
Abstract
Background
Plasma biomarkers for Alzheimer's disease (AD), including pTau217, are increasingly used to identify individuals at risk for underlying AD pathology. However, biomarkers alone do not capture the cognitive expression of disease, underscoring the need for brief cognitive measures capable of distinguishing impairment across biologically defined groups.
Objective
To evaluate the discriminative validity of the Brief Semantic Paired Associates Test (B-SPAT), a novel three-minute computerized cognitive screening test, among cognitively unimpaired and cognitively impaired older adults stratified by plasma pTau217 status.
Methods
Participants included 35 cognitively unimpaired (CU) older adults with negative plasma pTau217 (pTau217−), 22 cognitively impaired (CI) participants with pTau217−, and 20 CI participants with positive plasma pTau217 (pTau217+). All participants completed the B-SPAT, a fully digitized six-item semantic paired-associate learning task, along with a comprehensive neuropsychological battery.
Results
After adjustment for age, education, sex, and Mini-Mental State Examination scores, significant group differences in B-SPAT performance remained [F(2,70) = 8.28, p < 0.001]. Post-hoc analyses indicated that the CU pTau217− group performed significantly better than both cognitively impaired groups. Importantly, no significant differences were observed between the CI pTau217 + and CI pTau217− groups following covariate adjustment. Receiver operating characteristic analysis comparing CI pTau217 + and CU pTau217− participants yielded an area under the curve of 0.902 (SE = 0.041), with 95% sensitivity and 77.1% specificity.
Conclusions
The B-SPAT is a promising exploratory brief digital cognitive screening tool that differentiates cognitively impaired from cognitively unimpaired older adults across biomarker-defined groups and may have utility in community and primary care settings.
Keywords
Introduction
Alzheimer's disease (AD) is a progressive neurodegenerative disorder and the leading cause of dementia globally, currently affecting over 55 million individuals. 1 Advances in blood-based biomarkers, particularly phosphorylated tau species such as plasma phosphorylated tau 217 (pTau217), have demonstrated high diagnostic accuracy and predictive value for AD detection, comparable to cerebrospinal fluid (CSF) and positron emission tomography (PET) biomarkers.2–6 Plasma p-Tau217 has shown outstanding diagnostic accuracy (88–92%) for detecting AD pathology across both primary and secondary care settings.7,8 Reflecting this progress, recently issued clinical practice guidelines presented at the Alzheimer's Association International Conference now endorse the incorporation of FDA-cleared blood-based biomarker tests into the diagnostic evaluation of symptomatic individuals within specialty care contexts. 9 Plasma biomarkers are increasingly used to detect and monitor AD and ADRD in older adults. However, their interpretation may be complicated by biological and systemic factors unrelated to central nervous system pathology. 10 Cognitive assessment remains essential not only for establishing a clinical diagnosis but also for tracking disease progression and informing treatment decisions. 11
There is a critical need for brief, reliable, and scalable cognitive screening tools that can complement plasma biomarkers and be used in real-world settings like primary care for appropriate referral to specialty memory disorders clinics.12–14 This is particularly important since many individuals lack access to specialty clinics or advanced neuroimaging.15,16 Another consideration is that despite the promise of plasma biomarkers, autopsy studies have shown that some individuals harbor significant AD pathology without manifesting overt clinical symptoms during life. 17 Unfortunately, widely used brief cognitive screening tools often lack the sensitivity needed to detect early or subtle memory impairments, particularly in individuals with high levels of educational attainment or cognitive reserve.18–20 These limitations underscore the need for brief cognitive measures capable of detecting cognitive impairment and distinguishing individuals across biologically defined risk groups, including those stratified by plasma AD biomarkers.21,22
Memory binding, or the ability to form and maintain associations between discrete sets of information is a core process particularly vulnerable in the early stages of AD.23–25 Deficits in binding semantic elements, such as linking category cues with specific items or connecting names to faces, may emerge before global memory impairments are detectable with traditional neuropsychological tests. 26 Assessing memory binding allows researchers to probe the integrity of hippocampal and neocortical networks involved in associative learning and episodic memory consolidation, which are often impacted by AD pathology. 27 By focusing on how individuals encode, retrieve, and re-bind semantically related information, memory binding paradigms may measure subtle cognitive changes associated with early cognitive dysfunction.25,28
