When he wrote about Terry Matthews in 2018, 9 he stated: “I propose that physicians should act to relieve suffering insofar as that suffering is generated by and contributes to insults to health.” Terry died 30 hours after beginning sedation—in the gray zone that makes it difficult to decide whether sedation itself could be deemed the proximate cause of death.
On reflection, Curlin and I likely agree that the critical moral distinction is not whether death follows treatment, but whether physicians’ intent was to relieve suffering or to cause death. On that criterion, implementing a living will's instructions for a patient who can no longer understand that continued feeding will prolong and likely increase suffering—whether this patient lives in the Dementia Gap or endures currently undetected, Non-Observable Suffering-may reach an intensity similar to what Curlin endorsed as sedation-appropriate in the final clinical treatment of Terry Matthews’ terminal cancer.
Overcoming possible physician resistance to the ACP protocol
Timing of completing POLSTs and having POLST Conversations is not traditional:POLSTs—prior to my introduction of Future POLSTs—were always completed by seriously ill patients who are likely to die within one year. Yet justifying their completion during ACP is straightforward: surrogate-patient concordance for dementia is only 58%.
76
So, patients who want to control the last chapter of their lives must make advance treatment decisions for themselves while they still possess DMC, and for their decisions to be considered legally valid, have them notarized during ACP. Physician acceptance requires their understanding three facts: POLSTs are not unsigned but completed with signatures during ACP; only one POLST can be implemented at a time; changing the current POLST to another (Future) POLST requires the consensus of substituted judgments of PDC members and final approval of the treating physician. Physicians may resent sharing the determination of judging intensity of suffering—first with patients (during ACP) and then with PDC members when considering treatments of last resort: The protocol asks physicians if their clinical assessment matches “qualifying” conditions described in patients’ living wills. One prominent dementia clinical researcher described this part of the protocol diminishing their traditional role by using the word “mechanical.” Yet three factors justify the protocol's recommendation: (1) assessing inarticulate patients’ current suffering intensity is widely recognized as difficult
6
; (2) planning principals have a right to express their autonomy
30
; and (3) planning principals know their lifelong values and treatment preferences more accurately than surrogates.
76
Physicians’ fear of legal consequences: Most physicians have never been asked to implement a previously signed POLST. Some may worry whether MA is too similar to euthanasia to be legal. Still others may not be convinced that many patients experience N-O-S. In these and other intractable situations, agents can use their granted authority to transfer patients’ care to another physician who is comfortable with the protocol. Physicians may suspect planning principals inflated their judgments of intensity of suffering: Physicians have been alerted not to “up-code,” to fraudulently assign more severe diagnoses than warranted so they can collect higher fees. By analogy, physicians may doubt the motivation of planning principals who judge “too many” of the 36 conditions would cause intolerable suffering or who unreasonably assign “intolerable” to some conditions. Physicians could then suspect planning principals of “up-judging” the patient decision aid to qualify for Moderate Anesthesia because they cannot qualify for MAiD, or because MAiD is unavailable.
Are planning principals culpable? Not necessarily. Consider two points:
First, McCaffery taught the foundational principle that pain is subjective: “Pain is whatever the experiencing person says it is.” 77 This principle is relevant for all inner emotional states.
Second, planning principals can articulate this legitimate “cumulative suffering” rationale: They want to avoid prolonged suffering while they are being forced to wait in the Dementia Gap until they become dependent on others assisting their feeding and hydrating. They view the cumulative harm from prolonged severe suffering as great a harm as shorter episodes of intolerable suffering. This concept could be illustrated by a mathematical model that compares the areas under the curve that plots suffering-versus-time, though it is too sophisticated to expect from typical planning principals.
Developing guidelines with safeguards to protect vulnerable patients
Protocols using Patient Decision Committees offer meaningful, if imperfect, protection by polling members’ substituted judgment. If most PDC members will not benefit from an earlier inheritance, then conflicts of interest leading to premature death decisions may be reduced in this area. Similar reasoning applies to ending caregiving burdens. Ultimately, panels of experts from disciplines such as bioethics, healthcare law, palliative medicine, geriatrics, and ACP policy may convene to establish ethical safeguards that balance these two risks—unwanted sacrifice of living due to premature sedation and forced prolongation of suffering that respects patient's autonomous choices.
