
Abstract
Background
Alzheimer's disease (AD) is an increasing public health concern, especially among adults over age 40 in rural regions, where chronic conditions are prevalent and healthcare resources are limited.
Objective
This study aimed to determine the impact of aging and body mass index (BMI) on self-reported cognitive impairment, while controlling for covariates.
Methods
We analyzed cross-sectional survey data from hospital visits in Parmer and Cochran counties, using Pearson's chi-squared test, two sample proportions, and binary and multivariable logistic regression.
Results
Due to varying social involvement, individuals lacking social activities but becoming engaged at baseline experienced slower cognitive decline over time. Individuals aged 70 and above in Cochran and Parmer Counties had higher odds of cognitive impairment compared to those aged 40–49, with these associations remaining significant after adjusting for covariates (p < 0.05). Cochran County data showed that participants aged 60–69 who are overweight had much lower odds of cognitive impairment than those aged 40–49 with a normal BMI, after adjusting for anxiety, depression, and memory loss (OR = 0.2, CI: 0.1–0.8, p = 0.026). Similarly, in Parmer County, individuals aged 60–69 who are obese also had reduced odds compared to younger adults with a normal BMI (OR = 0.2, CI: 0.1–0.8, p = 0.027).
Conclusions
Aging remains associated with self-reported cognitive impairment, even after adjusting for risk factors, highlighting need for targeted interventions for elderly populations. Lower odds among overweight and obese seniors suggest a complex relationship between higher BMI and cognitive impairment in this population.
Introduction
Aging is broadly characterized as a gradual, time-dependent decline in cellular and organ function, leading to increased vulnerability to chronic diseases and mortality. 1 It is one of the most significant risk factors for neurodegenerative diseases such as Alzheimer's disease (AD), with approximately one in ten individuals aged 65 years and older diagnosed with AD, a prevalence rises with advancing age. 2 Neurodegenerative diseases are among the most common precursors of cognitive impairment and dementia. 3 Dementias associated with AD and AD-related disorders are marked by cognitive deterioration that substantially impairs the ability to carry out daily activities independently. 4
The increasing proportion of the elderly population is associated with an increased burden of cognitive impairment on communities, affecting not only patients and families but also placing considerable strain on public resources, including Social Security, Medicare, and Medicaid. 5 According to the World Health Organization, the global population aged 60 and older is projected to nearly double from 12% in 2015 to 22% by 2050. 6 The same trend is observed in Texas, a fast-growing state in the United States with 30 million people and about 13% of people 65 years and older. 4 This demographic shift underscores the urgent need to understand the life course factors that influence cognitive decline and dementia risk as people age. Such insight is vital for informing early interventions and public health strategies, given the extensive implications of cognitive impairment on individuals, caregivers, and healthcare systems. 5
Cognitive function plays a central role in the well-being and quality of life of individuals transitioning from midlife to older adulthood, influencing critical decisions related to employment, retirement planning, and financial management. 5 Sustaining cognitive health throughout aging is vital. It hinges on the adoption of health-promoting behaviors, including regular physical activity, adherence to a balanced diet, and the avoidance of smoking and excessive alcohol consumption.7,8 However, older adults in Texas, particularly those residing in rural West Texas, encounter substantial socioeconomic barriers that impede consistent engagement in such behaviors. Limited access to essential social determinants of health contributes to elevated rates of chronic conditions, which, if not adequately managed, increase the risk of cognitive decline and progression to dementia.9–13 Consequently, rural West Texas may carry a disproportionate burden of cognitive impairment. 13 These trends underscore the urgency of evaluating and addressing cognitive impairment, especially in underserved regions, as its growing impact places mounting pressure on individuals, families, and the broader healthcare infrastructure. 14
A variety of chronic conditions, which commonly share high body mass index (BMI) as a key factor, including hypertension, diabetes, obesity, cancer, neurological disorders, social isolation, and depression, have been identified as significant risk factors for both mild cognitive impairment and its progression to AD or dementia.5,6 In order to elucidate the interaction between these chronic diseases and aging in the development of cognitive impairment, research has focused on quantifying the influence of these risk factors throughout the aging continuum. Interestingly, evidence suggests that their influence on cognitive decline diminishes with advancing age. 15 One plausible explanation is that individuals who survive into older age tend to maintain healthier lifestyles, thereby reducing their cumulative exposure to these chronic conditions.5,15 Another consideration is that individuals heavily burdened by such risk factors may not live long enough to undergo clinical evaluation in later life stages, which could result in underestimation of their contribution to cognitive impairment among the oldest cohorts. 15
Project FRONTIER was established in 2006 to gather data from counties in rural West Texas to examine diverse chronic disease factors that affect rural elderly populations. 16 Our analysis of data from Project FRONTIER aims to identify the impact of aging and body mass index on cognitive impairment in rural West Texas adults. By assessing the prevalence of cognitive impairment across age groups and incorporating the impact of BMI, this research provides critical insights into cognitive impairment, the populations most affected, and opportunities for effective interventions tailored to these populations.
Methods
Data source and study population
Data were collected through a cross-sectional survey employing a convenience sampling approach among individuals receiving medical care in Cochran and Parmer counties, located in West Texas. This data collection was part of the Project FRONTIER initiative, which targets residents aged 40 years and older living in rural areas of West Texas. The initiative aims to advance the overarching objectives of identifying risk factors associated with chronic diseases and evaluating their impact on mental and physical health within these communities. Most study participants reside in isolated regions where social determinants of health are constrained.
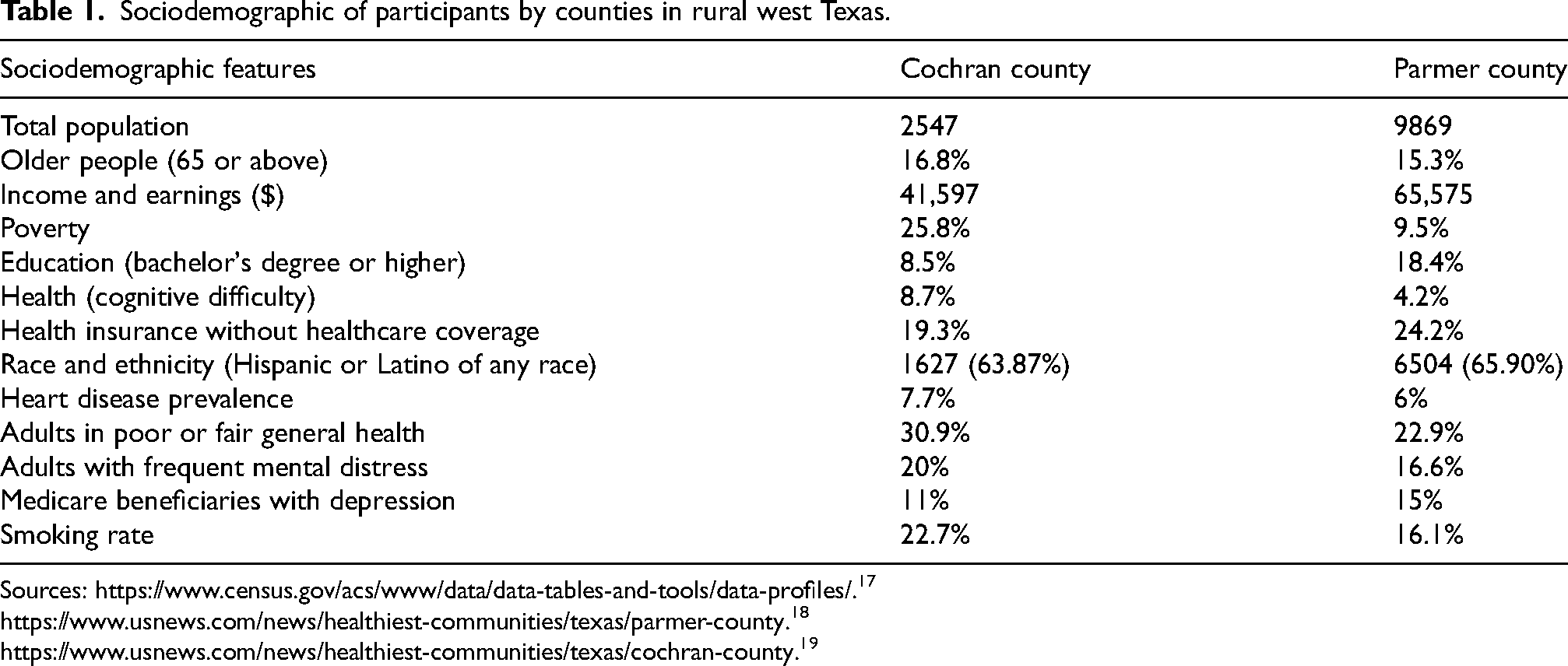
Table 1 presents the sociodemographic characteristics of participants by counties, Cochran and Parmer in rural West Texas. Cochran County has a population of 2,547, and Parmer County has a population of 9869. The percentage of older people (65 or older) is 16.8% in Cochran versus 15.3% in Parmer. Both counties are in rural West Texas, with differences in average household income and earnings ($65,575 in Parmer versus $41,597 in Cochran), poverty rates (9.5% in Parmer versus 25.8% in Cochran), higher education attainment (18.4% with a bachelor's degree or higher in Parmer versus 8.5% in Cochran), cognitive difficulty rates (4.2% in Parmer versus 8.7% in Cochran), health insurance coverage without healthcare coverage (24.2% in Parmer versus 19.3% in Cochran), and the percentage of adults experiencing frequent mental distress (16.6% in Parmer versus 20% in Cochran).