Several memory binding and associative learning tests are available to detect cognitive deficits associated with mild cognitive impairment and other memory disorders. The Free and Cued Selective Reminding Test (FCSRT) uses semantic cues during controlled learning to distinguish true storage impairments from normal age-related retrieval difficulties, demonstrating strong diagnostic validity across diverse populations, including primary care and multicultural samples.23,29–31 The Memory Binding Test (MBT) assesses paired-word learning and cued recall, reliably detecting subtle semantic binding deficits in amnestic mild cognitive impairment (MCI) stages, with performance linked to AD biomarkers.25,28,32 The MBT focuses primarily on semantic associative learning and memory binding processes 24 ; however, the test's performance may be influenced by age and education, though adjustments for these factors do not substantially change discriminative validity. 33 The Face-Name Associative Memory Exam (FNAME) evaluates visual-verbal associative memory, requiring participants to link faces with names or occupations. Poorer performance in older adults deemed clinically normal has been associated with early amyloid pathology, highlighting its relevance for early AD detection.26,27
While these measures are valid and reliable, demographic factors and sensory or educational differences may limit generalizability in some populations, underscoring the need for brief, scalable tools suitable for diverse clinical and community settings. Our research group has pioneered the development of innovative paradigms designed to capture early AD-related cognitive deficits, with a specific focus on heightened susceptibility to proactive semantic interference (PSI) or when old semantic learning disrupts the acquisition of new semantically competing information, failure to recover from PSI (frPSI), and semantic intrusion errors.34–40 These cognitive deficits are powerful markers for identifying cognitive impairment associated with AD-related processes and for predicting longitudinal clinical progression over time.41,42 Although semantic associative paradigms may not be specific to AD pathology, they may nevertheless provide clinically useful indicators of cognitive dysfunction under conditions of semantic interference and increased memory binding demands.43,44 Accordingly, the present study evaluated the Brief Semantic Paired Associates Test (B-SPAT) as a measure of cognitive dysfunction rather than as a direct marker of AD pathology.
In the current study, we introduce and evaluate the psychometric properties of a novel, brief, computerized cognitive screening test, developed using the theoretical framework employed by previous lengthier assessments as described above.43,44 The B-SPAT is a fully digitized, three-minute paired associates learning task designed to capture cognitive challenges associated with semantic interference and memory binding paradigms while substantially reducing administration time. This task exposes participants to a superordinate semantic category (e.g., animals) and requires them to bind items from two subordinate semantic categories (e.g., type of bird and non-bird animal). This paradigm challenges individuals to bind and retain associations under conditions that maximize the likelihood of semantic interference. Furthermore, we evaluate the discriminative validity of the B-SPAT for distinguishing cognitive/biological subgroups, including individuals stratified by plasma pTau217, a blood-based biomarker that has shown strong diagnostic accuracy for AD pathology.8,9 By linking cognitive performance on the B-SPAT with pTau217 status, we aim to assess whether subtle associative memory deficits correspond with biomarker-defined biological risk.
Methods
Sample
A total of 77 community-dwelling older adults aged 60 and above were recruited from a study funded by the Florida Department of Health. Participation was voluntary and the study was conducted at the University of Miami, Miller School of Medicine and was IRB-approved. All individuals completed a comprehensive clinical 45 and neuropsychological evaluation. Diagnostic group classification was adjudicated using a standardized multidisciplinary clinical consensus procedure that served as the reference standard for diagnostic classification. Importantly, the B-SPAT was not considered in the diagnostic determination to avoid potential circularity. This study was conducted and reported in accordance with key elements of the STARD (Standards for Reporting Diagnostic Accuracy Studies) guidelines. Participants were categorized into three groups based on cognitive status and pTau217 plasma levels as described below: Cognitively Unimpaired with negative pTau217 (CU pTau217-) n = 35, Cognitively Impaired with negative pTau217 (CI pTau217-) n = 22, and Cognitively Impaired with positive pTau217 (CI pTau217+) n = 20. The mean age of the full sample was 72.5 years (SD = 5.95). Across all groups, approximately 65% of participants were female. Demographic characteristics for each group are presented in Table 1. This study was designed as an exploratory pilot investigation intended to provide initial evidence regarding the discriminative validity of the B-SPAT.