Four types of patients when considering ACP effective for the Dementia Gap
The protocol considers four types of patients separately. Table 6 presents their current DMC status, prior ACP completed, specific actions needed to upgrade, and estimated prevalence.
Ethics consultations: mandatory for patients lacking DMC and prior consent.
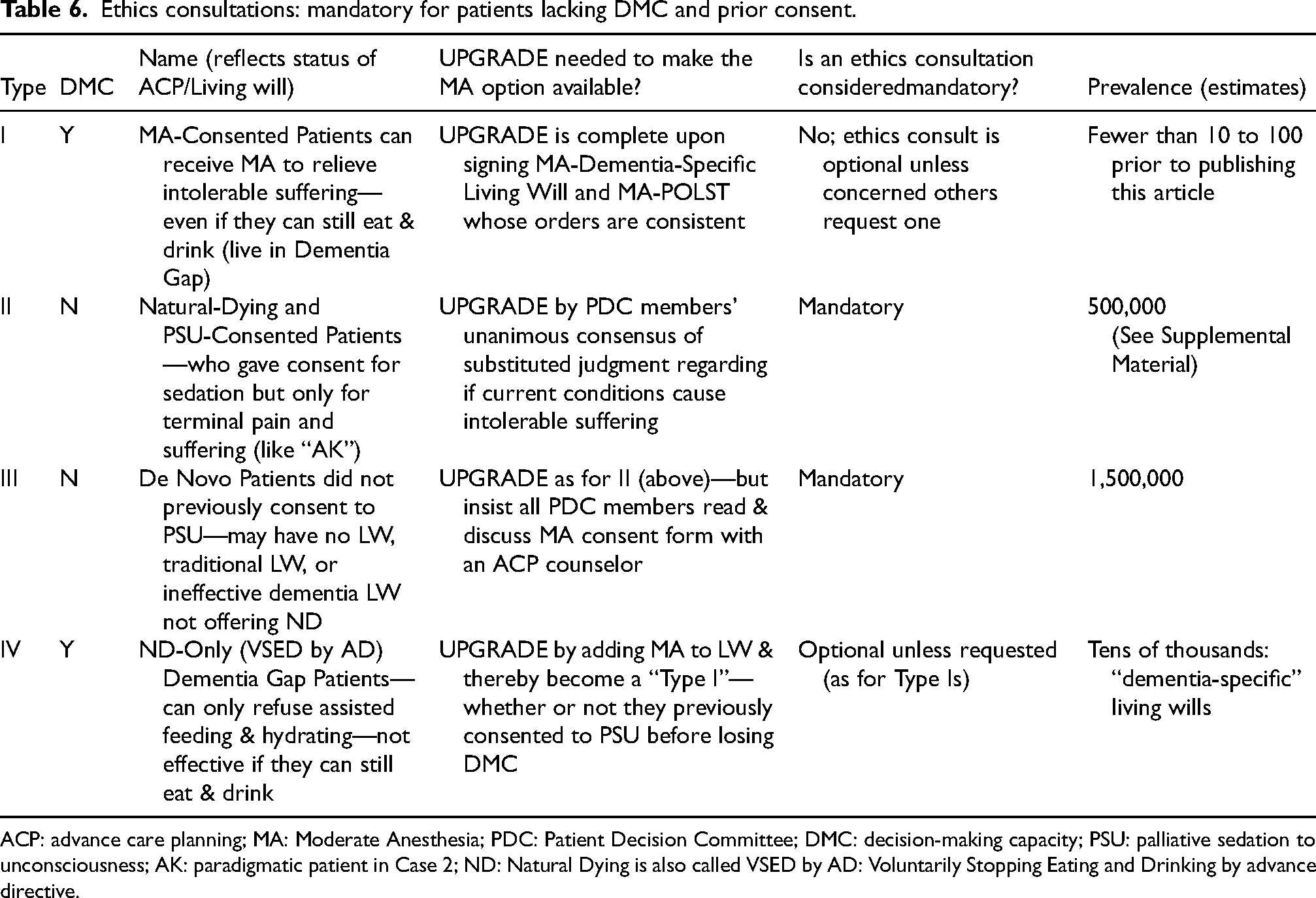
ACP: advance care planning; MA: Moderate Anesthesia; PDC: Patient Decision Committee; DMC: decision-making capacity; PSU: palliative sedation to unconsciousness; AK: paradigmatic patient in Case 2; ND: Natural Dying is also called VSED by AD: Voluntarily Stopping Eating and Drinking by advance directive.