Sociodemographic of participants by counties in rural west Texas.
Sample size and power calculation
The sample size for this study was established using G∗Power software (version 3.1.9.7). 20 Through logistic regression analysis, G*Power software calculated that a total of 197 participants are required to conduct statistical analysis, but the study used a large sample size (n = 1287) for the analysis. This determination was based on the expectation of the proportion of individuals with normal cognition and cognitive impairment to be 60% versus 40%, with alpha (α) = 0.05, power = 80%, and a two-sided testing procedure. In most instances, the sample sizes were adequate to allow for meaningful cross-tabulation analyses. Nevertheless, there were some cases where the sample sizes were insufficient. These cases with small sample sizes were excluded from the final statistical analysis to ensure the integrity and reliability of the study's results.
Study participants
Study participants were selected based on the following criteria: age greater than or equal to 40 years, had healthcare insurance, and were residing in rural West Texas, Cochran, and Parmer Counties. Informed consent was signed by all subject participants. Eligible participants were provided with a specially developed questionnaire during their hospital visit. The questionnaire was designed in a binary format, with questions requiring “yes” or “no” responses. Through this instrument, participants indicated whether they considered themselves to have normal cognitive function or to be experiencing cognitive impairment. Participants’ awareness of cognitive impairment was established prior to their involvement in the study. This awareness could have stemmed from previous discussions with healthcare providers, such as physicians or nurses, during earlier hospital visits. As such, patients may have already discussed or confirmed concerns related to cognitive impairment with their healthcare professionals. It is important to note that the assessment of cognitive status was subjective, and no diagnostic method was employed to determine cognitive impairment at the time of data collection during the hospital visit. Instead, the data for this study were obtained from an existing digital hospital database, which contains records of patients with health insurance who attend regular health checkups in West Texas counties. The primary purpose of these visits was to support the maintenance of a healthy lifestyle among the population.
The definition of cognitive impairment was self-reported and its questionnaire was binary (yes or no). The study was based on the FRONTIER cohort of individuals aged 40 and above who have health insurance and live in Rural West Texas, specifically Cochran and Parmer Counties, and were visited through healthcare providers. The FRONTIER project office is located at the Texas Tech University Health Sciences Center (TTUHSC), and its hospital is within TTUHSC.
The data on study participation in each county is shown in Figure 1. All subjects selected were compiled from the Project FRONTIER. This community-based research study collected health-related information from the visitors who commute to their hospital for regular health checkups in rural West Texas. The data set was carefully reviewed, and empty, missing, or incomplete responses were removed. The data were organized into categories to improve usability, making it easier to access and analyze statistically.
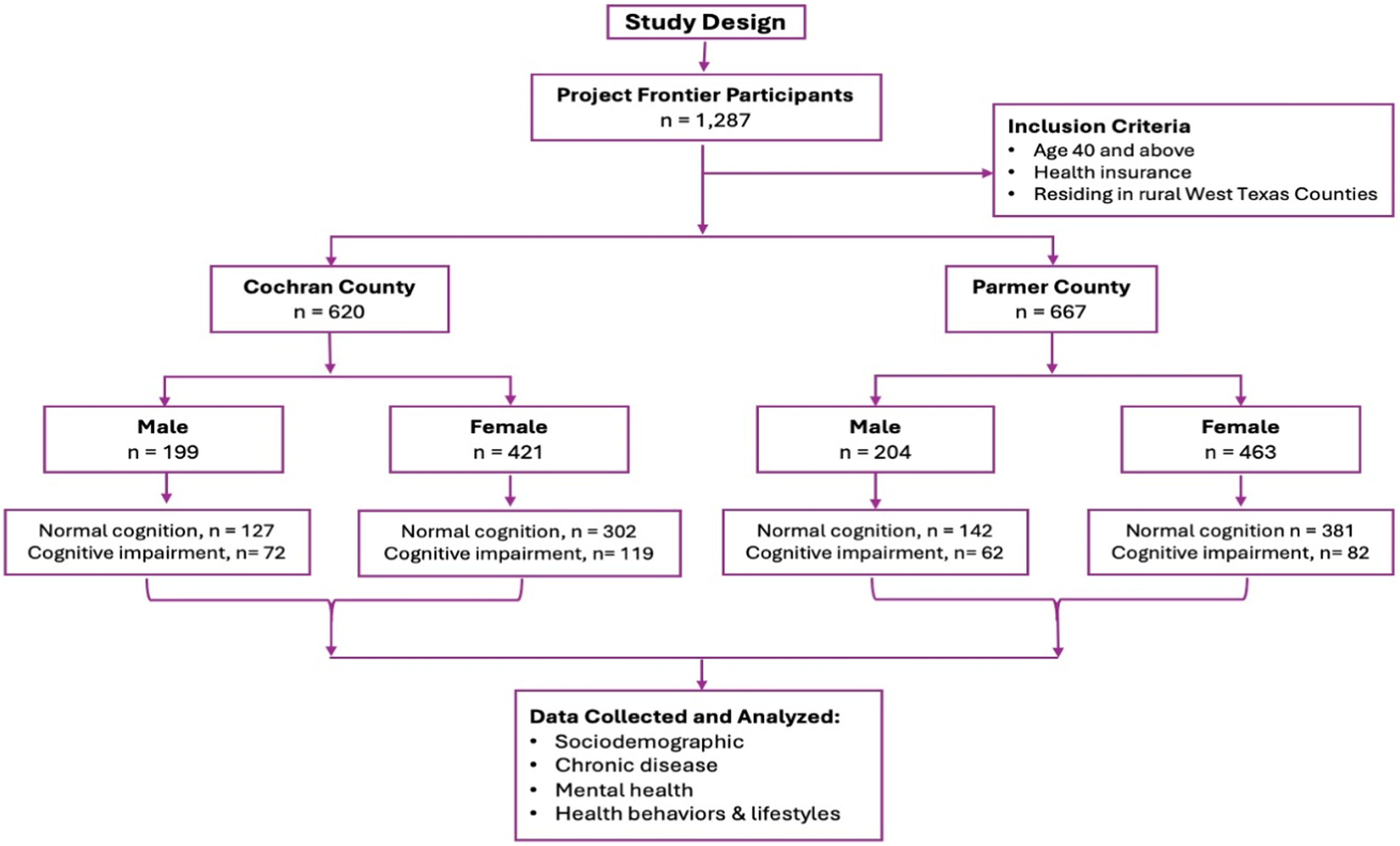
Flow of participants through study.
A total of 1287 subjects make up the sample size, out of which 403 were reported to be male, and 884 were reported to be female. Furthermore, 620 subjects belonged to Cochran County, and 667 were from Parmer County. Of the 620 participants in Cochran County, 199 were males and 421 were females. There were 127 individuals with normal cognition, and 72 individuals with cognitive impairment out of 199 male individuals in Cochran County. Of the 421 female individuals in Cochran County, 302 had normal cognition and 119 had cognitive impairments. Of the 204 male individuals in Parmer County, 142 had normal cognition, and 62 had cognitive impairment. In contrast, there were 381 female individuals with normal cognition, and 82 females had cognitive impairment in the same county. The sociodemographic factors such as age, BMI, sex, education, income, insurance, and race/ethnicity; the chronic disease factors such as cardiovascular disease, diabetes, stroke, and hypertension; the mental health factors such as anxiety, depression, and memory loss; and the health behaviors and lifestyle factors such as alcohol, caffeine, diet, exercise, and smoking were considered as risk factors for cognitive impairment. A total of 1287 participants’ data were used for statistical analysis.