Demographic characteristics for different diagnostic groups.

MMSE: Mini-Mental State Examination; B-SPAT: Brief Semantic Paired Associates Test; CU: Cognitively Unimpaired; CI: Cognitively Impaired.
Blood biomarker analysis
Blood samples were collected in EDTA tubes and centrifuged at room temperature within one hour of blood draw to isolate plasma. Plasma was then aliquoted and stored at −80°C. Plasma levels of pTau217 were measured using a Quanterix HD-X Analyzer and the pTau217 SiMoA assay kit. All samples were analyzed twice, and values were averaged to obtain the final concentration (reported in pg/mL). Samples were randomized and processed while blinded to participant's cognitive status, risk category, or other variables. All analyses followed the manufacturer's standard protocols. All samples employed in this investigation were required to have a coefficient of variation of less than 20%. Samples failing this quality threshold were excluded.
Thresholds for pTau217 positivity were based on internally derived cutoffs established using correspondence with amyloid PET visual reads consistent with recent studies. 46 A threshold of ≥0.55 pg/ml was established using receiver operating characteristic (ROC) curve analysis (AUC-0.91) and Youden's index, which yielded a sensitivity of 89.0% and a specificity of 82.4% for identifying amyloid PET positivity. 47 In a more recent study Ashton and colleagues, using independent global datasets, identified >0.63 pg/ml as the 95th percentile threshold for concordance with amyloid PET positivity. 48 However, they also noted that values between 0.55 and 0.63 pg/ml likely reflect accumulating AD pathology. This threshold was selected to maximize sensitivity for detecting early AD-related biological risk in this exploratory cohort.
Baseline diagnostic criteria
All of our community-dwelling participants had the ability to independently perform daily living activities, had knowledgeable collateral informants, and did not meet
Cognitively unimpaired group
Cognitively Unimpaired plasma pTau217 negative (CU pTau217-), participants (n = 35) (a) had no subjective memory concerns that were corroborated by a knowledgeable informant; (b) had a Global CDR score of 0; (c) did not meet criteria for either Major or Minor Neurocognitive Disorder by DSM-5 criteria; (d) scores within normal limits on all NACC-UDS tests, as mentioned above. Normal scores were defined as less than one standard deviation below expected levels for age, education, sex, and language of testing.
Cognitively impaired groups
A total of 42 participants were determined to be CI and these were distributed into two groups dependent on plasma p-Tau217 status (positive: CI pTau217+; or negative: CI pTau217-). The CI pTau217- group included 22 participants, while the CI pTau217 + group was composed of 20 participants. Participants in both cognitively impaired groups met the following criteria: (a) a memory complaint or noted cognitive decline preferably confirmed by a knowledgeable informant; (b) a Global CDR Score of 0.5; (c) did not meet criteria for a Major Neurocognitive Disorder based on DSM-5 criteria; (d) one or more memory measures were at least 1.5 standard deviations or more below the expected normative data.
The brief semantic paired associates test (B-SPAT)
The B-SPAT is a novel paradigm that is theoretically and empirically based on previous work developing cognitive challenge measures that tap semantic interference and literature on memory-binding vulnerabilities among individuals at risk for AD.25–33,43,44 The B-SPAT was developed as a challenging task designed to detect subtle cognitive deficits associated with early cognitive impairment and memory dysfunction. It consists of six items, each pairing a specific category word (e.g., bird) with a broader, non-overlapping category word (e.g., animal, non bird). For example, the first stem word “Pigeon” is coupled with “Cow”, the second stem word “Chicken” is coupled with “Alligator”, etc. Examinees learn all six pairs in a single trial, then recall the target when given the stem. By linking specific semantic exemplars (birds) with broader but non-inclusive categories (animals, non-birds), the task places greater cognitive demands, making it potentially sensitive to subtle early cognitive inefficiencies. Previous pilot testing with 43 cognitively unimpaired community dwelling older adults, indicated that the fully digitized test takes three minutes to administer in English or Spanish and demonstrated moderate test–retest reliability (r = 0.61, p < 0.001) over a three to four-week time interval. Unlike lengthier semantic interference paradigms, the B-SPAT was specifically designed to maximize brevity, scalability, and feasibility for implementation in primary care and community settings.