Type I patients have followed this article's protocol by completing a MA-Dementia-Specific Living Will during ACP. Type IV patients still possess DMC, so they can upgrade to Type I by adding Moderate Anesthesia to their current “dementia-specific” living wills that typically include Natural Dying (VSED by AD) but have no provision for Moderate Anesthesia.
Since our 2022 critical review of then-available “dementia-specific” living wills 66 did not (A) recognize existence of the Dementia Gap, (B) appreciate its additional therapeutic challenge to relieve suffering, or (C) propose MA as the treatment of last resort, many Type IVs must upgrade to avoid prolonged suffering in the Dementia Gap.
Type II and Type III patients lack DMC, which leaves the decision to implement MA to PDC members’ unanimous consensus of substituted judgment based on reaching specific, qualifying clinical conditions. These patients depend on others to complete their “end-of-life planning”—not “advance care planning.” Surrogates make their decisions regarding implementing MA without patients’ current participation. Example: AK (Case 2), the paradigmatic “PSU-Consented” Type II patient, had previously consented to PSU that has the same risks as MA. She also consented to another treatment of last resort (Natural Dying/VSED by AD) whose risk is an early death. Therefore, her upgrading process required a small leap.
Type III “De Novo” Patients did not consent to PSU, so the upgrade protocol adds this task for PDC members: they must read the MA consent form and discuss the risks and benefits of MA with an end-of-life planning counselor before rendering their substituted judgment. The goal is for PDC members to have an adequate medical/ethical knowledge base regarding consent to MA. Comment: a short quiz could be developed to test whether members’ gained this knowledge.
Should ethics consultations be mandatory before implementing MA?
Capacitated patients can legally express their autonomy to VSED. In contrast, laws protect vulnerable, incapacitated patients when others make the same decision on their behalf. To protect them, Supreme Court Chief Justice Rehnquist warned, in his 1990 Cruzan ruling: “Close family members may have a strong feeling—a feeling not at all ignoble or unworthy, but not entirely disinterested, either—that they do not wish to witness the continuation of the life of a loved one which they regard as hopeless, meaningless, and even degrading. But there is no automatic assurance that the view of close family members will necessarily be the same as the patient's would have been had she been confronted with the prospect of her situation while competent.” 78 This court established the cautionary precedent of “clear and convincing evidence” as the highest standard for surrogate decision-making in end-of-life care.
Similarly, vulnerable incapacitated patients (Type II and Type III), need protection that ethics consultations can provide.
Table 6 states the author's opinions that ethics consultations are mandatory for Type II and Type III patients; but optional for Type I and IV patients since they have capacity to give informed consent for themselves.
Comment on prevalence with respect to Gaster's “dementia-directive” 79 : While Gaster's directive has likely been downloaded more than all others combined, it does not offer the option, Natural Dying/VSED by AD. This living will cannot be effective for many patients; therefore, Table 6 classifies patients using this living will as Type III.
Why I did not request an ethics consultation for AK
I consulted two board-certified palliative care physicians before I implemented the MA-POLST for AK, but I did not request a full, independent ethics consultation, which Table 6 states is “mandatory.” I mulled over my reasons for months, which I summarize and assess below.
