
Abstract
Background
Resilience is an important positive construct supporting people with dementia; however, validated self-report instruments for this population remain limited, and no Turkish version is currently available.
Objective
This study aimed to adapt the Bangor Dementia Resilience Scale (BDRS) into Turkish and to evaluate its psychometric properties in individuals with mild cognitive impairment (MCI) and early-stage dementia.
Methods
This cross-sectional psychometric study included 118 individuals with MCI or early-stage dementia. The translation and cultural adaptation process followed established guidelines. Structural validity was examined using exploratory factor analysis (EFA). Convergent validity was assessed using Pearson correlations between the Turkish version of the BDRS (T-BDRS) scores and quality of life (QoL-AD), as well as clinical variables including Mini-Mental State Examination, Neuropsychiatric Inventory, and Katz Activities of Daily Living. Reliability was evaluated using Cronbach's alpha, McDonald's omega, item–total correlations, and test–retest reliability (n = 30).
Results
EFA supported a five-factor structure explaining 68.32% of the total variance. The internal consistency of the total scale was excellent (Cronbach's α = 0.946; ω = 0.946). Item–total correlations ranged from 0.604 to 0.787. Test–retest reliability demonstrated excellent stability (ICC = 0.993). Convergent validity was supported by a strong positive correlation with QoL-AD (r = 0.819, 95% CI: 0.744–0.872, p < 0.001).
Conclusions
The T-BDRS demonstrated satisfactory validity and reliability for assessing resilience in individuals with MCI and early-stage dementia. It represents a promising tool for research and clinical practice, supporting the assessment of positive psychosocial outcomes in dementia care.
Introduction
With the global aging of the population, dementia has become one of the most significant international public health challenges of the twenty-first century. Currently, more than 57 million people worldwide are living with dementia, a number projected to rise to 75 million by 2030 and 132 million by 2050. 1 Dementia is also recognized as one of the leading causes of death globally. 2 In Turkey, the prevalence of Alzheimer's disease among individuals aged 65 years and older is reported as 5.5%, 3 and the proportion of older adults who died due to Alzheimer's disease is 3.2%. 4 These data highlight the necessity of conducting methodologically robust research involving people living with dementia (PwD) in Turkey, in line with global efforts.
Research on psychosocial interventions for PwD has predominantly focused on deficit-oriented outcomes, such as anxiety, depression, agitation, and reduced quality of life. 5 However, recent perspectives emphasize the importance of positive constructs, including well-being, confidence, health, social participation, and human rights.6,7 In this regard, resilience has emerged as a key concept reflecting an individual's capacity to adapt to adversity and maintain psychological well-being.
Resilience is commonly defined as a dynamic process involving effective adaptation to stressors through the use of internal and external resources. In dementia, resilience is closely linked to the concept of “living well” and plays a critical role in supporting individuals’ ability to cope with cognitive decline and maintain engagement in daily life.8–10
Despite increasing interest in resilience, measurement tools specifically designed for PwD remain limited. While resilience scales exist for other populations, research in dementia has largely focused on caregivers, with relatively few studies directly assessing resilience in PwD.11–13 This highlights the need for valid and reliable self-report instruments that capture resilience from the perspective of PwD.
In this context, acknowledging the perspectives of PwD is essential in dementia research. Supporting self-expression is a cornerstone of person-centered care, and despite potential challenges related to cognitive impairment, PwD can provide meaningful subjective data when appropriate methods are used. 13 In the present study, these challenges were addressed by including only people with mild cognitive impairment (PwMCI) or people with early-stage dementia, using validated and comprehensible instruments, and providing researcher support during data collection to ensure accurate and reliable responses.
The Bangor Dementia Resilience Scale (BDRS) is a recently developed self-report instrument designed to assess resilience in PwD. It is based on a multidimensional understanding of resilience and focuses on positive adaptation, coping ability, and engagement in daily life. 14 The scale has demonstrated promising psychometric properties in its original development study.
To date, no validated Turkish instrument exists to assess resilience in PwD and PwMCI. Therefore, the aim of this study was to adapt the BDRS into Turkish and evaluate its psychometric properties, including validity and reliability, in individuals with MCI and early-stage dementia. We hypothesized that the Turkish version of the BDRS (T-BDRS) would demonstrate satisfactory internal consistency, a coherent factor structure, and meaningful associations with related constructs.
Methods
Design
This was a cross-sectional psychometric study with repeated measurements conducted two weeks apart to assess test-retest reliability. The cross-cultural adaptation of the BDRS followed established international guidelines for the translation and cultural adaptation of self-reported outcome measures. 15 The resulting T-BDRS is provided in Supplemental Material 1. In addition, the procedures and reporting were aligned with the COSMIN Reporting Guideline (see Supplemental Material 2) for studies on measurement properties of patient-reported outcome measures, particularly with respect to content validity and cross-cultural validity. 16
Participants
This study was conducted between April 2025 and January 2026 at the dementia outpatient clinic of a university hospital in western Turkey. Participants were individuals diagnosed with either MCI or early-stage dementia by a neurologist, based on DSM-V criteria and documented in their medical records. To ensure sufficient cognitive capacity for reliable self-report, only participants with a Mini-Mental State Examination (MMSE) score of 23 or higher and a Clinical Dementia Rating (CDR) of 0.5 or 1 were included. MMSE and CDR scores were extracted from participants’ medical records and used to support clinical classification rather than as the sole diagnostic criteria. Participants with MCI had a documented clinical diagnosis supported by cognitive screening results indicating mild impairment without meeting criteria for dementia, whereas participants with early-stage dementia met the clinical criteria for dementia and were classified accordingly.