Statistical analysis
Statistical analyses were conducted using SPSS version 31. Group differences in demographic variables were examined using analyses of variance (ANOVA) and chi-square analyses, as appropriate. Analysis of covariance (ANCOVA) was employed to compare B-SPAT performance across diagnostic groups while adjusting for age, education, sex, and MMSE scores. Bonferroni-adjusted post-hoc comparisons were used to evaluate between-group differences. Receiver operating characteristic (ROC) analyses were conducted to examine the discriminative utility of the B-SPAT. Optimal classification thresholds were determined using the Youden Index and logistic regression procedures. Statistical significance was set at p < 0.05. Although the sample size was modest, the observed effect sizes and ROC estimates suggest adequate sensitivity for this initial proof-of-concept investigation. Given the exploratory nature of the study, formal a priori power calculations were not performed.
Results
Demographic and cognitive characteristics are summarized in Table 1. B-SPAT performance differed significantly across diagnostic groups overall (p < 0.001). Groups also differed in educational attainment, global cognition (MMSE), and sex distribution, whereas age differences did not reach statistical significance. Accordingly, subsequent analyses adjusted for age (which approached statistical significance, p = 0.062), education, MMSE score, and sex. Significant differences in B-SPAT scores between diagnostic groups remained following covariate adjustment, F (2, 70) = 8.28, p < 0.001 (Table 2). Bonferroni-adjusted post-hoc comparisons indicated that the CU pTau217− group demonstrated the highest adjusted mean performance (M = 2.72, SE = 0.27)], relative to the CI pTau217− group (M = 1.48, SE = 0.36), and CI pTau217 + group (M = 0.823, SE = 0.60). Importantly, after adjustment, no significant post-hoc differences were observed between the CI pTau217 + and CI pTau217− groups. These findings suggest that B-SPAT performance was more strongly associated with the presence of mild cognitive impairment than with plasma pTau217 status alone.
B-SPAT scores after adjustment for age, education, MMSE, and sex.
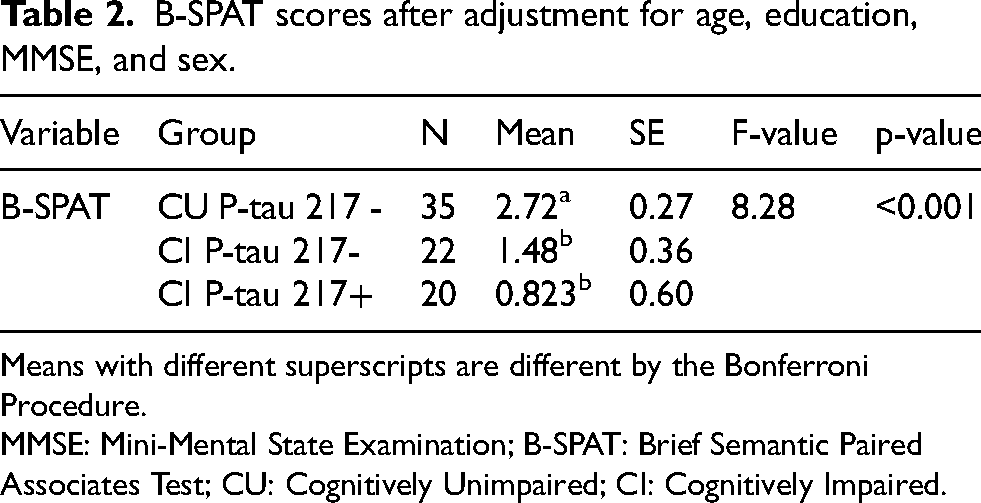
Means with different superscripts are different by the Bonferroni Procedure.