I was still learning. AK was my first Dementia Gap patient. While her treatment can be deemed successful (see Table 5), I ultimately decided on the recommendation to mandate ethics consultations in the protocol.
I consulted with Katherine Hammond, the daughter/agent of Margot Bentley, who died in 2016 after enduring nearly four years of court-ordered, forced spoon-feeding. Many consider the order overrode her living will's statement of reaching a condition for which she wanted “No nourishment or liquids.” The court accepted the argument she limited her wish to the more commonly requested refusal of artificial nutrition and hydration. 80 I speculate that her tragic end-of-life suffering might have been prevented had she added just one word to her living will, “oral,” between “No” and “nourishment.” (Bentley created her own living will before British Columbia or other sources provided guidelines and good examples that suggested adding “oral.”)
Hammond testified to Canadian Parliament that her mother was “forced to exist in the very state that she tried so hard to avoid…[that] her suffering prolonged by others.”81–83 One judge ruled the behavior of opening her mouth and swallowing what others put in, as reflecting her remaining DMC that expressed her continuing desire to be fed. Comment: This is an astonishingly low standard for DMC; I personally know no bioethicist who agrees.
Bentley died from slow starvation. The illustrated patient decision aid 84 that planning principals use to generate ND-Living Wills 85 includes a horrific photo after her long starvation, where she resembles a Holocaust victim. Force feeding likely caused suffering that included hunger, wasting with weakness, and a multitude of N-O-S, many of which will never be fully known—that in combination may have been a torturous experience.
A challenge: how to motivate Type IV patients to upgrade?
Type IV patients represent a new generation of planning principals: they have already completed a “Natural Dying-Only” (“VSED by AD”-only) Living Will, unaware that it will be ineffective if they reach the Dementia Gap. This applies to all patients who completed ACP with Caring Advocates prior to 2023 (like AK), plus many more who completed living wills drafted by others: perhaps tens of thousands need to upgrade. Motivating them could be challenging: it requires education that alerts them to the additional challenge presented by the Dementia Gap at a time when they may not be suffering and have lived thinking they already completed ACP. Since they will lose the opportunity to upgrade when they lose DMC, finding ways to motivate them is a research imperative.
Why this article deferred considering PINEs enduring “severe” suffering by first focusing on the smaller number enduring “intolerable” suffering
It is easier to justify a needed treatment of last resort for intolerable suffering than for “only” severe suffering, so others might more readily accept such treatments in two steps. A smaller number of patients minimizes the failure of clinicians and bioethicists to recognize patients in the Dementia Gap. (I hereby admit my own failure for not recognizing the Dementia Gap until September, 2023.) Others may be more willing to first accept the smaller number of patients with intolerable suffering and then accept the larger number with severe suffering. Learning about N-O-S via poignant clinical stories (Gladys, Henry, and the patient burned by hot coffee) may make it easier for clinicians and bioethicists to accept the concept that more patients than previously appreciated endure significant Non-Observable Suffering. Accepting arguments to view sedation to unconsciousness as ethical and moral for late-stage dementia patients with intolerable suffering may make it easier to then accept proportionate sedation for patients with severe suffering. Presenting protective safeguards addresses clinicians’ and bioethicists’ worry about harming vulnerable patients and provides needed balance—initially to alleviate intolerable suffering, and then to alleviate severe suffering—so it can be deemed reasonable for patients living in the Dementia Gap enduring severe chronic suffering to use MA as a treatment of last resort.
Comparing two protocols to judge intensity of suffering: single physician assessor versus three sources
In Quebec, Advance MAiD Requests (AMRs) recently became legal for patients diagnosed with neurocognitive disease. 86 To implement MAiD, the patient's current suffering must be judged intolerable. The question is, how to judge suffering intensity in inarticulate, incapacitated patients?