We used a purposive sampling method, a type of non-probability sampling. Based on the recommendation of recruiting 5–10 participants per scale item, the target sample size was calculated as 95–190 individuals for the 19-item BDRS. 17 A total of 121 participants were reached during the study period. However, three participants withdrew before completing the study procedures, resulting in a final sample of 118 PwMCI or early-stage dementia.
Instruments
This study was conducted utilizing paper-based scales administered face-to-face. Data were collected using a descriptive and clinical characteristics form, the T-BDRS, and the Quality of Life in Alzheimer's Disease (QoL-AD) Scale to assess resilience and quality of life. All measures were available in standard printed format and were completed with researcher support when required. In keeping with the Dementia Engagement and Empowerment Project Guide 18 on writing dementia-friendly information, we utilized clear, simple, and concise language to maximize comprehension. When necessary, items were read aloud to participants to support understanding, and responses were recorded by the researcher without interpretation. 18
Descriptive and clinical characteristics form
The 13-item form, developed by the researchers based on the literature, 19 captures the demographic and clinical characteristics of participants. Cognitive status was assessed via the MMSE, neuropsychiatric symptoms were evaluated using the Neuropsychiatric Inventory (NPI), and functional independence was measured utilizing the Katz Index of Activities of Daily Living (Katz ADL), based on data extracted from participants’ medical records. All these instruments have been validated for use in Turkish populations and demonstrated acceptable to good internal consistency in previous studies.20–22 The study by Güngen et al. (2002) demonstrated that the standardized MMSE is a valid and reliable instrument for the diagnosis of mild dementia in the Turkish population. The NPI is a 12-item scale with total scores ranging from 12 to 144. 21 Cronbach's alpha was 0.79 for the Turkish version of the NPI. 21 Arik et al. (2015) demonstrated that the Katz ADL is a valid and reliable instrument for assessing functional status in Turkish older adults, with good internal consistency (Cronbach's α = 0.84).
BDRS
The scale was developed in 2024 by Windle and colleagues to assess resilience in PwD. 14 The scale includes 19 items rated on a 5-point Likert scale, from 1 (strongly disagree) to 5 (strongly agree). The BDRS is intended to identify the strengths of PwD, inform person-centered care planning, and guide supportive interventions. Total scores were calculated by averaging the subscale scores, yielding a possible range of 5–25. Exploratory factor analysis (EFA) supported a five-factor structure (Outlook, Adaptation, Acceptance, Community and Peer Support, and Family and Friends), explaining 46.17% of the total variance, and the scale's Cronbach's alpha was 0.85. 14
QoL-AD
The QoL-AD was originally developed in 1999 by Logsdon, Gibbons, McCurry, and Teri. It consists of 13 items assessing patients’ QoL across multiple domains: health status, energy level, emotional state, living environment, memory, family and marital relationships, friendships, self-perception, ability to perform household responsibilities, engagement in leisure activities, financial situation, and overall life satisfaction. 23 The items are simple and clear, allowing individuals with cognitive impairment to respond reliably. Self-report and proxy assessments are scored independently. The Turkish version was validated by Akpınar Söylemez et al. (2012), 24 with a Cronbach's alpha of 0.84. In the present study, only the self- report of PwD on the scale was used to examine convergent validity.
Data collection and procedure
Data were collected from PwD or PwMCI who consented to participate using the descriptive and clinical characteristics form, the T-BDRS, and the QoL-AD scale. Completion of the forms took approximately 20 min. Prior to the main data collection, we conducted a pilot application with three PwD to evaluate the feasibility of the data collection procedure. In this pilot phase, no changes were made to the wording, content, or response options of the scales. The pilot revealed that the question-and-answer administration format was appropriate for the target population, and therefore the same procedure was used in the main study. Data from the pilot participants were not included in the psychometric analyses. Although the scale is self-reported, in the pilot study, the researcher read the questions aloud at the participants’ request, and researchers documented the participants’ responses. Following the pilot study, formal data collection for the main study was initiated and continued according to the same standardized procedure.
Translation/adaptation process
The adaptation process was carried out in accordance with the Beaton 2000 criteria. 15 The first step for language validity (Stage I) was the translation of the scale from English to Turkish independently by four study researchers (BAS, MAA, EÖ, and HE). In Stage II, the second step of adaptation process, the results from translating the scales were synthesized. The four researchers held a face-to-face meeting regarding the scale translations and subsequently compared the translated English scale with the original. The third step of adaptation (Stage III) was back translation. A linguist, who had never previously read the English version and possessed a deep understanding of both languages and cultures, conducted the back-translation of the scale from Turkish to English. We sought expert committee opinions in the fourth stage of the adaptation (Stage IV). Content validity was approved by seven experts (five academic nurses and two neurology specialist physicians) who were asked to evaluate the scale for language and content. We evaluated the pre-application test in the fifth step of the adaptation (Stage V). To test the clarity and comprehensibility of the items, a scale was given to a small group representing the sample. The researchers administered the scale to a group of ten PwD. Each of the items in the pilot study was found to be understandable, and the validity and reliability study continued with the data collection. It took participants approximately 15 min to complete the instrument. In the last step of the adaptation (Stage VI), submission of documents to the Professor Windle for evaluation of the adaptation process’ was carried out. Lastly, the adaptation process was verified by the owner of the scale.