Statistical analysis
Prior to conducting statistical analyses, all data were thoroughly cleaned and organized to ensure accuracy and consistency. This process enabled the production of reliable results and facilitated subsequent analyses. Both descriptive and inferential statistical methods were applied using IBM SPSS (Statistical Package for the Social Sciences) software, version 29.0. 21 Additionally, Python 3.14 was used to display the graphical representations of odds ratios and corresponding 95% confidence intervals across various age groups, by model and county. The justification for power and sample size was carefully considered to ensure the validity of the findings. Statistical summaries were generated for sociodemographic and chronic disease variables among participants residing in Cochran and Parmer Counties. Discrete variables were presented as counts (n) and percentages (%), while continuous variables were described using means and standard deviations. Statistical inference was conducted based on null and alternative hypotheses concerning the proportions of age groups of the participants. Cross-tabulations were performed to enumerate responses that matched specific characteristics, with results contributing to univariate analysis. Each cell frequency represented the number of participants with the corresponding attribute. Binary logistic regression was utilized for bivariate analysis, while multiple logistic regression was conducted for multivariable analysis. In these models, the dependent variable was categorical (normal cognition versus cognitive impairment), and the independent variables included dichotomous sociodemographic and chronic disease factors. The odds ratio and its 95% confidence intervals (CI) were calculated for each risk factor. A p-value threshold of <0.05 corresponds to an alpha level of 0.05. This approach was used to determine whether there was an association between risk factors and the occurrence of cognitive impairment. Bar graphs were used to present the frequencies of variables such as gender, age group, and BMI in relation to cognitive dysfunction. Additionally, a graph illustrating the odds ratio and 95% confidence interval was created and interpreted for significant predictors.
Results
Baseline characteristics for sociodemographic, chronic disease, mental health, and health behaviors & lifestyle within rural West Texas Counties associated with cognitive impairment are reported in Table 2. There were total of 1287 subjects, of whom 403 were reported to be male and 884 were reported to be female. The county descriptive statistics for the participants are: Cochran County, 199 (32.1%) were male and 421 (67.9%) were female participants. In Parmer County (n = 667), there were 204 (30.6%) male and 463 (69.4%) female participants.
Baseline characteristics for sociodemographic, chronic disease, mental health, and health behaviors & lifestyle within rural west Texas counties.
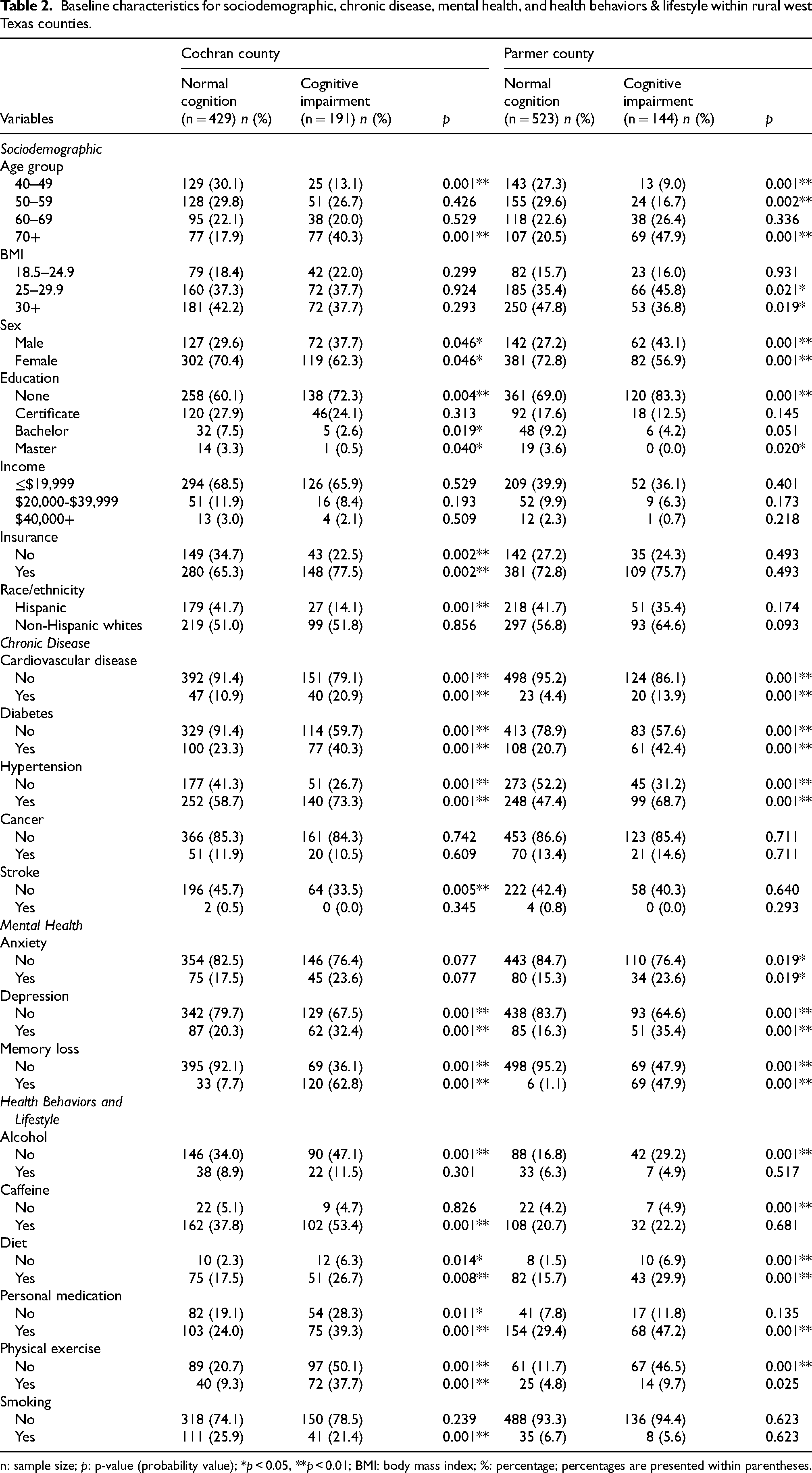
n: sample size; p: p-value (probability value); *p < 0.05, **p < 0.01; BMI: body mass index; %: percentage; percentages are presented within parentheses.
Out of 1287 individuals, of whom 335 (26%) were classified as cognitively impaired and 952 (74%) exhibited normal cognitive function. Age distribution was as follows: 310 participants (26%) were aged 40–49 years, 358 (28%) were 50–59 years, 289 (22%) were 60–69 years, and 330 (26%) were aged 70 + years. Regarding BMI, 226 participants (18%) had a normal BMI, while 483 (38%) were overweight and 556 (43%) were classified as obese. Statistical analyses such as cross-tabulation and two-sample proportions tests were carried out to compare the differences in normal cognition and cognitive impairment in the variables within the counties.
In Cochran County, a higher proportion of individuals aged 70 + had cognitive impairment (40.3%) compared to those with normal cognition (17.9%), while in Parmer County, 47.9% of those with cognitive impairment were aged 70 + . BMI was not significantly related to cognition in Cochran, but in Parmer, a larger share of cognitively impaired individuals had BMIs ≥25 (p < 0.05). In Cochran County, 37.7% of individuals diagnosed with cognitive impairment were male, compared to 29.6% among those with normal cognition (p = 0.046). Conversely, females constituted 62.3% of the cognitively impaired group, while they represented 70.4% of those with normal cognition (p = 0.046). These findings suggest that males in Cochran County were more likely to experience cognitive impairment than females, as indicated by the higher proportion of males in the impaired group compared to the group with normal cognition. In Parmer County, this trend was even more pronounced. Among individuals with cognitive impairment, 43.1% were male, whereas only 27.2% of those with normal cognition were male (p = 0.001). In contrast, females accounted for 56.9% of those with cognitive impairment and 72.8% of those with normal cognition (p = 0.001). The data from Parmer County underscored a significant sex-based difference, with males having a higher likelihood of cognitive impairment relative to females. Lower education levels were more prevalent among the cognitively impaired, with “none” reported by 72.3% in Cochran and 83.3% in Parmer (p < 0.01). Lack of health insurance was higher among those with normal cognition in Cochran (p = 0.002), but showed no significant difference in Parmer. Among ethnic groups, being Hispanic or non-Hispanic white was not statistically significant, except for a lower percentage of Hispanics with cognitive impairment in Cochran (14.1%, p = 0.001). For chronic diseases, cardiovascular disease, diabetes, and hypertension were notably more common among individuals with cognitive impairment (p = 0.001). Mental health conditions such as depression and memory loss were also more frequent among the cognitively impaired in both counties (p = 0.001). Regarding health behaviors, individuals with cognitive impairment were less likely to exercise or report being on medication, diets, or abstaining from alcohol, caffeine, and smoking (p < 0.01).