In 2026, Holland and Moreau (H&M) presented what I call a single “clinical assessor” protocol. 87 Example for a patient receiving incontinence care: If she “grimaces and cries while being assisted with toileting while appearing content at other times, the clinician can infer they are suffering” and execute MAiD; if not, “the clinician may infer that the person has accepted this loss of independence” and not execute MAiD. This protocol has potential errors of observation, interpretation, and inadequate information about values. Current Quebec forms do not capture values information; video is not routinely used to memorialize patients’ expressed values; and assessors are not asked to consider Non-Observable Suffering or to observe patients over several hours. H&M themselves identify the core vulnerability: “By requiring the assessor to determine the presence of unbearable suffering, the assessor's values may be introduced into the decision-making process.”
Terman's
Source 1: the patient's own voice. During ACP, patients judge how much suffering each condition would cause as trained ACP counselors encourage capacitated patients to elaborate on their lifelong values and treatment preferences, to explain why, using a 36-condition Illustrated Patient Decision Aid (IPDA). Each condition is depicted as a high-resolution color image revealing inner emotions through facial expression, body language, and thought bubbles. For the incontinence condition, the patient grimaces and thinks, “I feel so ashamed.” Yet the introductory narrative asks patients to also consider whether joy can be experienced at other times during the day. If so, suffering during incontinence care may be relatively brief and therefore tolerable. Interviews are memorialized on video and transcribed. Obtaining direct information from capacitated patients is more credible than inferring patients’ values after they have lost capacity.
Source 2: the Patient Decision Committee. Three or more surrogate decision-makers, Trusted Persons, chosen for their deep knowledge of the patient, are polled during a clinician-facilitated discussion. They contribute personal knowledge of the patient's lifelong values, sources of joy, and past experiences with dying—information treating clinicians infrequently possess. They also alert the clinician when a qualifying condition may have been reached, and confirm through substituted judgment that disease progression has brought the patient to a condition previously judged intolerable during ACP.
Source 3: the treating physician's current assessment and review. Physicians consider all available information—their own clinical assessment plus the patient's living will responses plus the PDC polling of substituted judgment, local statutes, and generally accepted medical practice. Their function therefore extends beyond merely matching current conditions to AMR conditions. Physicians are ultimately responsible for determining the clinical appropriateness of deciding that implementing a treatment of last resort is patient-centered rather than self-serving.
Three-Source Concordance relieves physicians from bearing sole responsibility for judging suffering intensity in incapacitated patients. In making the ultimate existential decision, it considers the patient's own advance decisions and PDC members’ input. The result can be confidence in implementing MAiD or a Future POLST, including one for Moderate Anesthesia. Its motivating principle is the operational respect of patient autonomy in the context of a humanitarian crisis: every patient in the Dementia Gap enduring severe chronic suffering without access to an effective treatment of last resort represents a preventable failure of end-of-life care.
Reducing late-stage dementia suffering requires academic research, scholarship, and education
Addressing late-stage dementia suffering requires sustained academic research, clinical education, and policy development. The Supplemental Material documents a profound disparity: MAiD receives substantial academic attention and funding despite accounting for only 0.2% of deaths, while dementia, present in one-third of people who die after age 65, remains dramatically understudied. Recent increases (approaching 2% of all deaths) can be attributed to changing the law to allow nonresidents access. Example: in the last two years in Vermont, 56 out-of-state residents added to 132 Vermont residents. 88 These patients were able to reduce their suffering for up to six months. In contrast, the Dementia Gap and Non-Observable Suffering may affect hundreds of thousands of patients, not for months but for years before they die, but have to date received almost no research attention or clinical resources. (See Supplemental Material to this article.) Across more than two decades, approximately one scholarly publication exists for every patient who has used MAiD—a ratio of roughly 1:1—while for patients living in the Dementia Gap, that ratio stands at 1:500,000. This huge gap in the literature should not remain.
Conclusion
The “just sitting there” fallacy: final comments
Many dementia patients appear to be “just sitting there”—not suffering but withdrawn, unable to enjoy meaningful interaction. Observers assume they cannot recognize relatives, chant religious hymns, or “dig” jazz. This assumption could be wrong; if so, it is dangerous. Dismissing patients as incapable of human connection without researching their personal interests and using advanced interviewing skills can deny their fundamental humanity, create self-fulfilling prophecies that allow severe suffering to continue undetected until death, deceive caregivers into believing apparent calm equals inner peace, and deprive patients of goal-concordant end-of-life care.