Statistical analysis
Data were analyzed using SPSS version 31. Descriptive statistics were reported as frequencies, percentages, means, and standard deviations. The psychometric evaluation of the T-BDRS focused on structural validity, convergent validity, and reliability, in line with COSMIN recommendations for studies on measurement properties.
Structural validity
Structural validity was examined using EFA with principal axis factoring and Varimax rotation. Although the original scale has an established factor structure, EFA was preferred due to the cross-cultural adaptation process and the possibility of variation in factor structure across different populations. This approach is consistent with COSMIN recommendations supporting exploratory methods in the early stages of scale adaptation. The suitability of the data for factor analysis was assessed using the Kaiser–Meyer–Olkin (KMO) measure and Bartlett's test of sphericity.
Convergent validity
Convergent validity was assessed by examining the relationship between T-BDRS scores and quality of life, measured via the QoL-AD scale, using Pearson correlation analysis. In addition, correlations between T-BDRS scores and clinical variables (MMSE, NPI, and the Katz ADL) were examined to provide further support for construct validity.
Reliability
Reliability was evaluated through internal consistency, item analysis, and test–retest reliability. 25 Internal consistency was assessed using Cronbach's alpha and McDonald's omega coefficients. 26 Mean inter-item correlations were calculated to evaluate item homogeneity. Item analysis was conducted using corrected item–total correlations to determine the contribution of each item to the overall scale.
Test–retest reliability was assessed using the intraclass correlation coefficient (ICC) with a two-way mixed-effects model, single-measure consistency. For the test–retest procedure, which is typically recommended to be conducted within a 2–6 week interval to minimize recall bias while ensuring stability of the construct, we applied a 2-week interval. 27 ICC values were interpreted according to established guidelines, with values above 0.90 indicating excellent reliability.
Results
Participant characteristics
A total of 118 participants were included in the study. Of these, 60.2% were female, and 84.7% were married. The majority reported that their income was equal to their expenses (76.3%), and 78.0% had at least one chronic disease. Regarding cognitive status, 69.5% had MCI and 30.5% had early-stage dementia. The mean age was 67.93 ± 8.49 years, and the mean time since diagnosis was 19.17 ± 14.95 months. The mean T-BDRS total score was 17.32 ± 2.86 (Table 1).
Descriptive and clinical characteristics of the sample (n = 118).
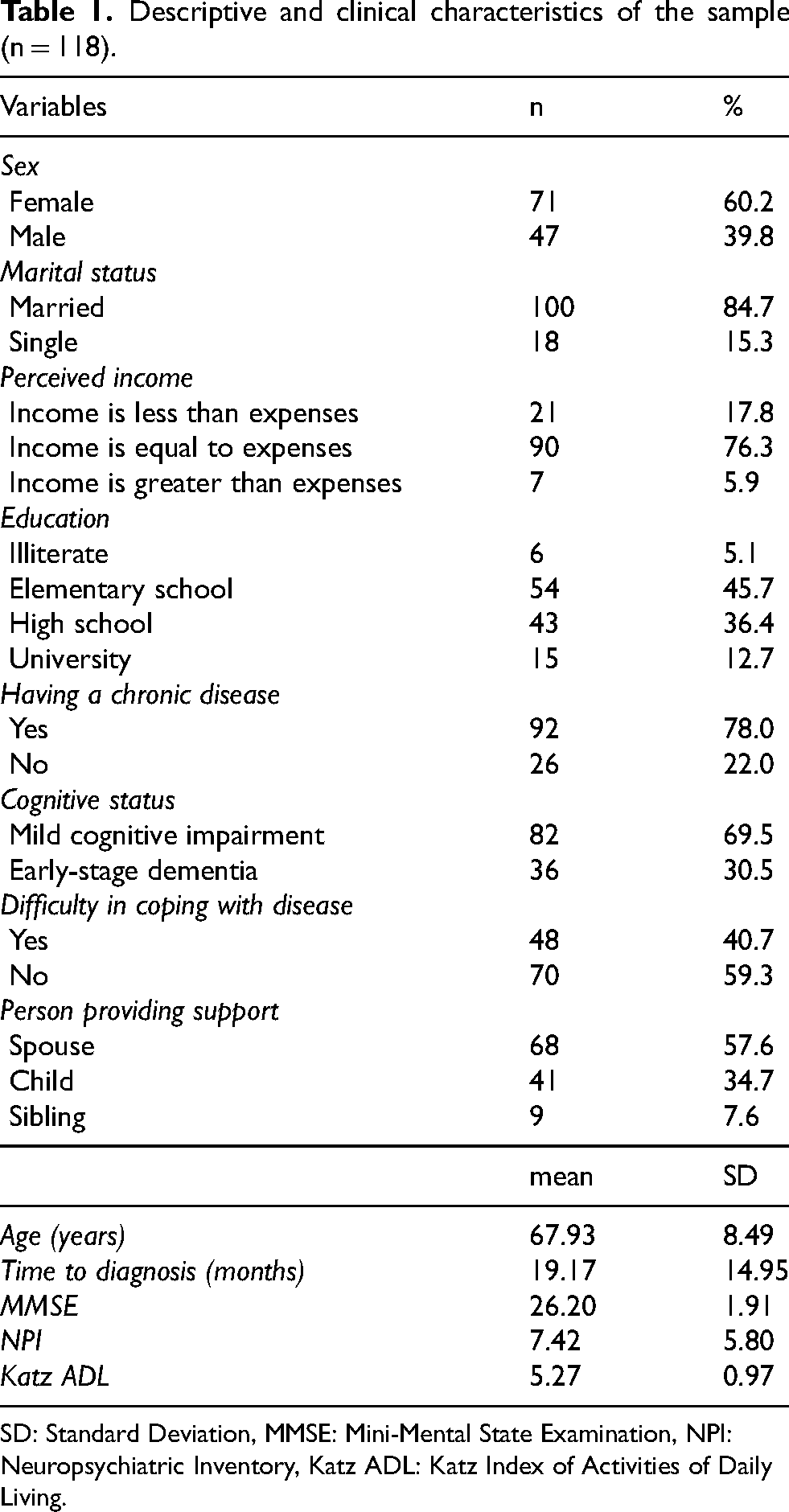
SD: Standard Deviation, MMSE: Mini-Mental State Examination, NPI: Neuropsychiatric Inventory, Katz ADL: Katz Index of Activities of Daily Living.