Figure 2(a) provides a visual summary of the comparison of cognitive dysfunction across different age groups, between genders, and across counties. The data demonstrated a clear trend of increasing cognitive decline from younger to older age groups in both Parmer and Cochran Counties, and this pattern is consistent across both male and female participants. In Parmer County, among males aged 40–49, 4 individuals (2%) exhibited signs of cognitive impairment. This percentage increased significantly in the 70 + age group, with 31 males (15%) affected. Similarly, in Cochran County, 8 males (4%) aged 40–49 showed cognitive impairment, compared to 29 males (15%) in the 70 + age group. For females in Parmer County, 9 individuals (2%) aged 40–49 experienced cognitive dysfunction. This number rose to 69 individuals (15%) in the 70 + age group. In Cochran County, 16 females (4%) aged 40–49 were affected, while 44 females (10%) in the 70 + age group exhibited cognitive impairment. Among participants aged 40–49, both males and females from Cochran County had a higher percentage (4%) of cognitive impairment compared to their counterparts in Parmer County (2%). In contrast, for the 70 + age group, the percentage of cognitive impairment among males was similar in both counties (15%). For females, the percentage in the 70 + age group was also similar (15%) in Parmer County but lower (10%) in Cochran County.
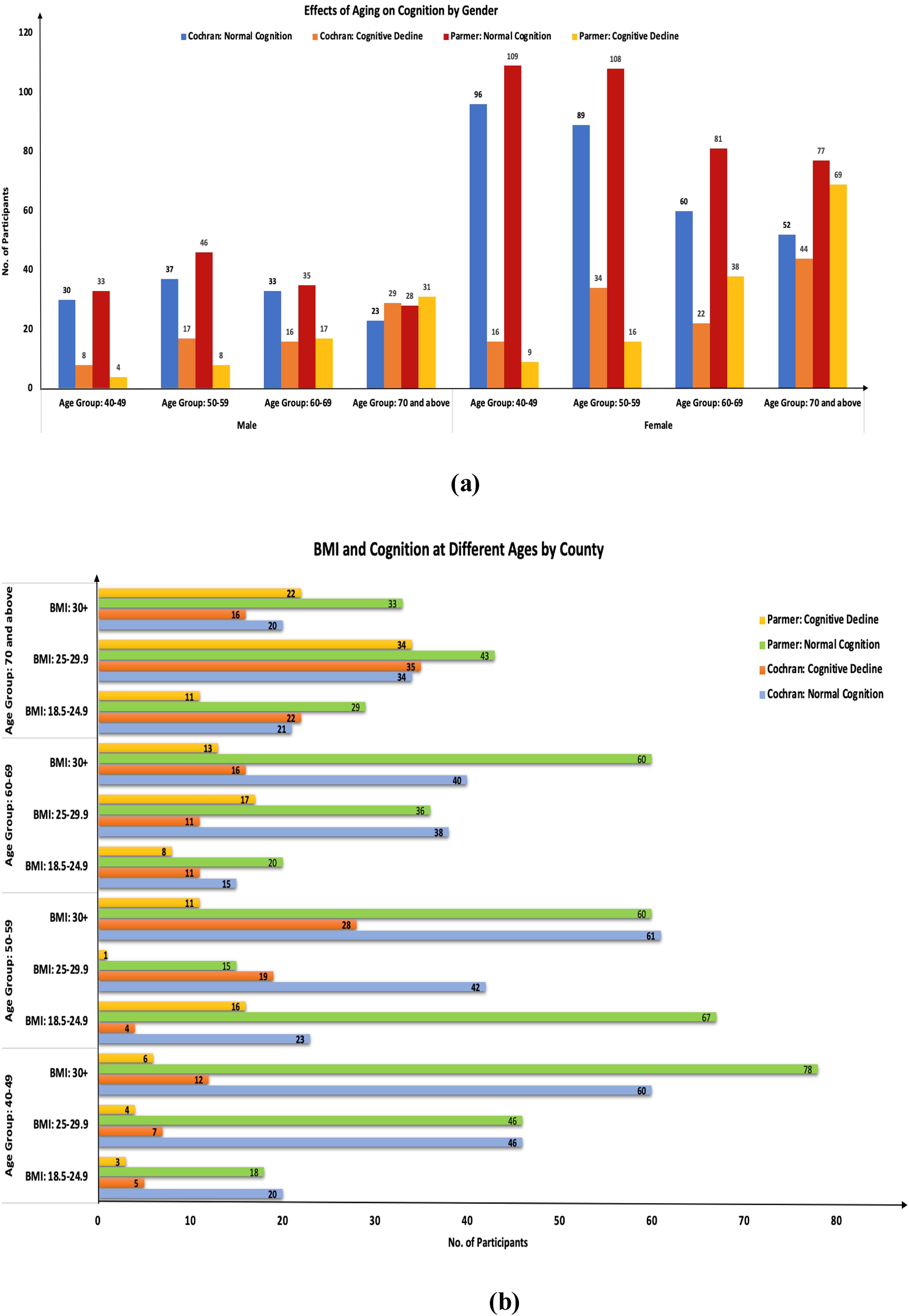
(a) Comparison of cognitive impairment at different age groups between genders and counties. (b) Comparison of cognitive impairment at different age groups and BMI between counties.
Figure 2(b) illustrates the relationship between cognitive dysfunction, age group, and BMI across Parmer and Cochran Counties. The data were examined within distinct age groups to highlight patterns associated with different BMI categories. For the 40–49 age group, both counties showed an increase in cognitive dysfunction numbers as BMI increased. In individuals with a normal BMI (18.5–24.9), the number of cases of cognitive dysfunction was 5 in Cochran County and 3 in Parmer County. Among those classified as overweight (BMI 25–29.9), cases increased to 7 in Cochran County and 4 in Parmer County. In the obese category (BMI 30+), the numbers further rose to 12 for Cochran County and 6 for Parmer County. These findings suggested a consistent trend of higher cognitive dysfunction rates with increasing BMI in the 40–49 age group for both counties. For the 50–59 age group, a similar pattern of increasing cognitive dysfunction with higher BMI was observed in Cochran County. Individuals with a normal BMI had 4 cases, while those in the overweight and obese categories had 19 and 28 cases, respectively. However, this trend was not evident in Parmer County, where 16 cases were observed in individuals with a normal BMI, only 1 case in the overweight category, and 11 cases in the obese category. The lack of a consistent increase with higher BMI in Parmer County distinguished this group from the trend seen in Cochran County. Among individuals aged 60–69, the association between BMI and cognitive dysfunction was less pronounced. In Cochran County, there were 11 cases in both the normal and overweight categories, and 16 cases among those with obesity. Parmer County showed 8 cases in the normal BMI group, 17 in the overweight group, and 13 in the obese group. The results in this age range did not demonstrate a consistent pattern of increased cognitive dysfunction with higher BMI. For participants aged 70years and older, cognitive dysfunction was noted across all BMI categories. In Cochran County, the numbers of cases were 22 for the normal BMI group, 35 for the overweight group, and 16 for the obese group. Parmer County reported 11 cases in the normal BMI category, 34 in the overweight group, and 22 among those with obesity. While some variation was present, the highest rates in both counties were generally observed in the overweight category.