The Dementia Gap crisis combined with N-O-S
As dementia progresses, an increasing percentage of patients will experience Non-Observable Suffering they cannot articulate. For those living in the Dementia Gap—able to eat and drink independently despite profound cognitive impairment—Moderate Anesthesia could be their only effective treatment of last resort. It is essential to distinguish patients who have potential to interact meaningfully if successfully awakened from withdrawal, from those who need sedation to relieve suffering. Progress cannot begin until clinicians stop assuming: “She's not suffering; she's just sitting there.”
This article argues that Moderate Anesthesia can be clinically appropriate, legal, ethical, and moral. It takes this bold stand: prognosis or life-expectancy is irrelevant. A trial of Respite Sedation and the use of proportional sedation that is not intended to hasten death may establish a sound basis to view MA as moral. Widespread acceptance could prevent prolonged suffering for an estimated 500,000 Americans in the Dementia Gap; extend lives by reducing premature deaths driven by “Dementia Fear” and “Loss of Autonomy Fear”; reduce attempts to die at “five minutes to midnight”; enable appropriate treatment for middle-stage patients rather than viewing illness as an “opportunity” to avoid late-stage dementia; provide legal, moral alternatives for families considering mercy killing; and stop wasting scarce resources on treatments that patients would refuse and cannot appreciate.
A proposal: begin the ARISE movement this humanitarian crisis demands
ARISE—Advocate by Recognizing and Investigating Suffering's (hidden) Existence—can be the rallying framework to recognize the humanitarian crisis this article calls the “Dementia Gap.” It aims to inspire Advocates to attend to individual patients’ needs and beyond: to investigate hidden suffering broadly and pursue the systemic changes this crisis demands. This can include expanding end-of-life curricula, developing skilled interviewing techniques, supporting effective PDC functioning, and ensuring that 500,000 to 1,000,000 patients in the Dementia Gap are not abandoned to suffering that goes undetected, unnamed, and untreated. Perhaps a “Registry for Dementia Gap Experiences” (RIDGE) will be established to transform individual caregiving experiences into collective wisdom. Family members and clinicians can share their experiences, adding to the clinical data that supports many more patients than we appreciate are actually “alive inside.”
Researchers must address critical unanswered questions: How long do patients remain in the Dementia Gap? What predicts loss of independent eating? How prevalent is N-O-S, and how satisfied are survivors after MA? Can assessment scales make N-O-S observable? Policymakers and professional organizations must convene expert panels to develop consensus guidelines with safeguards preventing premature sedation while ensuring severe suffering is not prolonged.
The moral imperative we all can share
The path forward requires collaboration across families, clinicians, researchers, educators, and policymakers. At worst, these patients are ignored. At best, intense efforts to discover and relieve their suffering can allow longer, more satisfying lives followed by timely dying consistent with their values and wishes.
With a 42% life-time risk of dementia after age 55, 70 any of us may one day be living in the Dementia Gap. At best, others will recognize and investigate our own hidden suffering—if our advance care planning was wise and strategic. Then we must, each in whatever way we are able, advocate for the half-million people currently suffering with no voice and possibly inadequate treatment, and for the millions who will follow. This is our moral imperative.
Supplemental Material
sj-docx-1-alr-10.1177_25424823261460085 - Supplemental material for For patients living in the “Dementia Gap”, a newly defined substage of late-stage Alzheimer's disease, with intolerable suffering: Can sedation to unconsciousness be moral?