Translation and content validity
The translation and cultural adaptation process demonstrated that the items retained their original meaning. All items were evaluated by an expert panel consisting of academic nurses and neurology specialists. The item-level content validity index (I-CVI) and scale-level content validity index (S-CVI) were both 1.00, indicating excellent content validity. No modifications were required following expert evaluation or pilot testing, and participants reported that the items were clear and understandable.
Structural validity (EFA)
The suitability of the data for factor analysis was confirmed by a KMO value of 0.837 and a significant Bartlett's test of sphericity (χ2 = 1749.095, p < 0.001). EFA revealed a five-factor structure consistent with the original scale. These five factors explained 68.32% of the total variance. Factor loadings ranged from 0.36 to 0.87 across domains (Table 2).
Exploratory factor analysis for T-BDRS (n = 118).
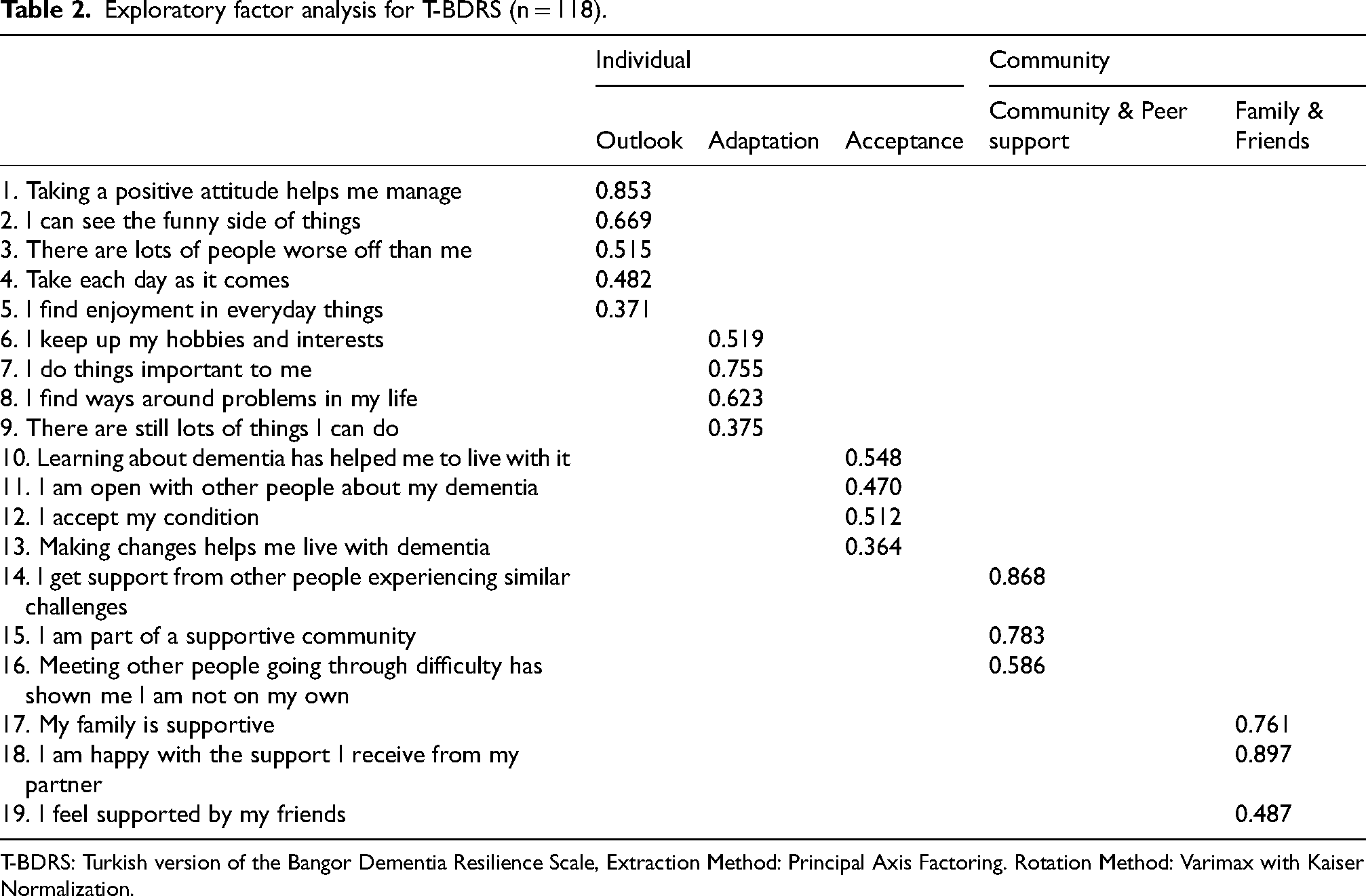
T-BDRS: Turkish version of the Bangor Dementia Resilience Scale, Extraction Method: Principal Axis Factoring. Rotation Method: Varimax with Kaiser Normalization.