MMSE: Mini-Mental State Examination; B-SPAT: Brief Semantic Paired Associates Test; CU: Cognitively Unimpaired; CI: Cognitively Impaired.
To evaluate the discriminative utility of the B-SPAT, an ROC curve analysis was conducted comparing CI individuals with positive plasma pTau217 status (CI pTau217+) to CU pTau217− participants (CU pTau217-) consistent with the binary classification framework required for ROC analyses and the greatest observed separation in adjusted B-SPAT performance; therefore, the resulting classification metrics may represent an upper-bound estimate of discriminative accuracy. The AUC was 0.902 (SE = 0.041, 95% CI [0.823, 0.982], p < 0.001), indicating high discriminative accuracy (Figure 1). Using the Youden index and logistic regression, optimal classification yielded a sensitivity of 95% and specificity of 77.1%. A separate ROC analysis comparing the CI pTau217 + and CI pTau217− groups was not conducted because covariate-adjusted analyses revealed no significant post-hoc differences in B-SPAT performance between these groups.
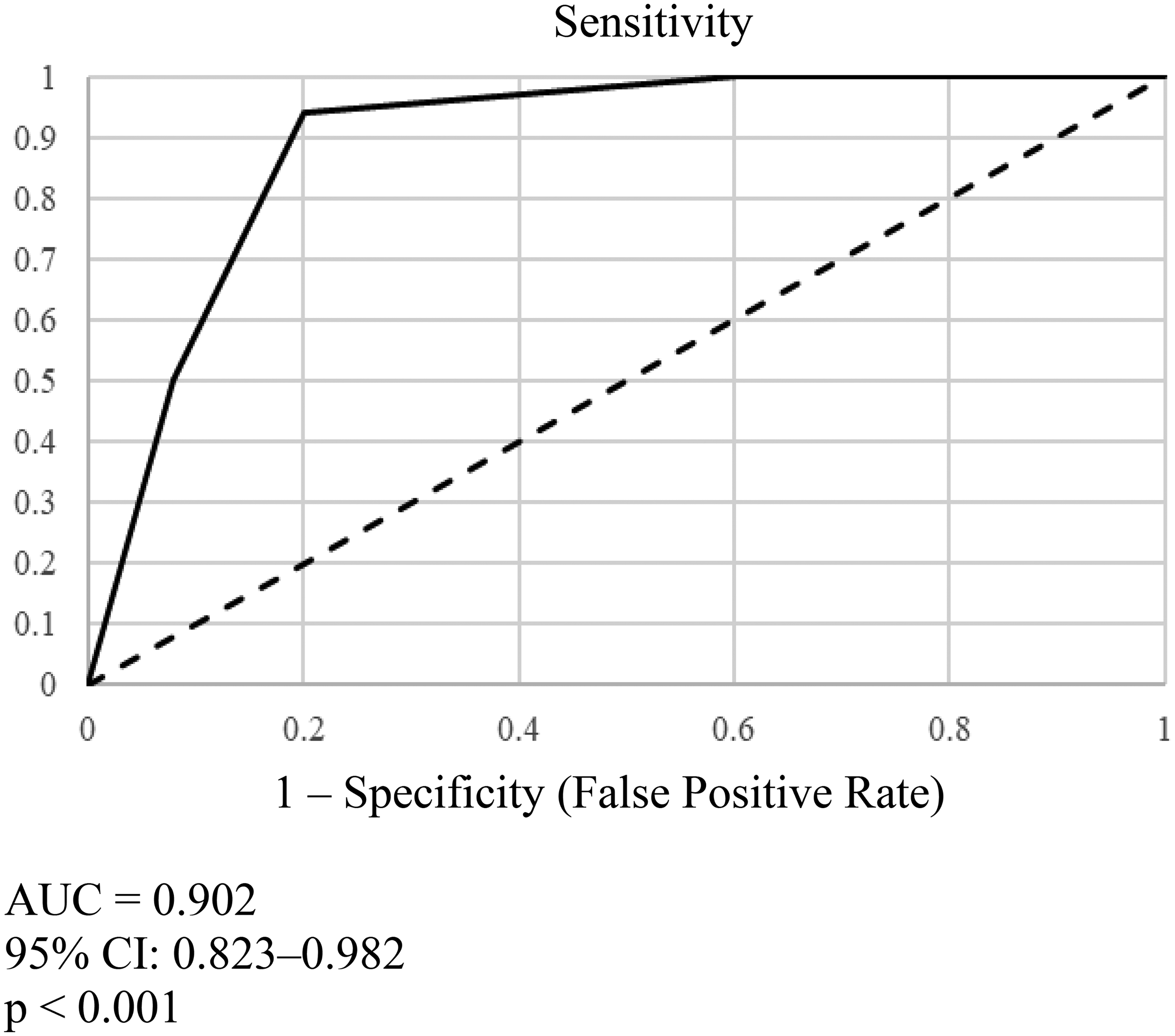
Receiver operating characteristic (ROC) curve for B-SPAT performance distinguishing cognitively impaired participants with positive plasma pTau217 (CI pTau217+) from cognitively unimpaired participants with negative plasma pTau217 (CU pTau217−).
Discussion
This study examined the B-SPAT, a novel three-minute computerized cognitive screening tool, for its ability to differentiate cognitively unimpaired older adults from cognitively impaired individuals without dementia across groups stratified by plasma pTau217 status. After adjustment for demographic and global cognitive covariates, the B-SPAT demonstrated significant mean differences between CU and CIgroups, as well as high sensitivity and strong ROC performance, indicating robust discrimination between CU and CI participants. Importantly, following covariate adjustment, the B-SPAT did not differentiate between CI individuals who were pTau217 + and those who were pTau217−.The fact that CI individuals with a positive biological marker strongly associated with AD measured by plasma pTau217 could not be differentiated from CI participants who were pTau217 negative, suggests that cognitive impairment, rather than plasma pTau217 status alone, primarily drove the observed differences between cognitively unimpaired and cognitively impaired participants. This interpretation was supported by the covariate-adjusted group comparisons described in the Results. Accordingly, the present findings do not support the interpretation of the B-SPAT as a measure of AD-specific pathology, but rather as a brief cognitive screening tool sensitive to the presence of cognitive impairment.