Supplemental material, sj-docx-1-alr-10.1177_25424823261460085 for For patients living in the “Dementia Gap”, a newly defined substage of late-stage Alzheimer's disease, with intolerable suffering: Can sedation to unconsciousness be moral? by Stanley A. Terman in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
Karl E. Steinberg, MD, reviewed selected portions relating to novel uses of POLSTs and ethics consultations. Francis L. Mueller, MD, reviewed selected portions relating to administration of sedating medications. Bioethicist Stephanie van Slyke read the entire manuscript and shared her critical comments. Coley A. Perry used his AI skills to generate color images of people affected by end-of-life or late-stage dementia conditions according to SAT's specific instructions—see “Generative AI Disclosure,” below. Thubi A. Kolobe, PhD, provided critical feedback in the areas of medical narrative writing and research design.
The patient decision aid My Way Cards contains 36 high-resolution color illustrations to depict common end-of-life or late-state dementia conditions. AI designer Coley A. Perry created these images using his Cardinal Loop Systems (CLS)—a workflow system combining multiple AI tools with human oversight to ensure quality and accuracy. They included Claude (by Anthropic) to help coordinate details of the creative process as image descriptions are further refined based on Terman's feedback, and Gemini (by Google) that generates the actual illustrations from the final text descriptions. This procedure was specifically developed and integrated to function as a patient decision aid. A few details regarding how collaboration proceeded: SAT provided (A) the black-and-white line drawings currently in use (for most, since 2009) and (B) verbal descriptions of the condition each image strived to illustrate, (C) SAT described the desired facial expressions needed to reflect specific emotions that were essential to judge suffering intensity, and (D) “bubbles” (as in cartoons) containing words—either spoken to clarify the situation or thinking -to provide insight into inner feelings of the illustrated characters. An iterative process refined the image until SAT was satisfied that each illustration accurately reflected the intended condition and reflected typical resulting emotions. These AI-generated illustrations replaced the black and while line drawings of now-retired illustrator William Young whose contribution previous publications acknowledged. In summary, this human-AI collaboration improved a previous human-human collaboration to create original artwork for use in a patient decision aid. SAT also used Claude (Anthropic) in several ways: For literature review augmentation, citation formatting to Sage Vancouver style, EndNote conversion to JAD requirements, refinement of selected paragraphs to improve clarity, conciseness, and impact, as a dialogue entity for exploring ethical reasoning on some clinical or ethical challenges, and to create an acronym with specific attributes. Yet all content, conceptual framework, clinical observations, opinions, and final editorial decisions remain the original creative work and responsibility of the author.
Ethical considerations
This study involved retrospective analysis of my best efforts to provide clinical care; therefore, no Institutional Review Board (IRB) approval was required.
Consent to participate
Not applicable
Consent for publication
Cases 1 and 2 involve deceased patients treated by the author. Case 1 (“BB”): Written consent for publication was provided by the patient's legally designated healthcare agent. Case 2 (“AK”): Written consent for publication was provided by the patient's surviving spouse. Cases 3–6 (Terry Matthews, Brittany Maynard, Gladys Wilson, and Henry Dryer) were based on publicly available information without additional consent.
Author contribution(s)
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declares no financial competing interests. Increased interest in the patient decision aid “My Way Cards” may follow publication; however, these cards are not sold commercially. They are available only through authorized, trained healthcare providers who incorporate them into advance care planning consultations—services typically reimbursed by health insurance. No fees currently exist for provider training and authorization.
Data availability statement
Additional clinical data regarding Cases 1 and 2 are available, but were judged irrelevant to understand how decisions treatments of last resort were made and to assess if they can be viewed as moral. Also, patient privacy needs to be protected. Additional information about Cases 3–6 is available from citations the manuscript provided, and most is on the Internet.
Author information
Stanley A. Terman, PhD, MD, is founder and medical director of Caring Advocates, a California nonprofit organization. Since 2000, its mission has been to reduce the suffering of terminally ill patients and their families, particularly those affected by Alzheimer's disease and related dementias. Dr Terman received his BA from Brown University, PhD from MIT, and MD from the University of Iowa. His psychiatric residency was at Indiana University. He was on the faculty at UC Irvine until beginning private practice in 1982. He resides in Sausalito, California.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.