Convergent validity
Convergent validity was assessed by examining correlations between T-BDRS scores and QoL-AD. A strong positive correlation was observed between T-BDRS and QoL-AD (r = 0.819, 95% CI: 0.744–0.872, p < 0.001), indicating that higher resilience was associated with better QoL.
In addition, T-BDRS scores showed moderate correlations with clinical variables. Resilience was negatively correlated with age (r = −0.423, 95% CI: −0.567 to −0.259, p < 0.001) and time since diagnosis (r = −0.449, 95% CI: −0.587 to −0.289, p < 0.001). Positive correlations were found with cognitive function (MMSE; r = 0.494, 95% CI: 0.340–0.622, p < 0.001) and functional status (Katz ADL; r = 0.601, 95% CI: 0.466–0.708, p < 0.001). NPI were negatively correlated with resilience (r = −0.415, 95% CI: −0.561 to −0.249, p < 0.001). These findings support the construct validity of the scale.
Reliability
Internal consistency
The internal consistency of the T-BDRS was high, with Cronbach's alpha and McDonald's omega both equal to 0.946 for the total scale. Subscale alpha values ranged from 0.819 to 0.883 (Table 3). Mean inter-item correlations ranged between 0.57 and 0.66 across subscales, indicating good item homogeneity without excessive redundancy. Corrected item–total correlations ranged from 0.604 to 0.787, indicating that all items contributed meaningfully to the total score (Table 4).
Reliability analysis results of the T-BDRS (n = 118).
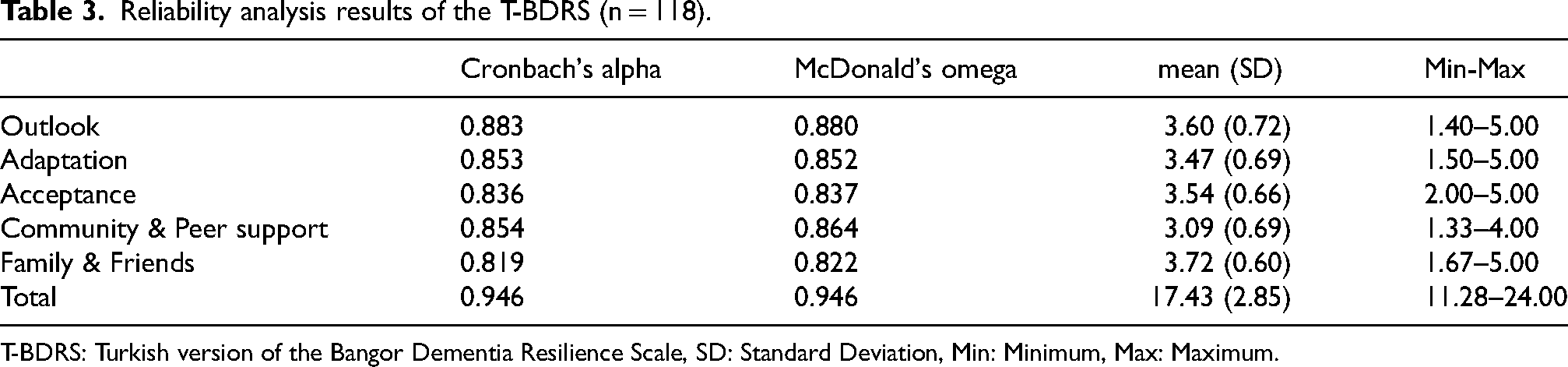
T-BDRS: Turkish version of the Bangor Dementia Resilience Scale, SD: Standard Deviation, Min: Minimum, Max: Maximum.
Item-subscale total score for T-BDRS (n = 118).