We posit that the B-SPAT's sensitivity to impairment in CI individuals without dementia is likely due to its unique cognitive demands using single trial paired associate learning. Participants must remember links between semantically related items (i.e., pairing a bird with a non-bird animal), which creates strong competition and renders the test especially sensitive to the memory binding problems seen in early AD and other memory disorders. Unlike many traditional screening measures that rely on rote recall or recognition, the B-SPAT targets higher-level semantic-episodic integration, a process known to be vulnerable in very early stages of cognitive impairment.25,44,51 The finding that CI individuals demonstrated impaired B-SPAT scores regardless of their pTau217 status, suggests that the task is sensitive to mild cognitive impairment itself and can serve as a rapid method of identifying early cognitive impairment. This finding further suggests that the B-SPAT reflects cognitive dysfunction irrespective of underlying pTau217 status. Taken together, the obtained pattern of findings suggests that brief cognitive measures such as the B-SPAT and plasma biomarkers of AD-related risk capture distinct but clinically relevant aspects of cognitive and biological status. Elevation of plasma pTau217 in the absence of overt cognitive impairment should be interpreted cautiously, as AD pathology may develop many years before clinical symptoms emerge,52,53 and autopsy studies have shown that some older adults may harbor significant AD pathology without manifesting cognitive decline during life.17,54
As an exploratory pilot study conducted at a single center, findings should be interpreted cautiously until replicated in larger and more diverse samples. While this is a promising pilot study, several limitations should be noted. The sample size, though adequate for initial validation, was relatively modest and may have limited generalizability. In addition, the cross-sectional design precludes conclusions about the B-SPAT's prognostic value or sensitivity to longitudinal cognitive decline; studies which are forthcoming. Another consideration is that while plasma pTau217 is a well-validated biomarker of AD pathology, 9 it does not fully capture the complexity of mixed pathologies that may contribute to cognitive impairment in older adults. Importantly, the current study compared cognitively unimpaired individuals with participants already demonstrating measurable cognitive impairment. Although all cognitively impaired participants remained functionally independent and did not meet DSM-5 criteria for Major Neurocognitive Disorder, heterogeneity within the CI group may still have included individuals along different points of the mild impairment continuum. Therefore, the present findings should be interpreted as reflecting discrimination between cognitively unimpaired and cognitively impaired older adults rather than detection of preclinical AD. Finally, although the computerized format of the B-SPAT offers scalability, usability and accessibility across individuals with varying levels of digital literacy and cultural background, this novel brief screening tool warrants further evaluation of its implementation potential across clinical contexts. Future studies should also examine usability, digital literacy requirements, and participant acceptance across diverse populations of older adults.