Table 3 presents the bivariate analysis of factors associated with cognitive impairment prevalence. Our analysis of sociodemographic variables revealed that advancing age was consistently associated with higher odds of cognitive impairment in both Cochran and Parmer Counties. In Cochran County, individuals aged 50–59 (OR = 1.9, 95% CI: 1.1–3.2, p = 0.017), 60–69 (OR = 2.0, 95% CI: 1.1–3.4, p = 0.018), and 70+ (OR = 4.8, 95% CI: 2.9–8.1, p = 0.001) exhibited progressively increased odds. Similarly, in Parmer County, elevated odds were observed for those aged 60–69 (OR = 3.7, 95% CI: 1.8–6.6, p = 0.001) and 70+ (OR = 6.6, 95% CI: 3.5–12.4, p = 0.001). Gender differences were also notable. Females in Parmer County had significantly lower odds of cognitive impairment compared to males (OR = 0.5, 95% CI: 0.3–0.7, p = 0.001), a trend similarly observed in Cochran County. Educational attainment emerged as an important factor, with those holding a bachelor's degree in both counties exhibiting lower odds of cognitive impairment compared to individuals without formal education, Cochran County (OR = 0.3, CI: 0.1–0.8, p = 0.011) and Parmer County (OR = 0.4, CI: 0.2–0.9, p = 0.026). Possession of healthcare insurance in Cochran County was associated with increased odds of cognitive impairment (OR = 1.8, CI: 1.2–7.1, p = 0.002). Individuals diagnosed with chronic conditions such as cardiovascular disease, diabetes, and hypertension were found to have significantly higher odds of experiencing cognitive impairment compared to those without these diseases. In Cochran County, the odds ratios for cardiovascular disease, diabetes, and hypertension were (OR = 2.7, CI: 1.7–4.4, p = 0.001), (OR = 2.2, CI: 1.5–3.2, p = 0.001), and (OR = 1.9, CI: 1.3–2.7, p = 0.001), respectively. In Parmer County, the corresponding odds ratios were (OR = 3.6, CI: 1.9–7.7, p = 0.001) for cardiovascular disease, (OR = 2.8, CI: 1.9–4.1, p = 0.001) for diabetes, and (OR = 2.5, CI: 1.7–3.7, p = 0.001) for hypertension. These findings suggest that chronic conditions are important risk factors in the development of cognitive impairment in both counties. Mental health indicators further highlighted important associations. In Parmer County, individuals with anxiety had higher odds of cognitive impairment compared to those without anxiety (OR = 1.7, CI: 1.1–2.7, p = 0.019). Depression was associated with increased odds of cognitive impairment in both counties: Cochran (OR = 1.9, CI: 1.3–2.7, p = 0.001) and Parmer (OR = 2.9, CI: 1.9–4.4, p = 0.001). Memory loss was especially strongly associated with cognitive impairment, with Cochran County showing an odds ratio of 15.9 (CI: 10.2–24.9, p = 0.001) and Parmer County an even greater odds ratio of 69.4 (CI: 28.9–166.2, p = 0.001). When examining lifestyle and behavioral factors, individuals who reported following dietary regimens had reduced odds of cognitive impairment compared to those not on a diet, Cochran County (OR = 0.9, CI: 0.9–1.0, p = 0.001) and Parmer County (OR = 0.9, CI: 0.8–0.9, p = 0.001). Use of personal medications was linked to higher odds of cognitive impairment in both Cochran (OR = 2.2, CI: 1.5–3.4, p = 0.001) and Parmer (OR = 2.5, CI: 1.5–4.4, p = 0.001) Counties. In Cochran County, those who were physically active showed increased odds of cognitive impairment compared to individuals with sedentary lifestyles (OR = 1.9, CI: 1.0–2.7, p = 0.033).
Bivariate analysis of factors associated with the prevalence of cognitive impairment.

−: indicates that data were not available due to small sample size or missing due to nonresponse; p: p-value; *p < 0.05, **p < 0.01; ref: referent group; OR: odds ratio; CI: confidence interval; %: percentage; BMI: body mass index.
Table 4 presents the results of a multivariable logistic regression analysis examining factors associated with cognitive impairment, adjusted for covariates. An adjustment was necessary in the multivariable logistic regression analysis to prevent the distortion of the relationship between an exposure variable and an outcome variable after removing the confounding effects from the model. After removing the influence of confounding factors, one can obtain a more accurate estimate of the relationship between variables, a process also known as controlling for covariates. The resulting outcome variable would provide a more precise estimate of the effect of interest and increase the statistical power of the study by detecting a significant relationship between the variables. We were interested in the effects of covariates specified by model I to IV on cognitive impairment across different age groups for Cochran County and Parmer County. Four models were developed to evaluate the impact of age on cognitive impairment while controlling for different sets of variables. Model I examined the odds of experiencing cognitive impairment among various age groups (50 and above) compared to the reference group (ages 40–49), after adjusting for BMI, gender, education, income, insurance, and race/ethnicity. In Cochran County, individuals aged 70 and older demonstrated higher odds of cognitive impairment compared to those aged 40–49 (ORδ = 2.5, CI: 1.0–5.9, p = 0.040). In Parmer County, the risk of cognitive impairment increased progressively with age: individuals aged 50–59 had an ORδ of 3.2 (CI: 1.1–9.4, p = 0.030), those aged 60–69 had an ORδ of 9.9 (CI: 3.2–30.6, p = 0.001), and those aged 70 and above had an ORδ of 16.8 (CI: 4.8–59.6, p = 0.001), all compared to the 40–49 age group. Model II focused on the odds of cognitive impairment in older age groups compared to those aged 40–49, after adjusting for chronic health conditions, including cardiovascular disease, diabetes, hypertension, cancer, and stroke. In Parmer County, individuals aged 60–69 and those 70 + exhibited significantly increased odds of cognitive impairment (ORδ = 4.7, CI: 1.6–14.2, p = 0.006 for ages 60–69; ORδ = 12.7, CI: 4.1–38.8, p = 0.001 for ages 70+) compared to the reference group. Model III evaluated cognitive impairment risk in older age groups relative to those aged 40–49, adjusting for mental health variables such as anxiety, depression, and memory loss. In Parmer County, the 60–69 age group had increased odds of cognitive impairment (ORδ = 3.6, CI: 1.6–8.3, p = 0.001). Both Cochran and Parmer Counties showed that individuals aged 70 and above had higher odds of cognitive impairment (ORδ = 2.9, CI: 1.5–5.7, p = 0.001 in Cochran; OR = 5.1, CI: 2.3–11.6, p = 0.001 in Parmer) compared to the 40–49 group after accounting for mental health conditions. Model IV investigated the odds of cognitive impairment in individuals aged 50 and above compared to the 40–49 age group, after adjusting for lifestyle and behavioral factors such as alcohol and caffeine consumption, dietary regimen, personal medication use, physical activity, and smoking. In Cochran County, those aged 70 and above had a notably higher likelihood of experiencing cognitive impairment compared to those aged 40–49 (ORδ = 6.7, CI: 2.9–15.5, p = 0.001) after controlling for these factors. The different adjustments in all four models consistently showed that age is positively correlated with cognitive impairment. These findings showed age is a key risk factor in the development of cognitive impairment.
Multivariable logistic regression analysis of factors associated with cognitive impairment after adjustment for covariates.