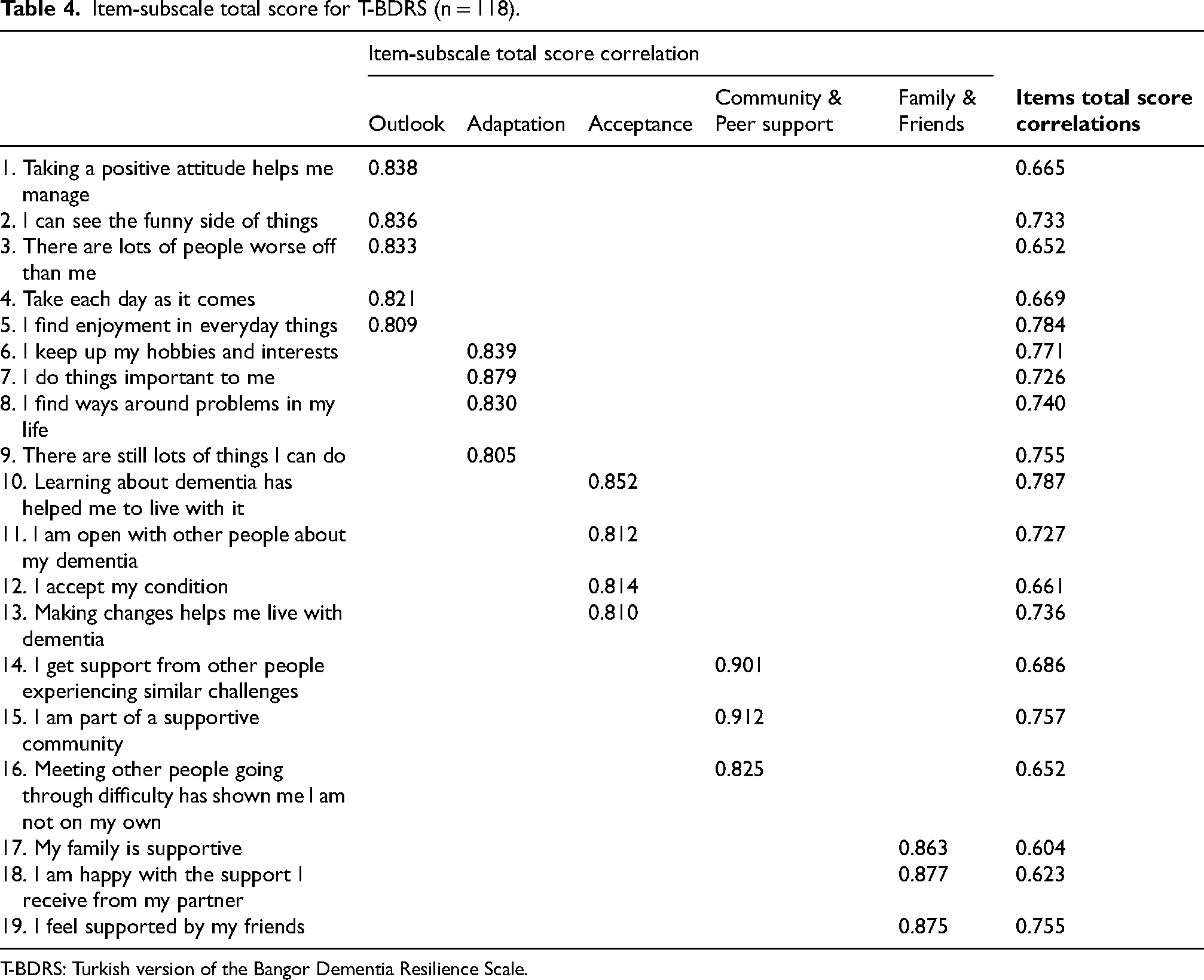
T-BDRS: Turkish version of the Bangor Dementia Resilience Scale.
Test–retest reliability
Test–retest reliability was assessed in a subsample of 30 participants over a two-week interval. The ICC for the total scale was 0.993 (95% CI: 0.986–0.997), indicating excellent temporal stability. ICC values for subscales ranged from 0.839 to 0.997 (Table 5).
Test-retest reliability results of the T-BDRS and its subscales (n = 30).
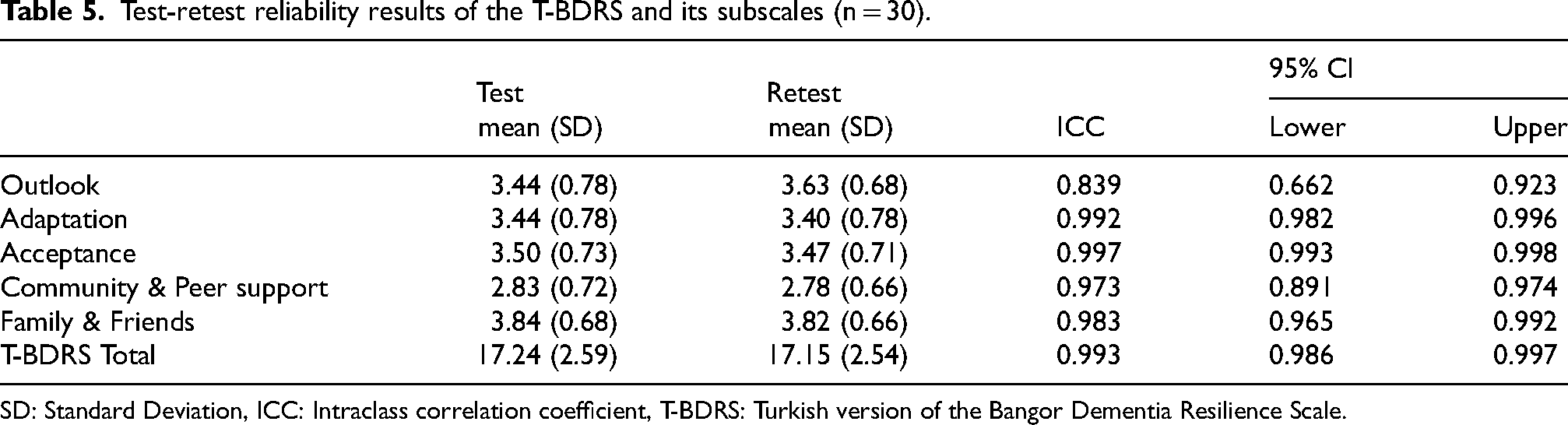
SD: Standard Deviation, ICC: Intraclass correlation coefficient, T-BDRS: Turkish version of the Bangor Dementia Resilience Scale.