Most older adults lack access to specialized cognitive testing, and primary care physicians often have limited time for extensive assessments, creating a critical need for brief, scalable tools that can reliably screen for cognitive impairment.12,13,55 The B-SPAT directly addresses this gap by offering a rapid, fully computerized assessment that can be completed in under three minutes. Importantly, this type of scalable computerized screening may be particularly valuable in community and primary care settings where access to specialty neuropsychological services is limited. As a novel and efficient cognitive screening tool, the B-SPAT has the potential to enhance the clinical interpretability of emerging plasma AD biomarkers, such as pTau217, particularly in settings where longer neuropsychological batteries are not feasible. By providing a quick and accessible measure of cognitive function, the B-SPAT may help identify individuals most likely to benefit from further diagnostic evaluation, enrollment in clinical trials, or early interventions. Future research should evaluate the utility of the B-SPAT relative to other brief cognitive screening tools across broader populations and for longitudinal disease monitoring.
Together, the findings of this study support the use of brief computerized cognitive screening as a clinically interpretable correlate of biomarker-defined AD risk among older adults. In this context, the combination of a very brief computerized cognitive measure such as the B-SPAT with plasma pTau217 testing provides an exceptionally practical and deployable approach for identifying individuals who warrant further evaluation but may not otherwise have access to specialty care. CU individuals who were AD biomarker negative demonstrated better B-SPAT performance than CI individuals regardless of AD biomarker status within the CI group. Blood-based biomarkers are tools that may have value in assessing the potential presence of underlying disease; however, clinicians are in dire need of brief cognitive screening tools that can more fully characterize persons in need of further diagnostic workup beyond what the presence or absence of a positive biomarker alone can provide. This highlights the potential value of brief cognitive screening tools such as the B-SPAT in providing clinically interpretable cognitive information alongside blood-based biomarkers. Used together in clinical settings, these approaches may help support early detection, guide appropriate referrals, and improve access to further diagnostic evaluation and emerging therapies and those in development.10,56 This work is directly relevant to AD research because it evaluates a brief cognitive screening approach in relation to plasma pTau217, a widely studied biomarker of AD pathology.
Footnotes
Acknowledgements
The authors thank the participants and their families for their invaluable contributions to this research.
ORCID iDs
Ethical considerations
This study was approved by the Institutional Review Board of the University of Miami Miller School of Medicine and was conducted in accordance with the Declaration of Helsinki.
Consent to participate
Written informed consent was obtained from all participants and their informants prior to enrollment.
Consent for publication
All participants provided consent for the use of de-identified research data for publication purposes.
Author contribution(s)
Funding
This work was supported by the following grants- CCT/23A10 and DEEP-AA FED/ RO1AG077677.
CCT State, Deep-AA FED, (grant number 23A10, RO1AG077677).
Declaration of conflicting interests
The University of Miami, Dr. Curiel Cid and Dr. Loewenstein, hold the rights to intellectual property used in the study and may financially benefit from the commercialization of the intellectual property. Other authors declare no conflicts of interest.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request and subject to institutional and regulatory requirements.