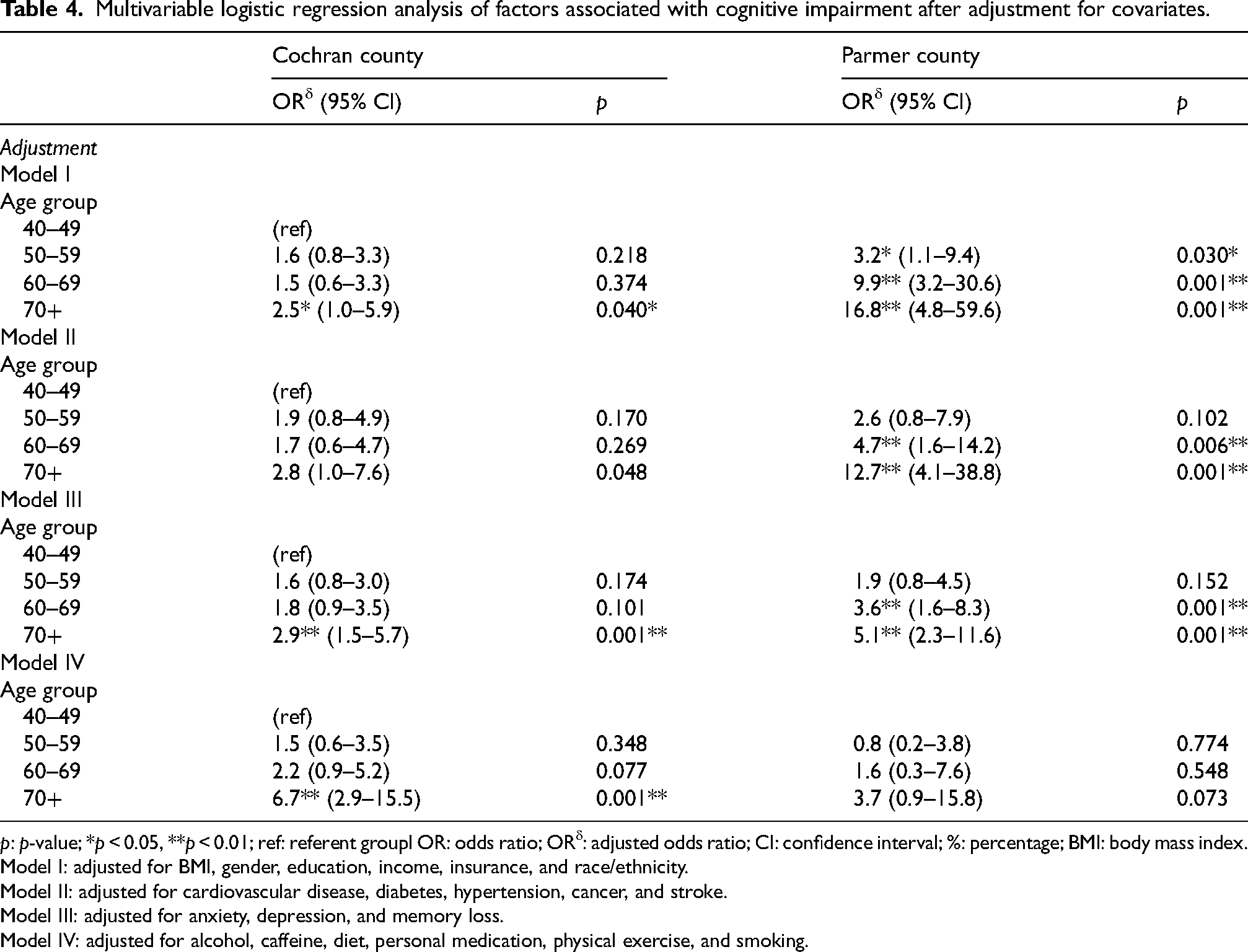
p: p-value; *p < 0.05, **p < 0.01; ref: referent groupl OR: odds ratio; ORδ: adjusted odds ratio; CI: confidence interval; %: percentage; BMI: body mass index.
Model I: adjusted for BMI, gender, education, income, insurance, and race/ethnicity.
Model II: adjusted for cardiovascular disease, diabetes, hypertension, cancer, and stroke.
Model III: adjusted for anxiety, depression, and memory loss.
Model IV: adjusted for alcohol, caffeine, diet, personal medication, physical exercise, and smoking.
Tables 5 and 6 provide comprehensive analyses of the relationship between BMI and cognitive impairment across various age groups, following adjustment for multiple covariates in Cochran and Parmer Counties, respectively. Age is a key risk factor for cognitive impairment. To explore whether the association between BMI classification and cognitive impairment changes with age, we divided the participants into four age groups (40–49 years old, 50–59 years old, 60–69 years old, and 70 + years old) and analyzed the association using four distinct models (V to VIII). Model VII showed the following findings: Cochran County, results demonstrated that individuals aged 60–69 with a BMI classified as overweight (25–29.9) had significantly reduced odds of cognitive impairment compared to those aged 40–49 with a normal BMI (18.5–24.9), when controlling for anxiety, depression, and memory loss (ORδ = 0.2, CI: 0.1–0.8, p = 0.026); Parmer County, individuals aged 60–69 identified as obese (BMI ≥ 30) exhibited lower odds of cognitive impairment relative to their counterparts aged 40–49 with a normal BMI, after adjusting for the same covariates (ORδ = 0.2, CI: 0.1–0.8, p = 0.027).
Association between BMI and cognitive impairment at different ages after adjustment for covariates, cochran county.
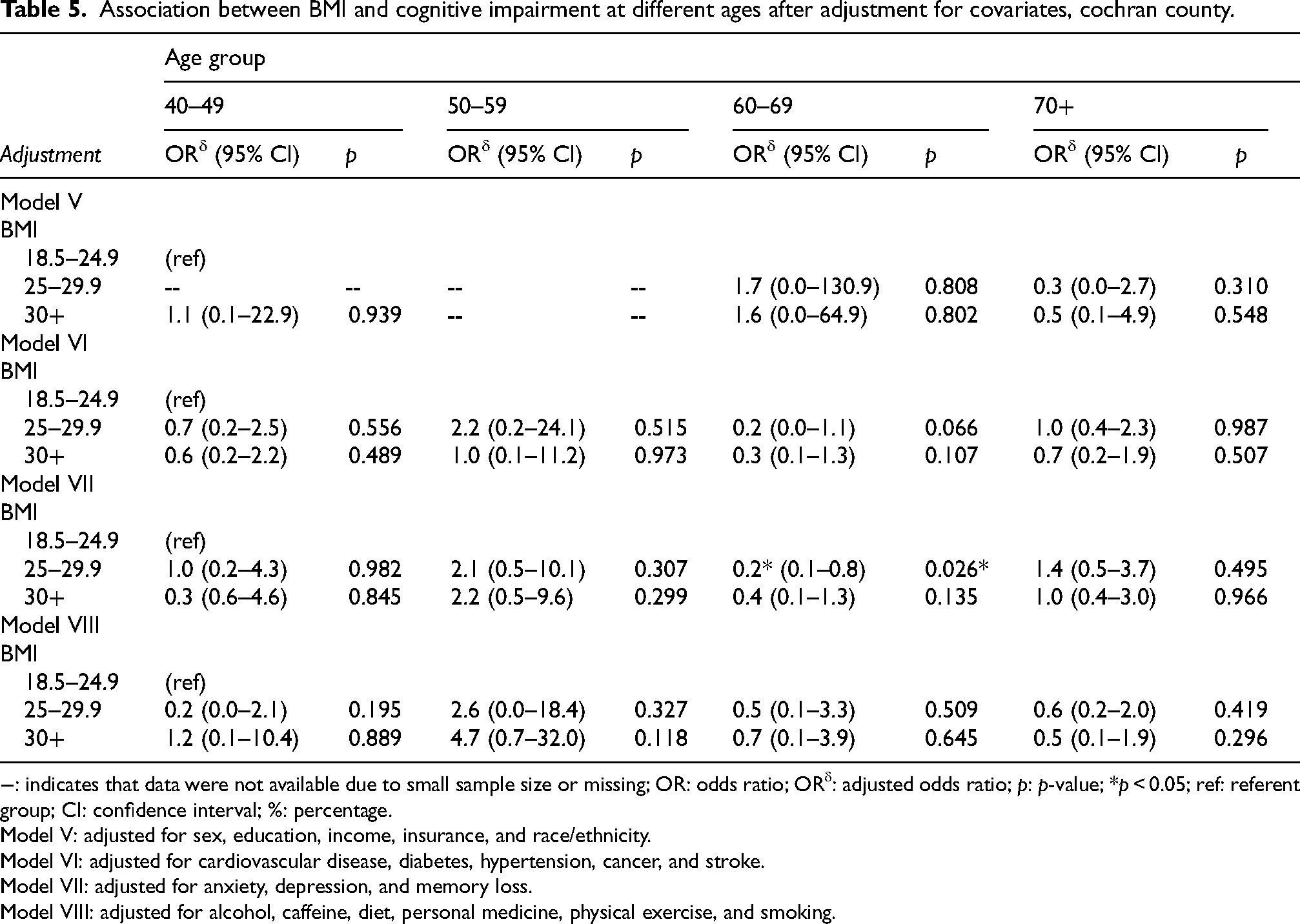
−: indicates that data were not available due to small sample size or missing; OR: odds ratio; ORδ: adjusted odds ratio; p: p-value; *p < 0.05; ref: referent group; CI: confidence interval; %: percentage.
Model V: adjusted for sex, education, income, insurance, and race/ethnicity.
Model VI: adjusted for cardiovascular disease, diabetes, hypertension, cancer, and stroke.
Model VII: adjusted for anxiety, depression, and memory loss.
Model VIII: adjusted for alcohol, caffeine, diet, personal medicine, physical exercise, and smoking.
Association between BMI and cognitive impairment at different ages after adjustment for covariates, parmer county.