Discussion
Contemporary dementia research increasingly emphasizes outcome measures that capture positive constructs and individual strengths rather than deficits. Resilience is a key construct in achieving this. This study adapted the BDRS into Turkish and evaluated its psychometric properties in PwMCI and people with early-stage dementia. Overall, the findings suggest that the T-BDRS demonstrates satisfactory internal consistency, a coherent factor structure, and meaningful associations with related constructs, supporting its validity in this population. As the prevalence of dementia increases, integrating resilience into dementia care is becoming vital. 13 For this reason, this tool represents a promising and relevant approach for dementia care research and practice.
The scale, consisting of 19 items, is concise and user-friendly, making it easy for PwD to complete and understand. In addition to this, the scale items convey positive messages to PwD, helping them notice the positive effects of resilience on themselves, and hence their caregivers will already gain awareness about resilience. Surely, the resilience levels of PwD cannot be reduced to a single number or statistic, but they can be made more measurable and improved by health care providers.
The EFA revealed the original five-factor solution, explaining 68.32% of the total variance, which is notably higher than the 46.17% reported in the original scale development study. 14 This higher variance explained may suggest a relatively strong factor structure in the Turkish sample, indicating that the items function cohesively within this cultural context.
This difference in explained variance may partly be attributable to sample characteristics, as the present sample had a relatively high mean MMSE score, suggesting preserved cognitive functioning, whereas MMSE data were not reported in the original study. In the current study, participation was restricted to PwMCI and people with early-stage dementia, defined by an MMSE score of 23 or higher and CDR scores of 0.5 or 1. This criterion reflects a deliberate methodological decision aligned with the self-report nature of the BDRS, as adequate cognitive capacity is essential for understanding scale items and providing reliable subjective responses. The findings demonstrate that individuals in the early stages of cognitive impairment are able to engage with resilience-related self-report measures. Although the original scale has an established factor structure, EFA was conducted in this study as part of the cross-cultural adaptation process. It is well documented that factor structures may vary across cultural contexts, and therefore, re-examination of the structure is recommended in newly adapted versions.15,16 Furthermore, the present study included a specific sample consisting of PwMCI and people with early-stage dementia, which may influence how scale items are interpreted. In line with COSMIN recommendations, exploratory approaches are considered appropriate in the early stages of scale adaptation. However, the confirmatory factor analysis (CFA) was not performed due to the relatively limited sample size. Future studies with larger samples are recommended to confirm the factor structure using the CFA. Therefore, the structural validity findings should be interpreted as preliminary until confirmed by future studies via the CFA.
Convergent validity was supported by a strong positive correlation between resilience and quality of life, as measured by the QoL-AD. The magnitude of the correlation (r = 0.819, 95% CI: 0.744–0.872) indicates that higher dementia resilience is closely associated with better quality of life among people with early-stage dementia and PwMCI.28,29 This finding is consistent with the theoretical framework of dementia resilience, which emphasizes the individual's capacity to maintain psychological well-being and functional adaptation despite cognitive decline. 29 A longer time to diagnosis was significantly associated with lower dementia resilience, suggesting that delays in receiving a formal diagnosis may negatively affect individuals’ ability to adapt to the disease. Early diagnosis may facilitate timely access to medical care, psychosocial support, and coping strategies, thereby strengthening resilience. 30 This finding underscores the importance of early recognition and diagnosis of dementia in promoting adaptive outcomes. Cognitive function, as measured by the MMSE, was positively associated with dementia resilience, indicating that individuals who maintain greater cognition exhibit higher resilience. Preserved cognition may enhance autonomy, self-efficacy, and engagement in daily life, all of which are key components of resilience. Interventions aimed at improving cognition and quality of life may therefore play a critical role in enhancing resilience among PwD and PwMCI.