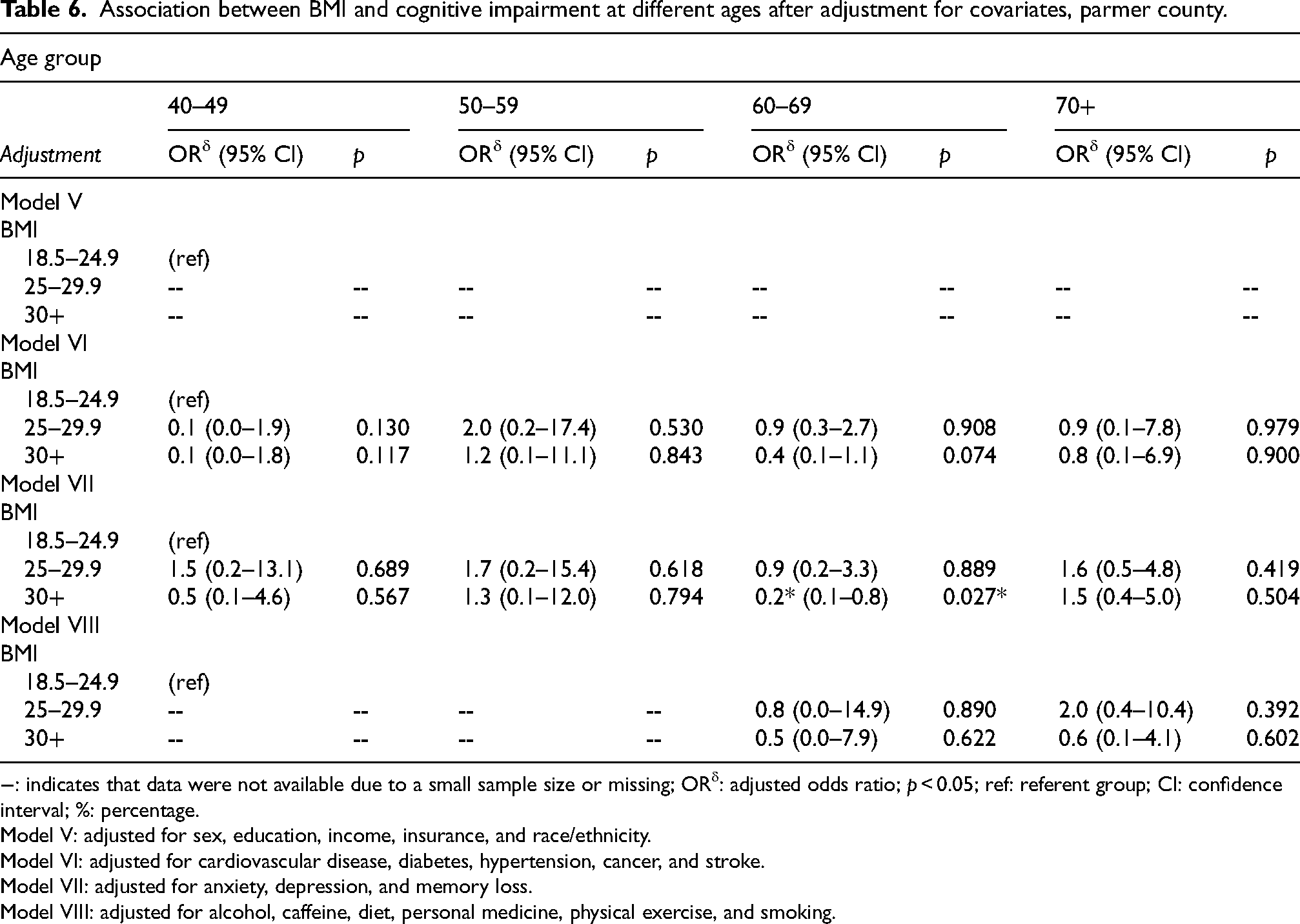
−: indicates that data were not available due to a small sample size or missing; ORδ: adjusted odds ratio; p < 0.05; ref: referent group; CI: confidence interval; %: percentage.
Model V: adjusted for sex, education, income, insurance, and race/ethnicity.
Model VI: adjusted for cardiovascular disease, diabetes, hypertension, cancer, and stroke.
Model VII: adjusted for anxiety, depression, and memory loss.
Model VIII: adjusted for alcohol, caffeine, diet, personal medicine, physical exercise, and smoking.
Active engagement in social activities can slow age-related cognitive decline, especially for the oldest-old group. Due to varying levels of social involvement, individuals who lacked social activities but became engaged in social activities at baseline showed slower rates of cognitive decline over time, Zhai et al. (2024). 30
Being underweight in the rural–dwelling participants increased the risk of cognitive impairment. Being overweight was a protective factor in rural–dwelling participants aged 65–69 years and 75–79 years, whereas being underweight was significantly associated with cognitive impairment. 26
Discussion
This study examined the influence of age and BMI on cognitive impairment among adults aged 40 years and older residing in Parmer and Cochran Counties in rural West Texas. As an initial investigation, we assessed these associations while adjusting for sociodemographic factors, chronic health conditions, health behaviors & lifestyle, and mental health status. Older adults, particularly those 70+, in both counties had increased odds of cognitive impairment compared to those aged 40–49. These associations remained strong after adjusting for various covariates. Given that elevated BMI is a well-established risk factor for numerous chronic conditions linked to cognitive impairment,8–12,22 we adjusted for multiple risk factors including sociodemographic variables, chronic diseases, health behaviors, and lifestyle factors to isolate the impact of BMI on cognitive impairment across different age groups. Cochran County data showed that people aged 60–69 who are overweight had much lower odds of cognitive impairment than those aged 40–49 with a normal BMI, after adjusting for anxiety, depression, and memory loss. Similarly, in Parmer County, individuals aged 60–69 who are obese also had reduced odds compared to younger adults with a normal BMI. Our findings contribute to a nuanced understanding of how these variables interact in shaping cognitive health among older adults in underserved rural settings.
We identified age as a significant independent risk factor for cognitive impairment, aligning with existing research that recognized aging as a primary driver of cognitive decline.2,5,7 Chronic conditions play a significant role in influencing cognitive impairment, particularly in younger individuals. However, as individuals age, especially those reaching 70 years and older, the impact of chronic conditions on cognitive impairment appears to diminish.5,15 This pattern is reflected in our findings, where the adjusted odds ratio for chronic conditions influencing cognitive impairment is lower among younger adults and increases with advancing age. These observations suggest that the effect of age alone on cognitive impairment becomes more pronounced over time, while the influence of chronic conditions becomes attenuated in older populations. This attenuation may indicate that individuals with severe chronic conditions are less likely to be represented in older age groups, possibly due to increased mortality earlier in life. As a result, those who survive to advanced ages may constitute a relatively healthier segment of the population. 15 Alternatively, the findings may simply imply that older age itself exerts a greater effect on the development of cognitive impairment. Age-related changes, such as the loss or weakening of functional abilities in nerve cells, could contribute to greater cognitive vulnerability among older adults. 1 Understanding the isolated effect of aging on cognitive impairment is essential for targeted interventions, particularly for older adults in rural communities.
In Parmer County, a larger percentage of cognitively impaired individuals had BMIs ≥25. This finding supports the established link between higher BMI and chronic conditions, which are themselves risk factors for cognitive impairment.23,24 Our study demonstrated associations between these conditions and cognitive impairment. After adjusting for chronic conditions in model VII, which adjusted for mental health diseases, we observed an inverse association between cognitive impairment and higher BMI. This suggests that higher BMI is associated with cognitive impairment. 25 A similar result was reported by Zhang et al. among urban residents in China; however, this trend was absent in rural populations, where lower BMI was significantly associated with cognitive impairment. 26 Zhang et al., 2021 26 reported that Being underweight in rural–dwelling participants increased the risk of cognitive impairment. Being overweight was a protective factor in rural–dwelling participants aged 65–69 years and 75–79 years, whereas being underweight was significantly associated with cognitive impairment. Another study conducted by Zhai et al. (2024), 30 and found that the older age is associated with higher odds of cognitive impairment in both counties, based on bivariate and multivariable analysis. Active engagement in social activities can slow age-related cognitive decline, especially for the oldest-old group. Due to varying levels of social involvement, individuals who lacked social activities but became involved in social engagement at baseline experienced slower rates of cognitive decline over time. 30
In our study, although significance was observed after adjusting for mental health conditions in model VII, no significant associations were found after controlling for sociodemographic factors (model V), chronic diseases (model VI), or health behaviors and lifestyle (model VIII). These results warrant further investigation into the relationship between BMI and cognitive impairment.
The presence of chronic conditions such as cardiovascular disease, diabetes, and hypertension was strongly associated with increased odds of cognitive impairment. These diseases can cause cerebrovascular pathology and metabolic changes that can lead to cognitive deficits. 27 Chronic hypertension is a major contributor to vascular dementia,27,28 while diabetes, according to a meta-analysis of 15 studies, significantly increases the risk of dementia. 29 Individuals with multiple comorbidities face even greater risks of developing cognitive impairment. 31 Given the obvious negative impact of these chronic conditions on cognition, we recommend prioritizing public health interventions focused on their prevention, screening, and early management, especially in underserved regions like rural West Texas, where access to primary healthcare providers may be limited. 32
Mental health indicators, such as depression and memory loss, demonstrated notable associations with the development of cognitive impairment in this study. Each of these conditions showed a significant relationship with cognitive impairment, highlighting the importance of considering mental health when evaluating cognitive decline in older adults. The strong connection between mental health disorders and cognitive impairment is well established in the literature. 33 Among older adults, depression can often present with symptoms that closely resemble those of dementia, which can complicate diagnosis and management.34,35 In addition, memory loss, though frequently regarded as a typical aspect of the aging process, may lead to delayed medical consultations. Such delays can result in missed opportunities for early intervention or treatment, limiting the effectiveness of available options. The direct clinical relationship between mental health disorders and cognitive impairment explains why these conditions are so strongly associated with cognitive decline. 36 Furthermore, factors such as the stigma surrounding mental illness can intensify its adverse effects, especially in rural settings where resources may be limited. 37 Given the influence of these mental health factors as contributors to cognitive impairment, it is essential to ensure adequate access to medical care, family support, and community-based awareness resources. These supports are critical in addressing the unique mental health challenges faced by individuals in rural communities.37,38
Our analysis revealed that individuals with cognitive impairment were less likely to adhere to prescribed dietary recommendations. This observation is consistent with earlier studies that emphasize the importance of lifestyle behaviors in both the development of chronic diseases and the onset of cognitive impairment.8,13,14 Dietary habits, particularly the consumption of antioxidant-rich foods, along with regular physical activity, have been shown to play a vital role in mitigating oxidative stress, enhancing mitochondrial function, and improving synaptic activity. These physiological benefits are associated with improved cognitive performance among older adults. Specific dietary patterns, such as the Mediterranean diet, have also been associated with a decreased risk of developing AD and dementia, as well as a slower progression of these conditions.39–41 Despite this, our findings did not show consistent or statistically significant decreases in the odds of developing cognitive impairment associated with regular physical activity, avoidance of smoking, or limiting excessive alcohol consumption. Nevertheless, the broader body of research supports the notion that maintaining a healthy lifestyle relates to reduced incidences of chronic diseases and cognitive decline.8,13,14,42 These findings highlight the critical importance of preventive strategies. Intervening before cognitive impairment develops is both more effective and more cost-efficient than reactive treatments, which are typically initiated during hospitalization when the range of intervention options becomes more limited. Therefore, prioritizing prevention and healthy lifestyle promotion is more advantageous than attempting to manage cognitive impairment after its onset. 37
The obesity paradox, which provides a clearer theoretical framework for the observed patterns in older populations. It helps explain how differential survival among individuals with higher chronic disease burdens may influence our findings. The prior evidence suggests that the influence of cardiometabolic and related risk factors on cognitive decline may attenuate with advancing age. One plausible explanation is selective survival, whereby individuals who reach older ages are more likely to have maintained relatively healthier lifestyles, resulting in lower cumulative exposure to these conditions. In addition, survivor bias may play an important role, as individuals with a high burden of chronic disease may be less likely to survive into older age and thus are underrepresented in later-life assessments. This phenomenon provides a useful framework for interpreting the observed patterns and is consistent with explanations proposed for the obesity paradox, where risk associations appear diminished or altered in older populations.
Strengths
This study is the first to examine the effect of age and BMI on cognitive impairment after adjusting for and controlling sociodemographic, chronic disease, mental health conditions, and health behavioral & lifestyle factors in rural West Texan adults aged 40 and above. Approved by the TTUHSC IRB, the study employed rigorous proportion tests and multivariable logistic regression to isolate the independent impact of age, BMI, and age-BMI on cognitive impairment. The findings inform public health stakeholders on where to tailor interventions to ensure effective results and improve health outcomes. We used data from Project FRONTIER's ongoing data collection to contribute valuable insights into healthy aging in rural West Texas.
Limitations
This was a cross-sectional study, which did not offer the possibility of establishing a causal relationship between risk factors and outcomes, and longitudinal tracking was not performed. The study relied on convenience sampling from Project FRONTIER, which may introduce bias. Data was collected using binary-response questionnaires, limiting in-depth exploration of participants’ conditions. The disproportionate number of participants in the sample may be due to females being more health-conscious than male participants. The cognitive impairment is a self-reported binary response (yes or no). There was no standardized assessment like the Montreal Cognitive Assessment or Mini-Mental State Examination used to measure cognitive impairment. The study population was individuals who attended hospitals in both counties for their regular health checkups and may not reflect the population distribution in the counties. Cross-tabulations were used to count the number of responses that meet specific characteristics in each cell. Some cell frequencies or responses are small in a crosstab analysis, so the chi-squared test may not be appropriate because the expected cell frequencies may be less than 5. Certain odds ratios for predicting cognitive impairment are high because the sample size is not large enough. A few confidence intervals are extremely wide due to sparse data in some subgroups, making the estimates unstable. Due to missing data, with no records or small cell responses for income or insurance, the data were limited. Therefore, the results for BMI with cognitive impairment across different age groups by Model V were partially available for Cochran County and completely unavailable for Parmer County. The protective association of overweight with cognitive impairment was not observed in Model V but observed in Models VI to VII.
The project FRONTIER continues to collect data from rural West Texas counties. In the future, when more data becomes available, there will be more Hispanic participants in the sample, and the study findings can then be generalized to similar demographic regions across the nation.
Conclusions
Older age remains a primary risk factor for cognitive impairment. As individuals advance in age, their likelihood of developing cognitive impairment significantly increases. This increased risk persists even after accounting for other potential risk factors. These findings underscore the importance of developing targeted interventions specifically for older adults living in rural areas, who may be particularly vulnerable to cognitive decline. Individuals with a BMI over 25, categorized as overweight or obese, typically exhibit higher odds of experiencing cognitive impairment. This association may be attributed to the presence of additional chronic conditions commonly found in these groups, which are also recognized as contributing risk factors for cognitive impairment. However, after adjusting for and controlling the influence of chronic comorbidities, the data did not reveal a consistent association between cognitive impairment and elevated BMI alone. Notably, among overweight and obese seniors, the odds of cognitive impairment were lower, suggesting that a higher BMI by itself might have an effect against cognitive decline in this population. The study identified risk factors associated with the prevalence of cognitive impairment among adults in rural West Texas after adjusting for covariates. It also showed the association between BMI and cognitive impairment at different ages in the rural West Texas counties of Cochran and Parmer. The findings from this study will advance fundamental knowledge in epidemiology and in the treatment of AD or dementia.
Footnotes
Acknowledgements
The authors express their sincere gratitude to the researchers, staff, and participants involved in Project FRONTIER for their ongoing commitment to data collection and their invaluable contributions to this study. Their dedication and efforts were instrumental in advancing our understanding of cognitive impairment in rural West Texas. Special thanks are extended to the Texas Tech University Health Sciences Center (TTUHSC) for their support in approving the Institutional Review Board (IRB) application, granting access to the Project FRONTIER database covering rural West Texas counties, and providing essential information. This support greatly enhanced the quality of the statistical data analysis and the presentation of the study's findings.
Ethical considerations
The study protocol underwent thorough evaluation and received approval from the Institutional Review Board (IRB) of the Texas Tech University Health Sciences Center (TTUHSC). Specifically, Project FRONTIER was granted IRB approval on January 30, 2006, under the IRB number L06–028. This process ensured that all research activities complied with established ethical guidelines and protected the rights and welfare of study participants.
Consent to participate
This study used deidentified data obtained from individuals who participated in Project FRONTIER. Each participant provided informed consent at the time of data collection, ensuring their voluntary involvement in the research process. The use of deidentified information safeguarded participant confidentiality and complied with ethical standards established by the overseeing Institutional Review Board. All data collection procedures adhered strictly to protocols designed to protect the rights and privacy of study subjects.
Consent for publication
Not applicable
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is partially supported by Arizona State University Grant P001500.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are not readily available upon request. This restriction is in place because the institution upholds rigorous ethical standards and is firmly committed to protecting the confidentiality of all study participants. We kindly request the readers’ understanding and respect regarding these ethical considerations, as maintaining participant privacy is of utmost importance to our research practices.