In the current study, both Cronbach's alpha and McDonald's omega coefficients for the total scale were 0.95, indicating excellent internal consistency. In contrast, the original scale development study reported Cronbach's alpha of 0.85. While the original study reported subscale Cronbach's alpha values ranging from 0.62 to 0.78, 14 the present study demonstrated higher reliability across all subscales, with alpha coefficients ranging from 0.82 to 0.88. These findings indicate high internal consistency according to commonly accepted reliability thresholds. Although Cronbach's alpha was high, the mean inter-item correlation values remained below commonly cited redundancy thresholds (e.g., 0.70), suggesting that the high reliability was not attributable to excessive item overlap. The higher reliability coefficients observed in the present study may reflect sample characteristics, item homogeneity, differences in data collection methods, or factors related to the cultural adaptation process. Although the values observed in this study were satisfactory, future research may consider examining the possibility of item reduction to improve the efficiency of the scale while maintaining its psychometric robustness. Item–total correlations were above commonly accepted thresholds (e.g., ≥0.30), suggesting that all items contributed meaningfully to the overall construct.28,29
The T-BDRS demonstrated high temporal stability, as indicated by excellent single-measure ICC for the total score and all subscales. These ICC values indicate strong agreement between test and retest administrations, supporting the stability of the construct over time. Such findings are consistent with validation studies of psychological scales, which emphasize the importance of high test-retest reliability in establishing measurement consistency across repeated administrations.31,32
The content validity indices in this study were found to be very high. While such values indicate strong agreement among experts, they may also reflect the composition of the expert panel, which primarily included clinicians and academic professionals familiar with dementia care. Although this supports the clinical relevance and clarity of the items, future studies may benefit from including experts with specific experience in psychometric scale development and from applying additional indices, such as modified kappa, to further strengthen the evaluation of content validity.
Strengths and limitations
One of the key strengths of this study is that resilience data were obtained directly from people with early-stage dementia or PwMCI. The findings indicate that people with early-stage dementia or PwMCI were able to meaningfully engage with the scale items, supporting the feasibility of self-reported resilience assessment in this population. Another important strength is the inclusion of test-retest reliability analysis, which was not reported in the original scale development study. The excellent ICC values observed between test and retest administrations provide additional evidence for the reliability of the Turkish version of the scale.
Despite these strengths, several limitations should be acknowledged. First, data collection was conducted in a hospital-based outpatient clinic, which may have influenced participants’ responses; resilience levels might differ if assessed in home or community settings. Second, the sample consisted solely of people with early-stage dementia or PwMCI, which limits the generalizability of the findings to individuals in later stages of dementia. Future studies are recommended to replicate the validation process in individuals with lower MMSE scores than those included in the present study. Although people with early-stage dementia and PwMCI were analyzed together due to sample size considerations, we clearly report the number in each diagnostic group. Future studies with larger samples should examine measurement invariance and psychometric properties separately in MCI and dementia groups. Additionally, although a target sample size was defined, recruitment of eligible participants took longer than anticipated, and the intended sample size could not be fully achieved within the predefined data collection period. Finally, the CFA was not conducted due to the limited sample size; thus, the structural validity findings should be considered preliminary. Future studies with larger and more diverse samples are needed to further validate the scale and examine its measurement invariance across different groups.
Conclusion
The T-BDRS demonstrated satisfactory psychometric properties, including good structural validity, strong internal consistency, and evidence of convergent validity in individuals with MCI and early-stage dementia. These findings suggest that the T-BDRS is a useful instrument for assessing resilience in this population and may support both clinical practice and research. As this is the first language adaptation of the BDRS, further validation in larger and more diverse samples is recommended. In addition, cross-cultural comparisons with other language versions may provide valuable insights into the generalizability of the scale. However, as the CFA was not conducted, the structural validity findings should be interpreted as preliminary. Future studies are needed to confirm the factor structure and further evaluate the measurement properties of the scale.
Supplemental Material
sj-pdf-1-alr-10.1177_25424823261461527 - Supplemental material for Psychometric evaluation of the Turkish version of the Bangor Dementia Resilience Scale
Supplemental material, sj-pdf-1-alr-10.1177_25424823261461527 for Psychometric evaluation of the Turkish version of the Bangor Dementia Resilience Scale by Burcu Akpınar Söylemez, Merve Aliye Akyol, Ecem Özgül, Hasret Erden, Özlem Küçükgüçlü, Marianna Tsatali, Görsev Yener and Birgit Teichmann in Journal of Alzheimer's Disease Reports
Supplemental Material
sj-pdf-2-alr-10.1177_25424823261461527 - Supplemental material for Psychometric evaluation of the Turkish version of the Bangor Dementia Resilience Scale
Supplemental material, sj-pdf-2-alr-10.1177_25424823261461527 for Psychometric evaluation of the Turkish version of the Bangor Dementia Resilience Scale by Burcu Akpınar Söylemez, Merve Aliye Akyol, Ecem Özgül, Hasret Erden, Özlem Küçükgüçlü, Marianna Tsatali, Görsev Yener and Birgit Teichmann in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
We sincerely thank all the participants who took part in this study. We would like to thank Taisiya Baysalova for proofreading the manuscript in English.
ORCID iDs
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and received approval from the Dokuz Eylul University of Institutional Ethics Committee, approval number: 9720-GOA. Confidentiality and anonymity of the data were strictly maintained throughout the study. Permission to use the scale was obtained from the original developer.
Consent to participate
Written informed consent was obtained from all participants or their legal representatives prior to participation. Participants were informed of the purpose of the study, the voluntary nature of their participation, and their right to withdraw at any time without any consequences.
Consent for publication
All participants or their legal representatives provided consent for the publication of anonymized data.
Author contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Birgit Teichmann is an Editorial Board Member of this journal but was not involved in the peer-review process of this article nor had access to any information regarding its peer-review.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.